
Relationship between Phase Angle and Physical Activity Intensity among Community-Dwelling Older Adults in Japan: A Cross-Sectional Study
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.1.1. Sample Size Calculation
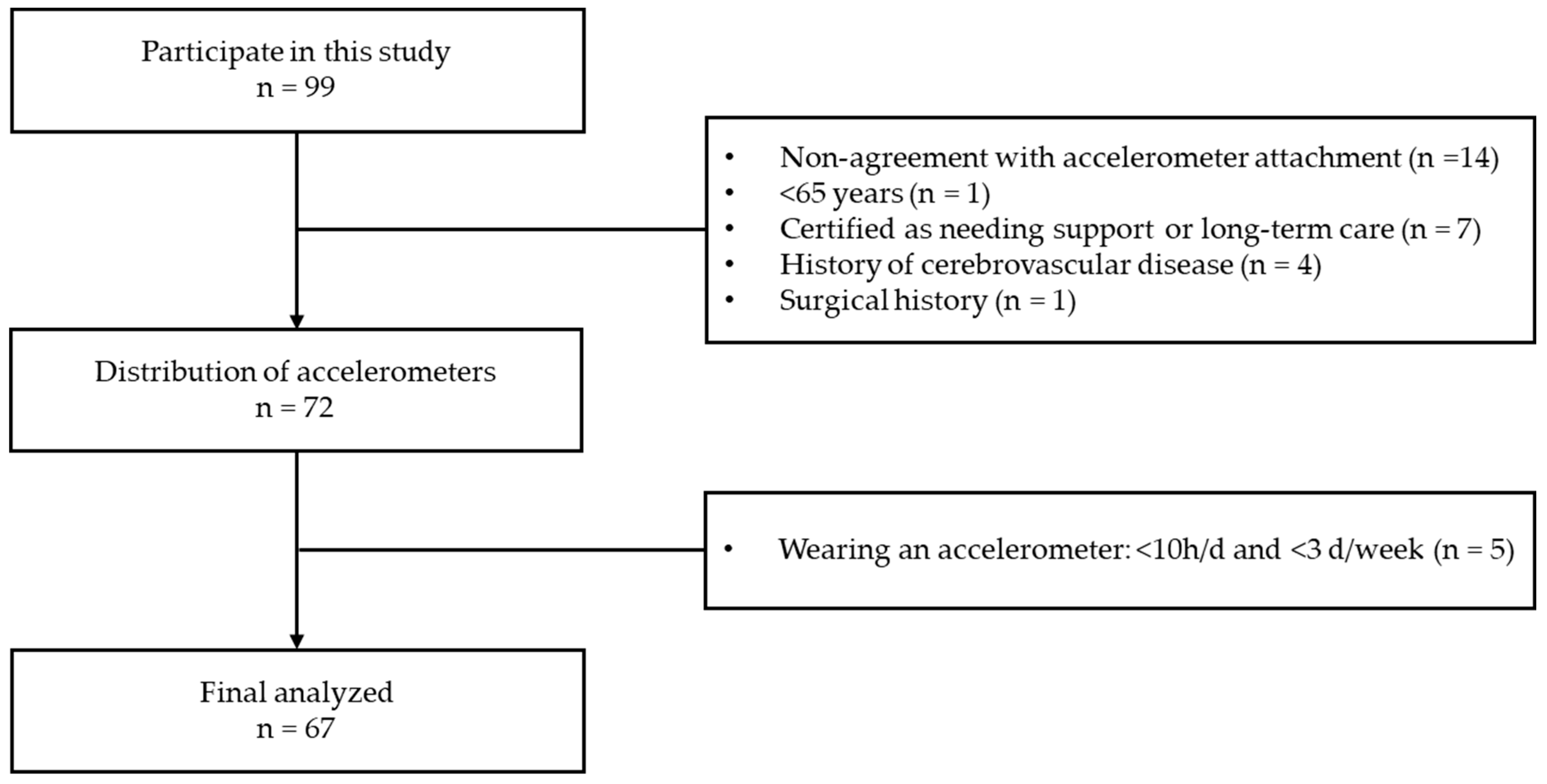
2.1.2. Recruitment of Research Participants and Selection of Participants for Analysis
2.2. Ethical Considerations
2.3. Measurement Variables
2.3.1. Participant Characteristics
2.3.2. Physical Activity
2.3.3. Body Composition
2.3.4. Global Leadership Initiative on Malnutrition (GLIM) Criteria
2.3.5. Grip Strength
2.3.6. Short Physical Performance Battery (SPPB)
2.3.7. Muscle Quality
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Correlation of PhA with LPA and MVPA
3.3. Model Selection
3.4. Relationship between PhA and Physical Activity (Bayesian Statistics)
3.5. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis—Clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm-Leen, E.R.; Hall, Y.N.; Horwitz, R.I.; Chertow, G.M. Phase angle, frailty and mortality in older adults. J. Gen. Intern. Med. 2014, 29, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Mundstock, E.; Amaral, M.A.; Baptista, R.R.; Sarria, E.E.; Dos Santos, R.R.G.; Filho, A.D.; Mattiello, R. Association between phase angle from bioelectrical impedance analysis and level of physical activity: Systematic review and meta-analysis. Clin. Nutr. 2019, 38, 1504–1510. [Google Scholar] [CrossRef]
- von Loeffelholz, C.; Birkenfeld, A.L. Non-Exercise Activity Thermogenesis in Human Energy Homeostasis. Endotext [Internet]. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK279077/ (accessed on 15 November 2023).
- Gunn, S.M.; Halbert, J.A.; Giles, L.C.; Stepien, J.M.; Miller, M.D.; Crotty, M. Bioelectrical phase angle values in a clinical sample of ambulatory rehabilitation patients. Dyn. Med. 2008, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Selberg, O.; Selberg, D. Norms and correlates of bioimpedance phase angle in healthy human subjects, hospitalized patients, and patients with liver cirrhosis. Eur. J. Appl. Physiol. 2002, 86, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, A.; Pillon, L.; Dumler, F. Impedance vector distribution by sex, race, body mass index, and age in the United States: Standard reference intervals as bivariate Z scores. Nutrition 2002, 18, 153–167. [Google Scholar] [CrossRef]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Bielemann, R.M.; Gallagher, D.; Heymsfield, S.B. Phase angle and its determinants in healthy subjects: Influence of body composition. Am. J. Clin. Nutr. 2016, 103, 712–716. [Google Scholar] [CrossRef]
- Barbosa-Silva, M.C.G.; Barros, A.J.; Wang, J.; Heymsfield, S.B.; Pierson, R.N., Jr. Bioelectrical impedance analysis: Population reference values for phase angle by age and sex. Am. J. Clin. Nutr. 2005, 82, 49–52. [Google Scholar] [CrossRef]
- Asano, Y.; Nagata, K.; Shibuya, K.; Fujii, Y.; Kitano, N.; Okura, T. Association of 24-h movement behaviors with phase angle in community-dwelling older adults: A compositional data analysis. Aging Clin. Exp. Res. 2023, 35, 1469–1476. [Google Scholar] [CrossRef]
- Soma, Y.; Tsunoda, K.; Kitano, N.; Jindo, T.; Tsuji, T.; Saghazadeh, T.; Okura, T. Relationship between built environment attributes and physical function in Japanese community-dwelling older adults. Geriatr. Gerontol. Int. 2017, 17, 382–390. [Google Scholar] [CrossRef]
- Iwai, N.; Yoshiike, N.; Saitoh, S.; Nose, T.; Kushiro, T.; Tanaka, H. Leisure-time physical activity and related lifestyle characteristics among middle-aged Japanese. J. Epidemiol. 2000, 10, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Shibata, A.; Oka, K. Environmental, psychological, and social influences on physical activity among Japanese adults: Structural equation modeling analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 61. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yatsuya, H.; Hanibuchi, T.; Ota, A.; Naito, H.; Otsuka, R.; Murata, C.; Hirakawa, Y.; Chiang, C.; Uemura, M.; et al. Positive association of physical activity with both objective and perceived measures of the neighborhood environment among older adults: The Aichi Workers’ Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 7971. [Google Scholar] [CrossRef]
- O’Loughlin, J.; Casanova, F.; Fairhurst-Hunter, Z.; Hughes, A.; Bowden, J.; Watkins, E.R.; Freathy, R.M.; Millwood, I.Y.; Lin, K.; Chen, Z.; et al. Mendelian randomisation study of body composition and depression in people of East Asian ancestry highlights potential setting-specific causality. BMC Med. 2023, 21, 37. [Google Scholar] [CrossRef] [PubMed]
- Anzai, I.; Sakamoto, K.; Togo, M.; Katsunuma, H. A comparative study of body composition of urban and rural Japanese boys 12 to 14 years old. Ann. Hum. Biol. 1981, 8, 109–117. [Google Scholar] [CrossRef]
- Wang, J.; Rennie, K.L.; Gu, W.; Li, H.; Yu, Z.; Lin, X. Independent associations of body-size adjusted fat mass and fat-free mass with the metabolic syndrome in Chinese. Ann. Hum. Biol. 2009, 36, 110–121. [Google Scholar] [CrossRef]
- Germano, M.L.; Dos Santos Gomes, C.; Azevedo, I.G.; Fernandes, J.; de Medeiros Freitas, R.V.; Guerra, R.O. Relationship between phase angle and physical performance measures in community-dwelling older adults. Exp. Gerontol. 2021, 152, 111466. [Google Scholar] [CrossRef]
- Kajiyama, S.; Nakanishi, N.; Yamamoto, S.; Ichikawa, T.; Okamura, T.; Hashimoto, Y.; Kitagawa, N.; Hamaguchi, M.; Fukui, M. The impact of nutritional markers and dietary habits on the bioimpedance phase angle in older individuals. Nutrients 2023, 15, 3599. [Google Scholar] [CrossRef]
- Matias, C.N.; Nunes, C.L.; Francisco, S.; Tomeleri, C.M.; Cyrino, E.S.; Sardinha, L.B.; Silva, A.M. Phase angle predicts physical function in older adults. Arch. Gerontol. Geriatr. 2020, 90, 104151. [Google Scholar] [CrossRef]
- Akamatsu, Y.; Kusakabe, T.; Arai, H.; Yamamoto, Y.; Nakao, K.; Ikeue, K.; Ishihara, Y.; Tagami, T.; Yasoda, A.; Ishii, K.; et al. Phase angle from bioelectrical impedance analysis is a useful indicator of muscle quality. J. Cachexia Sarcopenia Muscle 2022, 13, 180–189. [Google Scholar] [CrossRef]
- Uemura, K.; Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Kim, M.; Kurita, S.; Ishii, H.; Shimada, H. Predictivity of bioimpedance phase angle for incident disability in older adults. J. Cachexia Sarcopenia Muscle 2020, 11, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Honda, T.; Chen, S.; Narazaki, K.; Kumagai, S. Dose–response association between accelerometer-assessed physical activity and incidence of functional disability in older Japanese adults: A 6-Year Prospective Study. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1763–1770. [Google Scholar] [CrossRef] [PubMed]
- Peduzzi, P.; Concato, J.; Feinstein, A.R.; Holford, T.R. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J. Clin. Epidemiol. 1995, 48, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Government of Nara City. Population of Nara City. Available online: https://www-city-nara-lg-jp.translate.goog/soshiki/7/150603.html?_x_tr_sl=ja&_x_tr_tl=en&_x_tr_hl=ja (accessed on 15 November 2023).
- Government of Nara City. Population Trends. Available online: https://www-city-nara-lg-jp.translate.goog/soshiki/7/128757.html?_x_tr_sl=ja&_x_tr_tl=en&_x_tr_hl=ja (accessed on 15 November 2023).
- Government of Nara City. 2023 Basic Statistical Survey Data by School. Available online: https://www.city.nara.lg.jp/uploaded/attachment/162862.pdf (accessed on 15 November 2023).
- Murakami, H.; Kawakami, R.; Nakae, S.; Yamada, Y.; Nakata, Y.; Ohkawara, K.; Sasai, H.; Ishikawa-Takata, K.; Tanaka, S.; Miyachi, M. Accuracy of 12 wearable devices for estimating physical activity energy expenditure using a metabolic chamber and the doubly labeled water method: Validation study. JMIR mHealth uHealth 2019, 7, e13938. [Google Scholar] [CrossRef] [PubMed]
- Japan Physical Activity Research Platform. Device. Available online: http://paplatform.umin.jp (accessed on 29 March 2023). (In Japanese).
- Gibbs, B.B.; Hergenroeder, A.L.; Katzmarzyk, P.T.; Lee, I.M.; Jakicic, J.M. Definition, measurement, and health risks associated with sedentary behavior. Med. Sci. Sport. Exerc. 2015, 47, 1295–3000. [Google Scholar] [CrossRef] [PubMed]
- Hart, T.L.; Swartz, A.M.; Cashin, S.E.; Strath, S.J. How many days of monitoring predict physical activity and sedentary behaviour in older adults? Int. J. Behav. Nutr Phys. Act. 2011, 8, 62. [Google Scholar] [CrossRef] [PubMed]
- Kubo, Y.; Noritake, K.; Nakashima, D.; Fujii, K.; Yamada, K. Relationship between nutritional status and phase angle as a noninvasive method to predict malnutrition by sex in older inpatients. Nagoya J. Med. Sci. 2021, 83, 31–40. [Google Scholar] [PubMed]
- Kurban, M.; Zeng, N.; Wang, M.; Liu, H.; Wu, J.R.; Feng, G.; Liu, M.; Guo, Q. Role of Human Body Composition Analysis and Malnutrition Risk Questionnaire in the Assessment of Nutritional Status of Patients with Initially Diagnosed Crohn’s Disease. Front. Med. 2020, 7, 106. [Google Scholar] [CrossRef]
- Tanaka, H.; Kitamura, G.; Tamura, M.; Nankaku, M.; Taniguchi, M.; Kikuchi, T.; Maki, T.; Ikeguchi, R.; Miyamoto, S.; Takahashi, R.; et al. Pre-stroke physical activity is associated with post-stroke physical activity and sedentary behavior in the acute phase. Sci. Rep. 2023, 13, 21298. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Jentoft, A.J.; van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Kong, H.H.; Won, C.W.; Kim, W. Effect of sarcopenic obesity on deterioration of physical function in the elderly. Arch. Gerontol. Geriatr. 2020, 89, 104065. [Google Scholar] [CrossRef] [PubMed]
- Akazawa, N.; Kishi, M.; Hino, T.; Tsuji, R.; Tamura, K.; Hioka, A.; Moriyama, H. Relationship between muscle mass and fraction of intramuscular adipose tissue of the quadriceps in older inpatients. PLoS ONE 2022, 17, e0263973. [Google Scholar] [CrossRef]
- Gelman, A. Prior distributions for variance parameters in hierarchical models (comment on article by Browne and Draper). Bayesian Anal. 2006, 1, 515–534. [Google Scholar] [CrossRef]
- Gelman, A.; Carlin, J.B.; Stern, H.S.; Dunson, D.B.; Vehtari, A.; Rubin, D.B. Bayesian Data Analysis; Chapman & Hall/Crc.C: Boca Raton, FL, USA, 2013. [Google Scholar]
- Watanabe, S. Asymptotic equivalence of Bayes cross validation and widely applicable information criterion in singular learning theory. J. Mach. Learn. Res. 2010, 11, 3571–3594. [Google Scholar]
- Bellido, D.; García-García, C.; Talluri, A.; Lukaski, H.C.; García-Almeida, J.M. Future lines of research on phase angle: Strengths and limitations. Rev. Endocr. Metab. Disord. 2023, 24, 563–583. [Google Scholar] [CrossRef]
- Yamada, Y.; Yoshida, T.; Murakami, H.; Kawakami, R.; Gando, Y.; Ohno, H.; Tanisawa, K.; Konishi, K.; Julien, T.; Kondo, E.; et al. Phase angle obtained via bioelectrical impedance analysis and objectively measured physical activity or exercise habits. Sci. Rep. 2022, 12, 17274. [Google Scholar] [CrossRef]
- Government of Nara City. Environment of Nara City (Reiwa 4th Edition). Available online: https://www.city.nara.lg.jp/uploaded/attachment/162712.pdf (accessed on 15 November 2023).
- Government of Kasama City. Reiwa 4th Edition Statistics Kasama. Available online: https://www.city.kasama.lg.jp/data/doc/1677035792_doc_70_0.pdf (accessed on 15 November 2023).
- Kruschke, J.K. Bayesian estimation supersedes the t-test. J. Exp. Psychol. 2013, 142, 573–603. [Google Scholar] [CrossRef]
- Martins, A.D.; Fernandes, O.; Oliveira, R.; Bilro, V.; Lopes, G.; Rego, A.M.; Parraça, J.A.; Raimundo, A.M.M.; Brito, J.P. Effects of exercise programs on phase angle in older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2022, 103, 104787. [Google Scholar] [CrossRef]
- Safdar, A.; Hamadeh, M.J.; Kaczor, J.J.; Raha, S.; Debeer, J.; Tarnopolsky, M.A. Aberrant mitochondrial homeostasis in the skeletal muscle of sedentary older adults. PLoS ONE 2010, 5, e10778. [Google Scholar] [CrossRef]
- Uemura, K.; Yamada, M.; Saho, K.; Okamoto, H. Association of bio-impedance phase angle and physical activity level in older adults. Phys. Ther. Jpn. 2019, 46, 143–151. [Google Scholar]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://iris.who.int/bitstream/handle/10665/336656/9789240015128-eng.pdf?isAllowed=y&sequence=1 (accessed on 18 December 2023).
- Keadle, S.K.; McKinnon, R.; Graubard, B.I.; Troiano, R.P. Prevalence and trends in physical activity among older adults in the United States: A comparison across three national surveys. Prev. Med. 2016, 89, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Amagasa, S.; Fukushima, N.; Kikuchi, H.; Takamiya, T.; Oka, K.; Inoue, S. Light and sporadic physical activity overlooked by current guidelines makes older women more active than older men. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 59. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa-Takata, K.; Nakae, S.; Sasaki, S.; Katsukawa, F.; Tanaka, S. Age-related decline in physical activity level in the healthy older Japanese population. J. Nutr. Sci. Vitaminol. 2021, 67, 330–338. [Google Scholar] [CrossRef]
- Buckinx, F.; Reginster, J.Y.; Dardenne, N.; Croisiser, J.L.; Kaux, J.F.; Beaudart, C.; Slomian, J.; Bruyère, O. Concordance between muscle mass assessed by bioelectrical impedance analysis and by dual energy X-ray absorptiometry: A cross-sectional study. BMC Musculoskelet. Disord. 2015, 16, 60. [Google Scholar] [CrossRef]
- Jayanama, K.; Putadechakun, S.; Srisuwarn, P.; Vallibhakara, S.A.; Shantavasinkul, P.C.; Sritara, C.; Kantachuvesiri, S.; Komindr, S. Evaluation of Body Composition in Hemodialysis Thai Patients: Comparison between Two Models of Bioelectrical Impedance Analyzer and Dual-Energy X-Ray Absorptiometry. J. Nutr. Metab. 2018, 2018, 4537623. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Frequency (n = 67) | |
|---|---|---|
| Age (years), mean ± SD | 78.4 ± 5.5 | |
| Female (%) | 83.6 | |
| Body mass index (kg/m2), mean ± SD | 22.6 ± 3.4 | |
| Education (years), mean ± SD | 13.1 ± 2.1 | |
| Living alone (%) | 44.8 | |
| Accelerometer data | Wearing time (min/d), mean ± SD | 850.9 ± 93.9 |
| LPA (min/d), mean ± SD | 346.3 ± 84.0 | |
| MVPA (min/d), mean ± SD | 38.0 ± 23.2 | |
| Body Composition | Phase angle (°), mean ± SD | 4.4 ± 0.6 |
| Low phase angle (%) | 52.2 | |
| SMI (kg/m2), mean ± SD | 5.9 ± 0.8 | |
| Malnutrition (%) | 11.9 | |
| Grip strength (kg), mean ± SD | 22.1 ± 6.1 | |
| SPPB | Balance (score), median (first-third quartile) | 4 (4-4) |
| Gait speed (score), median (first-third quartile) | 4 (4-4) | |
| Chair stand (score), median (first-third quartile) | 4 (4-4) | |
| Total (score), median (first-third quartile) | 12 (12-12) | |
| Gait speed (m/s), mean ± SD | 1.5 ± 0.4 | |
| Muscle quality, mean ± SD | 44.0 ± 11.8 | |
| Characteristic | Correlation Coefficient | p-Value |
|---|---|---|
| Age (years) | −0.343 | <0.01 |
| Sex | −0.526 | <0.01 |
| Body mass index (kg/m2) | 0.204 | 0.099 |
| LPA (min/d) | −0.089 | 0.475 |
| MVPA (min/d) | 0.305 | 0.012 |
| SMI (kg/m2) | 0.581 | <0.01 |
| Malnutrition | −0.176 | 0.155 |
| Grip strength (kg) | 0.645 | <0.01 |
| SPPB; balance tests (score) | −0.011 | 0.927 |
| Gait speed (m/s) | −0.068 | 0.583 |
| Muscle quality | −0.250 | 0.041 |
| Model 1 | Model 2 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EAP | β | t | p-Value | 95% Bayesian CI | EAP | β | t | p-Value | 95% Bayesian CI | ||||
| LPA | −0.002 | −0.228 | −1.775 | 0.08 | −0.003 | 0.001 | −0.001 | −0.113 | −0.96 | 0.341 | −0.002 | 0.001 | |
| MVPA | 0.01 | 0.389 | 2.93 | 0.005 | 0.003 | 0.016 | 0.007 | 0.256 | 2.347 | 0.022 | 0.001 | 0.012 | |
| Age | −0.018 | −0.173 | −1.537 | 0.13 | −0.041 | 0.006 | |||||||
| Sex | 0.097 | 0.064 | 0.28 | 0.781 | −0.581 | 0.766 | |||||||
| Body mass index | 0.017 | 0.098 | 0.592 | 0.556 | −0.039 | 0.073 | |||||||
| SMI | 0.12 | 0.175 | 0.712 | 0.479 | −0.208 | 0.445 | |||||||
| Malnutrition | −0.017 | −0.014 | −0.115 | 0.909 | −0.318 | 0.265 | |||||||
| Grip strength | 0.034 | 0.358 | 1.64 | 0.107 | −0.008 | 0.074 | |||||||
| SPPB (balance tests) | −0.008 | −0.004 | −0.052 | 0.959 | −0.331 | 0.309 | |||||||
| Gait speed | −0.156 | −0.102 | −0.988 | 0.327 | −0.464 | 0.161 | |||||||
| Muscle quality | 0.002 | 0.043 | 0.385 | 0.702 | −0.008 | 0.012 | |||||||
| WAIC = 115.001 | WAIC = 94.017 | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakashima, D.; Fujii, K.; Tsubouchi, Y.; Kubo, Y.; Yorozuya, K.; Noritake, K.; Tomiyama, N.; Tsujishita, S.; Iitsuka, T. Relationship between Phase Angle and Physical Activity Intensity among Community-Dwelling Older Adults in Japan: A Cross-Sectional Study. Healthcare 2024, 12, 167. https://doi.org/10.3390/healthcare12020167
Nakashima D, Fujii K, Tsubouchi Y, Kubo Y, Yorozuya K, Noritake K, Tomiyama N, Tsujishita S, Iitsuka T. Relationship between Phase Angle and Physical Activity Intensity among Community-Dwelling Older Adults in Japan: A Cross-Sectional Study. Healthcare. 2024; 12(2):167. https://doi.org/10.3390/healthcare12020167
Chicago/Turabian StyleNakashima, Daiki, Keisuke Fujii, Yoshihito Tsubouchi, Yuta Kubo, Kyosuke Yorozuya, Kento Noritake, Naoki Tomiyama, Soma Tsujishita, and Terufumi Iitsuka. 2024. "Relationship between Phase Angle and Physical Activity Intensity among Community-Dwelling Older Adults in Japan: A Cross-Sectional Study" Healthcare 12, no. 2: 167. https://doi.org/10.3390/healthcare12020167