

The Association between Sleep Quality and Depressive Symptoms among Stroke Survivors and Caregivers
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurement Tools
2.2.1. Sociodemographic Questionnaire
2.2.2. Patient Health Questionnaire (PHQ-9)
2.2.3. Pittsburgh Sleep Quality Index (PSQI)
2.3. Data Collection Procedures
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Limitation of the Study
4.2. Implications and Recommendations for Nursing Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. The Top 10 Causes of Death. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 18 February 2022).
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Towfighi, A.; Ovbiagele, B.; El Husseini, N.; Hackett, M.L.; Jorge, R.E.; Kissela, B.M.; Mitchell, P.H.; Skolarus, L.E.; Whooley, M.A.; Williams, L.S. Poststroke depression: A scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2017, 48, e30–e43. [Google Scholar] [CrossRef] [PubMed]
- Al-Senani, F.; Al-Johani, M.; Salawati, M.; Alhazzani, A.; Morgenstern, L.B.; Ravest, V.S.; Cuche, M.; Eggington, S. An Epidemiological Model for First Stroke in Saudi Arabia. J. Stroke Cerebrovasc. Dis. 2020, 29, 104465. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, B.A.; Alenazi, A.M.; Hoover, J.C.; Alshehri, M.M.; Alghamdi, M.S.; Osailan, A.M.; Khunti, K. Incidence of stroke among Saudi population: A systematic review and meta-analysis. Neurol. Sci. 2020, 41, 3099–3104. [Google Scholar] [CrossRef] [PubMed]
- Robert, A.A.; Zamzami, M.M. Stroke in Saudi Arabia: A review of the recent literature. Pan. Afr. Med. J. 2014, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Basri, R.; Issrani, R.; Hua Gan, S.; Prabhu, N.; Khursheed Alam, M. Burden of stroke in the Kingdom of Saudi Arabia: A soaring epidemic. Saudi Pharm. J. 2021, 29, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Al-Senani, F.; Salawati, M.; AlJohani, M.; Cuche, M.; Ravest, V.S.; Eggington, S. Workforce requirements for comprehensive ischaemic stroke care in a developing country: The case of Saudi Arabia. Hum. Resour. Health 2019, 17, 90. [Google Scholar] [CrossRef] [PubMed]
- Babkair, L.A.; Chyun, D.; Dickson, V.V.; Almekhlafi, M.A. The Effect of Psychosocial Factors and Functional Independence on Poststroke Depressive Symptoms: A Cross-Sectional Study. J. Nurs. Res. 2021, 30, e189. [Google Scholar] [CrossRef]
- Fulk, G.; Duncan, P.; Klingman, K.J. Sleep problems worsen health-related quality of life and participation during the first 12 months of stroke rehabilitation. Clin. Rehabil. 2020, 34, 1400–1408. [Google Scholar] [CrossRef]
- He, W.; Ruan, Y. Poor sleep quality, vitamin D deficiency and depression in the stroke population: A cohort study. J. Affect. Disord. 2022, 308, 199–204. [Google Scholar] [CrossRef]
- Ho, L.Y.W.; Lai, C.K.Y.; Ng, S.S.M. Contribution of sleep quality to fatigue following a stroke: A cross-sectional study. BMC Neurol. 2021, 21, 151. [Google Scholar] [CrossRef] [PubMed]
- Khazaei, S.; Ayubi, E.; Khazaei, M.; Khazaei, M.; Afrookhteh, G. Sleep Quality and Related Determinants among Stroke Patients: A Cross-Sectional Study. Iran. J. Psychiatry 2022, 17, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Babkair, L.A. Risk Factors for Poststroke Depression: An Integrative Review. J. Neurosci. Nurs. 2017, 49, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Thambirajah, N.; Senanayake, S.; Gooneratne, K.; Suraweera, C.; Ranasinghe, L.; Kumbukage, M. Post-Stroke Depression: Prevalence, Associated Factors, and Relationship to Disability in a Tertiary Care Center in Sri Lanka. J. Neurosci. Rural. Pract. 2022, 13, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Hu, B.; Liu, Q.; Wang, Y.; Zhao, Y.; Zhu, X. Social support and sleep quality in patients with stroke: The mediating roles of depression and anxiety symptoms. Int. J. Nurs. Pract. 2022, 28, e12939. [Google Scholar] [CrossRef] [PubMed]
- APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR, 5th ed.; American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- Kavga, A.; Kalemikerakis, I.; Faros, A.; Milaka, M.; Tsekoura, D.; Skoulatou, M.; Tsatsou, I.; Govina, O. The Effects of Patients’ and Caregivers’ Characteristics on the Burden of Families Caring for Stroke Survivors. Int. J. Environ. Res. Public Health 2021, 18, 7298. [Google Scholar] [CrossRef] [PubMed]
- Byun, E.; Evans, L.; Sommers, M.; Tkacs, N.; Riegel, B. Depressive symptoms in caregivers immediately after stroke. Top. Stroke Rehabil. 2019, 26, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Mahalle, S.; Yahya, N.; Zailani, F.F. Psychological Issues on Family Caregivers of Stroke Patients in Brunei Darussalam: In the Era of Pandemic COVID-19. Educ. Q. Rev. 2022, 5, 299–305. Available online: https://www.asianinstituteofresearch.org/EQRarchives/Psychological-Issues-on-Family-Caregivers-of-Stroke-Patients-in-Brunei-Darussalam%3A-In-the-Era-of-Pandemic-Covid-19 (accessed on 25 February 2023). [CrossRef]
- Adegbohun, A.; Uwakwe, R.; Ii, A.; Fi, O. The Quality of Sleep, Burden of Care and Psychological Distress in Caregivers of Patients with Stroke. Int. J. Ment. Health Psychiatry 2017, 3, 104172. Available online: https://www.scitechnol.com/peer-review/the-quality-of-sleep-burden-of-care-and-psychological-distress-in-caregivers-of-patients-with-stroke-82GC.php?article_id=6715 (accessed on 24 February 2023).
- Teixeira, F.; Moura, A.; Alves, E. Decline in duration, satisfaction and sleep quality among informal caregivers of stroke survivors, 18-months post-stroke. Int. J. Epidemiol. 2021, 50 (Suppl. S1), dyab168.653. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Patient Health Questionnaire Primary Care Study Group. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Al Zaid, K.; Al Faris, E. Screening for Somatization and Depression in Saudi Arabia: A Validation Study of the Phq in Primary Care. Int. J. Psychiatry Med. 2002, 32, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Jerković, A.; Mikac, U.; Matijaca, M.; Košta, V.; Katić, A.; Dolić, K.; Vujović, I.; Šoda, J.; Đogaš, Z.; Pavelin, S.; et al. Psychometric Properties of the Pittsburgh Sleep Quality Index (PSQI) in Patients with Multiple Sclerosis: Factor Structure, Reliability, Correlates, and Discrimination. J. Clin. Med. 2022, 11, 2037. [Google Scholar] [CrossRef]
- Suleiman, K.; Hadid, L.; Duhni, A. Psychometric Testing of the Arabic version of the Pittsburgh Sleep Quality Index (A-PSQI) among Coronary Artery Disease Patients in Jordan. J. Nat. Sci. Res. 2012, 2, 15–19. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Publishers: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Silva, L.C.; Silva, A.; Rangel, M.F.D.A.; Caetano, L.C.G.; Teixeira-Salmela, L.F.; Scianni, A.A. Depressive symptoms and functional status are associated with sleep quality after stroke. Top. Stroke Rehabil. 2021, 28, 573–580. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Patients N = 100 N (%) | Caregivers N = 80 N (%) | |
|---|---|---|---|
| Sex | Male | 59 (59) | 35 (43.8) |
| Female | 41 (41) | 45 (46.3) | |
| Nationality | Saudi | 89 (89) | 69 (86.3) |
| Non-Saudi | 11 (11) | 11(13.8) | |
| Marital Status | Married | 66 (66) | 49 (61.3) |
| Single | 11 (11) | 25 (31.3) | |
| Widowed | 13 (13) | 3 (3.8) | |
| Divorced | 10 (10) | 3 (3.8) | |
| Education | Elementary school | 16 (16) | 2 (2.5) |
| Middle school | 17 (17) | 3 (3.8) | |
| High school | 35 (35) | 20 (25) | |
| University | 16 (16) | 46 (57.5) | |
| Higher degree | 3 (3) | 5 (6.3) | |
| Other | 13 (13) | 4 (5) | |
| Employment | Employed | 26 (26) | 46 (57.5) |
| Unemployed | 16 (16) | 10 (12.5) | |
| Retired | 26 (26) | 10 (12.5) | |
| Housewife | 32 (32) | 14 (17.5) | |
| Monthly salary (Saudi riyal) | <2000 | 19 (19) | 5 (6.3) |
| 2000–5000 | 17 (17) | 19 (23.8) | |
| 5000–10,000 | 14 (14) | 22 (27.5) | |
| >10,000 | 13 (13) | 18 (22.5) | |
| Do not know | 37 (37) | 16 (20) | |
| City | Jeddah | 92 (92) | 72 (90) |
| Makkah | 3 (3) | - | |
| Other | 5 (5) | 8 (10) | |
| Relation to patient | Father | - | 27 (33.8) |
| Mother | - | 29 (36.3) | |
| Spouse | - | 12 (15) | |
| Sibling | - | 7 (8.8) | |
| Other | - | 5 (6.3) | |
| Hospital | KFGH | 55 (55) | - |
| KAMC | 45 (45) | - | |
| Stroke duration | <Year | 30 (30) | - |
| One year | 26 (26) | - | |
| >Year | 44 (44) | - | |
| Characteristics | Patients N = 100 N (%) | Caregivers N = 80 N (%) |
|---|---|---|
| Diabetes Mellitus | 60 (60) | 13 (16.3) |
| Hypertension | 65 (65) | 20 (25) |
| Heart disease | 16 (16) | 7 (8.8) |
| Kidney disease | 6 (6) | 1 (1.3) |
| Hyperlipidemia | 35 (35) | 9 (11.3) |
| Obesity | 8 (8) | 2 (2.5) |
| Smoking | 16 (16) | 15 (18.8) |
| History of stroke | 18 (18) | - |
| Other | 7 (7) | 4 (5) |
| Patient N (%) | Caregiver N (%) | ||
|---|---|---|---|
| PHQ-9 severity | 0–4 None | 27 (27) | 29 (36.3) |
| 5–9 Mild | 23 (23) | 28 (35) | |
| 10–14 Moderate | 30 (30) | 13 (16.3) | |
| 15–19 Moderately Severe | 14 (14) | 10 (12.5) | |
| 20–27 Severe | 6 (6) | 0 | |
| Patient | Caregiver | |||||||
|---|---|---|---|---|---|---|---|---|
| Minimum | Maximum | Mean | SD | Minimum | Maximum | Mean | SD | |
| PSQI | 0 | 17 | 7.85 | 3.622 | 0 | 14 | 6.16 | 3.046 |
| PHQ-9 | 0 | 23 | 9.56 | 5.823 | 0 | 19 | 6.96 | 4.753 |
| Score | Patient N (%) | Caregivers N (%) | |
|---|---|---|---|
| PHQ-9 | ≥10 | 43 (43) | 17 (21.3) |
| <10 | 57 (57) | 63 (78.8) | |
| PQSI | >5 | 65 (65) | 37 (46.3) |
| <5 | 35 (35) | 42 (52.5) |
| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| 1—PHQ-9 for patient | - | |||
| 2—PSQI for patient | 0.885 ** | - | ||
| 3—PHQ-9 for caregivers | 0.502 ** | 0.492 ** | - | |
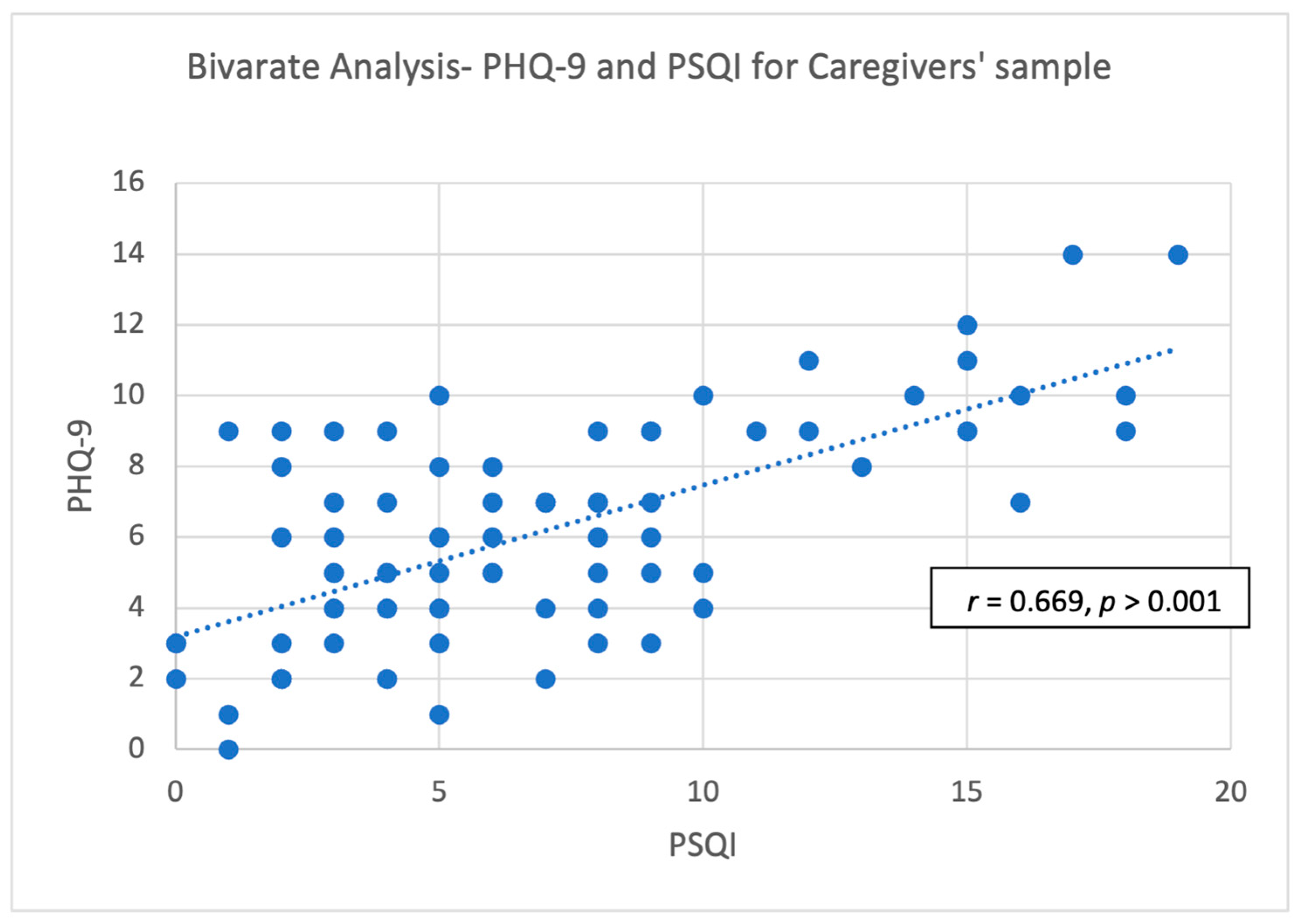
| 4—PSQI for caregivers | 0.456 ** | 0.407 ** | 0.669 ** | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babkair, L.A.; Huri, H.; Alharbi, W.; Turkistani, Y.; Alaslani, R.; Alandijani, N.; Hakami, F.H. The Association between Sleep Quality and Depressive Symptoms among Stroke Survivors and Caregivers. Healthcare 2024, 12, 58. https://doi.org/10.3390/healthcare12010058
Babkair LA, Huri H, Alharbi W, Turkistani Y, Alaslani R, Alandijani N, Hakami FH. The Association between Sleep Quality and Depressive Symptoms among Stroke Survivors and Caregivers. Healthcare. 2024; 12(1):58. https://doi.org/10.3390/healthcare12010058
Chicago/Turabian StyleBabkair, Lisa A., Hanadi Huri, Walaa Alharbi, Yara Turkistani, Ruba Alaslani, Nisreen Alandijani, and Fatimah Hamad Hakami. 2024. "The Association between Sleep Quality and Depressive Symptoms among Stroke Survivors and Caregivers" Healthcare 12, no. 1: 58. https://doi.org/10.3390/healthcare12010058