
Group Belonging and Social Identities in the Transition of Asylum-Seekers in Greece: Longitudinal Pathways to Adjustment

Abstract
:1. Introduction
1.1. Social Identity Approach to Health and SIMIC
1.2. SIMIC and Forced Migration
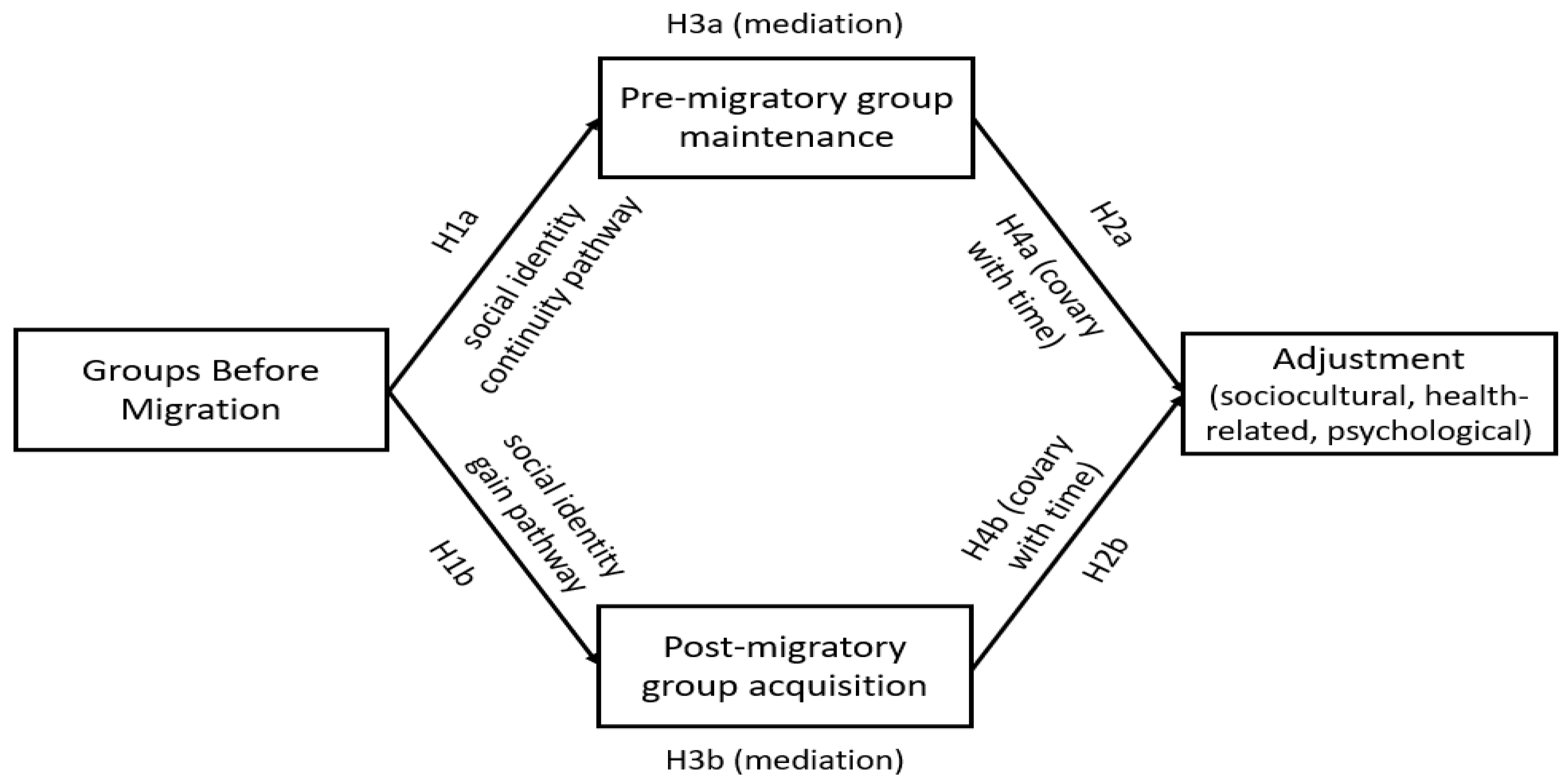
1.3. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Materials
2.3.1. Social Identity Measures
2.3.2. Sociocultural Adjustment
2.3.3. Health-Related Adjustment
2.3.4. Psychological Adjustment
2.4. Statistical Analyses
3. Results
3.1. Preliminary Analyses
3.2. Main Analyses
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations High Commissioner for Refugees. Refugee Population Statistics Database. 2023. Available online: https://www.unhcr.org/refugee-statistics/download (accessed on 1 November 2023).
- Danish Refugee Council. Global Displacement Forecast 2023: Using Data Modelling to Predict Displacement Crises. 2023. Available online: https://tinyurl.com/v3ym8n2c (accessed on 1 November 2023).
- Bogic, M.; Njoku, A.; Priebe, S. Long-term mental health of war-refugees: A systematic literature review. BMC Int. Health Hum. Rights 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R.A.; Van Ommeren, M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. JAMA 2009, 302, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Walther, L.; Fuchs, L.M.; Schupp, J.; Von Scheve, C. Living conditions and the mental health and well-being of refugees: Evidence from a large-scale German survey. J. Immigr. Minor. Health 2020, 22, 903–913. [Google Scholar] [CrossRef]
- Bakker, L.; Dagevos, J.; Engbersen, G. The importance of resources and security in the socio-economic integration of refugees. A study on the impact of length of stay in asylum accommodation and residence status on socio-economic integration for the four largest refugee groups in the Netherlands. J. Int. Migr. Integr. 2014, 15, 431–448. [Google Scholar] [CrossRef]
- Hvidtfeldt, C.; Petersen, J.H.; Norredam, M. Waiting for family reunification and the risk of mental disorders among refugee fathers: A 24-year longitudinal cohort study from Denmark. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 1061–1072. [Google Scholar] [CrossRef] [PubMed]
- Wicki, B.; Spiller, T.R.; Schick, M.; Schnyder, U.; Bryant, R.A.; Nickerson, A.; Morina, N. A network analysis of postmigration living difficulties in refugees and asylum seekers. Eur. J. Psychotraumatol. 2021, 12, 1975941. [Google Scholar] [CrossRef]
- Graef-Calliess, I.T.; Erdmann, L.; Mohwinkel, V.; Özkan, I.; Finkelstein, D.; Loos, K.; Penteker, G.; Trilesnik, B. Post-migration living difficulties, discrimination, and mental health of traumatized refugees in Germany: Data from the refuKey project for timely and need-adapted treatment in a stepped-care setting. Int. Rev. Psychiatry 2023, 35, 339–351. [Google Scholar] [CrossRef]
- Campbell, M.R.; Mann, K.D.; Moffatt, S.; Dave, M.; Pearce, M.S. Social determinants of emotional well-being in new refugees in the UK. Public Health 2018, 164, 72–81. [Google Scholar] [CrossRef]
- Berry, J.W.; Hou, F. Immigrant acculturation and wellbeing in Canada. Can. Psychol./Psychol. Can. 2016, 57, 254–264. [Google Scholar] [CrossRef]
- Buchanan, Z.E.; Abu-Rayya, H.M.; Kashima, E.; Paxton, S.J.; Sam, D.L. Perceived discrimination, language proficiencies, and adaptation: Comparisons between refugee and non-refugee immigrant youth in Australia. Int. J. Intercult. Relat. 2018, 63, 105–112. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Fabreau, G.E.; Raghavan, S.; Kentoffio, K.; Chang, Y.; He, W.; Atlas, S.J.; Percac-Lima, S. Risk of developing diabetes among refugees and immigrants: A longitudinal analysis. J. Community Health 2016, 41, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Reed, H.E.; Barbosa, G.Y. Investigating the refugee health disadvantage among the US immigrant population. J. Immigr. Refug. Stud. 2017, 15, 53–70. [Google Scholar] [CrossRef]
- Nakhaie, R. Language proficiency and sociocultural integration of Canadian newcomers. Appl. Psycholinguist. 2020, 41, 1437–1464. [Google Scholar] [CrossRef]
- Li, S.S.; Liddell, B.J.; Nickerson, A. The relationship between post-migration stress and psychological disorders in refugees and asylum seekers. Curr. Psychiatry Rep. 2016, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Albarosa, E.; Elsner, B. Forced Migration, Social Cohesion and Conflict: The 2015 Refugee Inflow in Germany. (World Bank Group). 2022. Available online: https://tinyurl.com/55fyy8zf (accessed on 1 November 2023).
- Haslam, C.; Haslam, S.A.; Jetten, J.; Cruwys, T.; Steffens, N.K. Life change, social identity, and health. Annu. Rev. Psychol. 2021, 72, 635–661. [Google Scholar] [CrossRef]
- Jetten, J.; Haslam, S.A.; Cruwys, T.; Greenaway, K.H.; Haslam, C.; Steffens, N.K. Advancing the social identity approach to health and well-being: Progressing the social cure research agenda. Eur. J. Soc. Psychol. 2017, 47, 789–802. [Google Scholar] [CrossRef]
- Greenaway, K.H.; Cruwys, T.; Haslam, S.A.; Jetten, J. Social identities promote well-being because they satisfy global psychological needs. Eur. J. Soc. Psychol. 2016, 46, 294–307. [Google Scholar] [CrossRef]
- Haslam, S.A.; Reicher, S.D.; Levine, M. When other people are heaven, when other people are hell: How social identity determines the nature and impact of social support. In The Social Cure: Identity, Health and Well-Being; Jetten, J., Haslam, C., Haslam, S.A., Eds.; Psychology Press: Hove, UK, 2012; pp. 157–174. [Google Scholar]
- Iyer, A.; Jetten, J.; Tsivrikos, D.; Postmes, T.; Haslam, S.A. The more (and the more compatible) the merrier: Multiple group memberships and identity compatibility as predictors of adjustment after life transitions. Br. J. Soc. Psychol. 2009, 48, 707–733. [Google Scholar] [CrossRef]
- Haslam, C.; Holme, A.; Haslam, S.A.; Iyer, A.; Jetten, J.; Williams, W.H. Maintaining group memberships: Social identity continuity predicts well-being after stroke. Neuropsychol. Rehabil. 2008, 18, 671–691. [Google Scholar] [CrossRef]
- Haslam, C.; Lam, B.C.; Branscombe, N.R.; Steffens, N.K.; Haslam, S.A.; Cruwys, T.; Fong, P.; Ball, T.C. Adjusting to life in retirement: The protective role of new group memberships and identification as a retiree. Eur. J. Work Organ. Psychol. 2018, 27, 822–839. [Google Scholar] [CrossRef]
- Cruwys, T.; Ng, N.W.; Haslam, S.A.; Haslam, C. Identity continuity protects academic performance, retention, and life satisfaction among international students. Appl. Psychol. 2021, 70, 931–954. [Google Scholar] [CrossRef]
- Seymour-Smith, M.; Cruwys, T.; Haslam, S.A.; Brodribb, W. Loss of group memberships predicts depression in postpartum mothers. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Dingle, G.A.; Cruwys, T.; Frings, D. Social identities as pathways into and out of addiction. Front. Psychol. 2015, 6, 1795. [Google Scholar] [CrossRef] [PubMed]
- Cruwys, T.; Dingle, G.A.; Haslam, C.; Haslam, S.A.; Jetten, J.; Morton, T.A. Social group memberships protect against future depression, alleviate depression symptoms and prevent depression relapse. Soc. Sci. Med. 2013, 98, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Craig, N.; Haslam, C.; Jetten, J.; Cruwys, T. Group memberships and post-traumatic growth: How we connect determines how we recover. Soc. Sci. Med. 2022, 315, 115529. [Google Scholar] [CrossRef] [PubMed]
- Henrich, J.; Heine, S.J.; Norenzayan, A. The weirdest people in the world? Behav. Brain Sci. 2010, 33, 61–83. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.X.L.; Jetten, J.; Cruwys, T.; Haslam, C.; Praharso, N. The more (social group memberships), the merrier: Is this the case for Asians? Front. Psychol. 2016, 7, 1001. [Google Scholar] [CrossRef]
- Wakefield, J.R.; Bowe, M.; Kellezi, B.; McNamara, N.; Stevenson, C. When groups help and when groups harm: Origins, developments, and future directions of the “Social Cure” perspective of group dynamics. Soc. Personal. Psychol. Compass 2019, 13, e12440. [Google Scholar] [CrossRef]
- Smeekes, A.; Verkuyten, M.; Çelebi, E.; Acartürk, C.; Onkun, S. Social identity continuity and mental health among Syrian refugees in Turkey. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1317–1324. [Google Scholar] [CrossRef]
- Dimitriadi, A. Governing migrant (im)mobility in Greece after the EU-Turkey statement. In Challenging Mobilities in and to the EU during Times of Crises: The Case of Greece; IMISCOE Research Series; Kousis, M., Chatzidaki, A., Kafetsios, K., Eds.; Springer: Cham, Switzerland, 2022; pp. 221–239. [Google Scholar] [CrossRef]
- Prodromidou, A.; Ververidou, F. From transit country to destination: The road to refugee and asylum seekers’ integration in Greece. In Policy and Politics of the Syrian Refugee Crisis in Eastern Mediterranean States: National and Institutional Perspectives; Stephenson, M.O., Jr., Stivachtis, Y.A., Eds.; E-International Relations Publishing: Bristol, UK, 2023; pp. 197–220. [Google Scholar]
- Nguyen, A.M.D.; Benet-Martínez, V. Biculturalism and adjustment: A meta-analysis. J. Cross-Cult. Psychol. 2013, 44, 122–159. [Google Scholar] [CrossRef]
- Maas, C.J.M.; Hox, J.J. Sufficient sample sizes for multilevel modeling. Methodology 2005, 1, 86–92. [Google Scholar] [CrossRef]
- Besevegis, E.; Pavlopoulos, V. Acculturation patterns and adaptation of immigrants in Greece. In Psychosocial Stress in Immigrants and Members of Minority Groups as a Factor of Terrorist Behavior; NATO Science for Peace and Security Series-E: Human and Societal Dynamics; Finklestein, M., Dent-Brown, K., Eds.; IOS Press: Amsterdam, The Netherlands, 2008; Volume 40, pp. 23–34. [Google Scholar] [CrossRef]
- Wilson, J.; Ward, C.; Fetvadjiev, V.H.; Bethel, A. Measuring cultural competencies: The development and validation of a revised measure of sociocultural adaptation. J. Cross-Cult. Psychol. 2017, 48, 1475–1506. [Google Scholar] [CrossRef]
- WHOQOL Group. Development of the World Health Organization WHOQOL-BREF Quality of Life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef]
- World Health Organization. French WHOQOL-BREF. 2020. Available online: https://tinyurl.com/2p9xt8jp (accessed on 1 November 2023).
- Schmalbach, B.; Zenger, M.; Tibubos, A.N.; Kliem, S.; Petrowski, K.; Brähler, E. Psychometric properties of two brief versions of the Hopkins Symptom Checklist: HSCL-5 and HSCL-10. Assessment 2019, 28, 617–631. [Google Scholar] [CrossRef] [PubMed]
- Le Bris, T. The Hopkins Symptoms Checklist in 25 Items: Translations in Castilian, Galician, Catalan, French, Greek, Italian, Polish, Bulgarian and Croatian Synthesis. Ph.D. Thesis, University of Western Brittany, Brest, France, 2017. Available online: https://dumas.ccsd.cnrs.fr/dumas-01537933 (accessed on 1 November 2023).
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Blais, M.R.; Vallerand, R.J.; Pelletier, L.G.; Brière, N.M. L’échelle de satisfaction de vie: Validation canadienne-française du “Satisfaction with Life Scale” [The satisfaction scale: Canadian-French validation of the Satisfaction with Life Scale]. Can. J. Behav. Sci./Rev. Can. Sci. Comport. 1989, 21, 210–223. [Google Scholar] [CrossRef]
- Zhang, Z.; Zyphur, M.J.; Preacher, K.J. Testing multilevel mediation using hierarchical linear models: Problems and solutions. Organ. Res. Methods 2009, 12, 695–719. [Google Scholar] [CrossRef]
- McNeish, D.M.; Stapleton, L.M. The effect of small sample size on two-level model estimates: A review and illustration. Educ. Psychol. Rev. 2016, 28, 295–314. [Google Scholar] [CrossRef]
- Rockwood, N.J. Advancing the Formulation and Testing of Multilevel Mediation and Moderated Mediation Models. Master’s Thesis, Ohio State University, Columbus, OH, USA, 2017. Available online: http://rave.ohiolink.edu/etdc/view?acc_num=osu1489578419777238 (accessed on 1 November 2023).
- Rockwood, N.J.; Hayes, A.F. Multilevel mediation analysis. In Multilevel Modeling Methods with Introductory and Advanced Applications; O’Connell, A.A., McCoach, D.B., Bell, B.A., Eds.; Information Age Publishing: Charlotte, NC, USA, 2022; pp. 567–597. [Google Scholar]
- Bauer, D.J.; Preacher, K.J.; Gil, K.M. Conceptualizing and testing random indirect effects and moderated mediation in multilevel models: New procedures and recommendations. Psychol. Methods 2006, 11, 142–163. [Google Scholar] [CrossRef]
- Preacher, K.J.; Selig, J.P. Advantages of Monte Carlo confidence intervals for indirect effects. Commun. Methods Meas. 2012, 6, 77–98. [Google Scholar] [CrossRef]
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 7th ed.; Pearson: New York, NY, USA, 2019. [Google Scholar]
- Mowbray, F.I.; Fox-Wasylyshyn, S.M.; El-Masri, M.M. Univariate outliers: A conceptual overview for the nurse researcher. Can. J. Nurs. Res. 2019, 51, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Lorah, J. Effect size measures for multilevel models: Definition, interpretation, and TIMSS example. Large-Scale Assess. Educ. 2018, 6, 8. [Google Scholar] [CrossRef]
- Çelebi, E.; Verkuyten, M.; Bagci, S.C. Ethnic identification, discrimination, and mental and physical health among Syrian refugees: The moderating role of identity needs. Eur. J. Soc. Psychol. 2017, 47, 832–843. [Google Scholar] [CrossRef]
- Hagstrom, P.; Pereira, J.; Wu, S. The happiness of refugees in the United States: Evidence from Utica, NY. J. Refug. Stud. 2021, 34, 614–633. [Google Scholar] [CrossRef]
- Schweitzer, R.; Melville, F.; Steel, Z.; Lacherez, P. Trauma, post-migration living difficulties, and social support as predictors of psychological adjustment in resettled Sudanese refugees. Aust. N. Z. J. Psychiatry 2006, 40, 179–187. [Google Scholar] [CrossRef]
- Muldoon, O.T.; Haslam, S.A.; Haslam, C.; Cruwys, T.; Kearns, M.; Jetten, J. The social psychology of responses to trauma: Social identity pathways associated with divergent traumatic responses. Eur. Rev. Soc. Psychol. 2019, 30, 311–348. [Google Scholar] [CrossRef]
- Fogden, G.; Berle, D.; Steel, Z. The impact of family separation and worry about family on psychological adjustment in refugees resettled in Australia. J. Trauma. Stress 2020, 33, 894–907. [Google Scholar] [CrossRef]
- Nickerson, A.; Bryant, R.A.; Steel, Z.; Silove, D.; Brooks, R. The impact of fear for family on mental health in a resettled Iraqi refugee community. J. Psychiatr. Res. 2010, 44, 229–235. [Google Scholar] [CrossRef]
- Bobowik, M.; Martinovic, B.; Basabe, N.; Barsties, L.S.; Wachter, G. ‘Healthy’ identities? Revisiting rejection-identification and rejection-disidentification models among voluntary and forced immigrants. Eur. J. Soc. Psychol. 2017, 47, 818–831. [Google Scholar] [CrossRef]
- Haindorfer, R.; Liedl, B.; Kittel, B. The integration resources of refugees and life satisfaction: Evidence from the city of Vienna. J. Immigr. Refug. Stud. 2022. [CrossRef]
- Tajfel, H.; Turner, J.C. An integrative theory of intergroup conflict. In The Social Psychology of Intergroup Relations; Austin, W.G., Worchel, S., Eds.; Brooks/Cole: Monterey, CA, USA, 1979; pp. 33–48. [Google Scholar]
- Alfadhli, K.; Güler, M.; Cakal, H.; Drury, J. The role of emergent shared identity in psychosocial support among refugees of conflict in developing countries. Int. Rev. Soc. Psychol. 2019, 32, 2. [Google Scholar] [CrossRef]
- El Khoury, S.J. Factors that impact the sociocultural adjustment and well-being of Syrian refugees in Stuttgart–Germany. Br. J. Guid. Couns. 2019, 47, 65–80. [Google Scholar] [CrossRef]
- Ward, C.; Kennedy, A. Acculturation strategies, psychological adjustment, and sociocultural competence during cross-cultural transitions. Int. J. Intercult. Relat. 1994, 18, 329–343. [Google Scholar] [CrossRef]
- Sønderlund, A.L.; Morton, T.A.; Ryan, M.K. Multiple group membership and well-being: Is there always strength in numbers? Front. Psychol. 2017, 8, 1038. [Google Scholar] [CrossRef]
- Kyprianides, A.; Easterbrook, M.J.; Cruwys, T. “I changed and hid my old ways”: How social rejection and social identities shape well-being among ex-prisoners. J. Appl. Soc. Psychol. 2019, 49, 283–294. [Google Scholar] [CrossRef]
- Belloni, M. When the phone stops ringing: On the meanings and causes of disruptions in communication between Eritrean refugees and their families back home. Glob. Netw. 2020, 20, 256–273. [Google Scholar] [CrossRef]
- Kellezi, B.; Bowe, M.; Wakefield, J.R.; McNamara, N.; Bosworth, M. Understanding and coping with immigration detention: Social identity as cure and curse. Eur. J. Soc. Psychol. 2019, 49, 333–351. [Google Scholar] [CrossRef]
- Steffens, N.K.; LaRue, C.J.; Haslam, C.; Walter, Z.C.; Cruwys, T.; Munt, K.A.; Haslam, S.A.; Jetten, J.; Tarrant, M. Social identification-building interventions to improve health: A systematic review and meta-analysis. Health Psychol. Rev. 2021, 15, 85–112. [Google Scholar] [CrossRef]
- Phinney, J.S.; Jacoby, B.; Silva, C. Positive intergroup attitudes: The role of ethnic identity. Int. J. Behav. Dev. 2007, 31, 478–490. [Google Scholar] [CrossRef]
- Jetten, J.; Branscombe, N.R.; Haslam, S.A.; Haslam, C.; Cruwys, T.; Jones, J.M.; Cui, L.; Dingle, G.; Liu, J.; Murphy, S.; et al. Having a lot of a good thing: Multiple important group memberships as a source of self-esteem. PLoS ONE 2015, 10, e0124609. [Google Scholar] [CrossRef]
- Lam, B.C.; Haslam, C.; Haslam, S.A.; Steffens, N.K.; Cruwys, T.; Jetten, J.; Yang, J. Multiple social groups support adjustment to retirement across cultures. Soc. Sci. Med. 2018, 208, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Salo, C.D.; Birman, D. Acculturation and psychological adjustment of Vietnamese refugees: An ecological acculturation framework. Am. J. Community Psychol. 2015, 56, 395–407. [Google Scholar] [CrossRef]
- Wassermann, M.; Fujishiro, K.; Hoppe, A. The effect of perceived overqualification on job satisfaction and career satisfaction among immigrants: Does host national identity matter? Int. J. Intercult. Relat. 2017, 61, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Vinokurov, A.; Birman, D.; Trickett, E. Psychological and acculturation correlates of work status among Soviet Jewish refugees in the United States. Int. Migr. Rev. 2000, 34, 538–559. [Google Scholar] [CrossRef]
- Sani, F.; Herrera, M.; Wakefield, J.R.; Boroch, O.; Gulyas, C. Comparing social contact and group identification as predictors of mental health. Br. J. Soc. Psychol. 2012, 51, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Robertson, Z.; Wilding, R.; Gifford, S. Mediating the family imaginary: Young people negotiating absence in transnational refugee families. Glob. Netw. 2016, 16, 219–236. [Google Scholar] [CrossRef]
- Haslam, C.; Cruwys, T.; Haslam, S.A.; Dingle, G.; Chang, M.X.L. Groups 4 Health: Evidence that a social-identity intervention that builds and strengthens social group membership improves mental health. J. Affect. Disord. 2016, 194, 188–195. [Google Scholar] [CrossRef]
- Haslam, C.; Cruwys, T.; Chang, M.X.L.; Bentley, S.V.; Haslam, S.A.; Dingle, G.A.; Jetten, J. GROUPS 4 HEALTH reduces loneliness and social anxiety in adults with psychological distress: Findings from a randomized controlled trial. J Consult. Clin. Psychol. 2019, 87, 787–801. [Google Scholar] [CrossRef]
- McNeish, D. Multilevel mediation with small samples: A cautionary note on the multilevel structural equation modeling framework. Struct. Equ. Model. Multidiscip. J. 2017, 24, 609–625. [Google Scholar] [CrossRef]
- Oppong, C. Familial roles and social transformations: Older men and women in sub-Saharan Africa. Res. Aging 2006, 28, 654–668. [Google Scholar] [CrossRef]
- Rohrer, J.M.; Murayama, K. These are not the effects you are looking for: Causality and the within-/between-persons distinction in longitudinal data analysis. Adv. Methods Pract. Psychol. Sci. 2023, 6, 25152459221140842. [Google Scholar] [CrossRef]


{kind=link}
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. GBM T1 | - | ||||||||||||||||||||
| 2. GBM T2 | 0.53 ** | - | |||||||||||||||||||
| 3. GBM T3 | 0.47 ** | 0.35 ** | - | ||||||||||||||||||
| 4. GM T1 | 0.52 ** | 0.28 * | 0.30 * | - | |||||||||||||||||
| 5. GM T2 | 0.25 | 0.40 * | 0.06 | 0.51 ** | - | ||||||||||||||||
| 6. GM T3 | 0.28 * | 0.14 | 0.32 * | 0.64 ** | 0.49 ** | - | |||||||||||||||
| 7. GA T1 | 0.63 ** | 0.29 * | 0.43 ** | 0.58 ** | 0.25 | 0.52 ** | - | ||||||||||||||
| 8. GA T2 | 0.38 ** | 0.59 ** | 0.30 * | 0.31 * | 0.47 ** | 0.36 ** | 0.48 ** | - | |||||||||||||
| 9. GA T3 | 0.37 ** | 0.15 | 0.49 ** | 0.50 ** | 0.33 * | 0.61 ** | 0.53 ** | 0.47 ** | - | ||||||||||||
| 10. SA T1 | 0.56 ** | 0.47 ** | 0.36 ** | 0.62 ** | 0.39 ** | 0.37 ** | 0.51 ** | 0.41 ** | 0.38 ** | - | |||||||||||
| 11. SA T2 | 0.27 * | 0.59 ** | 0.17 | 0.31 * | 0.52 ** | 0.28 * | 0.27 * | 0.69 ** | 0.25 | 0.59 ** | - | ||||||||||
| 12. SA T3 | 0.24 | 0.27 * | 0.41 ** | 0.35 ** | 0.21 | 0.51 ** | 0.44 ** | 0.52 ** | 0.46 ** | 0.56 ** | 0.54 ** | - | |||||||||
| 13. HA T1 | 0.18 | 0.18 | −0.02 | 0.42 ** | 0.25 | 0.38 ** | 0.41 ** | 0.21 | 0.25 | 0.34 ** | 0.14 | 0.31 * | - | ||||||||
| 14. HA T2 | 0.14 | 0.39 * | 0.16 | 0.36 ** | 0.63 ** | 0.44 ** | 0.23 | 0.43 ** | 0.30 * | 0.28 * | 0.39 ** | 0.19 | 0.52 ** | - | |||||||
| 15. HA T3 | 0.08 | 0.10 | 0.17 | 0.23 | 0.35 ** | 0.36 ** | 0.33 ** | 0.27 * | 0.41 ** | 0.16 | 0.13 | 0.19 | 0.47 ** | 0.55 ** | - | ||||||
| 16. PD T1 | 0.01 | 0.02 | 0.26 * | −0.19 | −0.32 * | −0.36 ** | −0.02 | −0.13 | −0.09 | −0.05 | −0.15 | −0.15 | −0.40 ** | −0.29 | −0.14 | - | |||||
| 17. PD T2 | 0.06 | 0.00 | 0.04 | −0.16 | −0.20 | −0.20 | −0.09 | −0.32 * | −0.16 | −0.14 | −0.14 | −0.33 * | −0.47 ** | −0.41 ** | −0.45 * | 0.43 ** | - | ||||
| 18. PD T3 | −0.13 | 0.02 | 0.19 | −0.22 | −0.34 ** | −0.36 ** | −0.20 | −0.18 | −0.17 | −0.08 | −0.17 | −0.17 | −0.37 ** | −0.42 ** | −0.52 ** | 0.57 ** | 0.46 ** | - | |||
| 19. LS T1 | 0.39 ** | 0.19 | 0.07 | 0.51 ** | 0.29 * | 0.30 * | 0.52 ** | 0.44 ** | 0.39 ** | 0.45 ** | 0.38 ** | 0.27 * | 0.58 ** | 0.38 ** | 0.32 * | −0.36 ** | −0.36 ** | −0.41 ** | - | ||
| 20. LS T2 | 0.33 * | 0.42 ** | 0.09 | 0.45 ** | 0.67 ** | 0.35 ** | 0.43 ** | 0.62 ** | 0.37 ** | 0.42 ** | 0.58 ** | 0.29 * | 0.23 | 0.50 ** | 0.23 | −0.23 * | −0.20 | −0.31 * | 0.56 ** | - | |
| 21. LS T3 | 0.39 ** | 0.22 | 0.27 * | 0.51 ** | 0.39 ** | 0.48 ** | 0.49 ** | 0.42 ** | 0.60 ** | 0.37 ** | 0.34 ** | 0.40 ** | 0.38 ** | 0.36 ** | 0.40 ** | −0.38 ** | −0.36 ** | −0.49 ** | 0.57 ** | 0.39 ** | - |
| Predictor | β | SE | 95% CI (LL, UL) | p | |
|---|---|---|---|---|---|
| Fixed Effects | |||||
| Outcome: Group Maintenance | |||||
| Intercept | 1.981 | 1.462 | −0.950 | 4.912 | 0.181 |
| Groups Before | 0.445 | 0.131 | 0.182 | 0.708 | 0.001 |
| Outcome: Group Acquisition | |||||
| Intercept | 0.611 | 1.481 | −2.357 | 3.580 | 0.681 |
| Groups Before | 0.733 | 0.133 | 0.467 | 0.999 | <0.001 |
| Predictor | β | SE | 95% CI (LL, UL) | p | ||
|---|---|---|---|---|---|---|
| Sociocultural Adjustment | Fixed Effects | |||||
| Intercept | 2.997 | 1.060 | 0.871 | 5.123 | 0.007 | |
| Groups Before | 0.207 | 0.117 | −0.027 | 0.441 | 0.081 | |
| Between-Person Group Maintenance | 0.210 | 0.115 | −0.020 | 0.441 | 0.073 | |
| Within-Person Group Maintenance | 0.399 | 0.071 | 0.259 | 0.539 | <0.001 | |
| Between-Person Group Acquisition | 0.246 | 0.113 | 0.018 | 0.473 | 0.035 | |
| Within-Person Group Acquisition | 0.108 | 0.056 | −0.003 | 0.219 | 0.057 | |
| Health-Related Adjustment | Fixed Effects | |||||
| Intercept | 4.356 | 0.970 | 2.411 | 6.302 | <0.001 | |
| Groups Before | −0.093 | 0.107 | −0.306 | 0.121 | 0.390 | |
| Between-Person Group Maintenance | 0.295 | 0.105 | 0.084 | 0.505 | 0.007 | |
| Within-Person Group Maintenance | 0.108 | 0.074 | −0.038 | 0.254 | 0.147 | |
| Between-Person Group Acquisition | 0.190 | 0.104 | −0.018 | 0.398 | 0.073 | |
| Within-Person Group Acquisition | 0.137 | 0.058 | 0.021 | 0.253 | 0.021 | |
| Psychological Distress | Fixed Effects | |||||
| Intercept | 4.440 | 1.161 | 2.112 | 6.769 | <0.001 | |
| Groups Before | 0.331 | 0.128 | 0.075 | 0.587 | 0.012 | |
| Between-Person Group Maintenance | −0.374 | 0.126 | −0.627 | −0.122 | 0.004 | |
| Within-Person Group Maintenance | 0.013 | 0.092 | −0.170 | 0.195 | 0.890 | |
| Between-Person Group Acquisition | −0.142 | 0.124 | −0.391 | 0.108 | 0.259 | |
| Within-Person Group Acquisition | −0.045 | 0.073 | −0.189 | 0.100 | 0.541 | |
| Life Satisfaction | Fixed Effects | |||||
| Intercept | 2.281 | 0.996 | 0.283 | 4.278 | 0.026 | |
| Groups Before | −0.083 | 0.110 | −0.302 | 0.137 | 0.454 | |
| Between-Person Group Maintenance | 0.274 | 0.108 | 0.058 | 0.491 | 0.014 | |
| Within-Person Group Maintenance | 0.246 | 0.086 | 0.077 | 0.416 | 0.005 | |
| Between-Person Group Acquisition | 0.432 | 0.107 | 0.218 | 0.646 | <0.001 | |
| Within-Person Group Acquisition | 0.164 | 0.068 | 0.030 | 0.299 | 0.017 | |
| Outcome | Indirect Effects | β | 95% MCCI | |
|---|---|---|---|---|
| LL | UL | |||
| Sociocultural Adjustment | Group Maintenance | 0.094 | −0.007 | 0.229 |
| Group Acquisition | 0.180 | 0.013 | 0.375 | |
| Health-Related Adjustment | Group Maintenance | 0.131 | 0.030 | 0.271 |
| Group Acquisition | 0.139 | −0.012 | 0.312 | |
| Psychological Distress | Group Maintenance | −0.166 | −0.339 | −0.043 |
| Group Acquisition | −0.104 | −0.299 | 0.072 | |
| Life Satisfaction | Group Maintenance | 0.122 | 0.022 | 0.261 |
| Group Acquisition | 0.317 | 0.140 | 0.532 | |
| Outcome | Between-Person (%) | Within-Person (%) | Total (%) |
|---|---|---|---|
| Sociocultural adjustment | 45.61 | 28.80 | 38.17 |
| Health-related adjustment | 36.01 | 7.59 | 21.48 |
| Psychological distress | 35.93 | 0.00 | 16.60 |
| Life satisfaction | 63.76 | 14.17 | 39.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panagiotopoulos, A.; Pavlopoulos, V. Group Belonging and Social Identities in the Transition of Asylum-Seekers in Greece: Longitudinal Pathways to Adjustment. Healthcare 2024, 12, 55. https://doi.org/10.3390/healthcare12010055
Panagiotopoulos A, Pavlopoulos V. Group Belonging and Social Identities in the Transition of Asylum-Seekers in Greece: Longitudinal Pathways to Adjustment. Healthcare. 2024; 12(1):55. https://doi.org/10.3390/healthcare12010055
Chicago/Turabian StylePanagiotopoulos, Angelos, and Vassilis Pavlopoulos. 2024. "Group Belonging and Social Identities in the Transition of Asylum-Seekers in Greece: Longitudinal Pathways to Adjustment" Healthcare 12, no. 1: 55. https://doi.org/10.3390/healthcare12010055