
Development of an Implementation Strategy Tailored to Deliver Evidence-Based and Person-Centred Nursing Care for Patients with Community-Acquired Pneumonia: An Intervention Mapping Approach


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. The Intervention Mapping Framework
3. Development of an Implementation Strategy
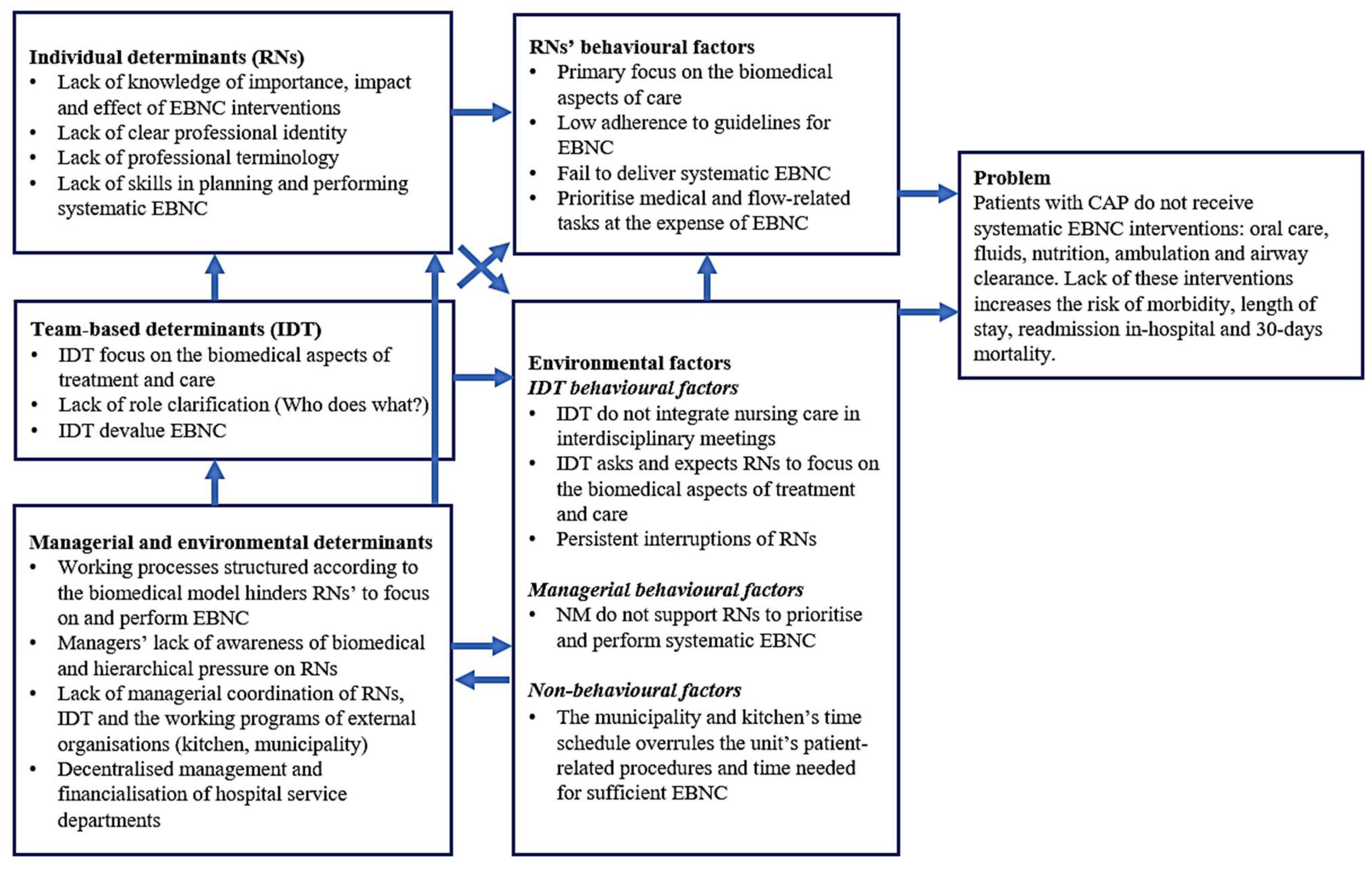
3.1. Step 1: Logic Model of the Problem (Needs Assessment)
3.1.1. Method
3.1.2. Results
Evidence-Based Nursing Care for CAP Patients and the Problem
Behavioural and Environmental Factors and Determinants Influencing Nursing Care
3.2. Step 2: Logic Model of Change
3.2.1. Method
3.2.2. Results
3.3. Step 3: Programme Design
3.3.1. Method
3.3.2. Results
3.4. Step 4: Programme Production
3.4.1. Method
3.4.2. Results
3.5. Step 5: Programme Implementation Plan
3.5.1. Method
3.5.2. Results
3.6. Step 6: Evaluation Plan
3.6.1. Method
3.6.2. Result
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ferreira-Coimbra, J.; Sarda, C.; Rello, J. Burden of Community-Acquired Pneumonia and Unmet Clinical Needs. Adv. Ther. 2020, 37, 1302–1318. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.E.; Myers, J.A.; Arnold, F.W.; Pass, L.A.; Ramirez, J.A.; Brock, G.N. Cost effectiveness of adherence to IDSA/ATS guidelines in elderly patients hospitalized for Community-Aquired Pneumonia. BMC Med. Inform. Decis. Mak. 2016, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Blasi, F.; Peetermans, W.E.; Viegi, G.; Welte, T. The aetiology and antibiotic management of community-acquired pneumonia in adults in Europe: A literature review. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1065–1079. [Google Scholar] [CrossRef] [PubMed]
- Khang, Y.H.; GBD 2016 Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef]
- Statistics Denmark. Admissions by Region, Diagnosis (99 Groups), Age and Sex. Denmark. Available online: http://www.statistikbanken.dk/statbank5a/default.asp?w=1684 (accessed on 1 November 2023).
- Søgaard, M.; Nielsen, R.B.; Schønheyder, H.C.; Nørgaard, M.; Thomsen, R.W. Nationwide trends in pneumonia hospitalization rates and mortality, Denmark 1997–2011. Respir. Med. 2014, 108, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Flachs, E.; Eriksen, L.; Koch, M. Sygdomsbyrden i Danmark—Sygdomme (The Burden of Disease in Denmark—Diseases); Sundhedsstyrelsen: Copenhagen, Denmark, 2015. [Google Scholar]
- Egelund, G.B.; Jensen, A.V.; Andersen, S.B.; Petersen, P.T.; Lindhardt, B.; von Plessen, C.; Rohde, G.; Ravn, P. Penicillin treatment for patients with Community-Acquired Pneumonia in Denmark: A retrospective cohort study. BMC Pulm. Med. 2017, 17, 66. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.; Arnold, D.M.; Bachanova, V.; Haspel, R.L.; Rosovsky, R.P.; Shustov, A.R.; Crowther, M.A. Evidence-based guidelines—An introduction. Hematol. Am. Soc. Hematol. Educ. Program 2008, 1, 26–30. [Google Scholar] [CrossRef]
- McCabe, C.; Kirchner, C.; Zhang, H.; Daley, J.; Fisman, D.N. Guideline concordant therapy and reduced mortality and length of stay in adults with community-acquired pneumonia: Playing by the rules. Arch. Intern. Med. 2009, 169, 1525–1531. [Google Scholar] [CrossRef]
- Arnold, F.W.; LaJoie, A.S.; Brock, G.N.; Peyrani, P.; Rello, J.; Menéndez, R.; Lopardo, G.; Torres, A.; Rossi, P.; Ramirez, J.A.; et al. Improving outcomes in elderly patients with community-acquired pneumonia by adhering to national guidelines: Community-Acquired Pneumonia Organization International cohort study results. Arch. Intern. Med. 2009, 169, 1515–1524. [Google Scholar] [CrossRef]
- Lindhardt, T.; Klausen, H.H.; Christiansen, C.; Smith, L.L.; Pedersen, J.; Andersen, O. Elderly patients with community-acquired pneumonia are not treated according to current guidelines. Dan. Med. J. 2013, 60, A4572. [Google Scholar]
- Komiya, K.; Rubin, B.K.; Kadota, J.I.; Mukae, H.; Akaba, T.; Moro, H.; Aoki, N.; Tsukada, H.; Noguchi, S.; Shime, N.; et al. Prognostic implications of aspiration pneumonia in patients with community acquired pneumonia: A systematic review with meta-analysis. Sci. Rep. 2016, 7, 38097. [Google Scholar] [CrossRef] [PubMed]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and Strategies in Guideline Implementation—A Scoping Review. Healthcare 2016, 4, 36. [Google Scholar] [CrossRef]
- Braithwaite, J.; Glasziou, P.; Westbrook, J. The three numbers you need to know about healthcare: The 60-30-10 Challenge. BMC Med. 2020, 18, 102. [Google Scholar] [CrossRef]
- Chaboyer, W.; Harbeck, E.; Lee, B.O.; Grealish, L. Missed nursing care: An overview of reviews. Kaohsiung J. Med. Sci. 2021, 37, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.; Recio-Saucedo, A.; Dall’Ora, C.; Briggs, J.; Maruotti, A.; Meredith, P.; Smith, G.B.; Ball, J. The association between nurse staffing and omissions in nursing care: A systematic review. J. Adv. Nurs. 2018, 74, 1474–1487. [Google Scholar] [CrossRef] [PubMed]
- Ball, J.E.; Bruyneel, L.; Aiken, L.H.; Sermeus, W.; Sloane, D.M.; Rafferty, A.M.; Lindqvist, R.; Tishelman, C.; Griffiths, P. Post-operative mortality, missed care and nurse staffing in nine countries: A cross-sectional study. Int. J. Nurs. Stud. 2018, 78, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Eekholm, S.; Ahlström, G.; Kristensson, J.; Lindhardt, T. Gaps between current clinical practice and evidence-based guidelines for treatment and care of older patients with Community Acquired Pneumonia: A descriptive cross-sectional study. BMC Infect. Dis. 2020, 20, 73. [Google Scholar] [CrossRef]
- Rotter, T.; de Jong, R.B.; Lacko, S.E.; Ronellenfitsch, U.; Kinsman, L. Improving Healthcare Quality in Europe. Characteristics, Effectiveness and Implementation of Different Strategies; OECD: London, UK, 2019; pp. 309–331. [Google Scholar]
- Askari, M.; Tam, J.; Klundert, J. The effectiveness of clinical pathway software in inpatient settings: A systematic review. Int. J. Med. Inform. 2021, 147, 104374. [Google Scholar] [CrossRef]
- Owodunni, O.P.; Hampton, J.; Bettick, D.; Sateri, S.; Magnuson, T.; Wick, E.; Psoter, K.J.; Gearhart, S.L. High Compliance to an Enhanced Recovery Pathway for Patients ≥65 Years Undergoing Major Small and Large Intestinal Surgery Is Associated with Improved Postoperative Outcomes. Ann. Surg. 2019, 270, 1117–1123. [Google Scholar] [CrossRef]
- Plishka, C.T.; Rotter, T.; Penz, E.D.; Hansia, M.R.; Fraser, S.A.; Marciniuk, D.D. Effects of Clinical Pathways for COPD on Patient, Professional, and Systems Outcomes: A Systematic Review. Chest 2019, 156, 864–877. [Google Scholar] [CrossRef]
- Rotter, T.; Kinsman, L.; James, E.; Machotta, A.; Willis, J.; Snow, P.; Kugler, J. The effects of clinical pathways on professional practice, patient outcomes, length of stay, and hospital costs: Cochrane systematic review and metaanalysis. Eval. Health Prof. 2012, 35, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Grol, R.; Wensing, M.; Eccles, M.; Davis, D. Improving Patient Care. The implementation of Change in Clinical Practice, 2nd ed.; Wiley Blackwell BMJ Books: Oxford, UK, 2013; pp. 21–386. [Google Scholar]
- Rapport, F.; Clay-Williams, R.; Churruca, K.; Shih, P.; Hogden, A.; Braithwaite, J. The struggle of translating science into action: Foundational concepts of implementation science. J. Eval. Clin. Pract. 2018, 24, 117–126. [Google Scholar] [CrossRef] [PubMed]
- French, S.D.; E Green, S.; O’connor, D.A.; McKenzie, J.E.; Francis, J.J.; Michie, S.; Buchbinder, R.; Schattner, P.; Spike, N.; Grimshaw, J.M. Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the Theoretical Domains Framework. Implement. Sci. 2012, 7, 38. [Google Scholar] [CrossRef] [PubMed]
- Tavender, E.J.; Bosch, M.; Gruen, R.L.; Green, S.E.; Michie, S.; Brennan, S.E.; Francis, J.J.; Ponsford, J.L.; Knott, J.C.; Meares, S.; et al. Developing a targeted, theory-informed implementation intervention using two theoretical frameworks to address health professional and organisational factors: A case study to improve the management of mild traumatic brain injury in the emergency department. Implement. Sci. 2015, 10, 74. [Google Scholar] [CrossRef] [PubMed]
- Craig, L.E.; Taylor, N.; Grimley, R.; Cadilhac, D.A.; McInnes, E.; Phillips, R.; Dale, S.; O’Connor, D.; Levi, C.; Fitzgerald, M.; et al. Development of a theory-informed implementation intervention to improve the triage, treatment and transfer of stroke patients in emergency departments using the Theoretical Domains Framework (TDF): The T(3) Trial. Implement. Sci. 2017, 12, 88. [Google Scholar] [CrossRef] [PubMed]
- Birken, S.A.; Powell, B.J.; Shea, C.M.; Haines, E.R.; Kirk, M.A.; Leeman, J.; Rohweder, C.; Damschroder, L.; Presseau, J. Criteria for selecting implementation science theories and frameworks: Results from an international survey. Implement. Sci. 2017, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Powell, B.J.; Fernandez, M.E.; Williams, N.J.; Aarons, G.A.; Beidas, R.S.; Lewis, C.C.; McHugh, S.M.; Weiner, B.J. Enhancing the impact of implementation strategies in healthcare: A research agenda. Front. Public Health 2019, 7, 3. [Google Scholar] [CrossRef]
- Nilsen, P.; Potthoff, S.; Birken, S.A. Conceptualising Four Categories of Behaviours: Implications for Implementation Strategies to Achieve Behaviour Change. Front. Health Serv. 2022, 1, 795144. [Google Scholar] [CrossRef]
- Spoon, D.; Rietbergen, T.; Huis, A.; Heinen, M.; van Dijk, M.; van Bodegom-Vos, L.; Ista, E. Implementation strategies used to implement nursing guidelines in daily practice: A systematic review. Int. J. Nurs. Stud. 2020, 111, 103748. [Google Scholar] [CrossRef]
- Wensing, M.; Wilson, P. Making implementation science more efficient: Capitalizing on opportunities beyond the field. Implement. Sci. 2023, 18, 40. [Google Scholar] [CrossRef]
- Waltz, T.J.; Powell, B.J.; Fernández, M.E.; Abadie, B.; Damschroder, L.J. Choosing implementation strategies to address contextual barriers: Diversity in recommendations and future directions. Implement. Sci. 2019, 14, 42. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Fixsen, D.L.; Grimshaw, J.M.; Eccles, M.P. Specifying and reporting complex behaviour change interventions: The need for a scientific method. Implement. Sci. 2009, 4, 40. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, H.L.; Squires, J.E.; Kolehmainen, N.; Fraser, C.; Grimshaw, J.M. Methods for designing interventions to change healthcare professionals’ behaviour: A systematic review. Implement. Sci. 2017, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G.; Gottlieb, N.H.; Fernandez, M.E. Planning Health Promotion Programs: An Intervention Mapping Approach, 3rd ed.; Jossey-Bass: San Francisco, CA, USA, 2011. [Google Scholar]
- Eekholm, S.; Samuelson, K.; Ahlstrom, G.; Lindhardt, T. ‘Stolen Time’—Delivering Nursing at the Bottom of a Hierarchy: An Ethnographic Study of Barriers and Facilitators for Evidence-Based Nursing for Patients with Community-Acquired Pneumonia. Healthcare 2021, 9, 1524. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Johnston, M.; Francis, J.; Hardeman, W.; Eccles, M. From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour change techniques. Appl. Psychol. 2008, 57, 660–680. [Google Scholar] [CrossRef]
- Kok, G.; Gottlieb, N.H.; Peters, G.-J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.; Fernández, M.E.; Markham, C.; Bartholomew, L.K. A taxonomy of behaviour change methods: An Intervention Mapping approach. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef]
- Kelder, S.H.; Hoelscher, D.; Perry, C.L. How Individuals, Environments, and Health Behaviors Interact: Social Cognitive Theory. In Health Behavior: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015; pp. 225–285. [Google Scholar]
- Bate, P.; Robert, G. Experience-based design: From redesigning the system around the patient to co-designing services with the patient. Qual. Saf. Health Care 2006, 15, 307–310. [Google Scholar] [CrossRef]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Admin. Policy Ment. Health 2011, 38, 65–76. [Google Scholar] [CrossRef]
- Recio-Saucedo, A.; Dall’Ora, C.; Msc, A.M.; Ball, J.; Briggs, J.; Meredith, P.; Redfern, O.C.; Kovacs, C.; Prytherch, D.; Smith, G.B.; et al. What impact does nursing care left undone have on patient outcomes? Review of the literature. J. Clin. Nurs. 2018, 27, 2248–2259. [Google Scholar] [CrossRef]
- Jones, T.L.; Hamilton, P.; Murry, N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. Int. J. Nurs. Stud. 2015, 52, 1121–1137. [Google Scholar] [CrossRef] [PubMed]
- Gattarello, S.; del Crips, I.; Ramírez, S.; Almarales, J.R.; Borgatta, B.; Lagunes, L.; Encina, B.; Rello, J. Causes of non-adherence to therapeutic guidelines in severe community-acquired pneumonia. Rev. Bras. Ter. Intensive 2015, 27, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Van den Heede, K.; Griffiths, P.; Busse, R.; Diomidous, M.; Kinnunen, J.; Kózka, M.; Lesaffre, E.; et al. Nurse staffing and education and hospital mortality in nine European countries: A retrospective observational study. Lancet 2014, 383, 1824–1830. [Google Scholar] [CrossRef] [PubMed]
- Needleman, J.; Liu, J.; Shang, J.; Larson, E.L.; Stone, P.W. Association of registered nurse and nursing support staffing with inpatient hospital mortality. BMJ Qual. Saf. 2019, 29, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, P.; Nilsson, E.; Forsell, M.; Johansson, O.; Hoogstraate, J. A systematic review of the preventive effect of oral hygiene on pneumonia and respiratory tract infection in elderly people in hospitals and nursing homes: Effect estimates and methodological quality of randomized controlled trials. J. Am. Geriatr. Soc. 2008, 56, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Linde-Zwirble, W.T.; Bittner, E.A.; Sahatjian, J.; Hansell, D. Fluid administration in severe sepsis and septic shock, patterns and outcomes: An analysis of a large national database. Intensive Care Med. 2017, 43, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Falvey, J.R.; Mangione, K.K.; Stevens-Lapsley, J.E. Rethinking Hospital-Associated Deconditioning: Proposed Paradigm Shift. Phys. Ther. 2015, 95, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Van Ancum, J.M.; Scheerman, K.; Jonkman, N.H.; Smeenk, H.E.; Kruizinga, R.C.; Meskers, C.G.; Maier, A.B. Change in muscle strength and muscle mass in older hospitalized patients: A systematic review and meta-analysis. Exp. Gerontol. 2017, 92, 34–41. [Google Scholar] [CrossRef]
- Kitson, A.L.; Muntlin, A.A.; Conroy, T. Anything but basic: Nursing’s challenge in meeting patients’ fundamental care needs. J. Nurs. Sch. 2014, 46, 331–339. [Google Scholar] [CrossRef]
- Baker, R.; Camosso-Stefinovic, J.; Gillies, C.; Shaw, E.J.; Cheater, F.; Flottorp, S.; Robertson, N.; Wensing, M.; Fiander, M.; Eccles, M.P.; et al. Tailored interventions to address determinants of practice. Cochrane Database Syst. Rev. 2015, 2015, Cd005470. [Google Scholar] [CrossRef]
- Grimshaw, J.M.; Shirran, L.; Thomas, R.; Mowatt, G.; Fraser, C.; Bero, L.; Grilli, R.; Harvey, E.; Oxman, A.; A O’Brien, M. Changing provider behavior: An overview of systematic reviews of interventions. Med. Care 2001, 39, II2–II45. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.C.; Fischer, S.; Weiner, B.J.; Stanick, C.; Kim, M.; Martinez, R.G. Outcomes for implementation science: An enhanced systematic review of instruments using evidence-based rating criteria. Implement. Sci. 2015, 10, 155. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. Framework for the development and evaluation of complex interventions: Gap analysis, workshop and consultation-informed update. Health Technol. Assess. 2021, 25, 1–132. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, P. Making sense of implementation theories, models and frameworks. Implement. Sci. 2015, 10, 53. [Google Scholar] [CrossRef] [PubMed]
- Bergström, A.; Ehrenberg, A.; Eldh, A.C.; Graham, I.D.; Gustafsson, K.; Harvey, G.; Hunter, S.; Kitson, A.; Rycroft-Malone, J.; Wallin, L. The use of the PARIHS framework in implementation research and practice-a citation analysis of the literature. Implement. Sci. 2020, 15, 68. [Google Scholar] [CrossRef] [PubMed]
- Garba, R.M.; Gadanya, M.A. The role of intervention mapping in designing disease prevention interventions: A systematic review of the literature. PLoS ONE 2017, 12, e0174438. [Google Scholar] [CrossRef]
- Abbey, M.; Bartholomew, L.K.; Chinbuah, M.A.; Gyapong, M.; Gyapong, J.O.; van den Borne, B. Development of a theory and evidence-based program to promote community treatment of fevers in children under five in a rural district in Southern Ghana: An intervention mapping approach. BMC Public Health 2017, 17, 120. [Google Scholar] [CrossRef]
- Geerligs, L.; Rankin, N.M.; Shepherd, H.L.; Butow, P. Hospital-based interventions: A systematic review of staff-reported barriers and facilitators to implementation processes. Implement. Sci. 2018, 13, 36. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef]
- Wagenaar, B.H.; Hammett, W.H.; Jackson, C.; Atkins, D.L.; Belus, J.M.; Kemp, C.G. Implementation outcomes and strategies for depression interventions in low- and middle-income countries: A systematic review. Glob. Ment. Health 2020, 7, e7. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Papoutsi, C. Studying complexity in health services research: Desperately seeking an overdue paradigm shift. BMC Med. 2018, 16, 95. [Google Scholar] [CrossRef] [PubMed]
- Bakhuys Roozeboom, M.C.; Wiezer, N.M.; Boot, C.R.L.; Bongers, P.M.; Schelvis, R.M.C. Use of Intervention Mapping for Occupational Risk Prevention and Health Promotion: A Systematic Review of Literature. Int. J. Environ. Res. Public Health. 2021, 18, 1775. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.E.; Ten Hoor, G.A.; Van Lieshout, S.; Rodriguez, S.A.; Beidas, R.S.; Parcel, G.; Kok, G. Implementation mapping: Using intervention mapping to develop implementation strategies. Front. Public Health 2019, 7, 158. [Google Scholar] [CrossRef] [PubMed]
- van Noort, H.H.J.; Heinen, M.; van Asseldonk, M.; Ettema, R.G.A.; Vermeulen, H.; Huisman-de Waal, G.; On the behalf of the Basic Care Revisited (BCR) Research Group. Using intervention mapping to develop an outpatient nursing nutritional intervention to improve nutritional status in undernourished patients planned for surgery. BMC Health Serv. Res. 2020, 20, 152. [Google Scholar] [CrossRef] [PubMed]
- Danish Society of Respiratory Medicine. Guidelines for Pneumonia-Initial Assessment And Treatment. 2010. Available online: https://www.lungemedicin.dk/fagligt/71-pneumoni.html (accessed on 1 July 2016).
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L.; et al. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64, iii1–iii55. [Google Scholar] [CrossRef]
- Frølund, J.C.; Klit, M.Ø.; Ladegaard, L.; Lytjohan, M.; Mielcke, H.; Nielsen, B.E.; Olesen, L.B. Clinical Guideline-Oral Hygiene for Adult Citizens and Patients 2016. Available online: http://cfkr.dk/media/351666/Mundhygiejne%20til%20voksne%20borgere%20og%20patienter.pdf (accessed on 1 July 2016).
- The Danish Diet & Nutrition Association. The National Nutrition Handbook 2016. Available online: https://kosthåndbogen.dk/content/om-kosthåndbogen-0 (accessed on 1 July 2016).
- The Danish Health Authority. Knowledge Base: Nutritional Interventions for the Older Medical Patient. 2017. Available online: https://www.sst.dk/da/udgivelser/2017/~/media/3AD0A0709E57494EB8726B9D004CAE00.ashx (accessed on 1 April 2017).
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; Van Der Heijden, G.; et al. Guidelines for the management of adult lower respiratory tract infections-full version. Clin. Microbiol. Infect. 2011, 17, E1–E59. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, B.R.; Howard, L.S.; Earis, J.; Mak, V. British Thoracic Society Guideline for oxygen use in adults in healthcare and emergency settings. BMJ Open Respir. Res. 2017, 4, e000170. [Google Scholar] [CrossRef]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]


{kind=link}
| Step | Tasks | Definitions |
|---|---|---|
|
|
|
|
|
|
|
|
|
|
| |
|
| |
|
|
| Individual Level | Team Level | Management Level | Environmental Level |
|---|---|---|---|
|
|
|
|
| Individual Level (RNs, LPNs) | Team Level (IDT) | Environmental (NM) Level |
|---|---|---|
|
|
|
| Materials | ||
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eekholm, S.; Samuelson, K.; Ahlström, G.; Lindhardt, T. Development of an Implementation Strategy Tailored to Deliver Evidence-Based and Person-Centred Nursing Care for Patients with Community-Acquired Pneumonia: An Intervention Mapping Approach. Healthcare 2024, 12, 32. https://doi.org/10.3390/healthcare12010032
Eekholm S, Samuelson K, Ahlström G, Lindhardt T. Development of an Implementation Strategy Tailored to Deliver Evidence-Based and Person-Centred Nursing Care for Patients with Community-Acquired Pneumonia: An Intervention Mapping Approach. Healthcare. 2024; 12(1):32. https://doi.org/10.3390/healthcare12010032
Chicago/Turabian StyleEekholm, Signe, Karin Samuelson, Gerd Ahlström, and Tove Lindhardt. 2024. "Development of an Implementation Strategy Tailored to Deliver Evidence-Based and Person-Centred Nursing Care for Patients with Community-Acquired Pneumonia: An Intervention Mapping Approach" Healthcare 12, no. 1: 32. https://doi.org/10.3390/healthcare12010032