
Respiratory Function Analysis in Patients with Chronic Pain: An Umbrella Review and Meta-Analysis of Pooled Findings
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.1.1. Patients
2.1.2. Outcome Measures
Respiratory Muscle Strength
Pulmonary Function
2.1.3. Study Design
2.2. Search Strategy
2.3. Selection Criteria and Data Extraction
2.4. Methodological Quality Assessment
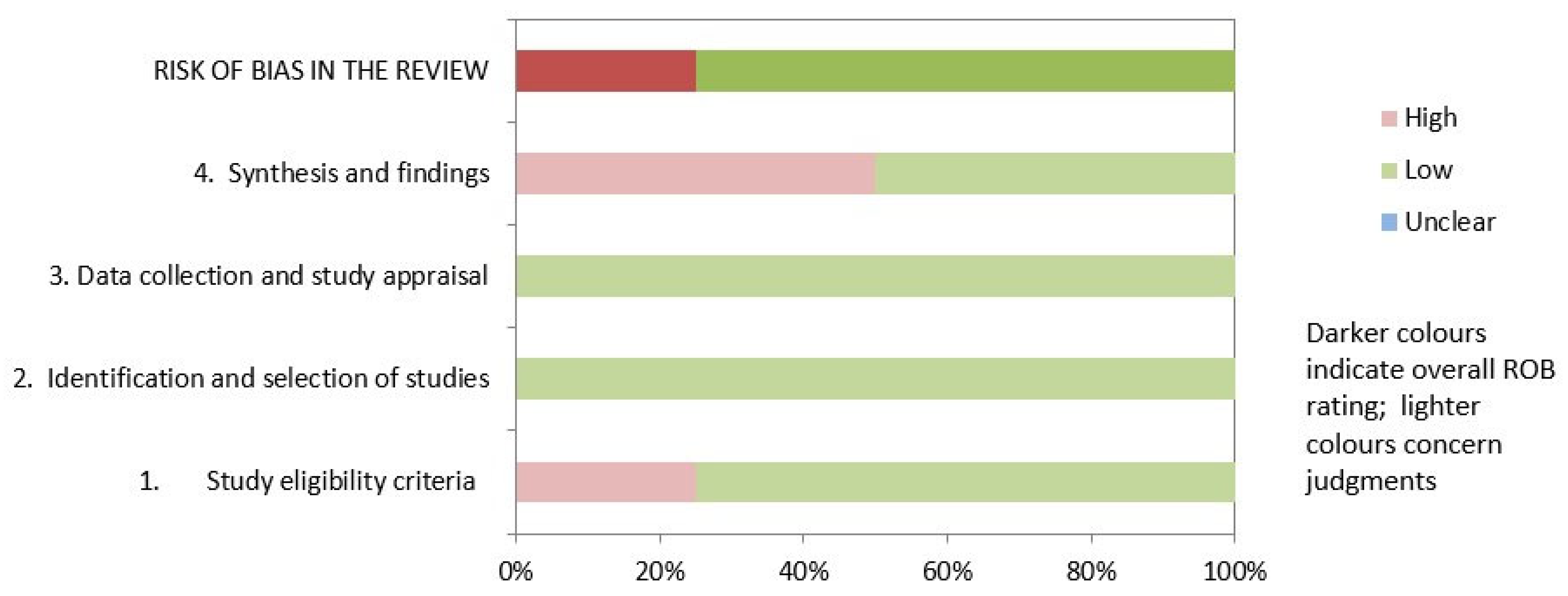
2.5. Risk of Bias Assessment
2.6. Grading of Evidence
2.7. Data Synthesis and Statistical Analysis
3. Results
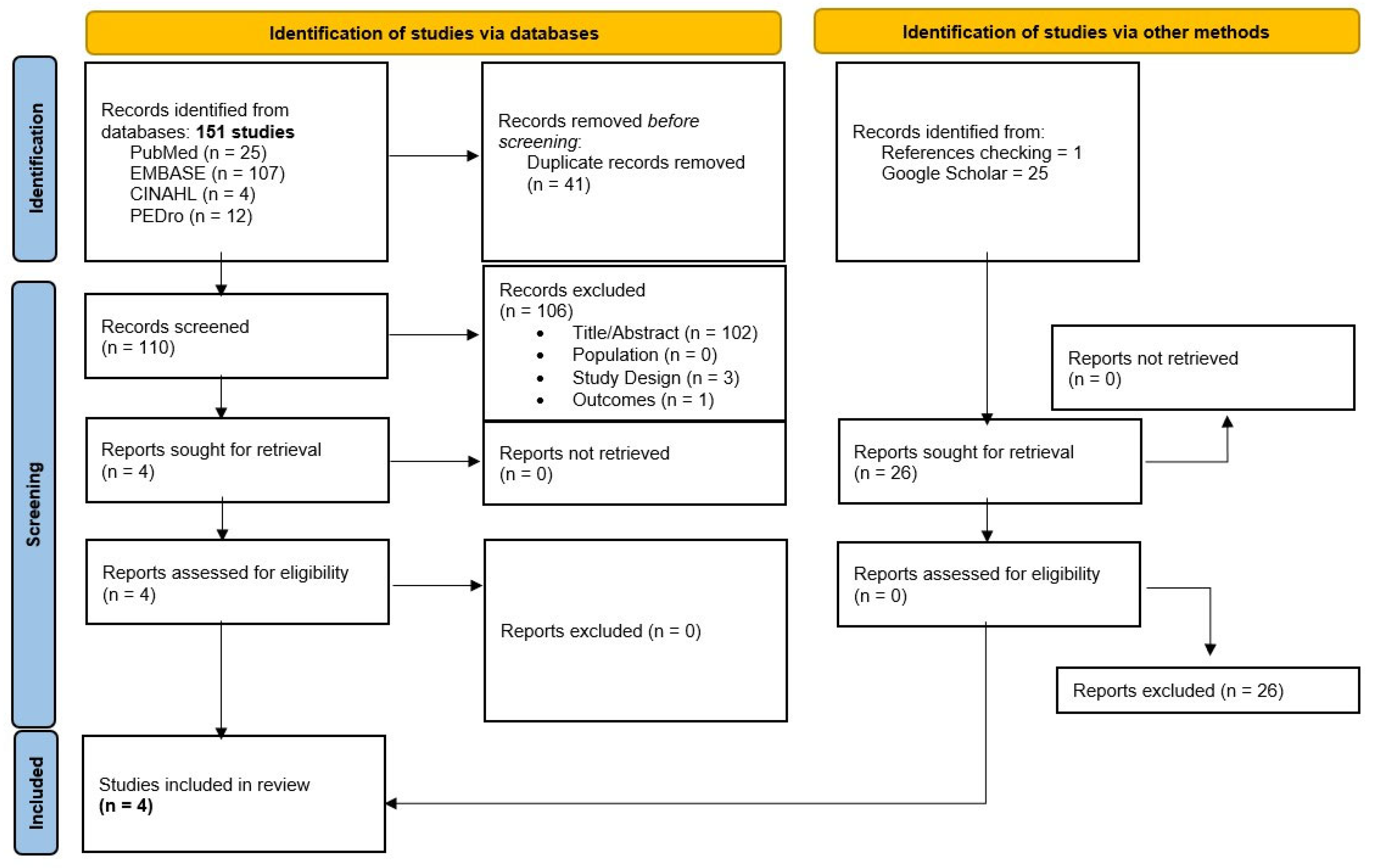
3.1. Study Selection
3.2. Characteristics of the Included Systematic Reviews
3.3. Results of AMSTAR and ROBIS
3.4. Grading of Evidence Results (PAGAC)
3.5. Qualitative Synthesis
3.5.1. Vital Capacity
3.5.2. Forced Expiratory Ratio
3.5.3. Forced Expiratory Flow from 25% to 75%
3.5.4. Peak Expiratory Flow
3.6. Meta-Analysis Results
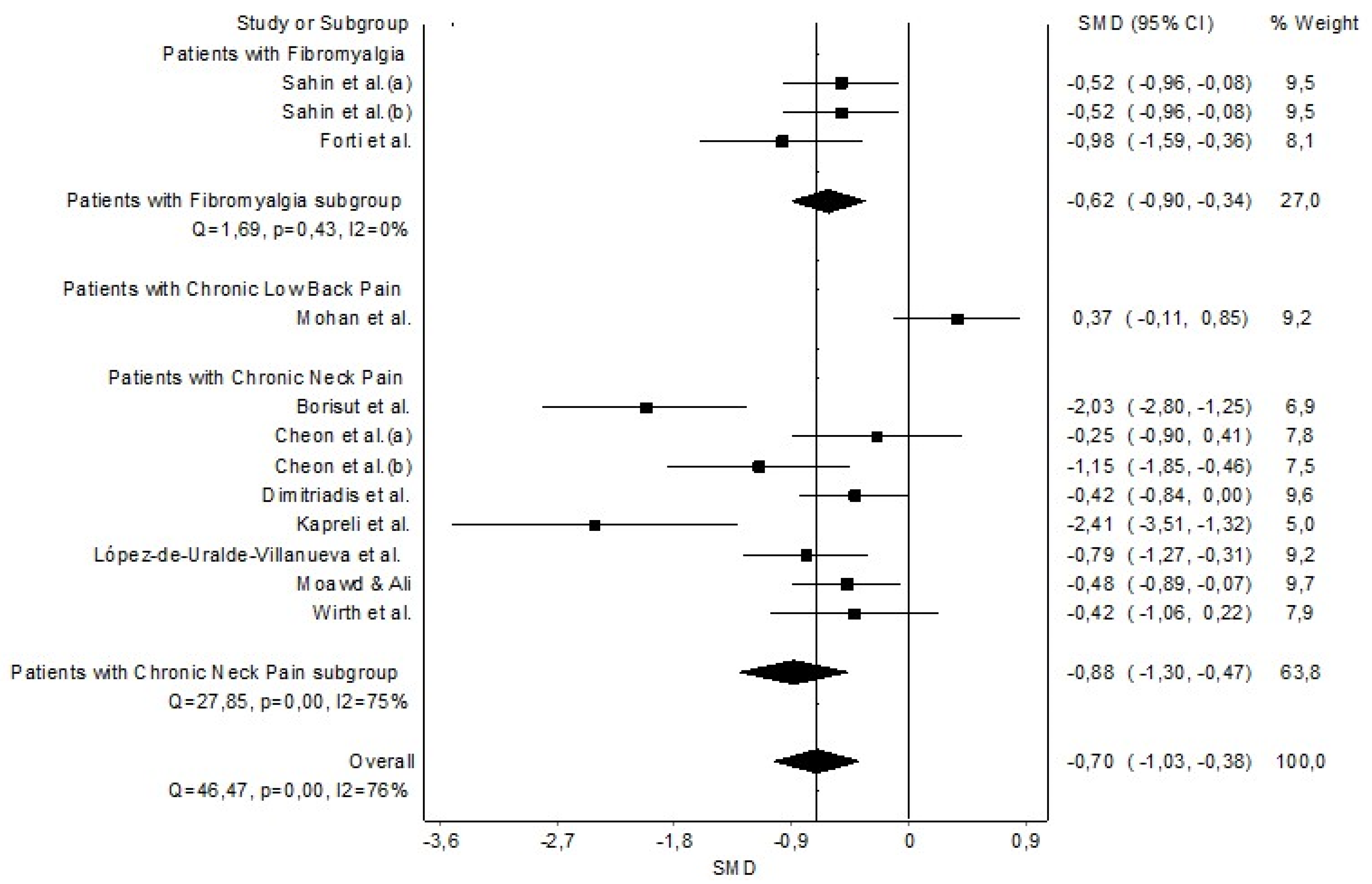
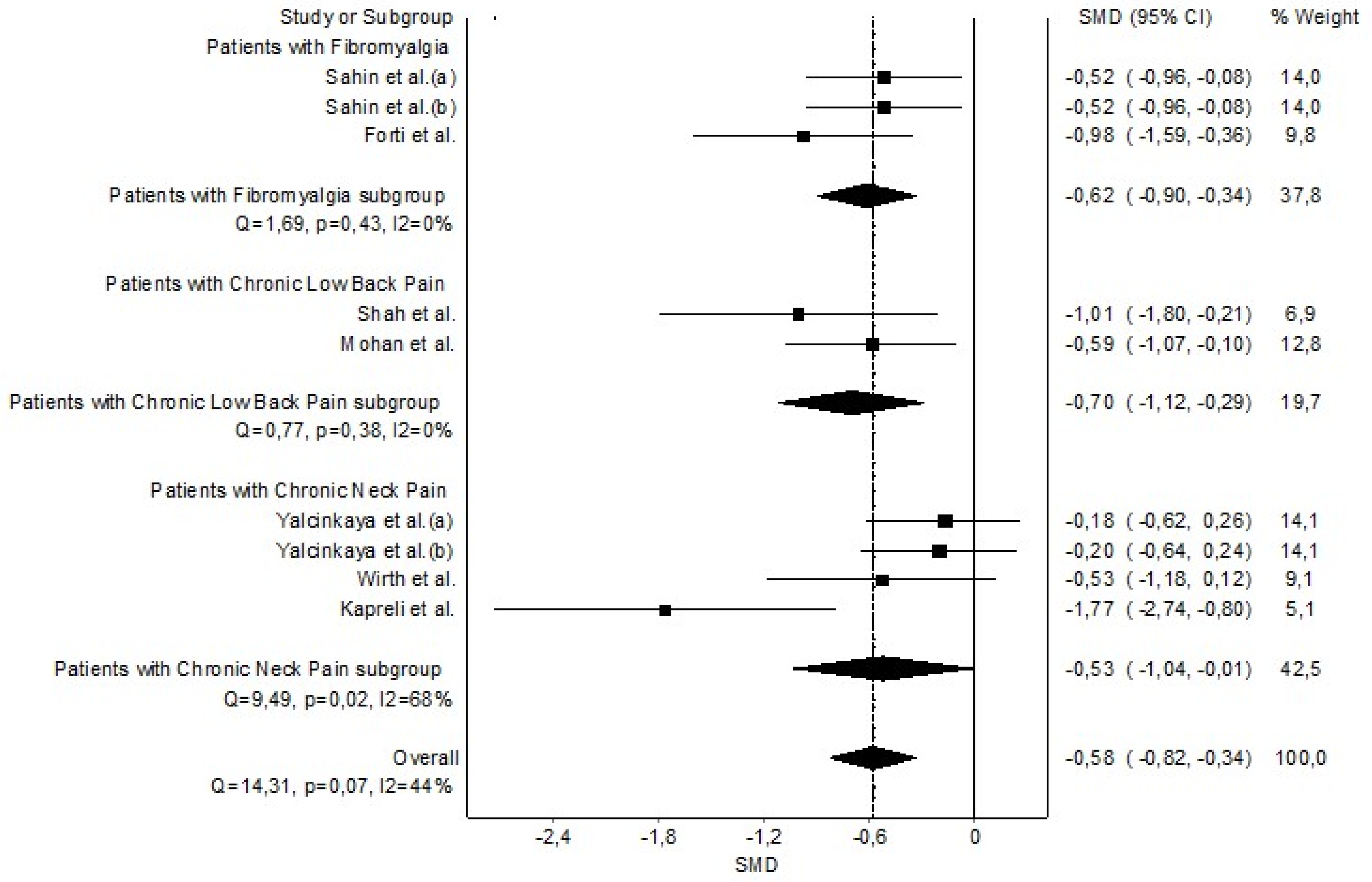
3.6.1. Maximal Inspiratory Pressure
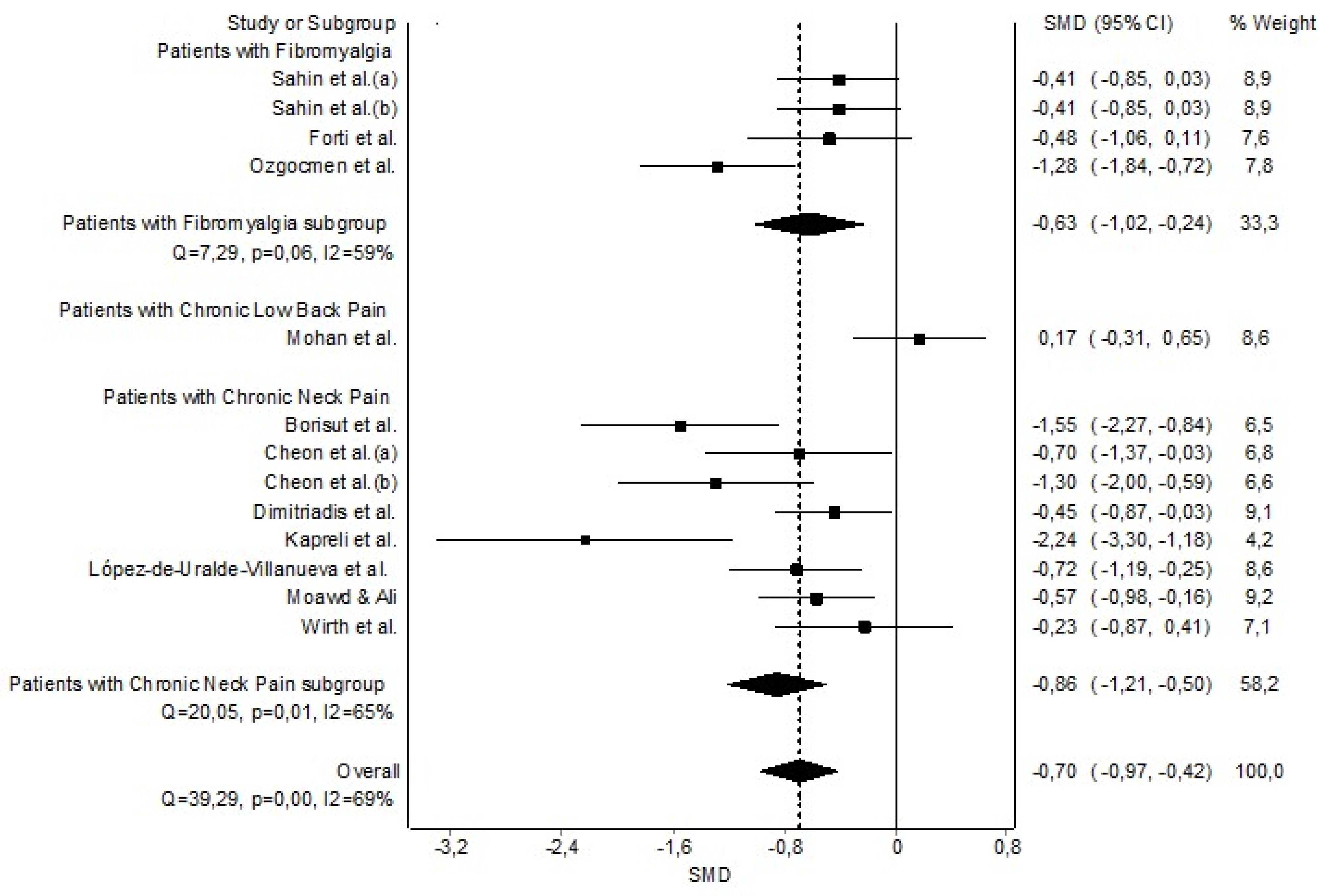
3.6.2. Maximal Expiratory Pressure
3.6.3. Maximum Voluntary Ventilation
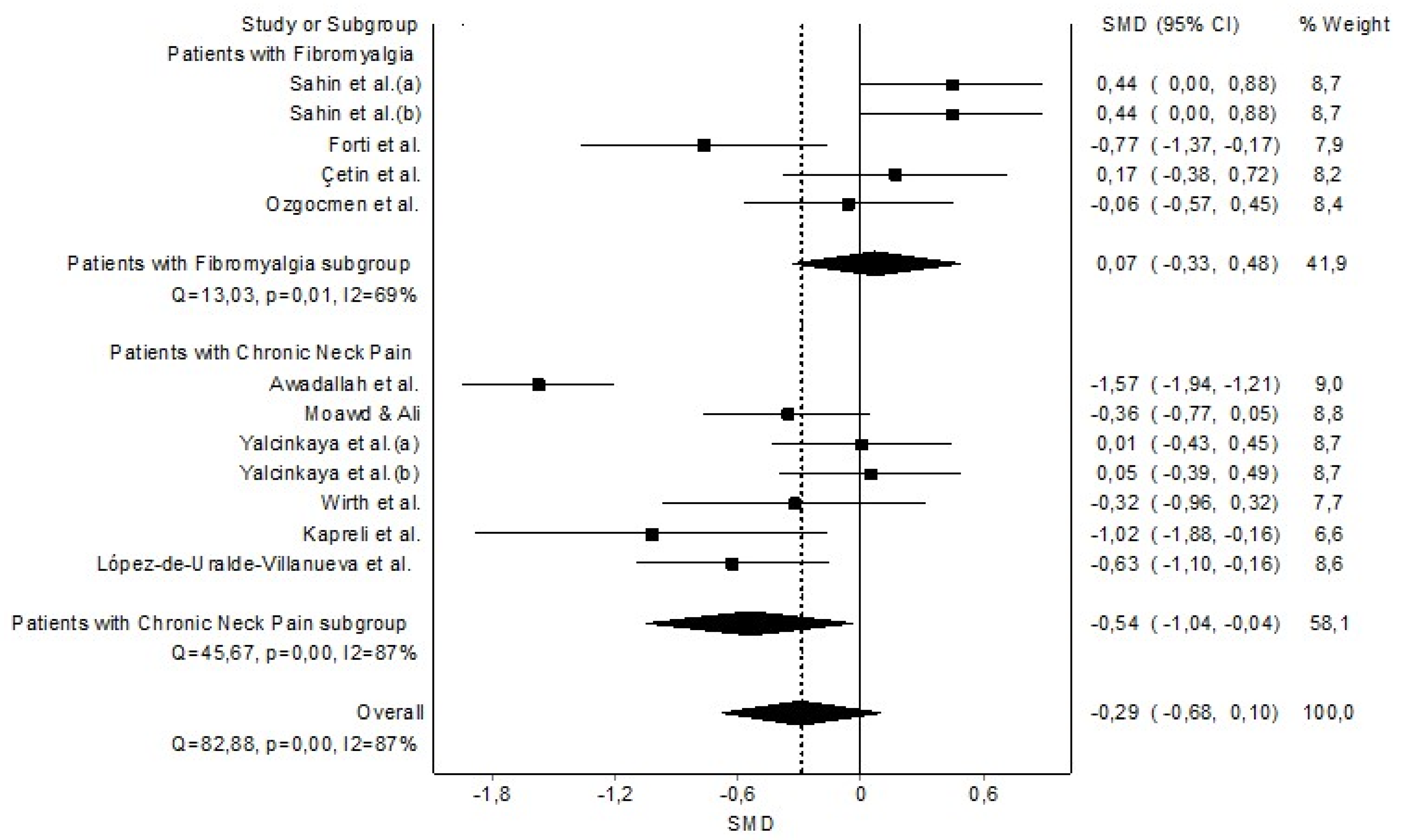
3.6.4. Forced Vital Capacity
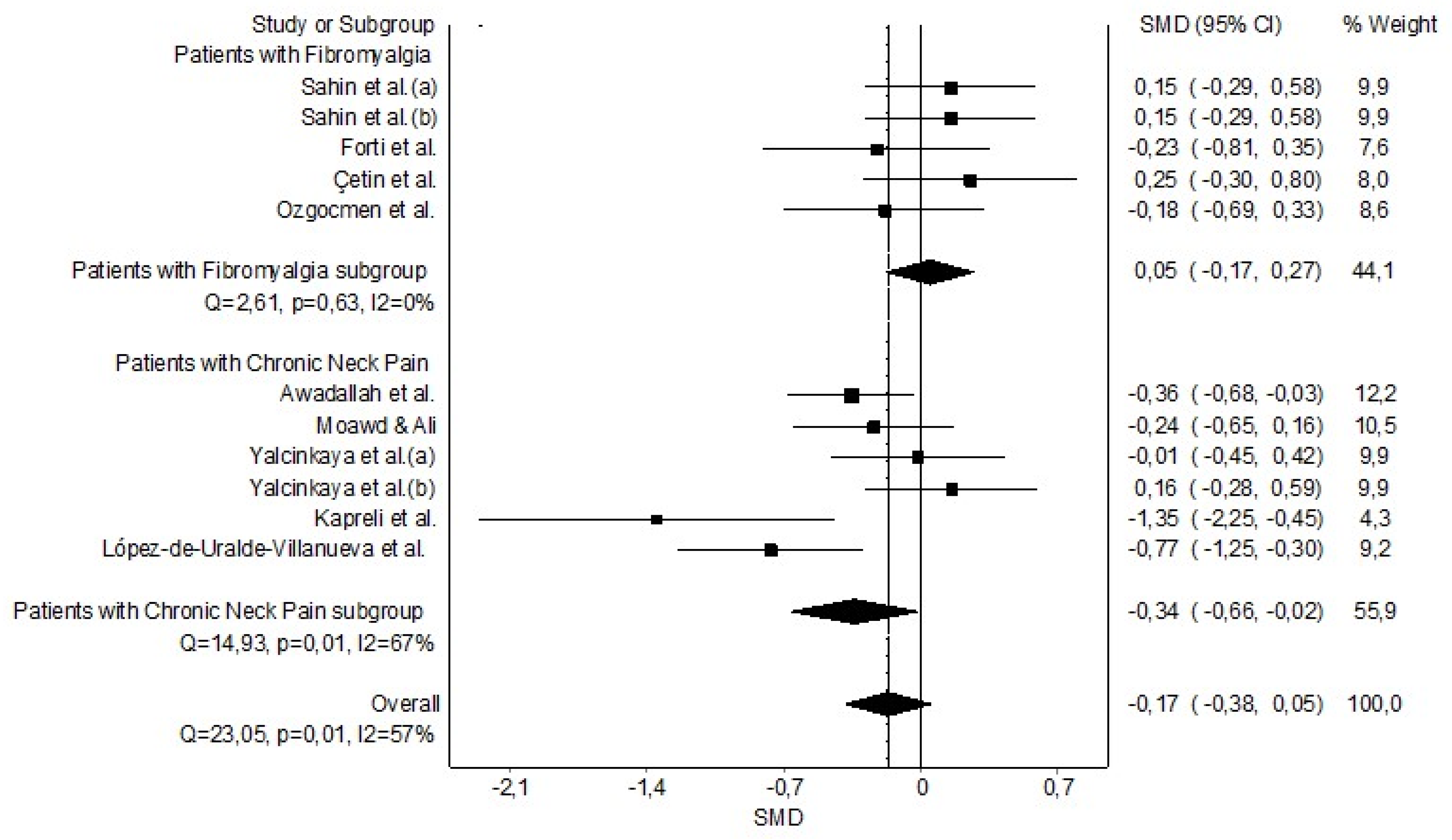
3.6.5. Forced Expiratory Volume during the First Second
4. Discussion
4.1. Clinical Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A
Appendix A.1. Database Search Strategies
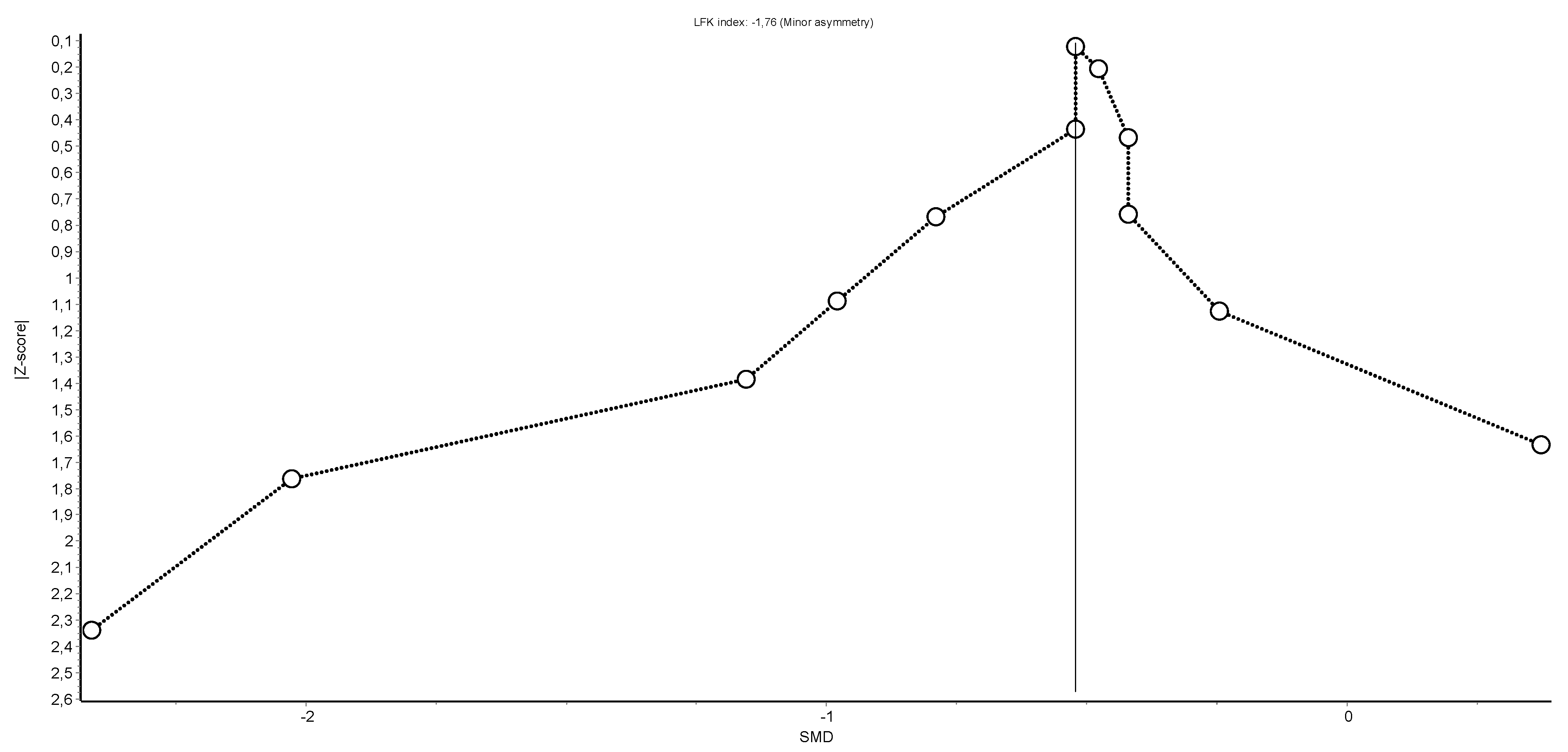
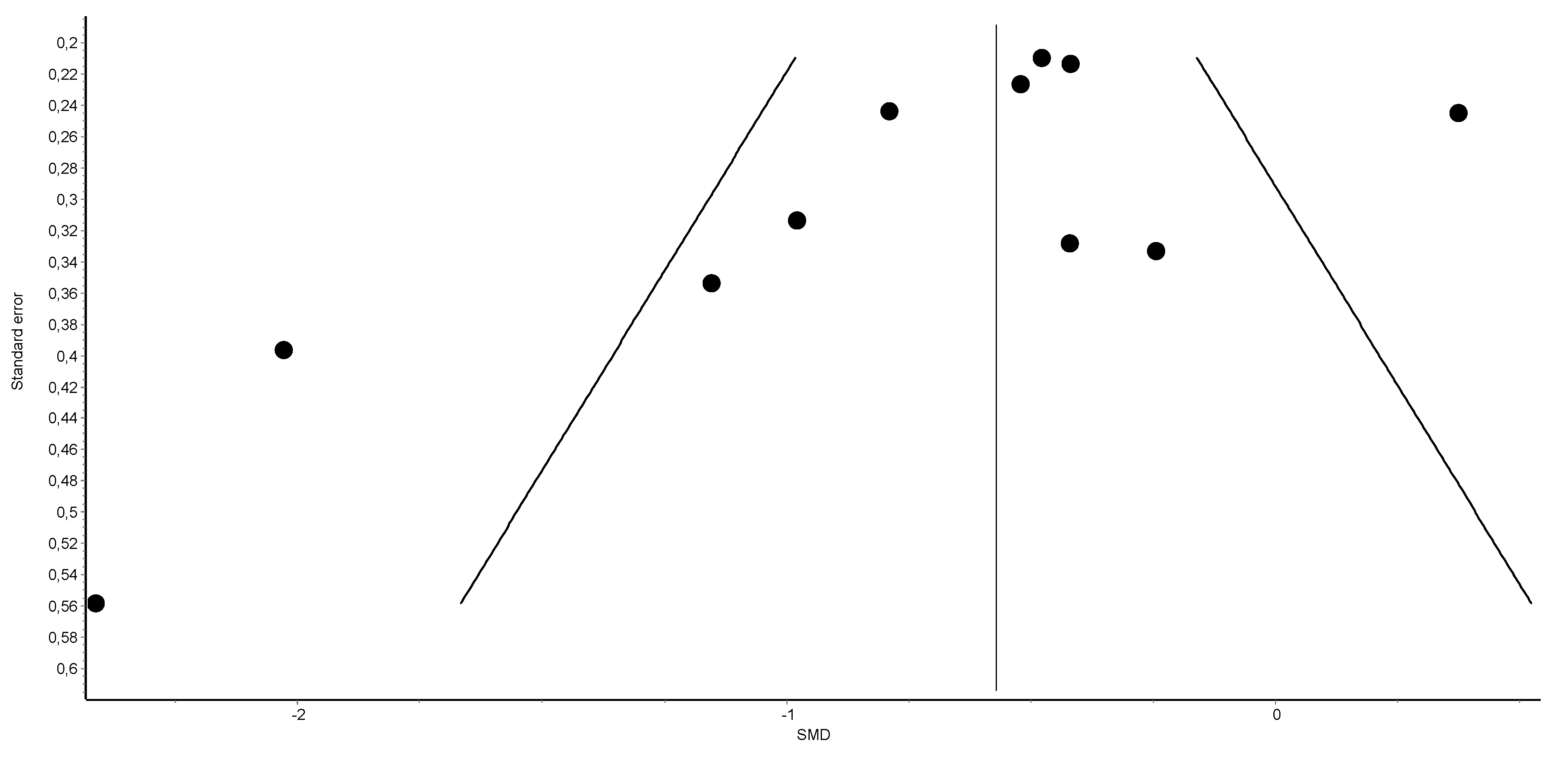
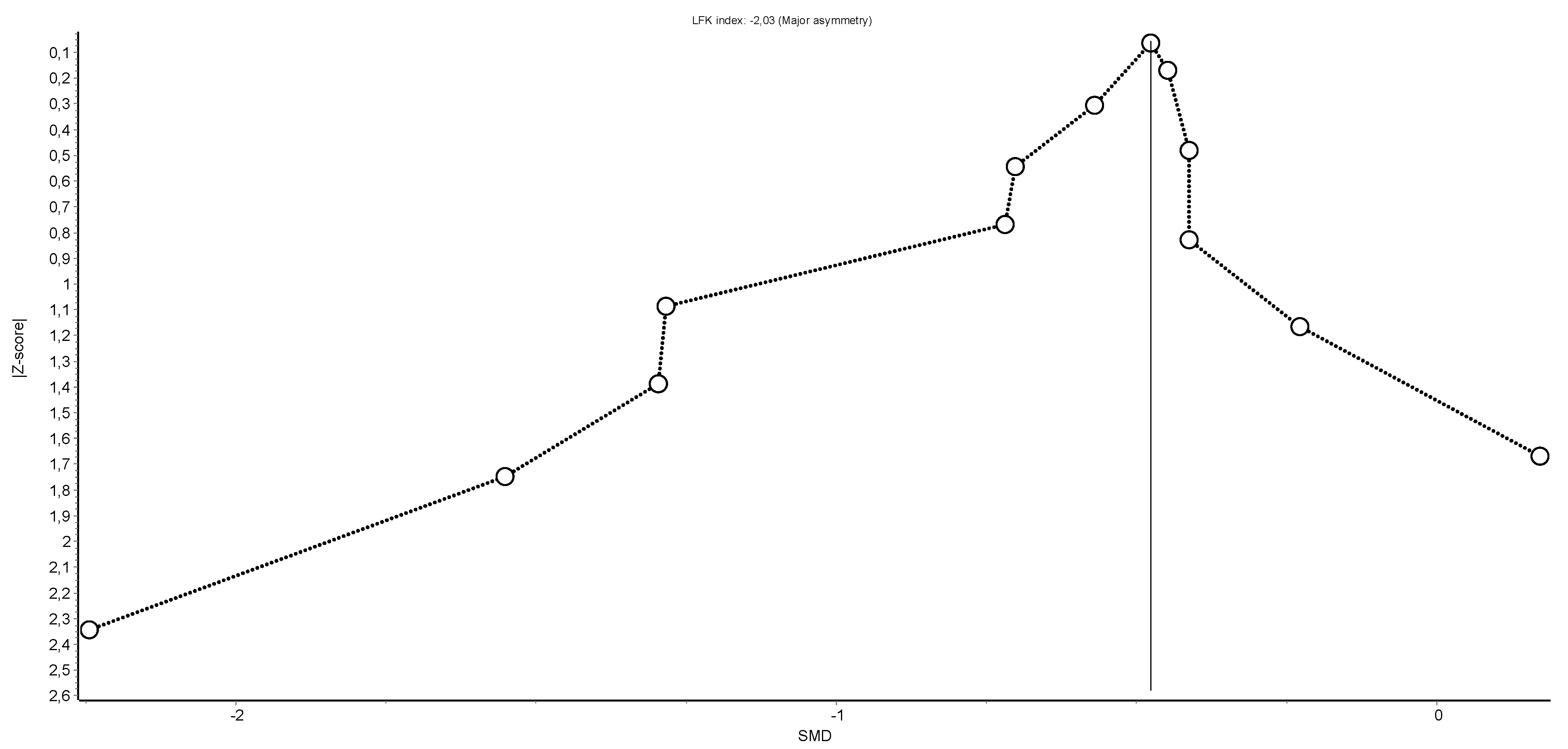
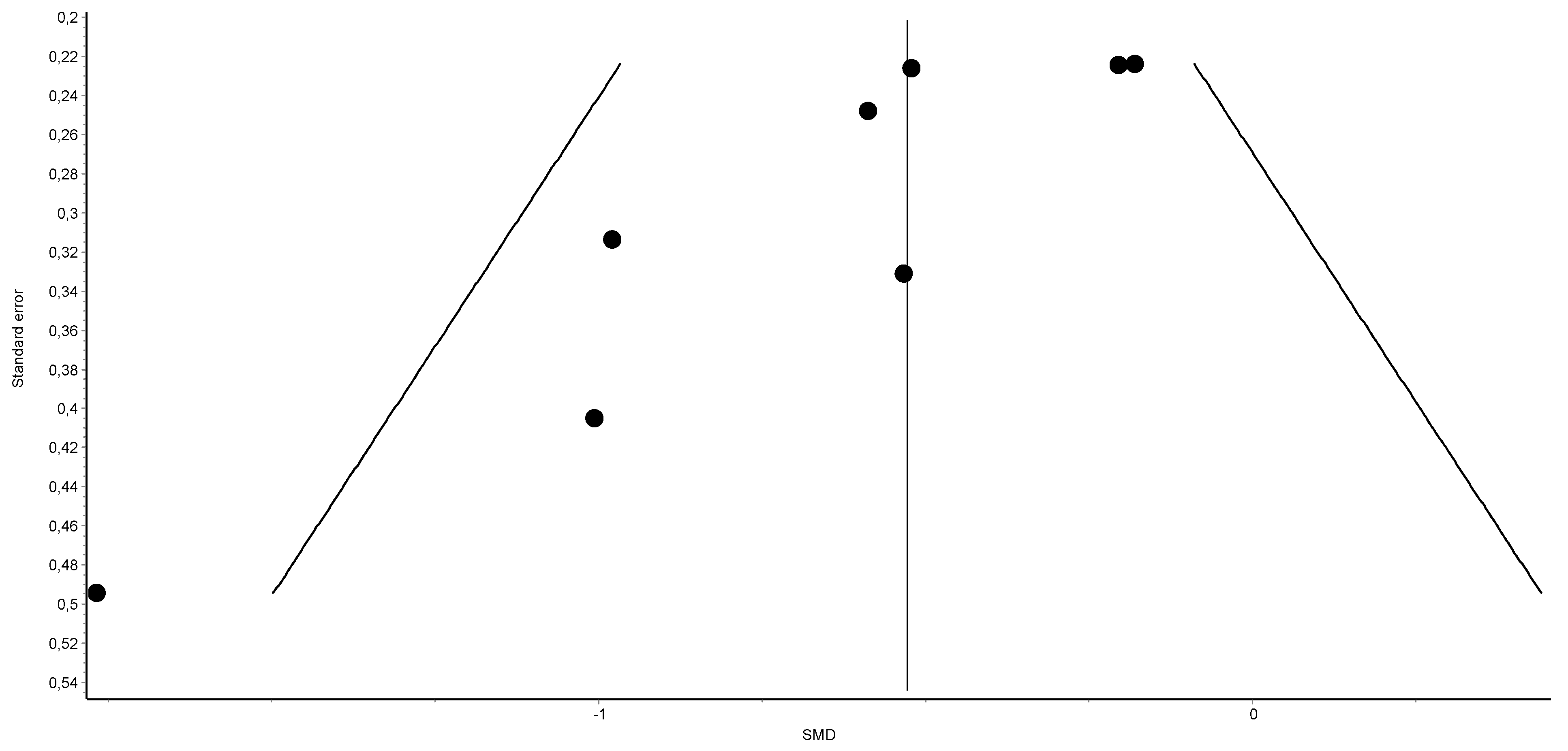
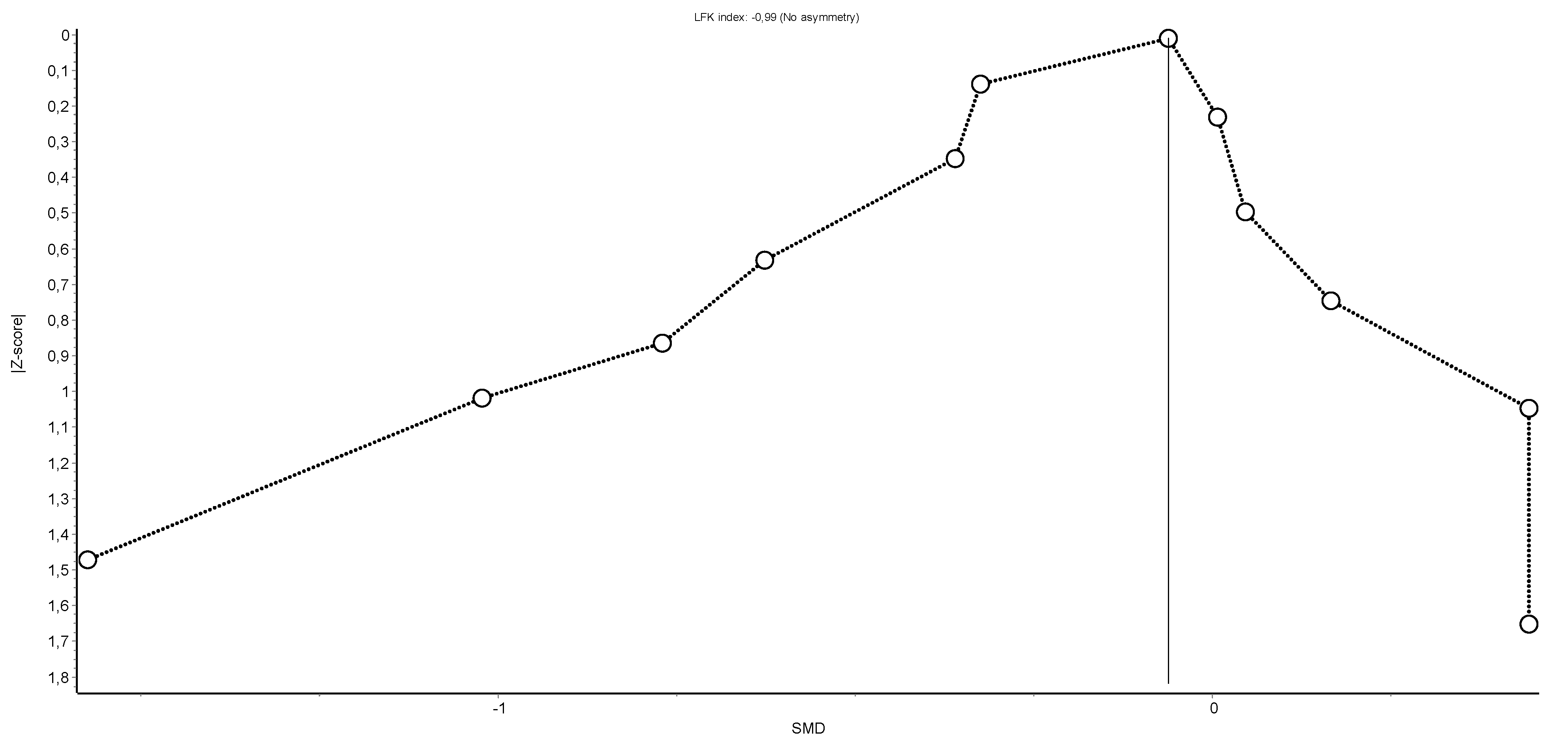
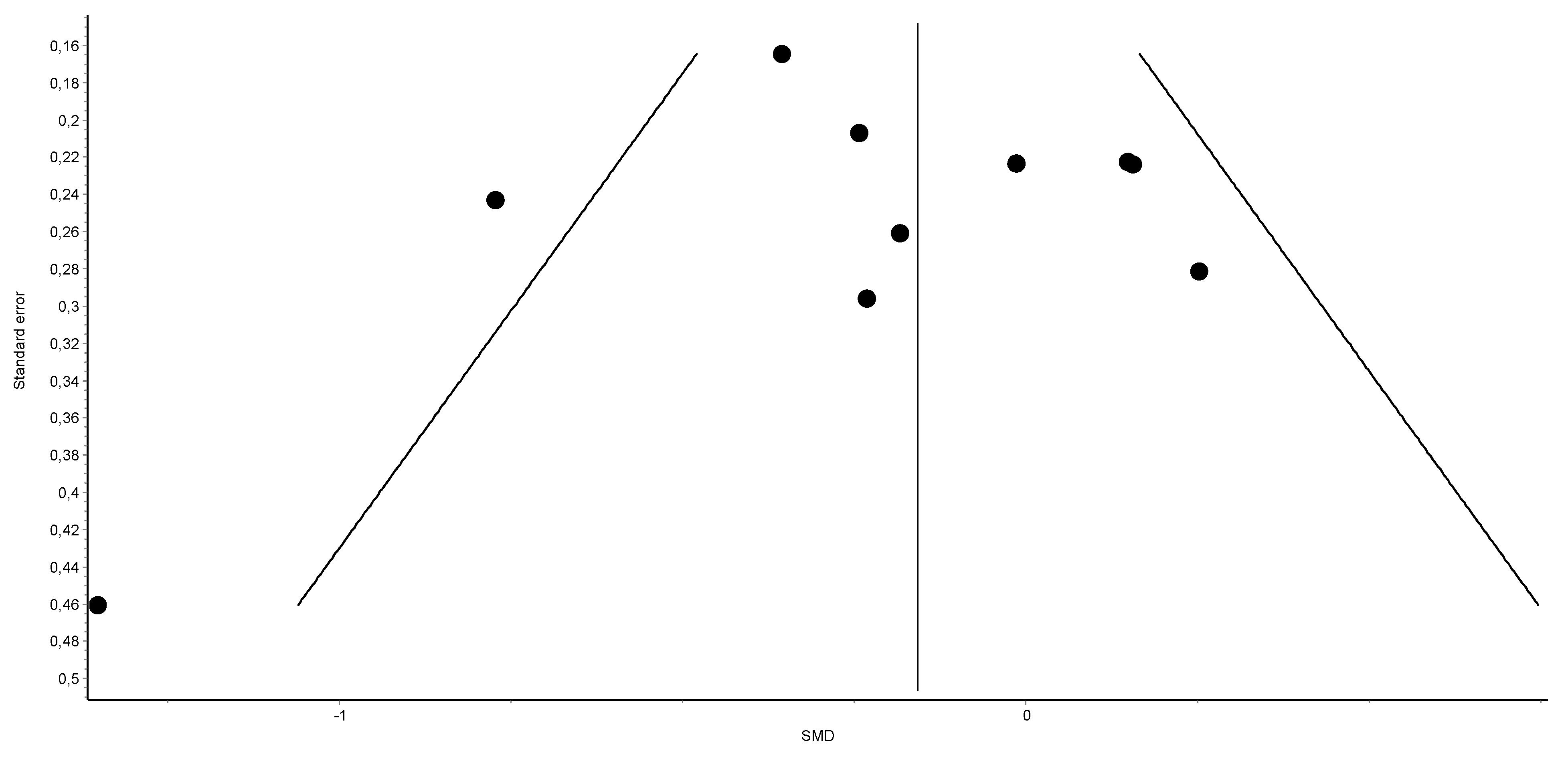
Appendix A.2. Synthesis Funnel Plot and Doi Plot (LFK Index) for Maximal Inspiratory Pressure Variable: Funnel Plot Aims to Assess the Existence of Publication Bias


Appendix A.3. Sensitivity Exclusion Analysis for Maximal Inspiratory Pressure Variable

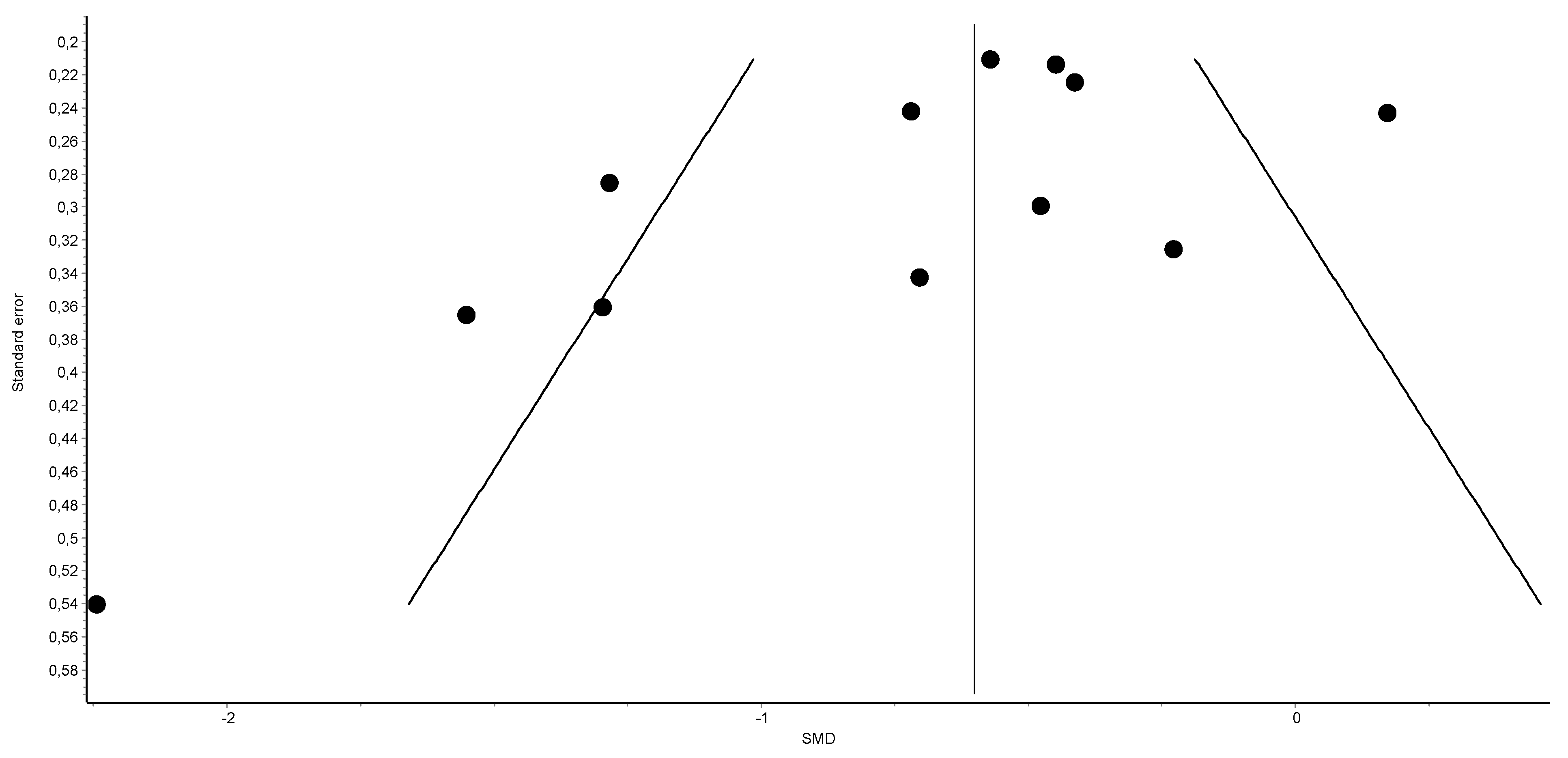
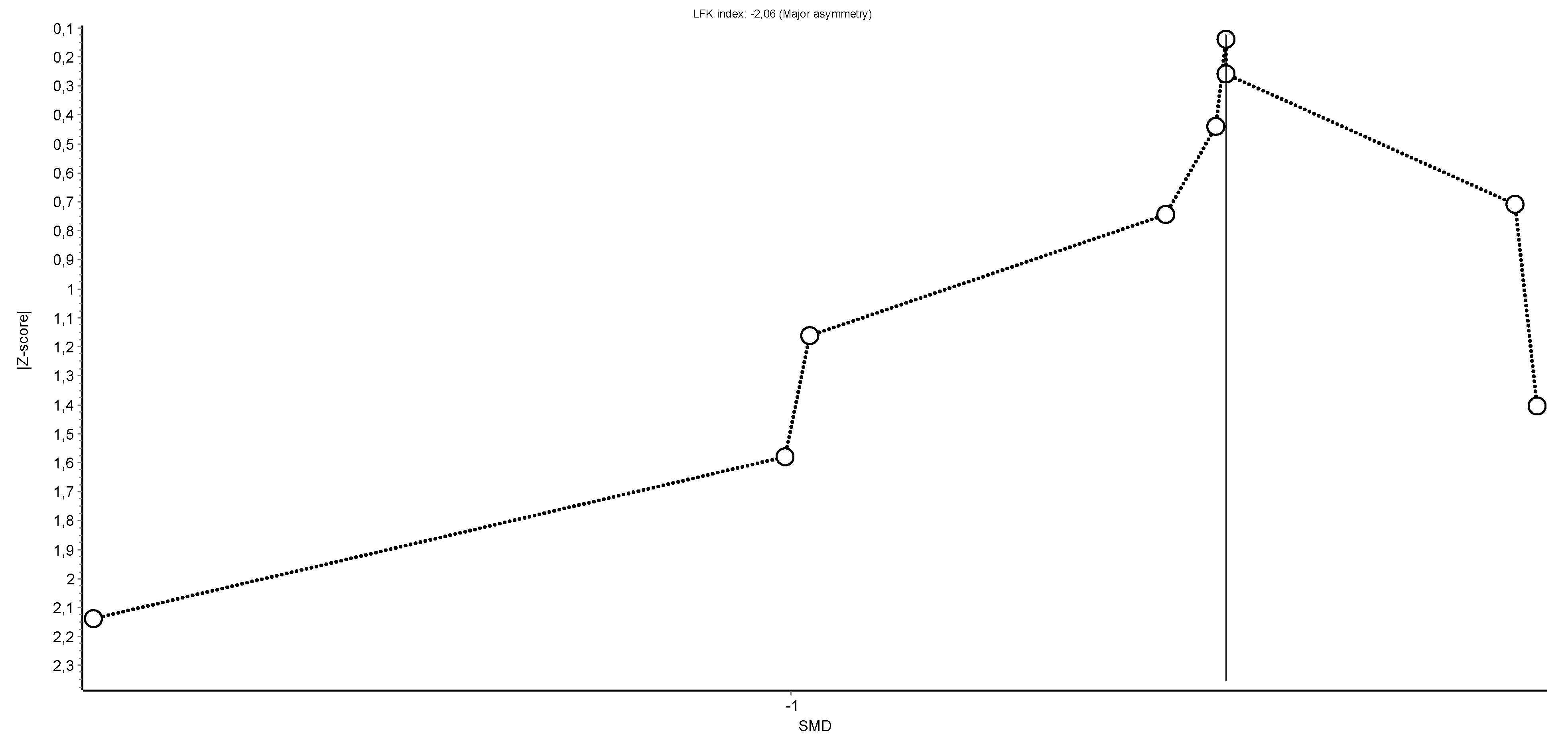
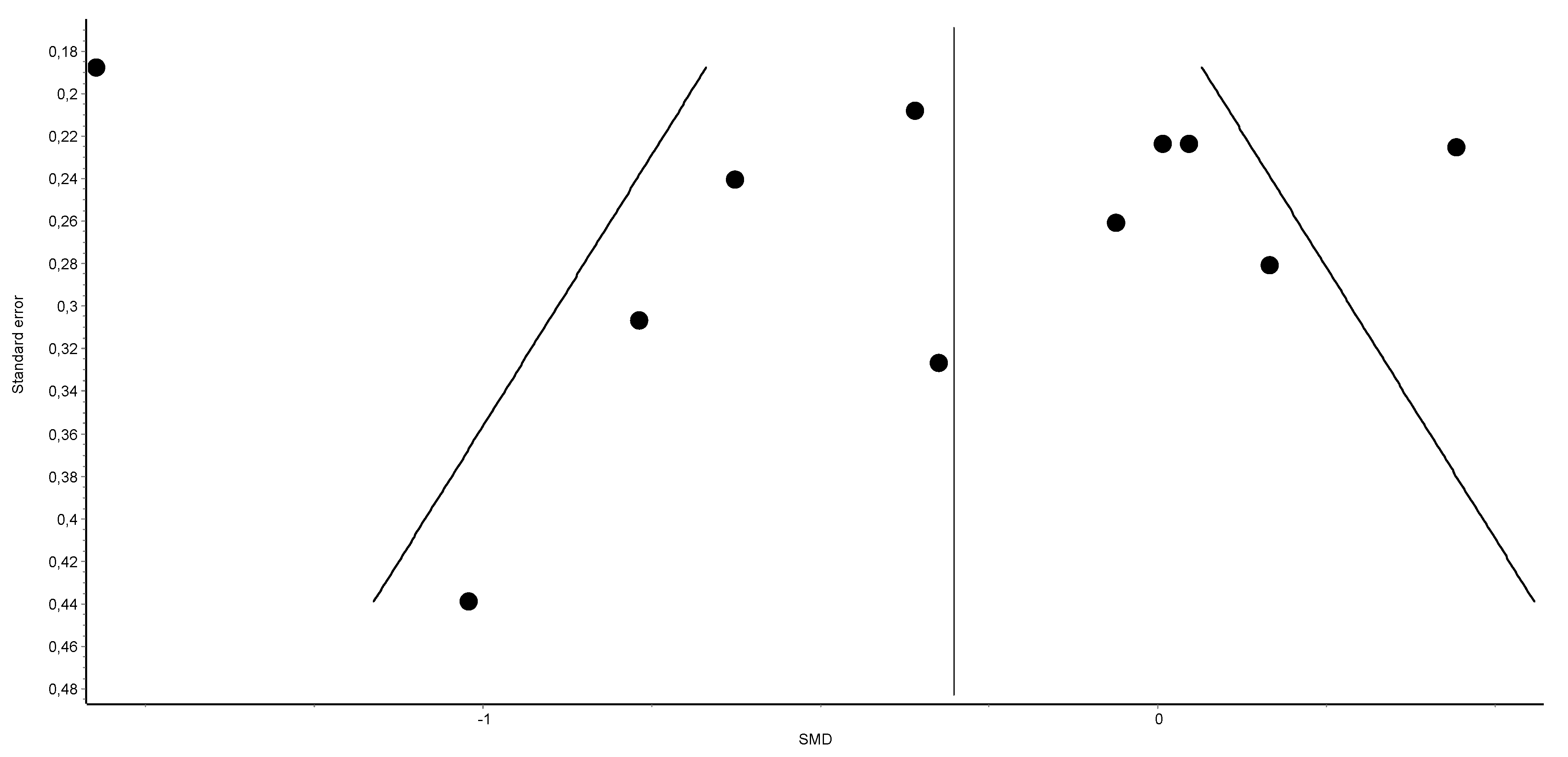
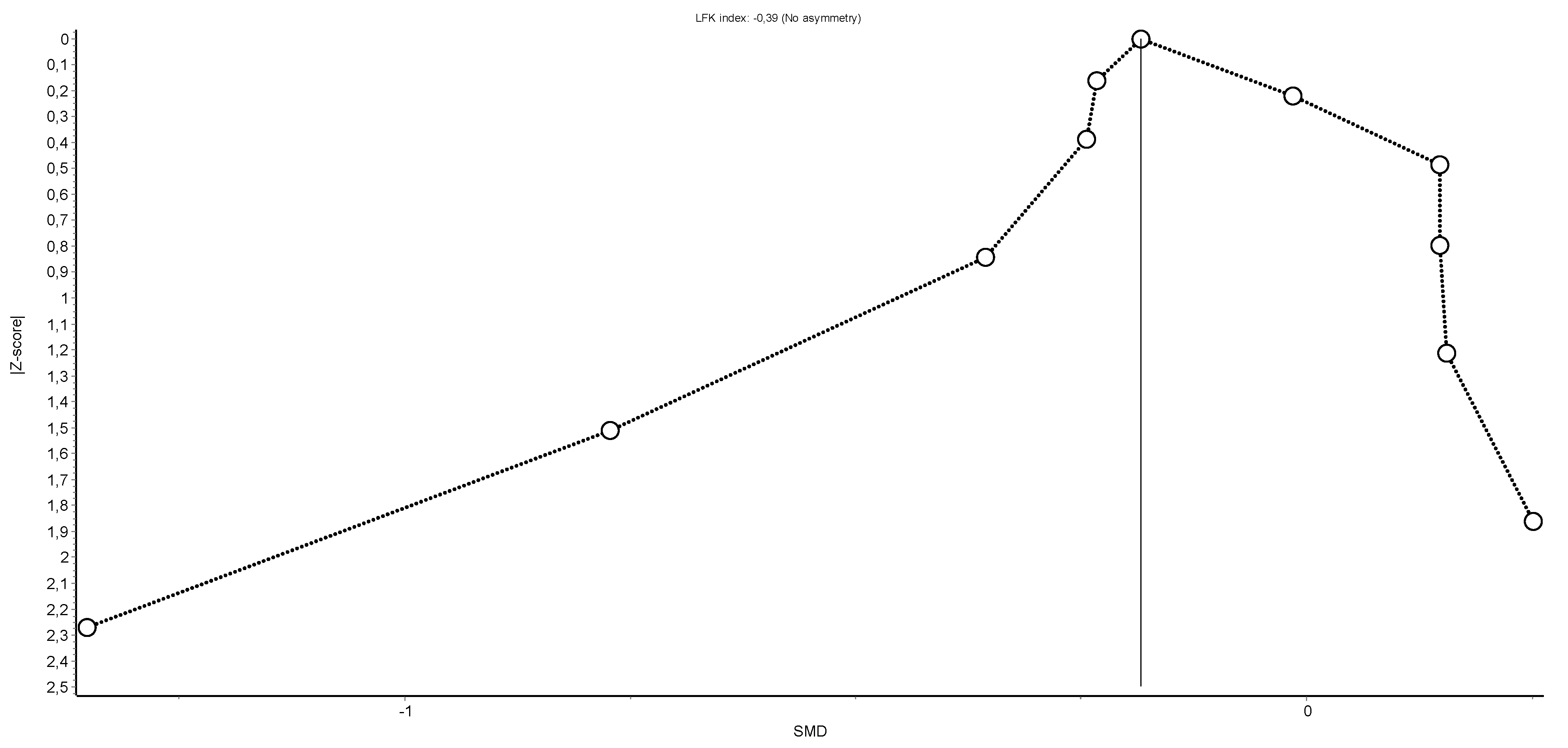
Appendix A.4. Synthesis Funnel Plot and Doi Plot (LFK Index) for Maximal Expiratory Pressure Variable: Funnel Plot Aims to Assess the Existence of Publication Bias


Appendix A.5. Sensitivity Exclusion Analysis for Maximal Expiratory Pressure Variable

Appendix A.6. Synthesis Funnel Plot and Doi Plot (LFK Index) for Maximum Voluntary Ventilation Variable: Funnel Plot Aims to Assess the Existence of Publication Bias


Appendix A.7. Sensitivity Exclusion Analysis for Maximum Voluntary Ventilation Variable

Appendix A.8. Synthesis Funnel Plot and Doi Plot (LFK Index) for Forced Vital Capacity Variable: Funnel Plot Aims to Assess the Existence of Publication Bias


Appendix A.9. Synthesis Funnel Plot and Doi Plot (LFK Index) for Forced Expiratory Volume during the First Second


References
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.S.; McGee, S.J. Pain as a global public health priority. BMC Public Health 2011, 11, 770. [Google Scholar] [CrossRef] [PubMed]
- St. Sauver, J.L.; Warner, D.O.; Yawn, B.P.; Jacobson, D.J.; McGree, M.E.; Pankratz, J.J.; Melton, L.J.; Roger, V.L.; Ebbert, J.O.; Rocca, W.A. Why Patients Visit Their Doctors: Assessing the Most Prevalent Conditions in a Defined American Population. Mayo Clin. Proc. 2013, 88, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Nahin, R.L. Estimates of pain prevalence and severity in adults: United States, 2012. J. Pain 2015, 16, 769–780. [Google Scholar] [CrossRef]
- Sharon, H.; Greener, H.; Hochberg, U.; Brill, S. The Prevalence of Chronic Pain in the Adult Population in Israel: An Internet-Based Survey. Pain Res. Manag. 2022, 2022, 3903720. [Google Scholar] [CrossRef]
- Steglitz, J.; Buscemi, J.; Ferguson, M.J. The future of pain research, education, and treatment: A summary of the IOM report “Relieving pain in America: A blueprint for transforming prevention, care, education, and research”. Transl. Behav. Med. 2012, 2, 6–8. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef]
- Apkarian, A.V.; Hashmi, J.A.; Baliki, M.N. Pain and the brain: Specificity and plasticity of the brain in clinical chronic pain. Pain 2011, 152, S49–S64. [Google Scholar] [CrossRef]
- Voscopoulos, C.; Lema, M. When does acute pain become chronic? Br. J. Anaesth. 2010, 105 (Suppl. S1), i69–i85. [Google Scholar] [CrossRef]
- Neumann, S.; Doubell, T.P.; Leslie, T.; Woolf, C.J. Inflammatory pain hypersensitivity mediated by phenotypic switch in myelinated primary sensory neurons. Nature 1996, 384, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Raecke, R.; Niemeier, A.; Ihle, K.; Ruether, W.; May, A. Brain Gray Matter Decrease in Chronic Pain Is the Consequence and Not the Cause of Pain. J. Neurosci. 2009, 29, 13746. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, J.A.; Baliki, M.N.; Huang, L.; Baria, A.T.; Torbey, S.; Hermann, K.M.; Schnitzer, T.J.; Apkarian, A.V. Shape shifting pain: Chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain 2013, 136, 2751–2768. [Google Scholar] [CrossRef]
- Dimitriadis, Z.; Kapreli, E.; Strimpakos, N.; Oldham, J. Respiratory dysfunction in patients with chronic neck pain: What is the current evidence? J. Bodyw. Mov. Ther. 2016, 20, 704–714. [Google Scholar] [CrossRef]
- López-de-Uralde-Villanueva, I.; del Corral, T.; Salvador-Sánchez, R.; Angulo-Díaz-Parreño, S.; López-Marcos, J.J.; Plaza-Manzano, G. Respiratory dysfunction in patients with chronic neck pain: Systematic review and meta-analysis. Disabil. Rehabil. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Rubio, A.; Torres-Sánchez, I.; Cabrera-Martos, I.; López-López, L.; Rodríguez-Torres, J.; Granados-Santiago, M.; Valenza, M.C. Respiratory disturbances in fibromyalgia: A systematic review and meta-analysis of case control studies. Expert Rev. Respir. Med. 2021, 15, 1217–1227. [Google Scholar] [CrossRef]
- Abdollahzadeh, Z.; Abbasi, H. Altered Respiratory Function in Patients with Low Back Pain: A Review Article. J. Mod. Rehabil. 2021, 15, 55–62. [Google Scholar] [CrossRef]
- Kahlaee, A.H.; Ghamkhar, L.; Arab, A.M. The Association between Neck Pain and Pulmonary Function: A Systematic Review. Am. J. Phys. Med. Rehabil. 2017, 96, 203–210. [Google Scholar] [CrossRef]
- Beeckmans, N.; Vermeersch, A.; Lysens, R.; Van Wambeke, P.; Goossens, N.; Thys, T.; Brumagne, S.; Janssens, L. The presence of respiratory disorders in individuals with low back pain: A systematic review. Man. Ther. 2016, 26, 77–86. [Google Scholar] [CrossRef]
- Bougioukas, K.I.; Liakos, A.; Tsapas, A.; Ntzani, E.; Haidich, A.B. Preferred reporting items for overviews of systematic reviews including harms checklist: A pilot tool to be used for balanced reporting of benefits and harms. J. Clin. Epidemiol. 2018, 93, 9–24. [Google Scholar] [CrossRef]
- Moher, D.; Pham, B.; Jones, A.; Cook, D.J.; Jadad, A.R.; Moher, M.; Tugwell, P.; Klassen, T.P. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet 1998, 352, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Barton, C.J.; Webster, K.E.; Menz, H.B. Evaluation of the scope and quality of systematic reviews on nonpharmacological conservative treatment for patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 2008, 38, 529–541. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Medica 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Tennant, B.; Ribeiro-Lucas, I.; Vaux-Bjerke, A.; Piercy, K.; Bloodgood, B. Umbrella and systematic review methodology to support the 2018 physical activity guidelines advisory committee. J. Phys. Act. Health 2018, 15, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Barendregt, J.J.; Doi, S.A. MetaXL User Guide, Version 5.3; EpiGear International Pty Ltd.: Sunrise Beach, QLD, Australia, 2016.
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.A. Rendering the Doi plot properly in meta-analysis. Int. J. Evid. Based. Healthc. 2018, 16, 242–243. [Google Scholar] [CrossRef] [PubMed]
- Furuya-Kanamori, L.; Barendregt, J.J.; Doi, S.A.R. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 195–203. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Cheon, J.H.; Lim, N.N.; Lee, G.S.; Won, K.H.; Lee, S.H.; Kang, E.Y.; Lee, H.K.; Cho, Y. Differences of Spinal Curvature, Thoracic Mobility, and Respiratory Strength between Chronic Neck Pain Patients and People without Cervical Pain. Ann. Rehabil. Med. 2020, 44, 58. [Google Scholar] [CrossRef]
- Borisut, S.; Tantisuwat, A.; Gaogasigam, C. The study of respiratory muscles activation during respiratory muscle strength effort in adult females with chronic neck pain. J. Phys. Ther. Sci. 2021, 33, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, Z.; Kapreli, E.; Strimpakos, N.; Oldham, J. Respiratory weakness in patients with chronic neck pain. Man. Ther. 2013, 18, 248–253. [Google Scholar] [CrossRef]
- Kapreli, E.; Vourazanis, E.; Billis, E.; Oldham, J.A.; Strimpakos, N. Respiratory dysfunction in chronic neck pain patients. A pilot study. Cephalalgia 2009, 29, 701–710. [Google Scholar] [CrossRef]
- López-de-Uralde-Villanueva, I.; Sollano-Vallez, E.; Del Corral, T. Reduction of cervical and respiratory muscle strength in patients with chronic nonspecific neck pain and having moderate to severe disability. Disabil. Rehabil. 2017, 40, 2495–2504. [Google Scholar] [CrossRef] [PubMed]
- Moawd, S.; Ali, S.E. Effect of Over-Usage of Smart Phone in a Non-Neutral Neck Position on Respiratory Function in Female Adults. Int. J. Ther. Rehabil. Res. 2015, 4, 104. [Google Scholar] [CrossRef]
- Wirth, B.; Amstalden, M.; Perk, M.; Boutellier, U.; Humphreys, B.K. Respiratory dysfunction in patients with chronic neck pain—Influence of thoracic spine and chest mobility. Man. Ther. 2014, 19, 440–444. [Google Scholar] [CrossRef]
- Yalcinkaya, H.; Ucok, K.; Ulasli, A.M.; Coban, N.F.; Aydin, S.; Kaya, I.; Akkan, G.; Tugrul Senay, T. Do male and female patients with chronic neck pain really have different health-related physical fitness, depression, anxiety and quality of life parameters? Int. J. Rheum. Dis. 2017, 20, 1079–1087. [Google Scholar] [CrossRef]
- Çetin, A.; Sivri, A. Respiratory function and dyspnea in fibromyalgia syndrome. J. Musculoskelet. Pain 2001, 9, 7–15. [Google Scholar] [CrossRef]
- Forti, M.; Zamunér, A.R.; Andrade, C.P.; Silva, E. Lung Function, Respiratory Muscle Strength, and Thoracoabdominal Mobility in Women with Fibromyalgia Syndrome. Respir. Care 2016, 61, 1384–1390. [Google Scholar] [CrossRef]
- Şahin, G.; Ulubaş, B.; Çalikoǧlu, M.; Çime, Ö.B.; Erdoǧan, C. Is chest expansion a determinant of pulmonary muscle strength in primary fibromyalgia? Jt. Bone Spine 2004, 71, 140–143. [Google Scholar] [CrossRef]
- Şahin, G.; Ulubaş, B.; Çalikoǧlu, M.; Erdoǧan, C. Handgrip Strength, Pulmonary Function Tests, and Pulmonary Muscle Strength in Fibromyalgia Syndrome: Is There Any Relationship? South. Med. J. 2004, 97, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Ozgocmen, S.; Cimen, O.B.; Ardicoglu, O. Relationship between Chest Expansion and Respiratory Muscle Strength in Patients with Primary Fibromyalgia. Clin. Rheumatol. 2002, 21, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.G.; Choezom, T.; Prabu Raja, G. Comparison of respiratory parameters in participants with and without chronic low back pain. J. Bodyw. Mov. Ther. 2019, 23, 894–900. [Google Scholar] [CrossRef]
- Mohan, V.; Paungmali, A.; Sitilerpisan, P.; Hashim, U.F.; Mazlan, M.B.; Nasuha, T.N. Respiratory characteristics of individuals with non-specific low back pain: A cross-sectional study. Nurs. Health Sci. 2018, 20, 224–230. [Google Scholar] [CrossRef]
- Falla, D. Unravelling the complexity of muscle impairment in chronic neck pain. Man. Ther. 2004, 9, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Van Dieën, J.H.; Peter Reeves, N.; Kawchuk, G.; Van Dillen, L.R.; Hodges, P.W. Analysis of Motor Control in Patients with Low Back Pain: A Key to Personalized Care? J. Orthop. Sports Phys. Ther. 2019, 49, 380. [Google Scholar] [CrossRef]
- O’sullivan, P. Diagnosis and classification of chronic low back pain disorders: Maladaptive movement and motor control impairments as underlying mechanism. Man. Ther. 2005, 10, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Jull, G.; Falla, D. Does increased superficial neck flexor activity in the craniocervical flexion test reflect reduced deep flexor activity in people with neck pain? Man. Ther. 2016, 25, 43–47. [Google Scholar] [CrossRef]
- Falla, D.; Jull, G.; Edwards, S.; Koh, K.; Rainoldi, A. Neuromuscular efficiency of the sternocleidomastoid and anterior scalene muscles in patients with chronic neck pain. Disabil. Rehabil. 2009, 26, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Ruhe, A.; Fejer, R.; Walker, B. Center of pressure excursion as a measure of balance performance in patients with non-specific low back pain compared to healthy controls: A systematic review of the literature. Eur. Spine J. 2011, 20, 358–368. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm. J. Appl. Physiol. 2000, 89, 967–976. [Google Scholar] [CrossRef]
- Janssens, L.; Brumagne, S.; McConnell, A.K.; Hermans, G.; Troosters, T.; Gayan-Ramirez, G. Greater diaphragm fatigability in individuals with recurrent low back pain. Respir. Physiol. Neurobiol. 2013, 188, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Kolář, P.; Šulc, J.; Kynčl, M.; Šanda, J.; Čakrt, O.; Andel, R.; Kumagai, K.; Kobesová, A. Postural function of the diaphragm in persons with and without chronic low back pain. J. Orthop. Sports Phys. Ther. 2012, 42, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- Jonsson, K.; Peterson, M. Peak expiratory flow rate and thoracic mobility in people with fibromyalgia. A cross sectional study. Scand. J. Pain 2019, 19, 755–763. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Studies k (n) Types | Meta-Analysis (k) | Population | Variables | Outcomes (Test) | Author’s Conclusions |
|---|---|---|---|---|---|---|
| López-de-Uralde-Villanueva et al. [15] | 11 OSs (929) | Yes (10) | -Patients with CNP -HC | -Pulmonary function (VC, MVV, FVC, FEV1, FEV1/FVC, FEV25–75, and PEF) -Respiratory muscle strength (MIP and MEP) | -Pulmonary function (spirometry test) -Respiratory muscle strength (portable mouth pressure meter) | Patients with CNP have reduced respiratory muscle strength and pulmonary function compared with HC. |
| Ortiz-Rubio et al. [16] | Seven OSs (504) | Yes (6) | -Patients with FMS -HC | -Pulmonary function (MVV, FVC, and FEV1) -Respiratory muscle strength (MIP and MEP) | -Pulmonary function (spirometry test) -Respiratory muscle strength (digital mouth pressure meter) | Patients with FMS experience respiratory disturbances in comparison with HC. |
| Abdollahzadeh and Abbasi [17] | Seven OSs (N/R) | No | -Patients with CLBP -HC | -Pulmonary function (MVV) -Respiratory muscle strength (MIP and MEP) | -Pulmonary function (spirometry test) -Respiratory muscle strength (portable mouth pressure meter) | A sub-optimal respiratory function was found in patients with CLBP. |
| Hossein-Kahlaee et al. [18] | Nine OSs (585) | No | -Patients with CNP -HC | -Pulmonary function (VC, MVV, FVC, FEV1, FEV1/FVC, and PEF) -Respiratory muscle strength (MIP and MEP) | -Pulmonary function (spirometry test) -Respiratory muscle strength (portable mouth pressure meter) | Patients with CNP have reduced respiratory muscle strength and pulmonary function compared with HC. |
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| López-de-Uralde-Villanueva [15] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 25 |
| Ortiz-Rubio et al. [16] | 2 | 2 | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 1 | 22 |
| Abdollahzadeh and Abbasi [17] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 0 | 15 |
| Hossein-Kahlaee et al. [18] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 0 | 18 |
| Study | Phase 2 | Phase 3 | |||
|---|---|---|---|---|---|
| Study Eligibility Criteria | Identification and Selection of Studies | Data Collection and Study Appraisal | Synthesis and Findings | Risk of Bias in the Review | |
| López-de-Uralde-Villanueva [15] |  | | | | |
| Ortiz-Rubio et al. [16] | | | | | |
| Abdollahzadeh and Abbasi [17] |  | | | | |
| Hossein-Kahlaee et al. [18] | | | | | |
: low risk. : high risk.| 2018 Physical Activity Guidelines Advisory Committee Grading Criteria | Grade | |||||
|---|---|---|---|---|---|---|
| Systematic Review Research Questions | Applicability | Generalizability | Risk of bias or study limitations | Quantity and consistency | Magnitude and precision of effect | |
| MIP | Strong | Limited | Moderate | Moderate | −0.70 (−1.03 to −0.38) | Moderate |
| MEP | Strong | Limited | Moderate | Moderate | −0.70 (−0.97 to −0.42) | Moderate |
| VC | Strong | Limited | Moderate | Limited | Not assignable | Limited |
| MVV | Strong | Limited | Moderate | Limited | −0.58 (−0.82 to −0.34) | Limited |
| FVC | Strong | Limited | Moderate | Moderate | −0.29 (−0.68 to 0.10) | Moderate |
| FEV1 | Strong | Limited | Moderate | Moderate | −0.17 (−0.38 to 0.005) | Moderate |
| FEV1/FVC | Strong | Limited | Moderate | Limited | Not assignable | Limited |
| FEV25–75 | Strong | Limited | Moderate | Limited | Not assignable | Limited |
| PEF | Strong | Limited | Moderate | Limited | Not assignable | Limited |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuenca-Martínez, F.; Sempere-Rubio, N.; Muñoz-Gómez, E.; Mollà-Casanova, S.; Carrasco-González, E.; Martínez-Arnau, F.M. Respiratory Function Analysis in Patients with Chronic Pain: An Umbrella Review and Meta-Analysis of Pooled Findings. Healthcare 2023, 11, 1358. https://doi.org/10.3390/healthcare11091358
Cuenca-Martínez F, Sempere-Rubio N, Muñoz-Gómez E, Mollà-Casanova S, Carrasco-González E, Martínez-Arnau FM. Respiratory Function Analysis in Patients with Chronic Pain: An Umbrella Review and Meta-Analysis of Pooled Findings. Healthcare. 2023; 11(9):1358. https://doi.org/10.3390/healthcare11091358
Chicago/Turabian StyleCuenca-Martínez, Ferran, Núria Sempere-Rubio, Elena Muñoz-Gómez, Sara Mollà-Casanova, Enrique Carrasco-González, and Francisco M. Martínez-Arnau. 2023. "Respiratory Function Analysis in Patients with Chronic Pain: An Umbrella Review and Meta-Analysis of Pooled Findings" Healthcare 11, no. 9: 1358. https://doi.org/10.3390/healthcare11091358