

Spiritual Needs of Older Adults Living with Dementia: An Integrative Review
 , and
, and
Abstract
:1. Introduction
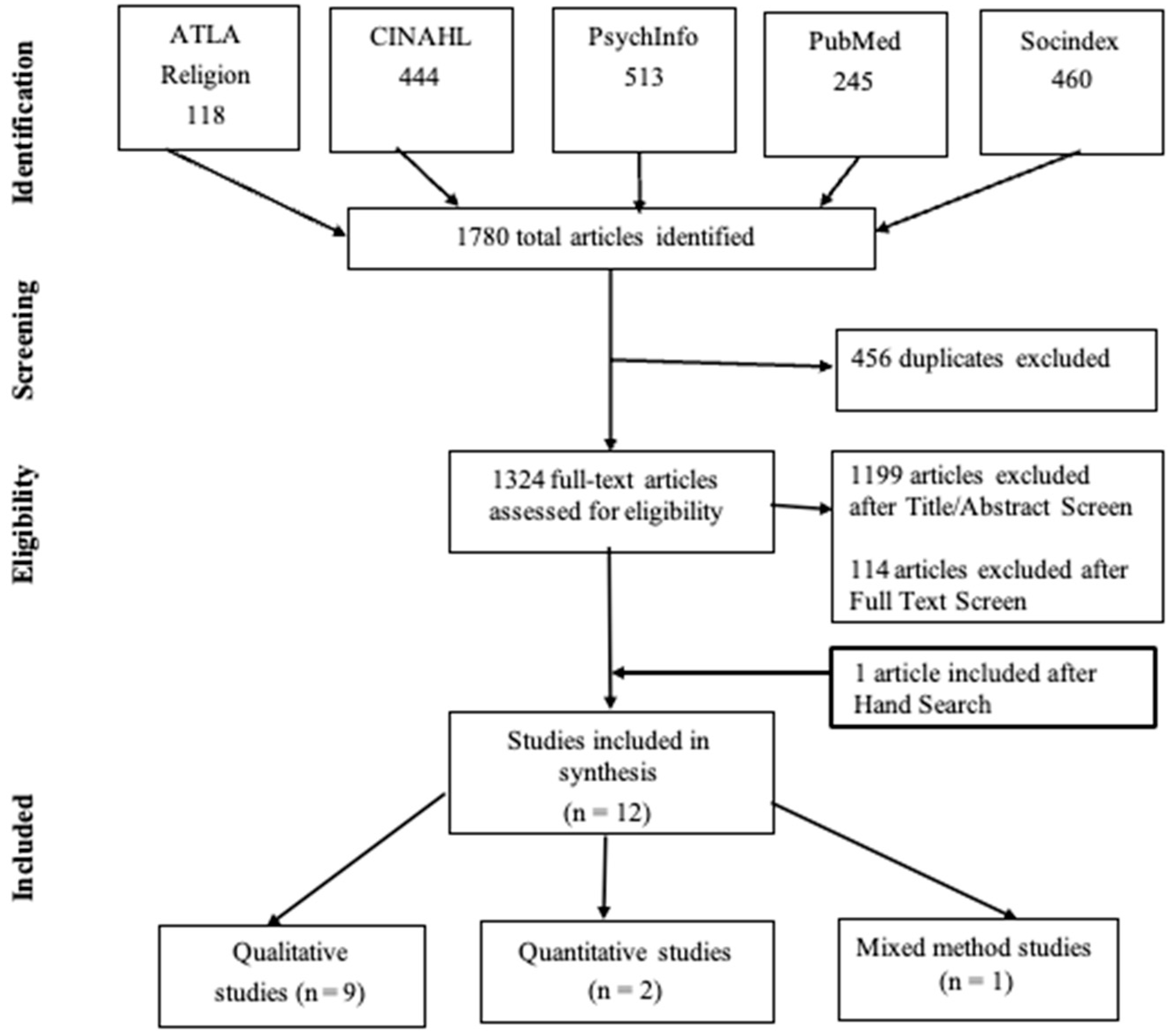
2. Materials and Methods
2.1. Study Design and Population
2.2. Search Strategy
2.3. Inclusion/Exclusion Criteria
2.4. Data Extraction
2.5. Methodological Quality
3. Summary of Findings
3.1. Thematic Domains
3.1.1. Characterizing Spiritual Needs, Preferences, Resources, Approaches, and Support
In Residents with Dementia, Family, Nursing Home Staff
In Residents with Dementia
In Nurses
3.1.2. Characterizing Spiritual Care and Support
In Clergy
3.1.3. Meaning of Spiritual Care
In Residents with Dementia, Family, and Staff
3.1.4. Assessing Spiritual Care Interventions + Support
- In Residents with dementia: Aloustani et al. [48] conducted a randomized control trial to investigate the effect of group spiritual therapy on the cognitive state of 50 older adults aged 60 with mild dementia. The result reported that group spiritual therapy, as a low-cost intervention, significantly enhanced the cognitive state in older adults (p < 0.01) over two weeks.
- In others: Connelly and Moss [49] examined whether music is useful for accessing spiritual needs and providing meaningful spiritual support for PLwDs. This qualitative study (n = 4) utilizing interpretative phenomenological analysis (IPA) explored the experiences of music therapists and chaplains working with PLwDs in hospitals. Authors identified five emerging themes from their analysis: (1) music can facilitate spiritual expression; (2) spirituality is necessarily a broad and evolving term; (3) spirituality may be a coping mechanism for PLwD; (4) music therapy contributes to validating the individuality of PLwD; and (5) collaborative work between music therapy and pastoral care is worthy of further exploration.
- In nurses: Of importance are the perspectives of healthcare workers who provide direct care to PLwDs. Palmer et al. [50] interviewed healthcare providers (n = 24) with no religious affiliation providing direct care to patients with dementia from Boston, M.A. (i.e., chaplains, nursing staff, social workers, and activities professionals) to gain insight into the spiritual needs of PLwDs. Findings suggest that loss of cognitive capacity may impact older adults’ ability to access faith in dementia, often leading to anxiety, spiritual distress, and frustration. However, there is the possibility that spiritual intervention at the mild stage of dementia may mitigate spiritual needs in severe dementia, per the providers.
3.1.5. Predicting Spiritual Care Provision
In Providers
4. Discussion
4.1. Characterizing Spiritual Needs
4.2. Addressing Spiritual Needs through Spiritual Care
4.3. Spiritual Care Barriers to Addressing Spiritual Needs
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 13 September 2022).
- World Health Organization. Available online: https://www.who.int/news/item/02-09-2021-world-failing-to-address-dementia-challenge (accessed on 13 September 2022).
- Perkins, C.; Egan, R.; Llewellyn, R.; Peterken, B. Still living, loving, and laughing: Spiritual life in the dementia unit. J. Relig. Spirit. Aging 2015, 27, 270–287. [Google Scholar] [CrossRef]
- Camacho-Montaño, L.R.; Pérez-Corrales, J.; Pérez-de-Heredia-Torres, M.; Martin-Pérez, A.M.; Güeita-Rodríguez, J.; Velarde-García, J.F.; Palacios-Ceña, D. Spiritual care in advanced dementia from the perspective of health providers: A qualitative systematic review. Occup. Ther. Int. 2021, 2021, 9998480. [Google Scholar] [CrossRef] [PubMed]
- Bursell, J.; Mayers, C.A. Spirituality within dementia care: Perceptions of health professionals. Br. J. Occup. Ther. 2010, 73, 144–151. [Google Scholar] [CrossRef]
- Lavretsky, H. Spirituality and aging. Aging Health 2010, 6, 749–769. [Google Scholar] [CrossRef]
- Rote, S.; Hill, T.D.; Ellison, C.G. Religious attendance and loneliness in later life. Gerontologist 2013, 53, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Manning, L.K. Navigating hardships in old age: Exploring the relationship between spirituality and resilience in later life. Qual. Health Res. 2013, 23, 568–575. [Google Scholar] [CrossRef]
- Agli, O.; Bailly, N.; Ferrand, C. Spirituality and religion in older adults with dementia: A systematic review. Int. Psychogeriatr. 2015, 27, 715–725. [Google Scholar] [CrossRef]
- Balboni, T.A.; VanderWeele, T.J.; Doan-Soares, S.D.; Long, K.N.G.; Ferrell, B.R.; Fitchett, G.; Koenig, H.G.; Bain, P.A.; Puchalski, C.; Steinhauser, K.E.; et al. Spirituality in serious illness and health. JAMA 2022, 328, 184–197. [Google Scholar] [CrossRef]
- Malone, J.; Dadswell, A. The role of religion, spirituality and/or Belief in positive ageing for older adults. Geriatrics 2018, 3, 28. [Google Scholar] [CrossRef]
- Balboni, T.A.; Vanderwerker, L.C.; Block, S.D.; Paulk, M.E.; Lathan, C.S.; Peteet, J.R.; Prigerson, H.G. Religiousness and spiritual support among advanced cancer patients and associations with end-of-life treatment preferences and quality of life. J. Clin. Oncol. 2007, 25, 555–560. [Google Scholar] [CrossRef]
- Koenig, H.G.; King, D.E.; Carson, V.B. Handbook of Religion and Health, 2nd ed.; Oxford University Press: Oxford, UK, 2012; pp. 1–1137. [Google Scholar]
- Koenig, H.G. Religion, spirituality, and health: A review and update. Adv. Mind Body Med. 2015, 29, 19–26. [Google Scholar] [PubMed]
- Puchalski, C.M.; Vitillo, R.; Hull, S.K.; Reller, N. Improving the spiritual dimension of whole person care: Reaching national and international consensus. J. Palliat. Med. 2014, 17, 642–656. [Google Scholar] [CrossRef]
- Delgado-Guay, M.O. Spirituality and religiosity in supportive and palliative care. Curr. Opin. Support. Palliat. Care 2014, 8, 308–313. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Definition of Palliative Care. Available online: http://www.who.int/cancer/palliative/definition/en (accessed on 30 December 2018).
- Balboni, M.J.; Sullivan, A.; Amobi, A.; Phelps, A.C.; Gorman, D.P.; Zollfrank, A.; Peteet, J.R.; Prigerson, H.G.; Vanderweele, T.J.; Balboni, T.A. Why is spiritual care infrequent at the end of life? Spiritual care perceptions among patients, nurses, and physicians and the role of training. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Gijsberts, M.H.E.; Liefbroer, A.I.; Otten, R.; Olsman, E. Spiritual Care in Palliative Care: A Systematic Review of the Recent European Literature. Med. Sci. 2019, 7, 25. [Google Scholar] [CrossRef]
- Yousefi, H.; Abedi, H.A. Spiritual care in hospitalized patients. Iran. J. Nurs. Midwifery Res. 2011, 16, 125–132. [Google Scholar]
- Britt, K.C.; Acton, G. Exploring the meaning of spirituality and spiritual care with help from Viktor Frankl. J. Holist. Nurs. 2022, 40, 46–55. [Google Scholar] [CrossRef]
- Hatamipour, K.; Rassouli, M.; Yaghmaie, F.; Zendedel, K.; Majd, H.A. Spiritual needs of cancer patients: A qualitative study. Indian J. Palliat. Care 2015, 21, 61–67. [Google Scholar]
- Britt, K.C.; Kwak, J.; Acton, G.; Richards, K.C.; Hamilton, J.; Radhakrishnan, K. Measures of religion and spirituality in dementia: An integrative review. Alzheimers Dement. 2022, 8, e12352. [Google Scholar] [CrossRef]
- Beuscher, L.; Beck, C. A literature review of spirituality in coping with early-stage Alzheimer’s disease. J. Clin. Nurs. 2008, 17, 88–97. [Google Scholar] [CrossRef]
- Beuscher, L.; Grando, V.T. Using spirituality to cope with early-stage Alzheimer’s disease. West J. Nurs. Res. 2009, 31, 583–598. [Google Scholar] [CrossRef] [PubMed]
- Jolley, D.; Benbow, S.M.; Grizzell, M.; Willmott, S.; Bawn, S.; Kingston, P. Spirituality and faith in dementia. Dementia 2010, 9, 311–325. [Google Scholar] [CrossRef]
- Daly, L.; McCarron, M.; Higgins, A.; McCallion, P. “Sustaining place”—A grounded theory of how informal carers of people with dementia manage alterations to relationships within their social worlds. J. Clin. Nurs. 2013, 22, 501–512. [Google Scholar] [CrossRef] [PubMed]
- van der Steen, J.T.; Radbruch, L.; Hertogh, C.M.; de Boer, M.E.; Hughes, J.C.; Larkin, P.; Francke, A.L.; Jünger, S.; Gove, D.; Firth, P.; et al. White paper defining optimal palliative care in older people with dementia: A Delphi study and recommendations from the European Association for Palliative Care. Palliat. Med. 2014, 28, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Durepos, P.; Wickson-Griffiths, A.; Hazzan, A.A.; Kaasalainen, S.; Vastis, V.; Battistella, L.; Papaioannou, A. Assessing palliative care content in dementia care guidelines: A systematic review. J. Pain Symptom Manag. 2017, 53, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Gijsberts, M.J.; van der Steen, J.T.; Muller, M.T.; Hertogh, C.M.; Deliens, L. Spiritual end-of-life care in Dutch nursing homes: An ethnographic study. J. Am. Med. Dir. Assoc. 2013, 14, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Daly, L.; Fahey-McCarthy, E. Attending to the spiritual in dementia care nursing. Br. J. Nurs. 2014, 23, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Puchalski, C.M. Spirituality in the cancer trajectory. Ann. Oncol. 2012, 23, iii49–iii55. [Google Scholar] [CrossRef]
- Jafari, N.; Farajzadegan, Z.; Zamani, A.; Bahrami, F.; Emami, H.; Loghmani, A. Spiritual well-being and quality of life in Iranian women with breast cancer undergoing radiation therapy. Support. Care Cancer 2013, 21, 1219–1225. [Google Scholar] [CrossRef]
- Delgado-Guay, M.O.; Chisholm, G.; Williams, J.; Frisbee-Hume, S.; Ferguson, A.O.; Bruera, E. Frequency, intensity, and correlates of spiritual pain in advanced cancer patients assessed in a supportive/palliative care clinic. Palliat. Support. Care 2016, 14, 341–348. [Google Scholar] [CrossRef]
- Salsman, J.M.; Pustejovsky, J.E.; Jim, H.S.; Munoz, A.R.; Merluzzi, T.V.; Park, C.L.; Danhauer, S.C.; Sherman, A.C.; Snyder, M.A.; Fitchett, G. A metanalytic approach to examining the correlation between religion/spirituality and mental health in cancer. Cancer 2015, 121, 3769–3778. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Zwingmann, C.; Klein, C.; Büssing, A. Measuring religiosity/spirituality: Theoretical differentiations and categorization of instruments. Religions 2011, 2, 345–357. [Google Scholar] [CrossRef]
- Palmer, J.A.; Smith, A.M.; Paasche-Orlow, R.S.; Fitchett, G. Research literature on the intersection of dementia, spirituality, and palliative care: A scoping review. J. Pain Symptom Manag. 2020, 60, 116–134. [Google Scholar] [CrossRef]
- Schmidt, H.; Eisenmann, Y.; Golla, H.; Voltz, R.; Perrar, K.M. Needs of people with advanced dementia in their final phase of life: A multi-perspective qualitative study in nursing homes. Palliat. Med. 2018, 32, 657–667. [Google Scholar] [CrossRef]
- Powers, B.A.; Watson, N.M. Spiritual nurturance and support for nursing home residents with dementia. Dementia 2011, 10, 59–80. [Google Scholar] [CrossRef]
- Chen, H.C.; Chan, S.W.; Yeh, T.P.; Huang, Y.H.; Chien, I.C.; Ma, W.F. The spiritual needs of community-dwelling older people living with early-stage dementia-a qualitative study. J. Nurs. Scholarsh. 2019, 51, 157–167. [Google Scholar] [CrossRef]
- Balqis, U.M.; Sahar, J.; Fitriyani, P. Older people with dementia experiences in receiving holistic support in long-term care institution: A phenomenology study. Enferm. Clin. 2021, 31, 78–81. [Google Scholar] [CrossRef]
- Toivonen, K.; Charalambous, A.; Suhonen, R. Supporting the spirituality of older people living with dementia in nursing care: A hermeneutic phenomenological inquiry into older people’s and their family members’ experiences. Int. J. Older People Nurs. 2023, 18, e12514. [Google Scholar] [CrossRef]
- Toivonen, K.; Charalambous, A.; Suhonen, R. Supporting spirituality in the care of older people living with dementia: A hermeneutic phenomenological inquiry into nurses’ experiences. Scand. J. Caring Sci. 2018, 32, 880–888. [Google Scholar] [CrossRef]
- Tomkins, C.J.; Sorrell, J.M. Older adults with Alzheimer’s disease in a faith community. Aging Matters 2008, 46, 22–25. [Google Scholar]
- Carr, T.J.; Hicks-Moore, S.; Montgomery, P. What’s so big about the ‘little things’: A phenomenological inquiry into the meaning of spiritual care in dementia. Dementia 2011, 10, 399–414. [Google Scholar] [CrossRef]
- Aloustani, S.; Hajibeglo, A.; Yazarlo, M.; Gharrehtapeh, S.R. The effect of religion therapy on the elderly cognitive status. J. Relig. Health 2021, 60, 2066–2076. [Google Scholar] [CrossRef] [PubMed]
- Connolly, L.; Moss, H. Music, spirituality and dementia: Exploring joint working between pastoral care professionals and music therapists to improve person-centered care for people with dementia. Dementia 2021, 20, 373–380. [Google Scholar] [CrossRef]
- Palmer, J.A.; Hilgeman, M.; Balboni, T.; Paasche-Orlow, S.; Sullivan, J.L. The spiritual experience of dementia from the health care provider perspective: Implications for intervention. Gerontologist 2022, 62, 556–567. [Google Scholar] [CrossRef]
- van der Steen, J.T.; Gijsberts, M.J.H.; Hertogh, C.M.; Deliens, L. Predictors of spiritual care provision for patients with dementia at the end of life as perceived by physicians: A prospective study. BMC Palliat. Care 2014, 13, 61. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool. (MMAT) Version 2018: User Guide; Department of Family Medicine, McGill University: Montreal, QC, Canada, 2018. [Google Scholar]
- Charavet, C.; Vives, F.; Aroca, S.; Dridi, S.M. “Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature. Healthcare 2022, 10, 379. [Google Scholar] [CrossRef]
- Ulley, J.; Harrop, D.; Ali, A.; Alton, S.; Fowler Davis, S. Deprescribing interventions and their impact on medication adherence in community-dwelling older adults with polypharmacy: A systematic review. BMC Geriatr. 2019, 19, 15. [Google Scholar] [CrossRef]
- Gilligan, C. In a Different Voice: Psychological Theory and Women’s Development; Harvard University Press: Cambridge, MA, USA, 1982. [Google Scholar]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Buckingham, UK, 1997; p. 176. [Google Scholar]
- Smrokowska-Reichmann, A. A senior as an individual in the situation of dementia. Tom Kitwood’s Person-Centred Care Model and the philosophy of dialogue. Nauk. Wychowaniu. Stud. Interdyscyplinarne 2020, 10, 51–61. [Google Scholar] [CrossRef]
- Swinton, J. Re-imagining personhood: Dementia, culture and citizenship. J. Relig. Spiritual. Aging 2021, 33, 172–181. [Google Scholar] [CrossRef]
- Vance, D.E. Procedural and Emotional Religious Activity Therapy. Act. Adapt. Aging 2005, 29, 27–45. [Google Scholar] [CrossRef]
- Puchalski, C.; Ferrell, B.; Delgado-Guay, M.; Blatt, B.; Vandenhoeck, A.; Haythorn, T.; Jacobs, C.; Bauer, R.W. Interprofessional Spiritual Care Education Curriculum. In Proceedings of the George Washington Institute for Spirituality and Health, Washington, DC, USA, 6–7 July 2020. [Google Scholar]
- Balboni, T.A.; Fitchett, G.; Handzo, G.F.; Johnson, K.S.; Koenig, H.G.; Pargament, K.I.; Puchalski, C.M.; Sinclair, S.; Taylor, E.J.; Steinhauser, K.E. State of the science of spirituality and palliative care research part II: Screening, assessment, and interventions. J. Pain Symptom Manag. 2017, 54, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Kevern, P. The spirituality of people with late-stage dementia: A review of the research literature, a critical analysis and some implications for person-centered spirituality and dementia care. Ment. Health Relig. Cult. 2015, 18, 765–776. [Google Scholar] [CrossRef]
- Giannouli, V.; Giannoulis, K. Gazing at Medusa: Alzheimer’s dementia through the lenses of spirituality and religion. Health Psychol. Res. 2020, 8, 8833. [Google Scholar] [CrossRef] [PubMed]
- Britt, K.C.; Richards, K.C.; Radhakrishnan, K.; Vanags-Louredo, A.; Park, E.; Gooneratne, N.S.; Fry, L. Religion, spirituality, and coping during the pandemic: Perspectives of dementia caregivers. Clin. Nurs. Res. 2023, 32, 94–104. [Google Scholar] [CrossRef]
- Simard, J. The End-Of-Life Namaste Program for People with Dementia, 2nd ed.; Health Professions Press: Baltimore, MD, USA; London, UK; Sydney, Australia, 2013; pp. 1–257. [Google Scholar]
- Higgins, P. Meeting the religious needs of residents with dementia. Nurs. Older People 2013, 25, 25–29. [Google Scholar] [CrossRef]
- Livingston, G.; Pitfield, C.; Morris, J.; Manela, M.; Lewis-Holmes, E.; Jacobs, H. Care at the end of life for people with dementia living in a care home: A qualitative study of staff experience and attitudes. Int. J. Geriatr. Psychiatry 2012, 27, 643–650. [Google Scholar] [CrossRef]
- O’Brien, M.R.; Kinloch, K.; Groves, K.E.; Jack, B.A. Meeting patients’ spiritual needs during end-of-life care: A qualitative study of nurses’ and healthcare professionals’ perceptions of spiritual care training. J. Clin. Nurs. 2019, 28, 182–189. [Google Scholar] [CrossRef]
- Brijnath, B.; Croy, S.; Sabates, J.; Thodis, A.; Ellis, S.; de Crespigny, F.; Moxey, A.; Day, R.; Dobson, A.; Elliott, C.; et al. Including ethnic minorities in dementia research: Recommendations from a scoping review. Alzheimers Dement. 2022, 8, e12222. [Google Scholar] [CrossRef]
- Schwalm, F.D.; Zandavalli, R.B.; de Castro Filho, E.D.; Lucchetti, G. Is there a relationship between spirituality/religiosity and resilience? a systematic review and meta-analysis of observational studies. J. Health Psychol. 2022, 27, 1218–1232. [Google Scholar] [CrossRef] [PubMed]
- Crandall, L.G.; White, D.L.; Schuldheis, S.; Talerico, K.A. Initiating person-centered care practices in long-term care facilities. J. Gerontol. Nurs. 2007, 33, 47–56. [Google Scholar] [PubMed]
- Ebrahimi, Z.; Patel, H.; Wijk, H.; Ekman, I.; Olaya-Contreras, P. A systematic review on implementation of person-centered care interventions for older people in out-of-hospital settings. Geriatr. Nurs. 2021, 42, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Van Haitsma, K.; Abbott, K.M.; Arbogast, A.; Bangerter, L.R.; Heid, A.R.; Behrens, L.L.; Madrigal, C. A preference-based model of care: An integrative theoretical model of the role of preferences in person-centered care. Gerontologist 2020, 60, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Kazawa, K.; Kodama, A.; Sugawara, K.; Hayashi, M.; Ota, H.; Son, D.; Ishii, S. Person-centered dementia care during COVID-19: A qualitative case study of impact on and collaborations between caregivers. BMC Geriatr. 2022, 22, 107. [Google Scholar] [CrossRef]
- Lee, K.H.; Lee, J.Y.; Kim, B. Person-centered care in persons living with dementia: A systematic review and meta-analysis. Gerontol. 2022, 62, e253–e264. [Google Scholar] [CrossRef]
- Mast, B.T.; Molony, S.L.; Nicholson, N.; Kate Keefe, C.; DiGasbarro, D. Person-centered assessment of people living with dementia: Review of existing measures. Alzheimers Dement. 2021, 7, e12138. [Google Scholar] [CrossRef]
- Sampson, E.L.; Anderson, J.E.; Candy, B.; Davies, N.; Ellis-Smith, C.; Gola, A.; Evans, C.J. Empowering better end-of-life dementia care (EMBED-Care): A mixed methods protocol to achieve integrated person-centered care across settings. Int. J. Geriatr. Psychiatry 2020, 35, 820–832. [Google Scholar] [CrossRef]
- Frankl, V.E. The Doctor and the Soul: From Psychotherapy to Logotherapy; Vintage Books: New York, NY, USA, 1986. [Google Scholar]


{kind=link}
| Database | Search Strategy |
|---|---|
| ATLA religion | (dementia OR Alzheimers OR cognitive impairment OR memory loss OR Lewy |
| body OR Lewy bodies) AND (needs OR care) | |
| PsychInfo | (dementia OR Alzheimers OR cognitive impairment OR memory loss OR cognitive |
| (decline) AND (spirituality OR spiritual needs OR religious needs OR spiritual care OR existential care OR faith) | |
| CINAHL | (dementia OR Alzheimers OR cognitive impairment OR memory loss OR |
| cognitive decline OR Lewy body OR Lewy bodies) AND (religious needs OR spiritual needs OR spirituality OR spiritual care OR existential care) | |
| PUBMED | (dementia OR memory loss OR Alzheimer OR cognitive decline) AND (spirituality OR spiritual needs OR religious needs OR spiritual care OR existential care OR faith) |
| SOCIndex | (dementia OR Alzheimers OR cognitive impairment OR memory loss OR cognitive |
| decline OR memory) AND (spirituality OR spiritual needs OR religious needs OR spiritual care OR existential care or faith) |
| Authors and Year Published | Study Purpose | Region and Setting | Dementia Type and Stage Evaluated | Study Participants/Data Source | Study Design and Quality Ratings * | Major Relevant Findings |
|---|---|---|---|---|---|---|
| In residents with dementia, family, NH staff | ||||||
| Schmidt et al., 2018 [40] | To identify, recognize and meet needs of older adults with advanced dementia towards end of life | Germany urban and rural, and religious and non-religious nursing homes | Advanced vascular, Alzheimer’s disease, or unspecified dementia GDS = 6–7 and loss of verbal communication ability | Health professionals (N = 41) working with advanced dementia residents (i.e., caregivers, providers, housekeepers, and others) | Qualitative Grounded theory Semi-structured group discussions, interviews, and observations 5/5 rating | Spiritual needs are religious needs Spiritual needs, either individual or communal: (1) religious expressing, (2) participating in religious rituals including religious exclamations, songs, mealtime prayers, communion, holding religious objects, and talking about religious activities such as church choir or excursions Residents displayed positive reactions and signs of well-being Some previously religious residents did not show interest |
| Powers and Watson, 2011 [41] | To identify and examine multi-perspective views of residents’ spiritual orientation, practices, preferences; perceptions of spiritual nurturance and support; and resources and approaches to spiritual needs | New York, USA, 48 nursing homes with and without religious affiliations | All stages: mild, moderate, and severe dementia CPS = 0–6 | Residents with dementia (N = 83), family members (N = 30), and nursing home staff (N = 66) (clergy, pastoral care providers, nurses, nursing assistants, social workers, recreation and physical therapists, housekeepers, food service workers, administrators, and volunteers) mild (N = 26) moderate (N = 30) severe (N = 27) N = 36 unable to verbally communicate N = 47 able to verbally communicate | Mixed methods concurrent nested, predominantly qualitative 4/5 rating | Residents: Religious practices: Sabbath candles, mealtime grace, and bedtime prayers Spiritual activities: classical music, longtime hobbies, card games, and holiday celebrations Spiritual concerns: prayer, doubt, and disillusionment Family/NH Staff: residents need spiritual connectedness support, and need to nurture spirit within Institutional resources/approaches:religious and spiritual activities held at facilities and spiritual care providers NH Staff: importance of accommodating religious diversity |
| In residents with dementia | ||||||
| Chen et al., 2019 [42] | Explore spiritual needs of older adults living with mild dementia in the community | Taiwan, community receiving home care services from mental health hospital staff | Mild dementia CDR = 1 or MMSE 18–23 | Older adults living with mild dementia (N = 10) Ages 68–93 years | Qualitative Descriptive, semi-structured interviews with content analysis 5/5 rating | Four themes: (1) desire to turn back time, (2) to retain some control of remaining life, (3) to instill meaning into past experiences, and (4) to rely on faith-based strength Spiritual needs centered around wanting to turn back time and reverse impaired memory and loss of independence |
| Balqis et al., 2021 [43] | To identify support needs of older adults with dementia living in long-term care | Indonesia, long-term care | Mild to moderate dementia CDR, score unspecified | Older adults living with dementia, (N = 10), mild stage (N = 7), and moderate stage (N = 3) Age 64–86 years High school education or higher | Qualitative Descriptive phenomenology with structural analysis 4/5 rating | Older adults living with mild to moderate dementia have ability to share their experiences for holistic support (i.e., bio-psycho-social-spiritual needs) Spiritual support included support to get closer to God, help in worship, and at end of life Holistic support can help maintain current abilities and improve their quality of life LTC needs to improve the quality of care and quantity of caregivers to maximize holistic support for this population |
| Toivonen et al., 2023 [44] | To understand how older adults with dementia experience spirituality and spiritual support in nursing care | Finland, home care and long-term care | Various types of dementia, including Alzheimer’s, Vascular, and unspecified Mild to moderate | Older adults living with dementia (N = 10) and family members (N = 9) | Qualitative Ricoeurian hermeneutic phenomenology with structural analysis 5/5 rating | Older adults living with dementia need spiritual support in nursing care, which should be personalized Four elements of spirituality were identified: religion, meaningful relationships, nature, and art Barriers identified in nursing care provision: spiritual care competence, limited time, presence, and experience |
| In nurses | ||||||
| Toivenen et al., 2018 [45] | Describe the experiences of nurses supporting spirituality in the care of older people living with dementia | Finland, dementia Nursing units | Unspecified, but includes severe dementia | Female nurses and nursing assistants (N = 17) with at least 1 year of nursing experience | Qualitative Heideggerian hermeneutic phenomenology with inductive analysis 5/5 rating | Spiritual needs of older adults can be understood through verbal and non-verbal expressions, verbally both directly and indirectly, and by valuing their spiritual backgrounds |
| In clergy | ||||||
| Tomkins and Sorell, 2008 [46] | To explore how clergy meet the needs of Alzheimer’s disease patients and their families | Virginia, USA, their own established churches and congregations within local communities | Unspecified | Clergy (N = 12) from Mennonite and Lutheran congregations | Qualitative Open-ended interviews and focus groups Grounded Theory 3/5 rating | Many of the clergy stated the importance of simple religious rituals, such as prayer and song, in helping maintain spiritual connections for individuals with Alzheimer’s disease Lack of training for clergy, and an opportunity to create a curriculum for an educational program for clergy and leaders in faith communities |
| In residents with dementia, family, NH staff | ||||||
| Carr et al., 2011 [47] | To explore the meaning of spiritual care from the perspectives of patients living with moderate to severe dementia, their families, and their care provider | Canada, urban tertiary care center | Moderate to severe dementia MMSE > 10 | (N = 29) Older adults with dementia (N = 8) Family members (N = 5) Healthcare workers (N = 11) | Qualitative Hermeneutic phenomenologicalOpen-ended interviews 5/5 rating | Spiritual care focuses on promoting personhood through intentional caring attitudes and actions: listening to and being with, meeting religious needs, and facilitating religious rites and rituals Recognizing and attending to ‘little things’ promoted a sense of personhood and connectedness to self and others Spiritual care provides opportunities for the one caring to feel valued, cared for, and connected |
| In residents with dementia | ||||||
| Aloustani et al., 2021 [48] | Effect of group spiritual therapy on cognitive function of older adults | Iran, center for older adults | Mild dementia MMSE > 20 | Older adults with dementia (N = 50), Experimental group (N = 25) and control group (N = 25) Age 60 years and above | Randomized control trial For 2 weeks 4/5 rating | A significant difference in effect of cognitive state after the spiritual therapy intervention (p < 0.01) Group spiritual therapy can be used as a complementary, low-cost, and effective method for improving the cognitive state of older adults |
| In others | ||||||
| Connelly and Moss, 2021 [49] | Whether music may prove a useful tool for assessing spiritual needs and providing meaningful spiritual support for people with dementia | Ireland, hospital setting | Unspecified | Music therapists (N = 3) and a pastoral care professional (N = 1) | Qualitative Open-ended interviews Interpretative phenomenological analysis 3/5 rating | Five themes: (1) musichas the capacity to facilitate spiritual expression; (2) spirituality is necessarily a broad and evolving term; (3) spirituality may be a coping mechanism for people with dementia; (4) music therapy contributes to validating the individuality of the person with dementia; and (5) collaborative work between music therapy and pastoral care is worthy of further exploration As individual services, music therapy and pastoral care are exploring how to provide good-quality spiritual care for people with dementia |
| In nurses | ||||||
| Palmer et al., 2022 [50] | Explore the salient spiritual needs in dementia to inform future intervention development | Boston, USA, community-based and long-term care facilities | All dementia stages (mild, moderate, and severe) | Providers including chaplains (N-10), nursing staff (N = 6), social workers (N = 6), and activity professionals (N = 2) | Qualitative Semi-structured with thematic analysis 5/5 rating | No difference in findings by provider type or by religious/spiritual affiliation Spiritual experience in dementia differs from other medical conditions (1) fear, profound loss of self, inability to access faith, and progressive and incurable nature of dementia make it different (2) there is a window of opportunity in the mild phase since there is awareness of mild dementia, which precipitates spiritual distress |
| In providers | ||||||
| van der Steen et al., 2014a [51] | Examine provision of spiritual end-of-life care in dementia | Netherlands, 28 long-term care | All-cause severe dementia BANS-S ≥ 17 | Long-term care physicians providing care at end-of-life for residents with dementia (N = 88) | Prospective and Retrospective Unspecified length of time 5/5 rating * | Spiritual end-of-life care was provided shortly before death to 20.8% of the residents Predictors of end-of-life spiritual care provision were families’ satisfaction with physicians’ communication at baseline, faith or spirituality very important to residents, and female family caregiving |
| Characteristics | Frequency (n) |
|---|---|
| Publication year | |
| 2008–2014 | 4 |
| 2015–2020 | 3 |
| 2021–2022 | 5 |
| Region | |
| the Netherlands | 1 |
| USA | 3 |
| Canada | 1 |
| Germany | 1 |
| Iran | 1 |
| Taiwan | 1 |
| Indonesia | 1 |
| Finland | 2 |
| Ireland | 1 |
| Setting | |
| Long-term care | 6 |
| Community-based | 3 |
| Hospitals Variety of settings | 2 1 |
| Dementia stage evaluated | |
| Unspecified | 3 |
| All three stages | 2 |
| Mild | 2 |
| Mild to Moderate Moderate to Severe Severe | 2 1 2 |
| Study participants/Data source | |
| Professionals | 6 |
| PLwD | 3 |
| Combined | 3 |
| Study design | |
| RCT | 1 |
| Mixed Methods | 1 |
| Qualitative | 9 |
| Quantitative | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Britt, K.C.; Boateng, A.C.O.; Zhao, H.; Ezeokonkwo, F.C.; Federwitz, C.; Epps, F. Spiritual Needs of Older Adults Living with Dementia: An Integrative Review. Healthcare 2023, 11, 1319. https://doi.org/10.3390/healthcare11091319
Britt KC, Boateng ACO, Zhao H, Ezeokonkwo FC, Federwitz C, Epps F. Spiritual Needs of Older Adults Living with Dementia: An Integrative Review. Healthcare. 2023; 11(9):1319. https://doi.org/10.3390/healthcare11091319
Chicago/Turabian StyleBritt, Katherine Carroll, Augustine C. O. Boateng, Hui Zhao, Francesca C. Ezeokonkwo, Chad Federwitz, and Fayron Epps. 2023. "Spiritual Needs of Older Adults Living with Dementia: An Integrative Review" Healthcare 11, no. 9: 1319. https://doi.org/10.3390/healthcare11091319