
Influence of Face Masks on Physiological and Subjective Response during 130 Min of Simulated Light and Medium Physical Manual Work—An Explorative Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
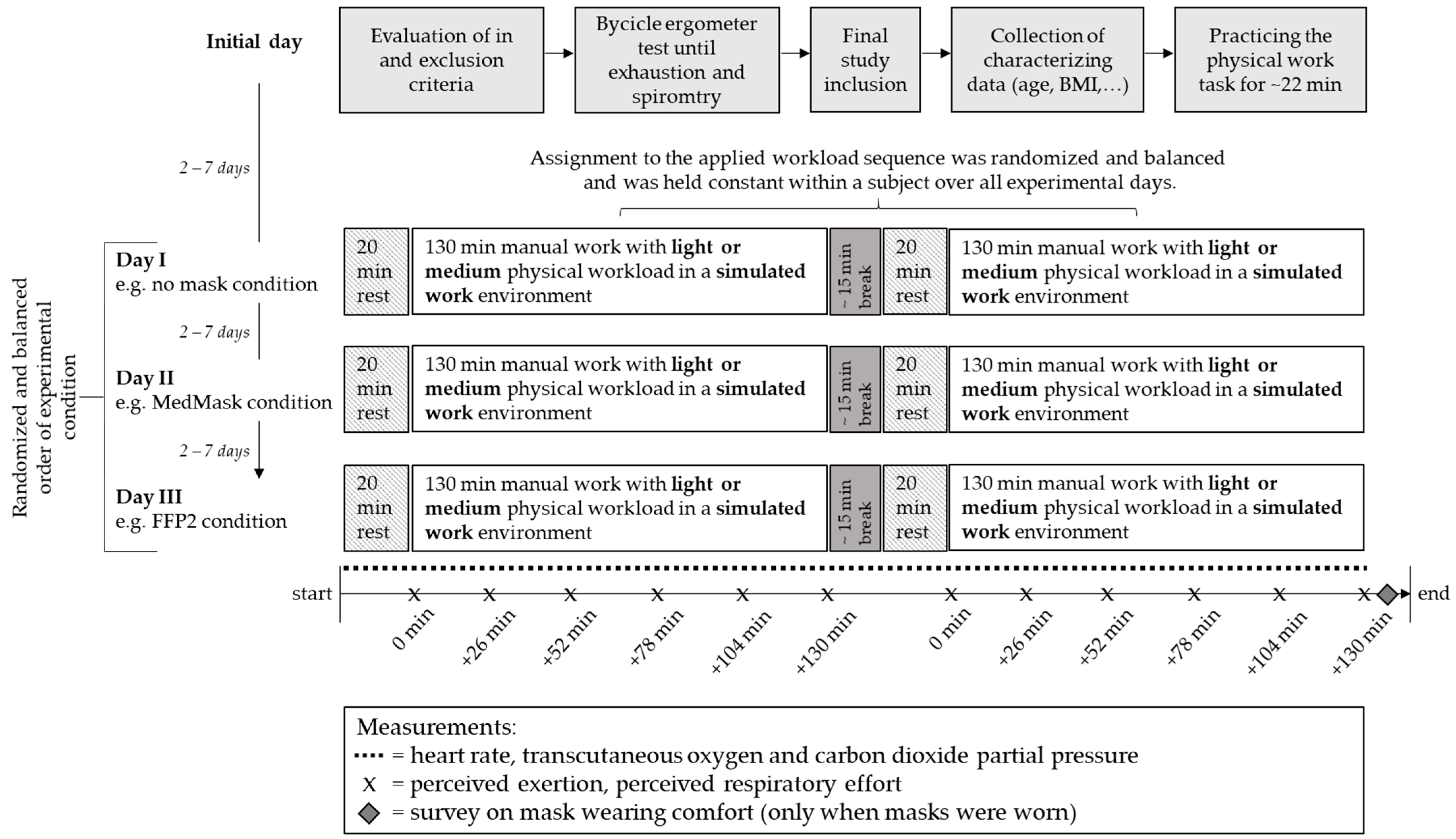
2.2. Study Design and Study Procedure
2.2.1. Study Design and Sample Size
2.2.2. Face Masks
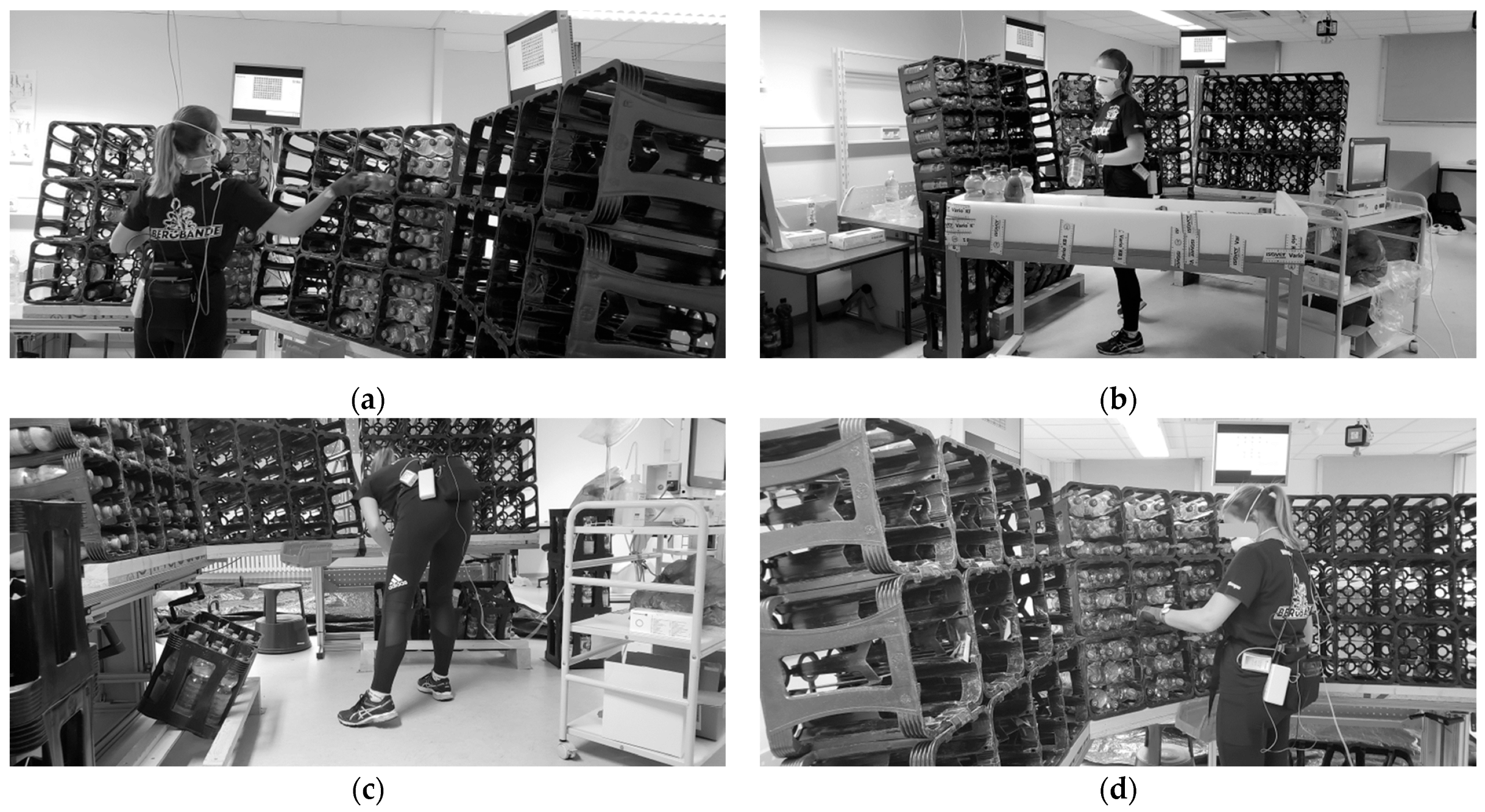
2.2.3. Simulated Light and Medium Physical Manual Work
2.2.4. Procedures
2.3. Outcomes and Measuremsents
2.3.1. Heart Rate
2.3.2. Transcutaneous Oxygen and Carbon Dioxide Partial Pressure
2.3.3. Subjective Measurements
2.3.4. Survey on Mask Wearing Comfort
2.4. Data Analysis
2.4.1. Parameter Calculation
2.4.2. Data Synchronization
2.4.3. Statistical Analysis
3. Results
3.1. Dropouts
3.2. Characteristics of the Final Study Sample
3.3. Normal Distribution and Missing Data
3.4. Physiological Outcomes—Heart Rate, Transcutaneous O2 and CO2
3.4.1. Baseline Values of Heart Rate, Transcutaneous O2 and CO2 Partial Pressure
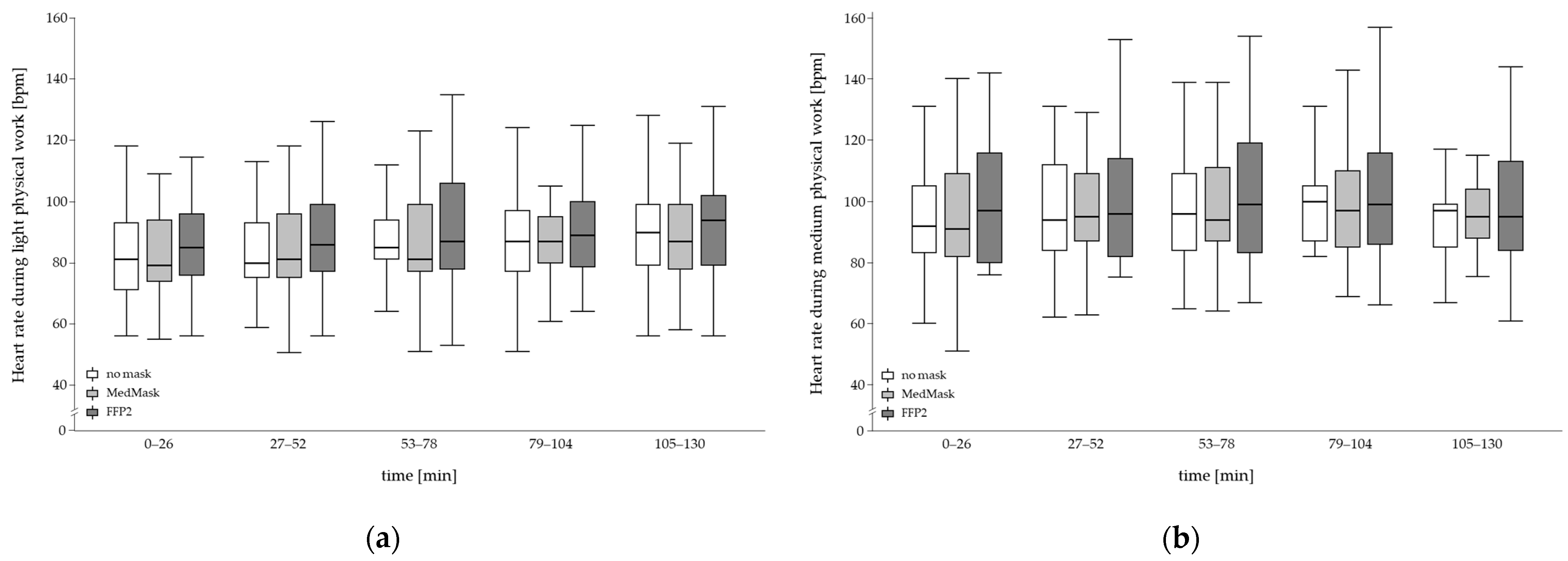
3.4.2. Heart Rate
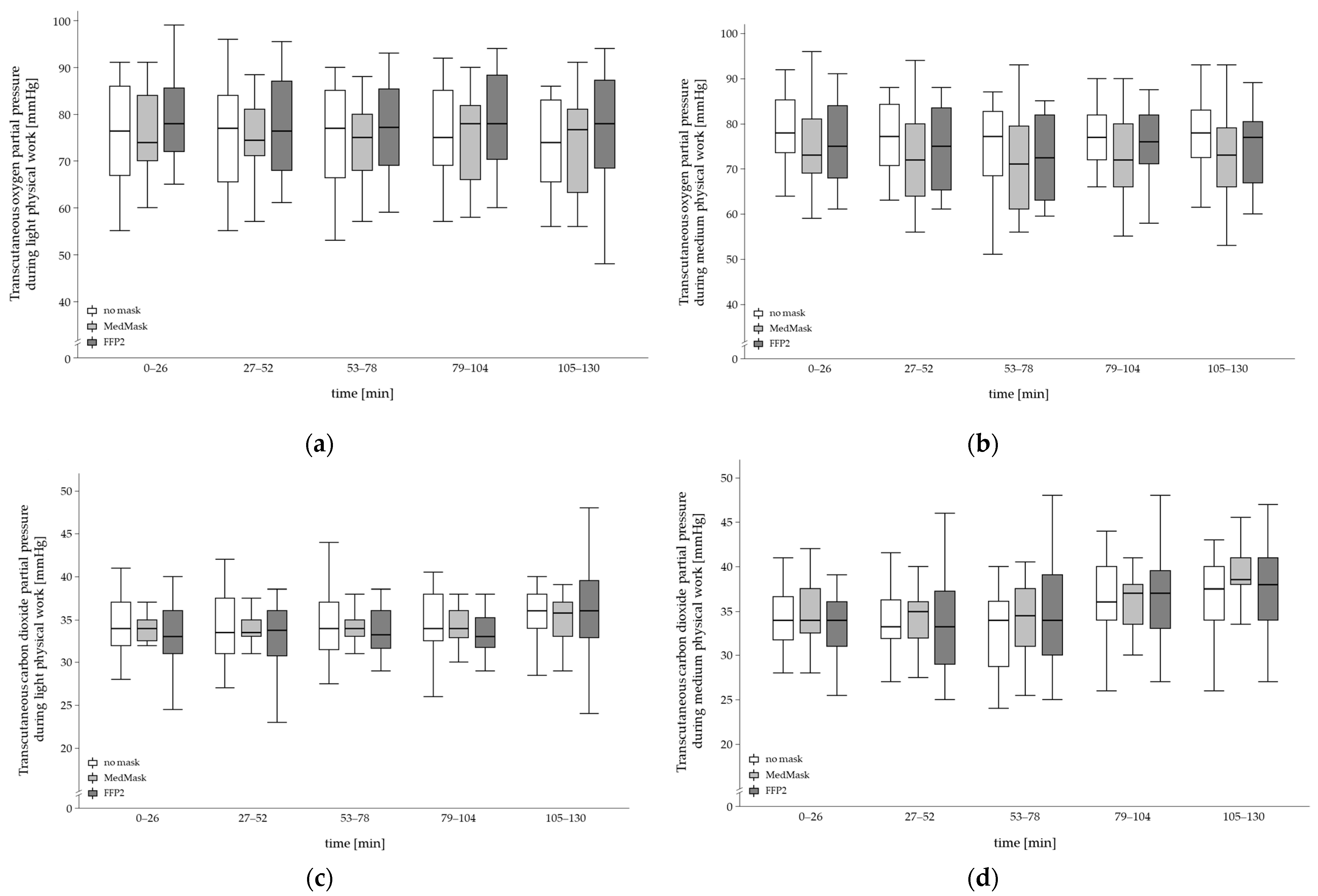
3.4.3. Transcutaneous O2 and CO2 Partial Pressure
3.5. Subjective Outcomes—Perceived Physical Exertion and Respiratory Fitness Level
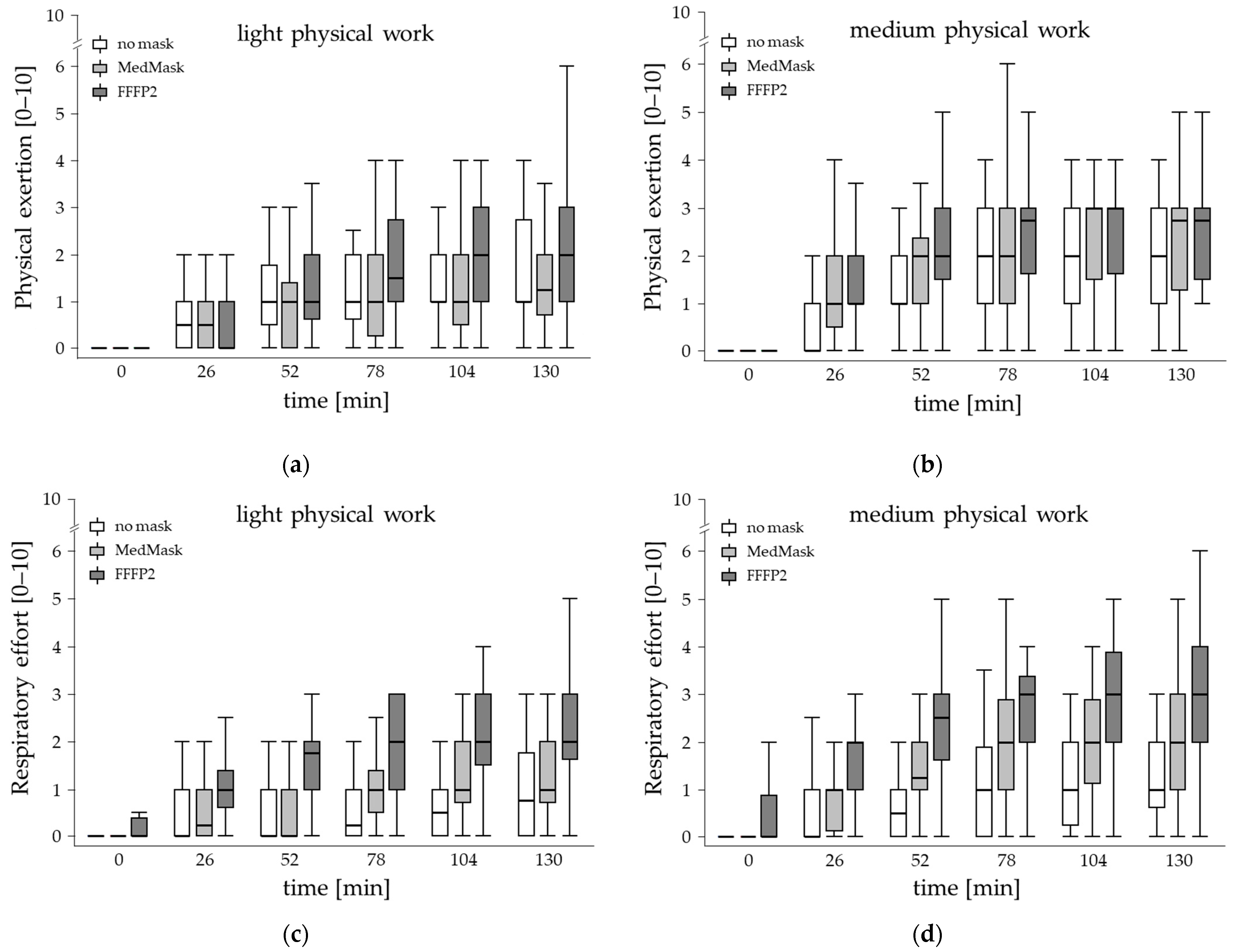
3.5.1. Perceived Physical Exertion
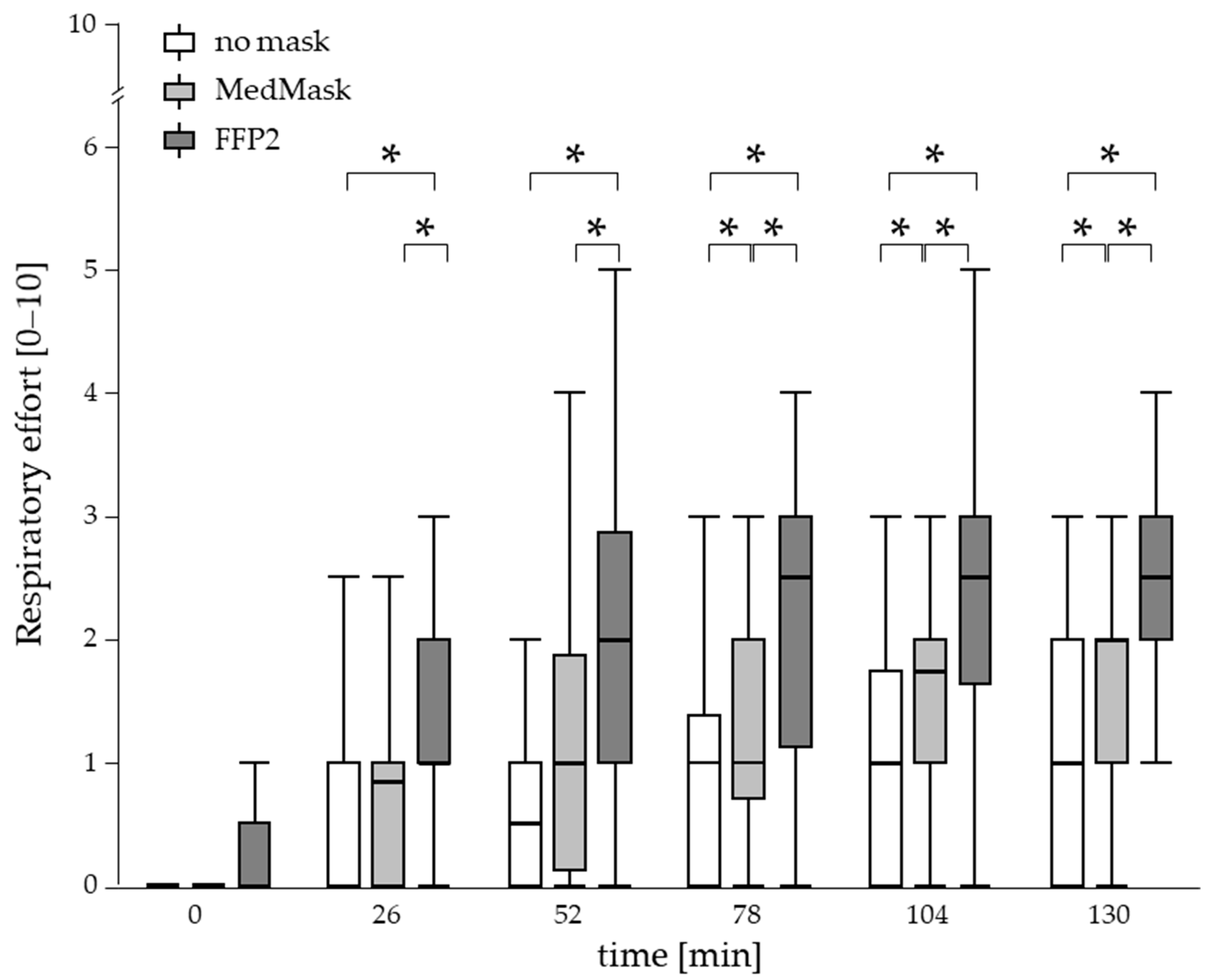
3.5.2. Perceived Respiratory Effort
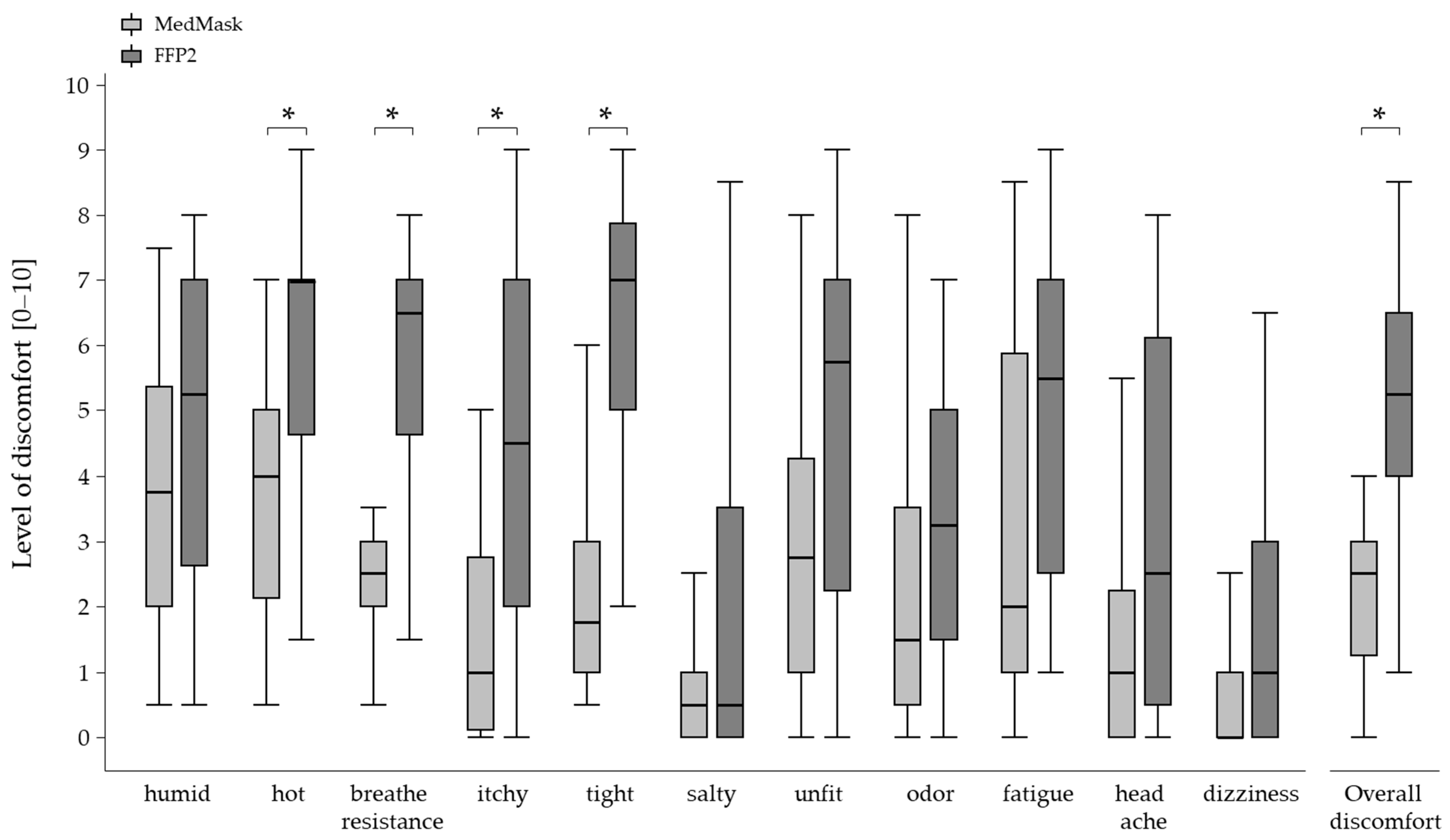
3.5.3. Wearing Comfort
4. Discussion
4.1. Physiological Outcomes—Heart Rate, PtcO2, and PtcCO2
4.2. Perceived Physical Exertion and Respiratory Effort
4.3. Wearing Comfort
4.4. Recommendation of Face Mask Use
4.5. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- People from the German Working Age (age between 18 and 67 years);
- Being able to work full shift;
- No diseases of the metabolism or cardiovascular or respiratory system;
- Written informed consent;
- Medically unobtrusive physical maximum endurance test and pulmonary function test.
- Acute myocardial infarction (within the last 48 h);
- Unstable angina pectoris with a high risk of infection;
- Uncontrolled symptomatic and hemodynamically unstable arrhythmias;
- Severe symptomatic aortic stenosis;
- Uncontrolled symptomatic heart failure;
- Acute myo- or pericarditis;
- Acute pulmonary embolism or acute pulmonary infarction;
- Acute aortic dissection;
- Main stem stenosis;
- Slight aortic stenosis;
- Arrhythmias tachyarrhythmia, bradyarrhythmia, frequent ventricular extra systoles;
- Higher atrioventricular block;
- Severe hypertrophic obstructive cardiomyopathy of an outflow tract;
- Severe arterial hypertension (systolic BD > 200 mmHg and/or diastolic BD > 110 mmHg);
- Electrolyte disorders, especially hyperkalemia;
- Physical or psychological impairments, due to which an optimal examination is not possible (e.g., febrile infection);
- Diabetes;
- Acute illness;
- Under- or overweight (adipositas degree 1)—BMI < 18,5 kg/m²; or >30 kg/m²;
- Indications of a disease or disorder of the cardiovascular system assessed by a physical performance test (until subjective exhaustion on a standard bicycle ergometer);
- Indications of a disease or disorder of the respiratory system assessed by the pulmonary function test;
- Pregnancy.
Appendix B

References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 16 March 2023).
- Caroppo, E.; Mazza, M.; Sannella, A.; Marano, G.; Avallone, C.; Claro, A.E.; Janiri, D.; Moccia, L.; Janiri, L.; Sani, G. Will Nothing Be the Same Again?: Changes in Lifestyle during COVID-19 Pandemic and Consequences on Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 8433. [Google Scholar] [CrossRef] [PubMed]
- Long, E.; Patterson, S.; Maxwell, K.; Blake, C.; Boso Perez, R.; Lewis, R.; McCann, M.; Riddell, J.; Skivington, K.; Wilson-Lowe, R.; et al. COVID-19 pandemic and its impact on social relationships and health. J. Epidemiol. Community Health 2022, 76, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Abboah-Offei, M.; Salifu, Y.; Adewale, B.; Bayuo, J.; Ofosu-Poku, R.; Opare-Lokko, E.B.A. A rapid review of the use of face mask in preventing the spread of COVID-19. Int. J. Nurs. Stud. Adv. 2021, 3, 100013. [Google Scholar] [CrossRef] [PubMed]
- 3M. Comparison of FFP2, KN95, and N95 Filtering Facepiece Respirator Classes. Available online: https://multimedia.3m.com/mws/media/1791500O/comparison-ffp2-kn95-n95-filtering-facepiece-respirator-classes-tb.pdf (accessed on 31 January 2023).
- Bundesanstalt für Arbeitsschutz und Arbeitsmedizin. [Recommendations of the BAuA on the Use of Protective Masks in the Working Environment in Connection with SARS-CoV-2]. Empfehlungen der BAuA zum Einsatz von Schutzmasken in der Arbeitswelt im Zusammenhang mit SARS-CoV-2. Available online: https://www.baua.de/DE/Themen/Arbeitsgestaltung-im-Betrieb/Coronavirus/pdf/Schutzmasken.pdf?__blob=publicationFile&v=20 (accessed on 31 January 2023).
- Sommerstein, R.; Fux, C.A.; Vuichard-Gysin, D.; Abbas, M.; Marschall, J.; Balmelli, C.; Troillet, N.; Harbarth, S.; Schlegel, M.; Widmer, A.; et al. Risk of SARS-CoV-2 transmission by aerosols, the rational use of masks, and protection of healthcare workers from COVID-19. Antimicrob. Resist. Infect. Control 2020, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- Azap, A.; Erdinc, F.S. Medical mask or N95 respirator: When and how to use? Turk. J. Med. Sci. 2020, 50, 633–637. [Google Scholar] [CrossRef]
- Cheng, Y.; Ma, N.; Witt, C.; Rapp, S.; Wild, P.S.; Andreae, M.O.; Poschl, U.; Su, H. Face masks effectively limit the probability of SARS-CoV-2 transmission. Science 2021, 372, 1439–1443. [Google Scholar] [CrossRef]
- Lee, H.P.; Wang, D.Y. Objective assessment of increase in breathing resistance of N95 respirators on human subjects. Ann. Occup. Hyg. 2011, 55, 917–921. [Google Scholar] [CrossRef]
- Vainshelboim, B. Retracted: Facemasks in the COVID-19 era: A health hypothesis. Med. Hypotheses 2021, 146, 110411. [Google Scholar] [CrossRef]
- Kisielinski, K.; Giboni, P.; Prescher, A.; Klosterhalfen, B.; Graessel, D.; Funken, S.; Kempski, O.; Hirsch, O. Is a Mask That Covers the Mouth and Nose Free from Undesirable Side Effects in Everyday Use and Free of Potential Hazards? Int. J. Environ. Res. Public Health 2021, 18, 4344. [Google Scholar] [CrossRef]
- De Brouwer, C. Wearing a Mask, a Universal Solution Against COVID-19 or an Additional Health Risk? Available online: https://ssrn.com/abstract=3676885 (accessed on 31 January 2023).
- Hopkins, S.R.; Dominelli, P.B.; Davis, C.K.; Guenette, J.A.; Luks, A.M.; Molgat-Seon, Y.; Sa, R.C.; Sheel, A.W.; Swenson, E.R.; Stickland, M.K. Face Masks and the Cardiorespiratory Response to Physical Activity in Health and Disease. Ann. Am. Thorac. Soc. 2021, 18, 399–407. [Google Scholar] [CrossRef]
- Litwinowicz, K.; Choroszy, M.; Ornat, M.; Wrobel, A.; Waszczuk, E. Bayesian network meta-analysis of face masks’ impact on human physiology. Sci. Rep. 2022, 12, 5823. [Google Scholar] [CrossRef] [PubMed]
- Koordinierungskreis für Biologische Arbeitsstoffe (KOBAS). [Recommendation for the Wearing Time Limit for Mouth-Nose-Coverings (MNB) in Terms of the SARS-CoV-2 Occupational Health and Safety Standard and the SARS-CoV-2 Occupational Health and Safety Rule]. Empfehlung zur Tragezeitbegrenzung für Mund-Nase-Bedeckungen (MNB) im Sinne des SARS-CoV-2-Arbeitsschutzstandards und der SARS-CoV-2-Arbeitsschutzregel. Available online: https://vdsi.de/media/tragezeitbegrenzung_kobas_07.10.2020.pdf (accessed on 31 January 2023).
- Zheng, C.; Poon, E.T.; Wan, K.; Dai, Z.; Wong, S.H. Effects of Wearing a Mask During Exercise on Physiological and Psychological Outcomes in Healthy Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2022, 53, 125–150. [Google Scholar] [CrossRef] [PubMed]
- Engeroff, T.; Groneberg, D.A.; Niederer, D. The Impact of Ubiquitous Face Masks and Filtering Face Piece Application During Rest, Work and Exercise on Gas Exchange, Pulmonary Function and Physical Performance: A Systematic Review with Meta-analysis. Sports Med. Open 2021, 7, 92. [Google Scholar] [CrossRef]
- Fikenzer, S.; Uhe, T.; Lavall, D.; Rudolph, U.; Falz, R.; Busse, M.; Hepp, P.; Laufs, U. Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clin. Res. Cardiol. 2020, 109, 1522–1530. [Google Scholar] [CrossRef] [PubMed]
- Georgi, C.; Haase-Fielitz, A.; Meretz, D.; Gasert, L.; Butter, C. The Impact of Commonly-Worn Face Masks on Physiological Parameters and on Discomfort During Standard Work-Related Physical Effort. Dtsch. Arztebl. Int. 2020, 117, 674–675. [Google Scholar] [CrossRef]
- Steinhilber, B.; Seibt, R.; Gabriel, J.; Brountsou, J.; Muljono, M.; Downar, T.; Bar, M.; Bonsch, R.; Brandt, A.; Martus, P.; et al. Effects of Face Masks on Physical Performance and Physiological Response during a Submaximal Bicycle Ergometer Test. Int. J. Environ. Res. Public Health 2022, 19, 1063. [Google Scholar] [CrossRef]
- Chatterjee, M.; Schmeißer, G. [Updated guideline for ergometry as part of occupational medical examinations] Aktualisierter Leitfaden für die Ergometrie im Rahmen arbeitsmedizinischer Untersuchungen. Arb. Soz. Umweltmed. 2017, 52, 913–921. [Google Scholar]
- Finger, J.D.; Krug, S.; Gößwald, A.; Härtel, S.; Bös, K. English Version: [Cardiorespiratory fitness in adults in Germany] Kardiorespiratorische Fitness bei Erwachsenen in Deutschland. Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundh. Gesundh. Gesundh. 2013, 56, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Stemper, T. [Health, Fitness, Recreational Sports: Practice of Modern Health Sports] Gesundheit, Fitness, Freizeitsport: Praxis des Modernen Gesundheitssports; Bund: Köln, Germany, 1988; p. 144. [Google Scholar]
- Statista. [Number of People Employed in Manufacturing (Excluding Construction) in Germany from 1991 to 2022] Anzahl der Erwerbstätigen im produzierenden Gewerbe (ohne Baugewerbe) in Deutschland von 1991 bis 2022. Available online: https://de.statista.com/statistik/daten/studie/2190/umfrage/anzahl-der-erwerbstaetigen-im-produzierenden-gewerbe/?locale=de (accessed on 16 March 2023).
- Wang, B.-S.; Wang, X.-J.; Gong, L.-K. The Construction of a Williams Design and Randomization in Cross-Over Clinical Trials Using SAS. J. Stat. Softw. 2009, 29, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19): Masks. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks (accessed on 22 January 2023).
- Cibis, W. REFA-System. Available online: https://www.pschyrembel.de/REFA-System/S020G (accessed on 31 January 2023).
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sorensen, F.; Andersson, G.; Jorgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Fuchs, R.; Klaperski, S.; Gerber, M.; Seeling, H. [Measuring physical activity and sport with the BSA questionnaire. A methodological interim review]. Messung der Bewegungs- und Sportaktivität mit dem BSA-Fragebogen. Eine methodische Zwischenbilanz. Z. Für Gesundh. 2015, 23, 16. [Google Scholar] [CrossRef]
- Carter, R.; Banham, S.W. Use of transcutaneous oxygen and carbon dioxide tensions for assessing indices of gas exchange during exercise testing. Respir. Med. 2000, 94, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Boshuizen, R.C.; Vincent, A.D.; van den Heuvel, M.M. Comparison of modified Borg scale and visual analog scale dyspnea scores in predicting re-intervention after drainage of malignant pleural effusion. Support. Care Cancer 2013, 21, 3109–3116. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Tokura, H.; Guo, Y.P.; Wong, A.S.; Wong, T.; Chung, J.; Newton, E. Effects of wearing N95 and surgical facemasks on heart rate, thermal stress and subjective sensations. Int. Arch. Occup. Environ. Health 2005, 78, 501–509. [Google Scholar] [CrossRef]
- Schielzeth, H.; Dingemanse, N.J.; Nakagawa, S.; Westneat, D.F.; Allegue, H.; Teplitsky, C.; Reale, D.; Dochtermann, N.A.; Garamszegi, L.Z.; Araya-Ajoy, Y.G. Robustness of linear mixed-effects models to violations of distributional assumptions. Methods Ecol. Evol. 2020, 11, 1141–1152. [Google Scholar] [CrossRef]
- Rebmann, T.; Carrico, R.; Wang, J. Physiologic and other effects and compliance with long-term respirator use among medical intensive care unit nurses. Am. J. Infect. Control 2013, 41, 1218–1223. [Google Scholar] [CrossRef]
- Lassing, J.; Falz, R.; Pokel, C.; Fikenzer, S.; Laufs, U.; Schulze, A.; Holldobler, N.; Rudrich, P.; Busse, M. Effects of surgical face masks on cardiopulmonary parameters during steady state exercise. Sci. Rep. 2020, 10, 22363. [Google Scholar] [CrossRef]
- Jesus, J.P.; Gomes, M.; Dias-Goncalves, A.; Correia, J.M.; Pezarat-Correia, P.; Mendonca, G.V. Effects of surgical masks on the responses to constant work-rate cycling performed at different intensity domains. Clin. Physiol. Funct. Imaging 2022, 42, 43–52. [Google Scholar] [CrossRef]
- Seibt, R.; Bar, M.; Rieger, M.A.; Steinhilber, B. Limitations in evaluating COVID-19 protective face masks using open circuit spirometry systems: Respiratory measurement mask introduces bias in breathing pressure and perceived respiratory effort. Physiol. Meas. 2023, 44, 015001. [Google Scholar] [CrossRef]
- Sammito, S.; Thielmann, B.; Seibt, R.; Klussmann, A.; Weippert, M.; Böckelmann, I. Guideline for the application of heart rate and heart rate variability in occupational medicine and occupational science. ASU Int. 2015, 06, 1–29. [Google Scholar] [CrossRef]
- Blake, D.F.; Young, D.A.; Brown, L.H. Transcutaneous oximetry: Variability in normal values for the upper and lower limb. Diving Hyperb. Med. 2018, 48, 2–9. [Google Scholar] [CrossRef]
- Weaver, L.K. Transcutaneous oxygen and carbon dioxide tensions compared to arterial blood gases in normals. Respir. Care 2007, 52, 1490–1496. [Google Scholar]
- Gericke, A.; Militky, J.; Venkataraman, M.; Steyn, H.; Vermaas, J. The Effect of Mask Style and Fabric Selection on the Comfort Properties of Fabric Masks. Materials 2022, 15, 2559. [Google Scholar] [CrossRef] [PubMed]
- Radonovich, L.J., Jr.; Cheng, J.; Shenal, B.V.; Hodgson, M.; Bender, B.S. Respirator tolerance in health care workers. JAMA 2009, 301, 36–38. [Google Scholar] [CrossRef]
- Deutsche Gesetzliche Unfallversicherung. [DGUV Regulation 112-190 Use of Respiratory Protective Equipment]. DGUV Regel 112–190 Benutzung von Atemschutzgeräten. Available online: https://publikationen.dguv.de/regelwerk/dguv-regeln/1011/benutzung-von-atemschutzgeraeten (accessed on 31 January 2023).
- Buzzin, A.; Domenech-Gil, G.; Fraschetti, E.; Giovine, E.; Puglisi, D.; Caputo, D. Assessing the consequences of prolonged usage of disposable face masks. Sci. Rep. 2022, 12, 16796. [Google Scholar] [CrossRef] [PubMed]
- Miko, H.-C.; Zillmann, N.; Ring-Dimitriou, S.; Dorner, T.E.; Titze, S.; Bauer, R. Effects of Physical Activity on Health. Gesundheitswesen 2020, 82 (Suppl. 3), S184–S195. [Google Scholar] [CrossRef]
- Das, T.K. Effects of the menstrual cycle on timing and depth of breathing at rest. Indian J. Physiol. Pharmacol. 1998, 42, 498–502. [Google Scholar] [PubMed]
- Ginszt, M.; Zielinski, G.; Szkutnik, J.; Wojcicki, M.; Baszczowski, M.; Litko-Rola, M.; Rozylo-Kalinowska, I.; Majcher, P. The Effects of Wearing a Medical Mask on the Masticatory and Neck Muscle Activity in Healthy Young Women. J. Clin. Med. 2022, 11, 303. [Google Scholar] [CrossRef] [PubMed]
- Ginszt, M.; Zielinski, G.; Szkutnik, J.; Wojcicki, M.; Baszczowski, M.; Litko-Rola, M.; Zielinska, D.; Rozylo-Kalinowska, I. The Difference in Electromyographic Activity While Wearing a Medical Mask in Women with and without Temporomandibular Disorders. Int. J. Environ. Res. Public Health 2022, 19, 15559. [Google Scholar] [CrossRef]
- Mummery, V.; Rogers, E.; Padmanaban, V.; Matthew, D.; Woodcock, T.; Bloch, S. Transcutaneous carbon dioxide measurement is not a reliable alternative to arterial blood gas sampling in the acute medical setting. Eur. Respir. J. 2019, 53, 1801726. [Google Scholar] [CrossRef]
- Bonnie, F.; Marianna, S.; Suzanne, L.; American Thoracic, S. Patient information series. Pulmonary function tests. Am. J. Respir. Crit. Care Med. 2014, 189, P17–P18. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Overall | Fitness Level 1 | Fitness Level 2 | Fitness Level 3 | ||
|---|---|---|---|---|---|---|
| PWCmax 1 | [W/kg] | mean | 3.1 | 2.5 | 3.0 | 4.4 |
| SD | 0.8 | 0.4 | 0.2 | 0.8 | ||
| sex | [n, %] | overall | 24, 100% | 9, 37.5% | 10, 41.7% | 5, 20.8% |
| men | 12, 50.0% | 5, 20.8% | 5, 20.8% | 2, 8.3% | ||
| women | 12, 50.0% | 4, 16.7% | 5, 20.8% | 3, 12.5% | ||
| smokers | [n, %] | 1, 4.2% | 1, 4.2% | 0, 0% | 0, 0% | |
| age 2 | [years] | mean | 37.8 | 43.2 | 38.8 | 25.8 |
| SD | 13.0 | 11.9 | 13.6 | 4.9 | ||
| BMI 2 | [kg/m²] | mean | 23.8 | 25.1 | 23.3 | 22.3 |
| SD | 2.3 | 2.1 | 2.3 | 1.5 | ||
| Physical sport activity 2, 3 | [minutes/week] | mean | 132.6 | 56.1 | 128.5 | 278.3 |
| SD | 147.3 | 106.7 | 131.7 | 152.6 |
| Physiological Outcome | Statistics (F-Value p-Value) | Baseline Values before the Working Period and without Wearing a Mask (Means and Confidence Intervals) | ||
|---|---|---|---|---|
| No Mask | MedMask | FFP2 | ||
| Heart rate [bpm] | F-value 0.59 p = 0.556 | 80.1 lower CI = 76.5 upper CI = 83.7 | 79.6 lower CI 76.0, upper CI 83.2 | 82.2 lower CI 78.6 upper CI 85.9 |
| PtcO2 [mmHg] | F-value 1.89 p = 0.156 | 74.5 lower CI 70.5 upper CI 78.4 | 69.4 lower CI 65.4 upper CI 73.4 | 70.1 lower CI 66.0 upper CI 74.1 |
| PtcCO2 [mmHg] | F-value 0.05 p = 0.954 | 32.4 lower CI 31.4 upper CI 33. | 32.5 lower CI 31.5 upper CI 33.6 | 32.5 lower CI 31.5 upper CI 33.6 |
| Outcome | Factor | Degree of Freedom | F-Value | p-Value |
| heart rate | mask condition | 2 | 13.41 | <0.0001 |
| workload | 1 | 212.07 | <0.0001 | |
| time | 4 | 6.71 | <0.0001 | |
| fitness level | 2 | 2.35 | 0.121 | |
| mask condition × time | 8 | 0.17 | 0.995 | |
| mask condition × time × workload | 8 | 0.20 | 0.990 | |
| mask condition × time × fitness level | 16 | 0.21 | 1.000 | |
| PtcO2 | mask condition | 2 | 4.09 | 0.017 |
| workload | 1 | 0.63 | 0.429 | |
| time | 4 | 1.16 | 0.329 | |
| fitness level | 2 | 2.83 | 0.083 | |
| mask condition × time | 8 | 0.04 | 1.000 | |
| mask condition × time × workload | 8 | 0.03 | 1.000 | |
| mask condition × time × fitness level | 16 | 0.11 | 1.000 | |
| PtcCO2 | mask condition | 2 | 3.43 | 0.033 |
| workload | 1 | 16.88 | 0.0001 | |
| time | 4 | 26.17 | <0.0001 | |
| fitness level | 2 | 0.50 | 0.613 | |
| mask condition × time | 8 | 0.39 | 0.928 | |
| mask condition × time × workload | 8 | 0.62 | 0.760 | |
| mask condition × time × fitness level | 16 | 0.613 | 0.875 |
| Outcome | Factor | Degree of Freedom | F-Value | p-Value |
|---|---|---|---|---|
| perceived physical exertion | mask condition | 2 | 31.69 | <0.0001 |
| workload | 1 | 162.94 | <0.0001 | |
| time | 5 | 153.36 | <0.0001 | |
| fitness level | 2 | 0.23 | 0.793 | |
| mask condition × time | 10 | 1.28 | 0.240 | |
| mask condition × time × workload | 10 | 0.68 | 0.739 | |
| mask condition × time × fitness level | 20 | 0.30 | 1.000 | |
| perceived respiratory effort | mask condition | 2 | 203.37 | <0.0001 |
| workload | 1 | 109.54 | <0.0001 | |
| time | 5 | 103.86 | <0.0001 | |
| fitness level | 2 | 1.05 | 0.368 | |
| mask condition × time | 10 | 6.68 | <0.0001 | |
| mask condition × time × workload | 10 | 0.31 | 0.978 | |
| mask condition × time × fitness level | 20 | 0.54 | 0.952 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinhilber, B.; Seibt, R.; Gabriel, J.; Bär, M.; Dilek, Ü.; Brandt, A.; Martus, P.; Rieger, M.A. Influence of Face Masks on Physiological and Subjective Response during 130 Min of Simulated Light and Medium Physical Manual Work—An Explorative Study. Healthcare 2023, 11, 1308. https://doi.org/10.3390/healthcare11091308
Steinhilber B, Seibt R, Gabriel J, Bär M, Dilek Ü, Brandt A, Martus P, Rieger MA. Influence of Face Masks on Physiological and Subjective Response during 130 Min of Simulated Light and Medium Physical Manual Work—An Explorative Study. Healthcare. 2023; 11(9):1308. https://doi.org/10.3390/healthcare11091308
Chicago/Turabian StyleSteinhilber, Benjamin, Robert Seibt, Julia Gabriel, Mona Bär, Ümütyaz Dilek, Adrian Brandt, Peter Martus, and Monika A. Rieger. 2023. "Influence of Face Masks on Physiological and Subjective Response during 130 Min of Simulated Light and Medium Physical Manual Work—An Explorative Study" Healthcare 11, no. 9: 1308. https://doi.org/10.3390/healthcare11091308