
Quality of Life and Family Support in Critically Ill Patients following ICU Discharge
 ,
,
Abstract
:1. Introduction
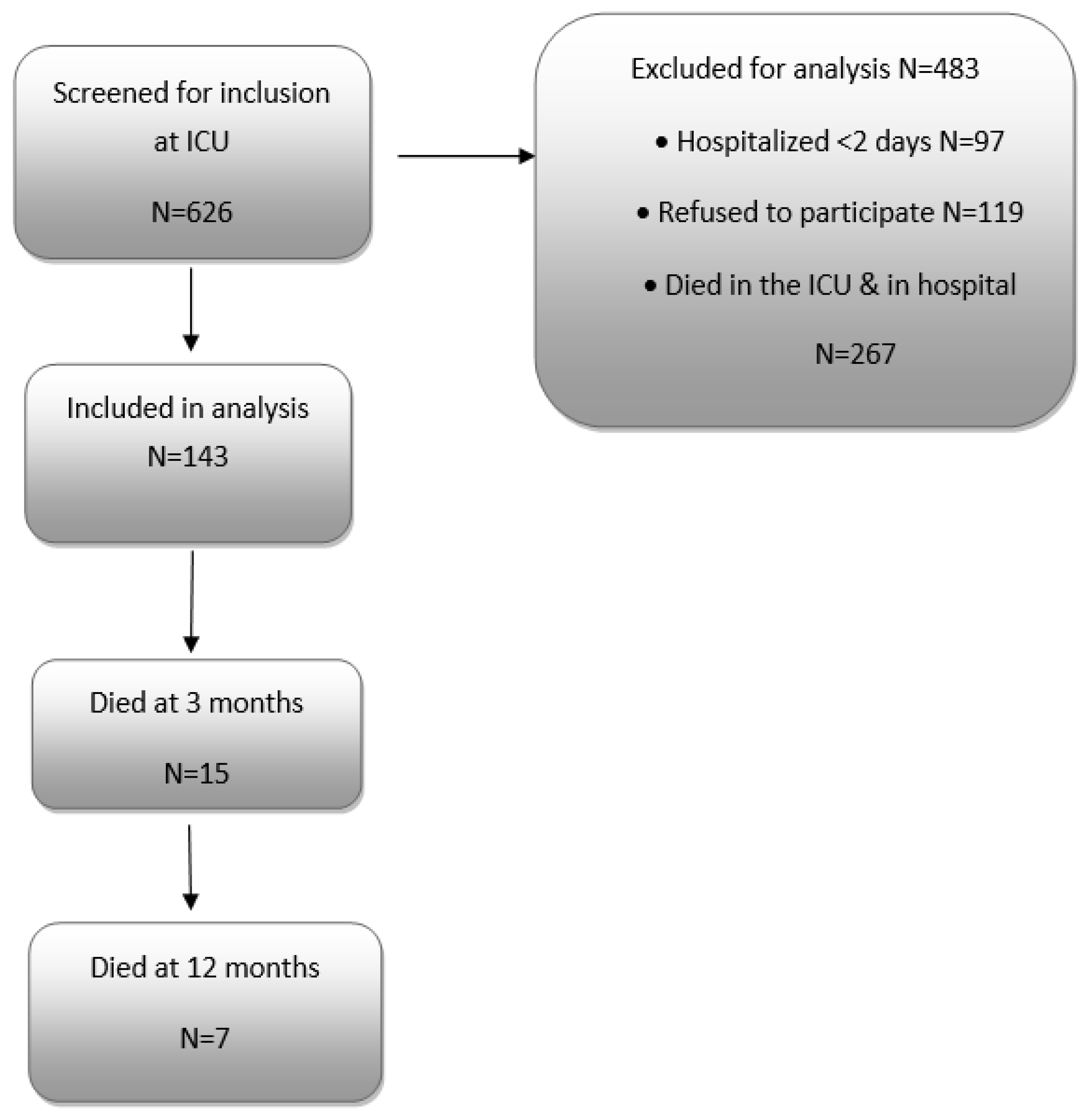
2. Methods
2.1. Study Outcomes
2.2. Data Collection
2.3. Questionnaire Interview
2.4. Respiratory Function Assessment
2.5. 6-Min Walk (6MWT)
2.6. Statistical Analysis
3. Results
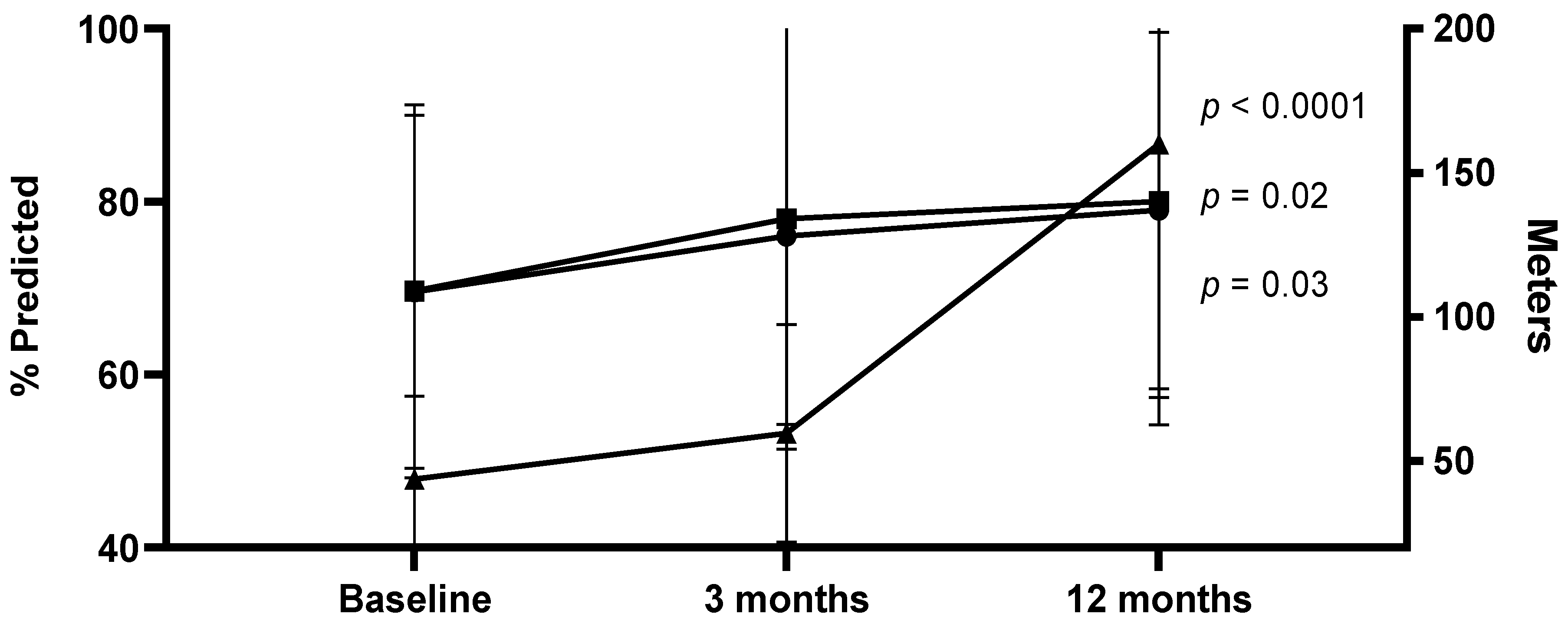
3.1. Lung Function and 6MWT
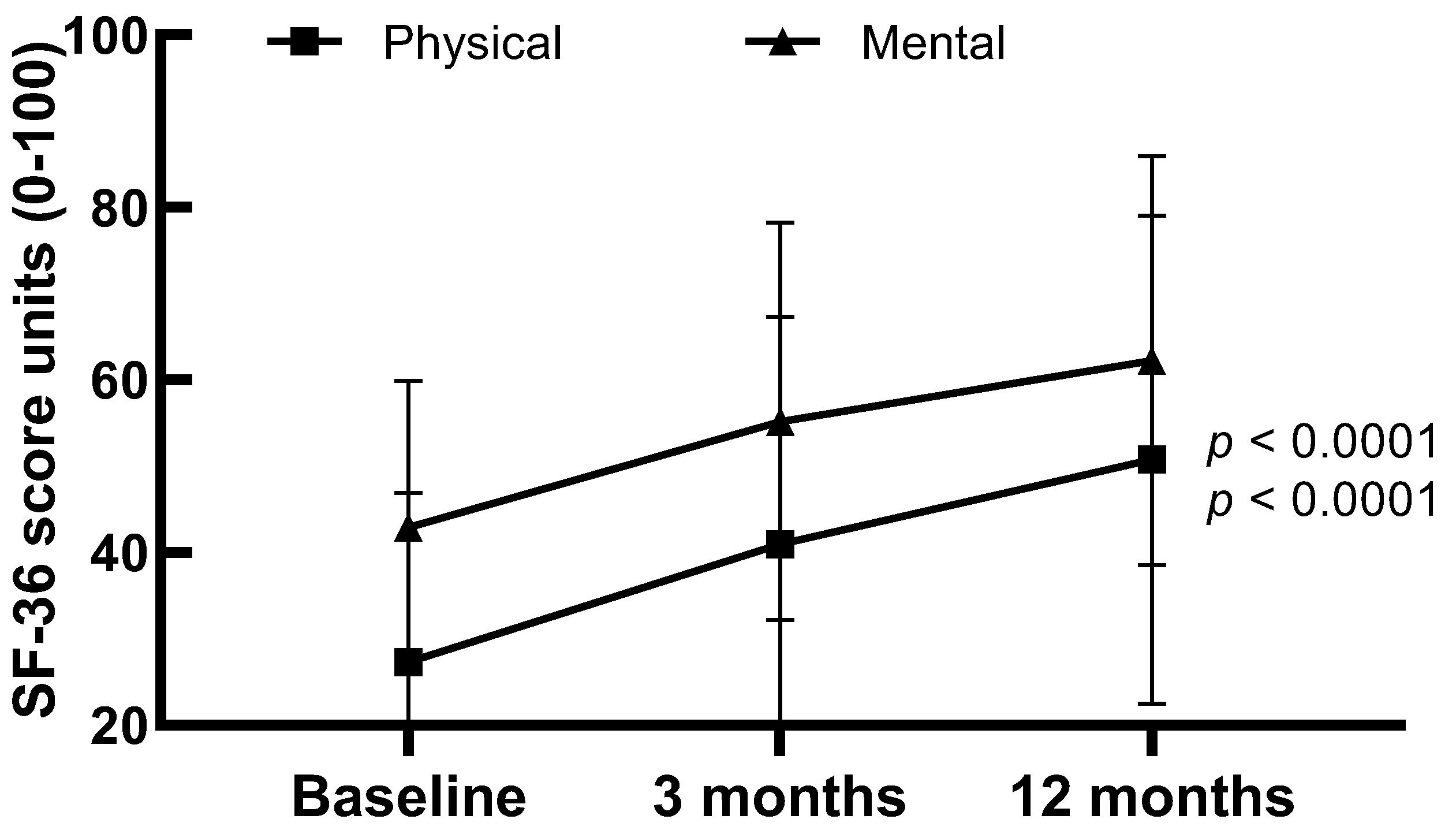
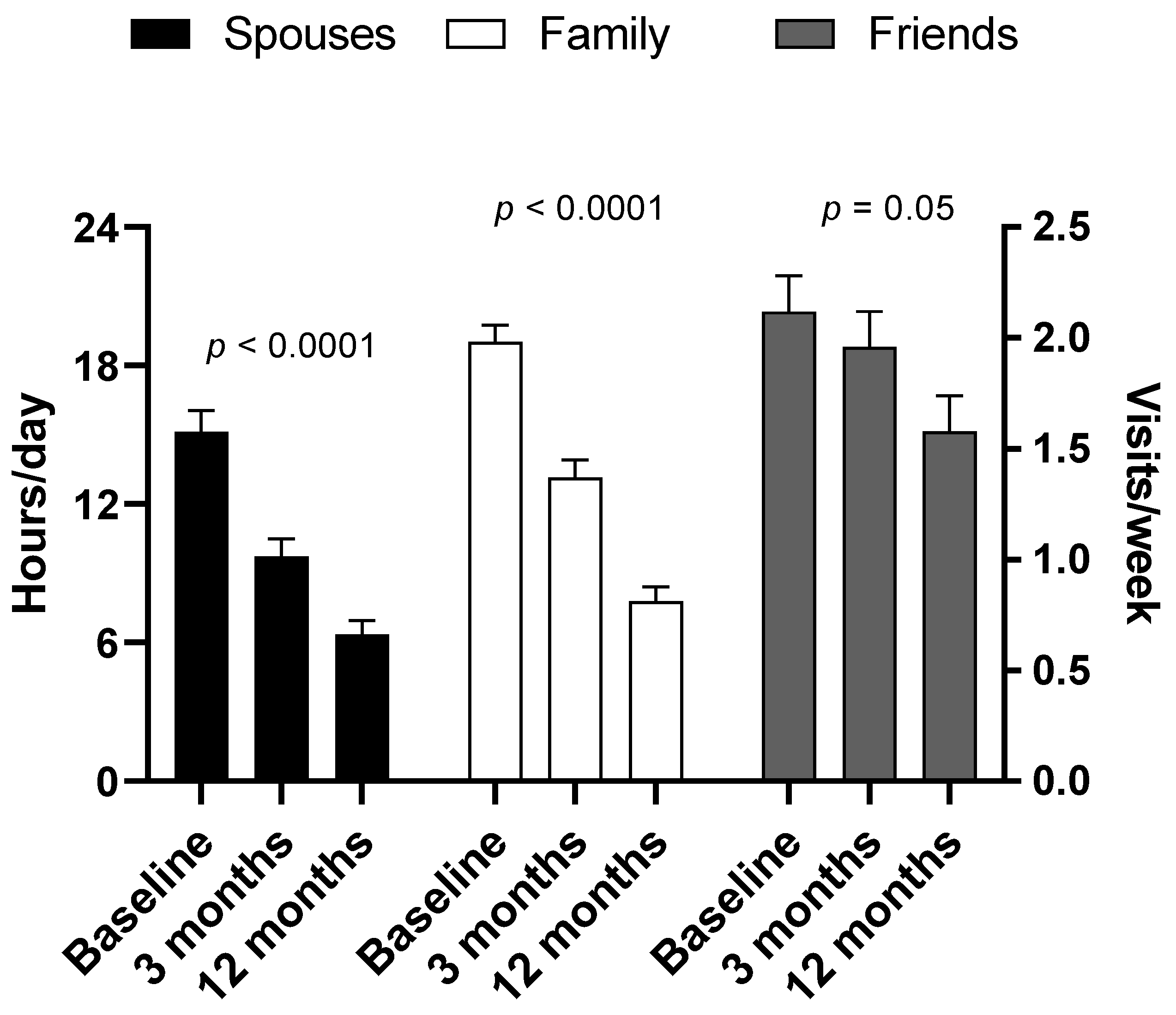
3.2. Family Support and SF-36 Scores
4. Discussion
5. Conclusions
6. Relevance to Clinical Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernando, A.; Santos, C.; Maia, P.; Maria, A. Castro and Henrique Barros. Quality of life after stay in surgical intensive care unit. BMC Anesthesiol. 2007, 7, 8. [Google Scholar]
- Amy, P.; Bradley, M. Post-intensive care syndrome symptoms and health-related quality of life in family decision-makers of critically ill patients. Palliat. Support. Care 2018, 16, 719–724. [Google Scholar]
- Sidiras, G.; Patsaki, I.; Karatznos, E.; Dakoutrou, M.; Kouvarakos, A.; Mitsiou, G.; Routsi, C.; Stranjalis, G.; Nanas, S.; Gerovasili, V. Long term follow-up of quality of life and functional ability in patients with ICU acquired Weakness-A post hoc analysis. J. Crit. Care 2019, 53, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Vogel, G.; Forinder, U.; Sandgren, A.; Svensen, C.; Joelsson-Alm, E. Health-related quality of life after general surgical intensive care. Acta Anaesthesiol. Scand. 2018, 23, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Sarah, E.; Jolley, D.; Aaron, E.; Bunnell, D.; Catherine, L. Icu-acquired weakness. Chest 2016, 150, 1129–1140. [Google Scholar]
- Davidson, E.; Aslakson, A.; Long, C.; Puntillo, A.; Kross, K.; Hart, J.; Cox, E.; Wunsch, H.; Wickline, A.; Nunnally, E.; et al. Guidelines for family-Centered Care in the Neonatal, Pediatric and adult ICU. Crit. Care Med. 2017, 45, 103–128. [Google Scholar] [CrossRef]
- White, B.; Angus, C.; Shields, M.; Buddadhumaruk, R.; Pidro, C.; Paner, C.; Chaitin, E.; Chang, C.; Pike, F.; Weissfeld, L.; et al. A Randomized Trial of a Family-Support Intervention in Intensive Care Units. N. Engl. J. Med. 2018, 378, 2365–2375. [Google Scholar] [CrossRef]
- Davidson, J.E.; Powers, K.; Hedayat, K.M.; Tieszen, M.; Kon, A.A.; Shepard, E.; Spuhler, V.; Todres, I.D.; Levy, M.; Barr, J.; et al. Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine Task Force 2004–2005. Crit. Care Med. 2007, 35, 605–622. [Google Scholar] [CrossRef] [Green Version]
- Davidson, E.; Jones, C.; Joseph, O. Family response to critical illness. Crit. Care Med. 2012, 40, 618–624. [Google Scholar] [CrossRef]
- Ashwin, K.; Emily, A.; Diaz-Ramirez, G.; Amy, K.; Ornstein, K.; Boscardin, J.; Smith, A. “Til death do us part”: End-of-life experiences of married couples in a nationally representative survey. J. Am. Geriatr. Soc. 2018, 66, 2360–2366. [Google Scholar]
- American Thoracic Society. Standardization of Spirometry, 1994 Update. American Thoracic Society. Am. J. Respir. Crit. Care Med. 1995, 152, 1107–1136. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Soliman, I.; Dylan, W.L.; Peelen, L.; Cremer, L.; Slooter, A.; Pasma, W.; Kesecioglu, J.; Dijk, D. Single-center large-cohort study into quality of life in Dutch intensive care unit subgroups, 1 year after admission, using EuroQoL EQ-6D-3L. J. Crit. Care 2015, 30, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Wytske, W. The Impact of Critical Illness: Long Term Physical, Mental and Cognitive Health Problems in ICU Survivors. 2021. Available online: https://repository.ubn.ru.nl/bitstream/handle/2066/239950/239950.pdf?sequence=1 (accessed on 9 April 2023).
- Nilsson, E.; Festin, K.; Lowen, M.; Kristenson, M. SF-36 predicts 13-year CHD incidence in a middle-age Swedish general population. Qual Life Res. 2020, 29, 971–975. [Google Scholar] [CrossRef] [Green Version]
- Family Caregiver Alliance Caregiver Assessment: Principles, Guidelines and Strategies for Change. Report from a National Consensus Development Conference. 2006. Available online: https://www.caregiver.org/sites/caregiver.org/files/pdfs/v1consensus.pdf (accessed on 22 January 2023).
- National Association of Chronic Disease Directors CDC Seeks to Protect Health of Family Caregivers. 2009. Available online: https://cdn.ymaws.com/www.chronicdiseas.org/resource/resmgr/healthy_aging_critical_issues_brief/ha_cib_healthoffamilycaregiv.pdf (accessed on 22 January 2023).
- Wintermann, G.; Petrowski, K.; Weidner, K.; Straub, B.; Rosendahl, J. Impact of post-traumatic stress symptoms on the health-related quality of life in a cohort study with chronically critically ill patients and their partners: Age matters. Crit. Care 2019, 23, 39. [Google Scholar] [CrossRef]
- Kalavina, R.; Chisati, E.; Mlenzana, N.; Mlenzana, M. The challenges and experiences of stroke patients and their spouses in Blantyre, Malawi. Wazakili Malawi Med. J. 2019, 31, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, E.; Moore, K. Stroke: Holistic care and management. Nurs. Stand. 2004, 18, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Hege, H.; Regina, E.; Ingeborg, A.; Tove, P.; Berit, S.; Stine, L.; Gorill, H. From breaking point to breakthrough during the ICU stay: A qualitative study of family members’ experiences of long-term intensive care patient’ pathway towards survival. J. Clin. Nurs. 2018, 27, 3630–3640. [Google Scholar]
- Barcellos, R.; Chatkin, J. Impact of multidisciplinary checklist on the duration of invasive mechanical ventilation and length of ICU stay. J. Bras. Pneumol. 2020, 46, 1806–3756. [Google Scholar] [CrossRef]
- Henrique, N.; Queiros, P. Patient with stroke: Hospital discharge planning, functionality and quality of life. Rev. Bras. Enferm. 2017, 70, 415–423. [Google Scholar]
- Mohamed, D.; Hashem, N.; Swaroopa, N.; Krishidhar, N.; Nausran, U.; Robinson, K.; Dinglas, V.; Needham, D.; Michelle, N. Eakin Patients’ outcomes after critical illness: A systematic review of qualitative studies following hospital discharge. Crit. Care 2016, 20, 345. [Google Scholar]
- Chun, P.; Yip, P.; Tai, J.; Lou, F. Needs of family caregivers of stroke patients: A longitudinal study of caregivers’ perspectives. Patient Prefer. Adherence 2015, 9, 449–457. [Google Scholar]
- Tran, P.; Mannen, J. Improving oral healthcare: Improving the quality of life for patients after a stroke. Spec. Care Dent. 2009, 29, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Regis, R.; Dietrich, C.; Valle, T.; Denise, S.; Tagliari, L.; Mattioni, M.; Tonietto, F.; Rosa, R.; Barbosa, G.; Lovatel, G.; et al. The 6-Minute Walk test predicts long-term physical improvement among intensive care unit survivors: A prosective study. Rev. Bras. Ter. Intensiv. 2021, 33, 374–383. [Google Scholar]
- Halliday, S.; Wang, L.; Yu, C.; Vickers, B.; Newman, J.; Fremont, R.; Huerta, L.; Brittain, E.; Hemnes, A. Six-minute walk distance in healthy young adults. Respir. Med. 2020, 165, 105933. [Google Scholar] [CrossRef]
- Herridge, M.S.; Tansey, C.M.; Matté, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional disability 5 years after acute respiratory distress syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [Green Version]
- Ferrand, N.; Zaouter, C.; Chastel, B.; Dewitte, A.; Ouattara, A.; Fleureau, C.; Roze, H. Health related quality of life and predictive factors six months after intensive care unit discharge. Anaesth. Crit. Care Pain Med. 2019, 38, 137–141. [Google Scholar] [CrossRef]
- Kattainanen, S.; Lindahl, A.; Vasankari, T.; Ollila, H.; Volmonen, K.; Piirila, P.; Kauppi, P.; Paajanen, J.; Kreivi, R.; Ulenius, L.; et al. Lung function and exersice capacity 6 months after hospital discharge for critical COVID-19. BMC Pulm. Med. 2022, 22, 243. [Google Scholar]
- Heyland, D.; Groll, D.; Caeser, M. Survivors of acute respiratory distress syndrome: Relationship between pulmonary dysfuction and long-term health-related quality of life. Crit. Care Med. 2005, 33, 1549–1556. [Google Scholar] [CrossRef]
- Rabe, K.F.; Hurd, S.; Anzueto, A.; Barnes, P.J.; Buist, S.A.; Calverley, P.; Zielinski, J. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: Gold executive summary. Am. Respir. Care Med. 2007, 176, 532–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuai, S.; Hanyujie, K.; Zhenbei, Q.; Yingquan, W.; Zhaohui, T. Effect of different levels of PEEP on mortality in ICU patients without acute respiratory distress syndrome: Systematic review and meta-analysis with trial sequential analysis. J. Crit. Care 2021, 65, 246–258. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age, years | 56.8 (17.49) |
| Female Sex, n (%) | 57 (39.86) |
| Family Status | |
| Married, n (%) | 106 (74.12) |
| Not-married, n (%) | 31 (21.68) |
| Widow/er, n (%) | 6 (4.20) |
| Accommodation | |
| Urban, n (%) | 76 (56.70) |
| Daily area, n (%) | 34 (25.40) |
| Agricultural, n (%) | 24 (17.90) |
| Education | |
| Basic education, n (%) | 28 (19.59) |
| High School graduates, n (%) | 86 (60.15) |
| Technical School graduates, n (%) | 6 (4.19) |
| University graduates, n (%) | 10 (6.99) |
| Post graduate training, n (%) | 3 (2.09) |
| No education, n (%) | 10 (6.99) |
| Type of Profession | |
| State employee, n (%) | 13 (9.09) |
| Private employee, n (%) | 25 (17.5) |
| Freelance, n (%) | 9 (6.30) |
| Farmer, n (%) | 10 (6.9) |
| Worker, n (%) | 6 (4.19) |
| Housekeeper, n (%) | 14 (9.80) |
| Retired, n (%) | 52 (36.36) |
| University student, n (%) | 5 (3.49) |
| Unemployed, n (%) | 9 (6.29) |
| Rehabilitation after ICU, n (%) | 70 (48.9) |
| Time to return to daily routine after ICU | |
| 1–6 months, n (%) | 58 (40.5) |
| 6–12 months, n (%) | 31 (21.7) |
| >12 months, n (%) | 54 (37.3) |
| Cause of Admission | |
|---|---|
| -Medical, n (%) | 79 (55.25) |
| -Pneumonia, n (%) | 6 (4.20) |
| -ARDS, n (%) | 10 (6.99) |
| -Stroke, n (%) | 31 (21.6) |
| Surgical, n (%) | 48 (33.56) |
| APACHE II score | 19 (1.1) |
| Mechanical ventilation, n (%) | 126 (88.1) |
| Mechanical ventilation duration, (median (IQR)), days | 5 (2–12) |
| ICU stay, (median (IQR)), days | 7 (3–14) |
| Hospital Stay, (median (IQR)), days | 20 (15–20) |
| Spirometry * | |
| FEV1, %pred | 69.5 (21.5) |
| FVC, %pred | 69.5 (20.4) |
| FEVI/FVC, %pred | 106 (97–121) |
| PEF, %pred | 58.5 (25.1) |
| 6MWT *, meters | 43.84 (28.79) |
| ≥Median SF36 Score N = 71 | <Median SF36 Score N = 72 | p Value | |
|---|---|---|---|
| Age, years | 54 (35–69) | 66 (52–75) | 0.0001 |
| Male, n (%) | 43 (60.5) | 42 (58.3) | 0.6 |
| Stroke, n (%) | 7 (9.8) | 24 (33.3) | 0.0001 |
| ICU stay > 10 days, n (%) | 17 (23.9) | 36 (50) | 0.001 |
| Hospital stay > 10 days, n (%) | 58 (81.6) | 69 (95.8) | 0.001 |
| FEV1, % pred | 86 (73–97.7) | 49.5 (43.2–54.7) | 0.0001 |
| FVC, % pred | 81 (68–93) | 48 (44–53.5) | 0.0001 |
| FEV1/FVC, % pred | 104 (95.5–112.5) | 46 (43–52) | 0.0001 |
| PEF, % pred | 81 (69–95) | 47 (38–51) | 0.0001 |
| 6MWT, meters | 153 (99–250) | 65 (38–101.5) | 0.0001 |
| Support by spouses 24/24 h, n (%) | 10 (14.0) | 12 (16.6) | 0.8 |
| Friends’ visits > 3/week, n (%) | 39 (54.9) | 14 (19.4) | 0.0001 |
| Family-Support > 2 members, n (%) | 61 (85.9) | 46 (63.8) | 0.001 |
| ≥Median SF36 Score N = 73 | <Median SF36 Score N = 70 | p Value | |
|---|---|---|---|
| Age, years | 54 (36.5–69) | 65.5 (53–74) | 0.0001 |
| Male, n (%) | 45 (61.6) | 40 (57.1) | 0.9 |
| Stroke, n (%) | 7 (9.6) | 24 (34.3) | 0.001 |
| ICU stay > 10 days, n (%) | 19 (26) | 39 (55.7) | 0.001 |
| Hospital stay > 10 days, n (%) | 57 (78) | 69 (97.1) | 0.002 |
| FEV1, % pred | 88 (74–100) | 54 (48.5–58.5) | 0.0001 |
| FVC, % pred | 84 (78–99) | 60 (52–65) | 0.0001 |
| FEV1/FVC, % pred | 104 (95.5–112.5) | 46 (43–52) | 0.0001 |
| PEF, % pred | 88 (78–97) | 49 (39.5–55) | 0.0001 |
| 6MWT, meters | 170 (106–250) | 36.6 (7.5–58) | 0.0001 |
| Support by spouses 24/24 h, n (%) | 12 (16.4) | 10 (14.3) | 0.3 |
| Friends’ visits > 3/week, n (%) | 36 (49.3) | 17 (24.3) | 0.001 |
| Family-Support > 2 members, n (%) | 60 (82.2) | 47 (67.1) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avgeri, K.; Zakynthinos, E.; Tsolaki, V.; Sgantzos, M.; Fotakopoulos, G.; Makris, D. Quality of Life and Family Support in Critically Ill Patients following ICU Discharge. Healthcare 2023, 11, 1106. https://doi.org/10.3390/healthcare11081106
Avgeri K, Zakynthinos E, Tsolaki V, Sgantzos M, Fotakopoulos G, Makris D. Quality of Life and Family Support in Critically Ill Patients following ICU Discharge. Healthcare. 2023; 11(8):1106. https://doi.org/10.3390/healthcare11081106
Chicago/Turabian StyleAvgeri, Konstantina, Epaminondas Zakynthinos, Vasiliki Tsolaki, Markos Sgantzos, George Fotakopoulos, and Demosthenes Makris. 2023. "Quality of Life and Family Support in Critically Ill Patients following ICU Discharge" Healthcare 11, no. 8: 1106. https://doi.org/10.3390/healthcare11081106