
Engaging Leadership and Psychological Safety as Moderators of the Relationship between Strain and Work Recovery: A Cross-Sectional Study of HSS Employees

 , and
, and 
Abstract
:1. Introduction
Potential Job Resouces
2. Materials and Methods
2.1. Measures
2.2. Methods
3. Results
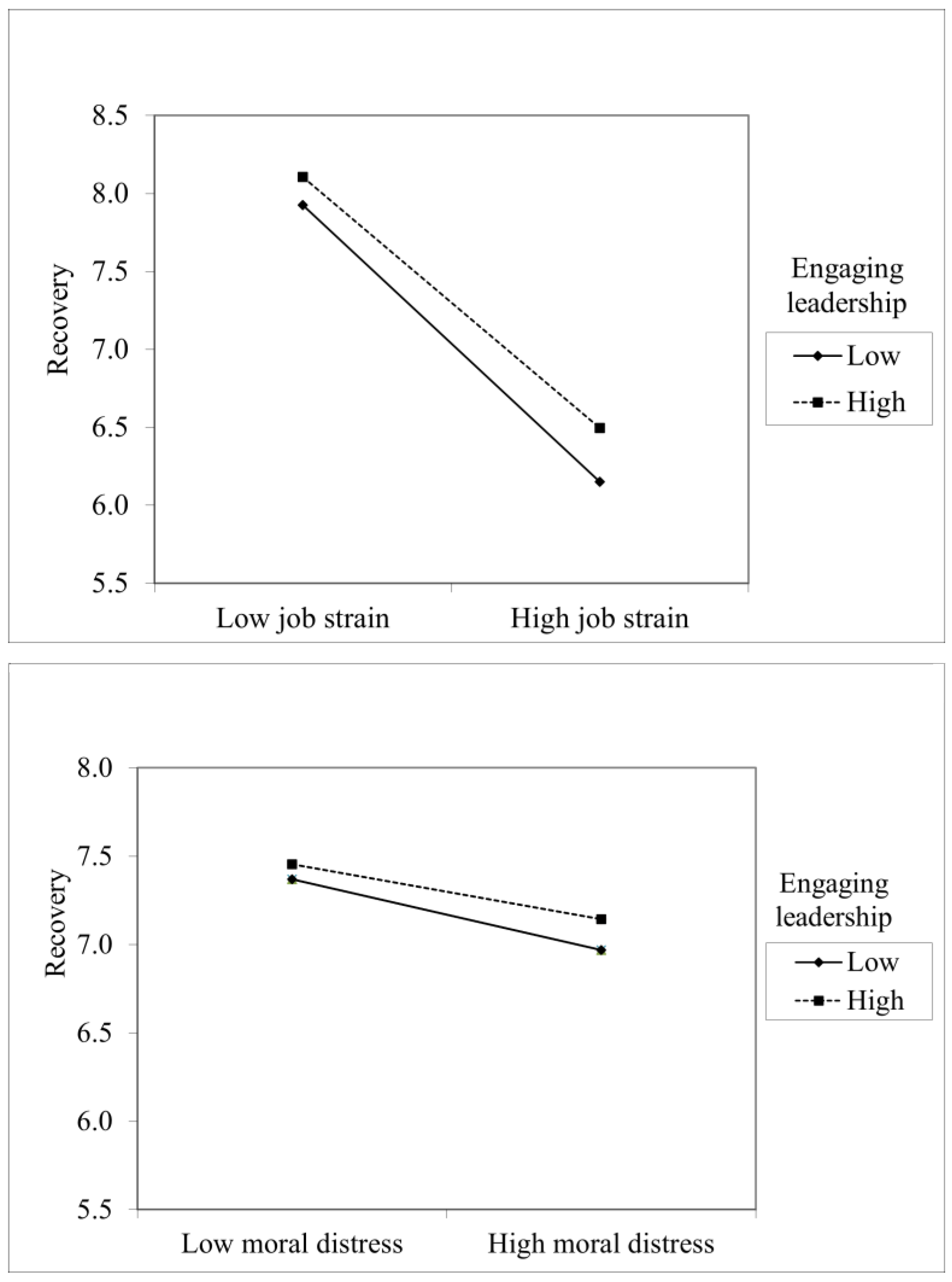
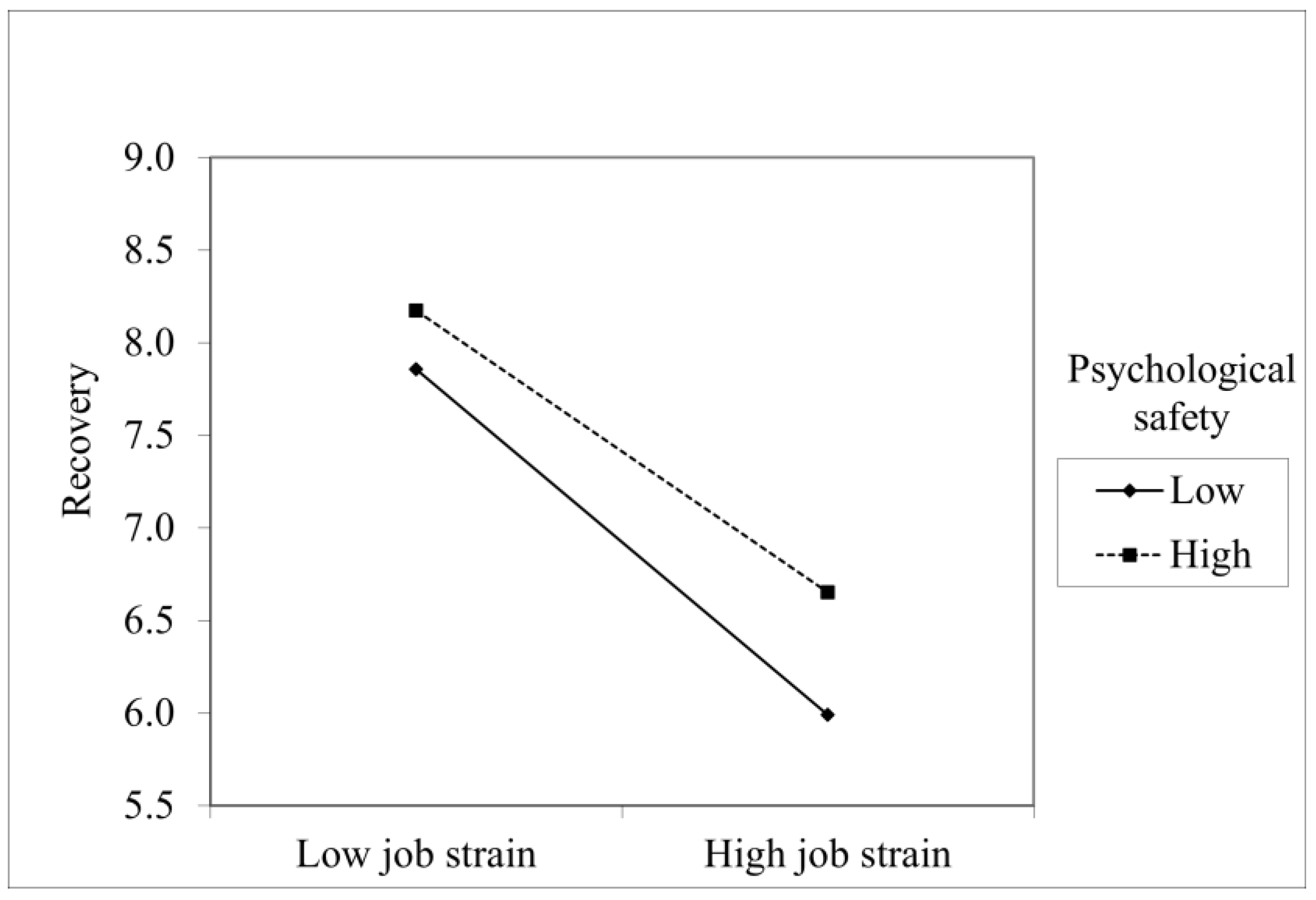
Associations between Work Recovery, Job Demands and Job Resources
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Selander, K.; Nikunlaakso, R.; Laitinen, J. Association between work ability and work stressors: Cross-sectional survey of elderly services and health and social care service employees. Arch. Public Health 2022, 80, 83. [Google Scholar] [CrossRef] [PubMed]
- Juvani, A.; Oksanen, T.; Virtanen, M.; Salo, P.; Pentti, J.; Kivimäki, M.; Vahtera, J. Clustering of job strain, effort-reward imbalance, and organizational injustice and the risk of work disability: A cohort study. Scand. J. Work Environ. Health 2018, 44, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Carse, A.; Rushton, C.H. Harnessing the Promise of Moral Distress: A Call for Re-Orientation. J. Clin. Ethics. 2017, 28, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Fourie, C. Moral distress and moral conflict in clinical ethics. Bioethics 2015, 29, 91–97. [Google Scholar] [CrossRef]
- Rivera, A.S.; Akanbi, M.; O′Dwyer, L.C.; McHugh, M. Shift work and long work hours and their association with chronic health conditions: A systematic review of systematic reviews with meta-analyses. PLoS ONE 2020, 15, e0231037. [Google Scholar] [CrossRef]
- Kivimäki, M.; Batty, G.D.; Hublin, C. Shift Work as a Risk Factor for Future Type 2 Diabetes: Evidence, Mechanisms, Implications, and Future Research Directions. PLoS Med. 2011, 8, e1001138. [Google Scholar] [CrossRef]
- Sonnentag, S.; Cheng, B.H.; Parker, S.L. Recovery from work: Advancing the field toward the future. Annu. Rev. Organ. Psychol. Organ. Behav. 2022, 9, 33–60. [Google Scholar] [CrossRef]
- Verbeek, J.; Ruotsalainen, J.; Laitinen, J.; Korkiakangas, E.; Lusa, S.; Mänttäri, S.; Oksanen, T. Interventions to enhance recovery in healthy workers: A scoping review. Occup. Med. 2019, 69, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Steed, L.B.; Swider, B.W.; Keem, S.; Liu, J.T. Leaving work at work: A meta-analysis on employee recovery from work. J. Manag. 2021, 47, 867–897. [Google Scholar] [CrossRef]
- Sonnetag, S.; Venz, L.; Casper, A. Advances in recovery research: What have we learned? What should be done next? J. Occup. Health Psychol. 2017, 22, 365–380. [Google Scholar] [CrossRef]
- Sonnetag, S.; Fritz, C. Recovery Experience Questionnaire: Development and validation of a measure assessing recuperation and unwinding form work. J. Occup. Health Psychol. 2007, 12, 204–221. [Google Scholar] [CrossRef] [Green Version]
- Newman, D.B.; Tay, L.; Diener, E. Leisure and subjective well-being: A model of psychological mechanisms as mediating factors. J. Happiness Stud. 2014, 15, 555–578. [Google Scholar] [CrossRef]
- Härmä, M.; Shiri, R.; Ervasti, J.; Karhula, K.; Turunen, J.; Koskinen, A.; Ropponen, A.; Sallinen, M. National recommendations for shift scheduling in healthcare: A 5-year prospective cohort study on working hour characteristics. Int. J. Nur. Stud. 2022, 134, 104321. [Google Scholar] [CrossRef] [PubMed]
- Blasche, G.; Bauböck, V.M.; Haluza, D. Work-related self-assessed fatigue and recovery among nurses. Int. Arch. Occup. Environ. Health 2017, 90, 197–205. [Google Scholar] [CrossRef]
- Virtanen, A.; Van Laethem, M.; de Bloom, J.; Kinnunen, U. Drammatic breaks: Break recovery experiences as mediators between job demands and affect in the afternoon and evening. Stress Health 2021, 34, 801–818. [Google Scholar] [CrossRef] [PubMed]
- Sianoja, M.; Kinnunen, U.; de Bloom, J.; Korpela, K.; Geurts, S. Recovery during Lunch Breaks: Testing Long-Term Relations with Energy Levels at Work. Scand. J. Work Organ. Psychol. 2016, 1, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Sonnentag, S.; Binnewies, C.; Mojza, E.J. “Did you have a nice evening?” A day-level study on recovery experiences, sleep, and affect. J. Appl. Psychol. 2008, 93, 674–684. [Google Scholar] [CrossRef] [Green Version]
- Fritz, C.; Sonnentag, S. Recovery, well-being, and performance-related outcomes: The role of workload and vacation experiences. J. Appl. Psychol. 2006, 91, 936–945. [Google Scholar] [CrossRef] [Green Version]
- Fritz, C.; Sonnentag, S. Recovery, Health, and Job Performance: Effects of Weekend Experiences. J. Occup. Health Psychol. 2005, 10, 187–199. [Google Scholar] [CrossRef] [Green Version]
- Kinnunen, U.; Feldt, T.; Siltaloppi, M.; Sonnentag, S. Job demands–resources model in the context of recovery: Testing recovery experiences as mediators. Eur. J. Work Organ. Psychol. 2011, 20, 805–832. [Google Scholar] [CrossRef] [Green Version]
- Demerouti, E.; Bakker, A.B.; Nachreiiner, F.; Schaufeli, W.B. The job demands–resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B. Job demands, job resources, and their relationship with burnout and engagement: A multi-sample study. J. Organ. Behav. 2004, 25, 293–315. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Demerouti, E. Job demands-resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef]
- Bennett, A.A.; Bakker, A.B.; Field, J.G. Recovery from work-related effort: A meta-analysis. J. Organ. Behav. 2018, 39, 262–275. [Google Scholar] [CrossRef]
- Breevaart, K.; Bakker, A.B.; Hetland, J.; Demerouti, E.; Olsen, O.K.; Espevik, R. Daily transactional and transformational leadership and daily employee engagement. J. Occup. Organ. Psychol. 2014, 87, 138–157. [Google Scholar] [CrossRef]
- Tummers, L.; Bakker, A.B. Leadership and Job Demands-Resources Theory: A Systematic Review. Front. Psychol. 2021, 12, 722080. [Google Scholar] [CrossRef]
- Schaufeli, W. Engaging leadership in the job demands-resources model. Career Dev. Int. 2015, 20, 446–463. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.; Deci, E. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef]
- Nikolova, I.; Schaufeli, W.; Notelaers, G. Engaging leader–Engaged employees? A cross-lagged study on employee engagement. Eur. Manag. J. 2019, 37, 772–783. [Google Scholar] [CrossRef]
- Schaufeli, W. Engaging leadership: How to promote work engagement? Front. Psychol. 2021, 12, 754556. [Google Scholar] [CrossRef]
- Bakker, A.B.; de Vries, J.D. Job Demands–Resources theory and self-regulation: New explanations and remedies for job burnout. Anxiety Stress Coping 2021, 34, 1–21. [Google Scholar] [CrossRef]
- Rivkin, W.; Diestel, S.; Schmidt, K.H. The positive relationship between servant leadership and employees’ psychological health: A multi-method approach. Ger. J. Hum. Resour. Man. 2014, 28, 52–72. [Google Scholar] [CrossRef]
- Edmondson, A. Psychological safety and learning behavior in work teams. Adm. Sci. Q. 1999, 44, 350–383. [Google Scholar] [CrossRef] [Green Version]
- Edmondson, A.C.; Lei, Z. Psychological safety: The history, renaissance, and future of an interpersonal construct. Annu. Rev. Organ. Psychol. Organ. Behav. 2014, 1, 23–43. [Google Scholar] [CrossRef] [Green Version]
- Karabinski, T.; Haun, V.C.; Nübold, A.; Wendsche, J.; Wegge, J. Interventions for improving psychological detachment from work: A meta-analysis. J. Occup. Health Psychol. 2021, 26, 224–242. [Google Scholar] [CrossRef]
- Frazier, M.L.; Fainshmidt, S.; Klinger, R.L.; Pezeshkan, A.; Vracheva, V. Psychological safety: A meta-analytic review and extension. Pers. Psychol. 2017, 70, 113–165. [Google Scholar] [CrossRef] [Green Version]
- Newman, A.; Donohue, R.; Eva, N. Psychological safety: A systematic review of the literature. Hum. Resour. Manag. Rev. 2017, 27, 521–535. [Google Scholar] [CrossRef]
- Ma, Y.; Faraz, N.A.; Ahmed, F.; Iqbal, M.K.; Saeed, U.; Mughal, M.F.; Raza, A. Curbing nurses’ burnout during COVID-19: The roles of servant leadership and psychological safety. J. Nurs. Manag. 2021, 29, 2383–2391. [Google Scholar] [CrossRef]
- Kinnunen, U.; Feldt, T. Job Characteristics, Recovery Experiences and Occupational Well-being: Testing Cross-lagged Relationships across 1 Year. Stress Health 2013, 29, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef]
- Courvoisier, D.S.; Perneger, T.V. Validation of alternative formulations of job strain. J. Occup. Health 2010, 52, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, L. Good intentions aside. In A Manger’s Guide to Resolving Ethical Problems; Harvard Business School Press: Boston, MA, USA, 1993. [Google Scholar]
- Anderson, N.R.; West, M.A. Measuring climate for work group innovation: Development and validation of the Team Climate Inventory. J. Organ. Behav. 1998, 19, 235–258. [Google Scholar] [CrossRef]
- Ferrie, J.E.; Kivimäki, M.; Westerlund, H.; Head, J.; Melchior, M.; Singh-Manoux, A.; Zins, M.; Goldberg, M.; Alexanderson, K.; Vahtera, J. Differences in the association between sickness absence and long-term sub-optimal health by occupational position: A 14-year follow-up in the GAZEL cohort. Occup. Environ. Med. 2011, 68, 729–733. [Google Scholar] [CrossRef] [Green Version]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage: Newbury Park, CA, USA, 1991. [Google Scholar]
- Koivisto, T.; Sinervo, T.; Laitinen, J. Hyvä Veto! Henkilöstön Saatavuuden ja Alan Vetovoimaisuuden Turvaaminen Iäkkäiden Palveluissa Loppuraportti; Finnish Institute of Occupational Health: Helsinki, Finland, 2023; (In Finnish, abstract in English); Available online: https://urn.fi/URN:ISBN:978-952-391-075-1 (accessed on 27 March 2023).
- Nikunlaakso, R.; Selander, K.; Oksanen, T.; Laitinen, J. Interventions to reduce the risk of mental health problems in health and social care workplaces: A scoping review. J. Psychiatr. Res. 2022, 152, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Nikunlaakso, R.; Selander, K.; Weiste, E.; Korkiakangas, E.; Paavolainen, M.; Koivisto, T.; Laitinen, J. Understanding Moral Distress among Eldercare Workers: A Scoping Review. Int. J. Environ. Health Res. 2022, 19, 9303. [Google Scholar] [CrossRef] [PubMed]
- Duchaine, C.S.; Aube, K.; Gilbert-Ouimet, M.; Vezina, M.; Ndjaboue, R.; Massamba, V.; Talbot, D.; Lavigne-Robichaud, M.; Trudel, X.; Pena-Gralle, A.P.B.; et al. Psychosocial Stressors at Work and the Risk of Sickness Absence Due to a Diagnosed Mental Disorder: A Systematic Review and Meta-analysis. JAMA Psychiatry 2020, 77, 842–851. [Google Scholar] [CrossRef]
- de Vries, J.D.; van Hooff, M.L.; Geurts, S.A.; Kompier, M.A. Exercise to reduce work-related fatigue among employees: A randomized controlled trial. Scand. J. Work Environ. Health 2017, 4, 337–349. [Google Scholar] [CrossRef]
- Lidegaard, M.; Søgaard, K.; Krustrup, P.; Holtermann, A.; Korshøj, M. Effects of 12 months aerobic exercise intervention on work ability, need for recovery, productivity and rating of exertion among cleaners: A worksite RCT. Int. Arch. Occup. Environ. Health 2018, 91, 225–235. [Google Scholar] [CrossRef] [Green Version]
- Ding, J.; Gehrman, P.R.; Liu, S.; Yang, F.; Ma, R.; Jia, Y.; Yang, X. Recovery Experience as the Mediating Factor in the Relationship Between Sleep Disturbance and Depressive Symptoms Among Female Nurses in Chinese Public Hospitals: A Structural Equation Modeling Analysis. Psychol. Res. Behav. Manag. 2020, 13, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Krueger, J.; Frank, M.G.; Wisor, J.P.; Roy, S. Sleep function: Toward elucidating an enigma. Sleep Med. Rev. 2016, 28, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Olafsen, A.H.; Niemiec, C.P.; Halvari, H.; Deci, E.; Williams, G.C. On the dark side of work: A longitudinal analysis using self-determination theory. Eur. J. Work Organ. Psychol. 2017, 26, 275–285. [Google Scholar] [CrossRef]
- Ahmed, F.; Zhao, F.; Faraz, N.A. How and When Does Inclusive Leadership Curb Psychological Distress During a Crisis? Evidence From the COVID-19 Outbreak. Front. Psychol. 2020, 11, 1898. [Google Scholar] [CrossRef] [PubMed]
- Chughtai, A.A. Servant leadership and follower outcomes: Mediating effects of organizational identification and psychological safety. J. Psychol. 2016, 150, 866–880. [Google Scholar] [CrossRef] [PubMed]
- Schaubroeck, J.; Lam, S.S.K.; Peng, A.C. Cognition-based and affect-based trust as mediators of leader behaviour influences on team performance. J. Appl. Psychol. 2011, 96, 863–871. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) | Recovery from Work, Mean (95%CI) | |||||
|---|---|---|---|---|---|---|
| All HSS Employees | Eldercare | Other HSS Employees | All HSS Employees | Eldercare | Other HSS Employees | |
| Gender | ||||||
| Males | 2950 (13%) | 194 (4%) | 2756 (15%) | 6.91 (6.82–6.99) | 6.26 (5.91–6.62) | 6.95 (6.86–7.04) |
| Females | 19,552 (87%) | 4153 (96%) | 15,399 (85%) | 6.28 (6.24–6.31) | 5.84 (5.77–5.92) | 6.39 (6.36–6.43) |
| Age | ||||||
| Less than 35 | 5135 (23%) | 925 (21%) | 4210 (23%) | 6.07 (6.00–6.13) | 5.41 (5.25–5.58) | 6.21 (6.14–6.28) |
| 35–54 | 11,722 (52%) | 2137 (49%) | 9585 (53%) | 6.38 (6.34–6.43) | 5.90 (5.79–6.00) | 6.49 (6.45–6.54) |
| 55+ | 5645 (25%) | 1285 (30%) | 4360 (24%) | 6.57 (6.51–6.54) | 6.13 (5.99–6.26) | 6.70 (6.63–6.77) |
| Supervisory position | ||||||
| Yes | 20,653 (8%) | 177 (4%) | 1590 (9%) | 7.02 (6.91–7.14) | 6.85 (6.32–7.38) | 7.03 (6.91–7.15) |
| No | 1767 (92%) | 4156 (96%) | 16,497 (91%) | 6.26 (6.23–6.29) | 5.80 (5.72–5.88) | 6.38 (6.35–6.42) |
| Shift work | ||||||
| Yes | 10,813 (48%) | 3371 (78%) | 7442 (41%) | 5.80 (5.75–5.85) | 5.60 (5.52–5.69) | 5.89 (5.83–5.95) |
| No | 11,639 (52%) | 966 (22%) | 10,673 (59%) | 6.84 (6.79–6.88) | 6.71 (6.55–6.87) | 6.85 (6.80–6.89) |
| Perceived health | ||||||
| Poor | 5434 (24%) | 1327 (31%) | 4107 (23%) | 4.95 (4.88–5.01) | 4.58 (4.45–4.71) | 5.06 (4.99–5.14) |
| Good | 17,022 (76%) | 3011 (69%) | 14,011 (73%) | 6.81 (6.78–6.84) | 6.43 (6.34–6.51) | 6.89 (6.86–6.93) |
| Occupations | ||||||
| Administration and clerical | 2794 (13%) | 119 (3%) | 2675 (16%) | 7.06 (6.97–7.14) | 6.97 (6.60–7.35) | 7.06 (6.98–7.15) |
| Nutrition and cleaning | 725 (4%) | 86 (2%) | 639 (4%) | 6.29 (6.11–6.47) | 6.60 (6.08–7.13) | 6.25 (6.05–6.44) |
| Practical nurses | 4816 (23%) | 3015 (72%) | 1801 (11%) | 5.92 (5.85–5.99) | 5.66 (5.56–5.75) | 6.36 (6.25–6.47) |
| Nurses | 7068 (34%) | 689 (16%) | 6379 (38%) | 5.94 (5.88–5.99) | 5.91 (5.72–6.09) | 5.94 (5.88–6.00) |
| Social workers and social counselors | 2081 (10%) | 173 (4%) | 1908 (12%) | 6.61 (6.52–6.71) | 6.48 (6.13–6.83) | 6.63 (6.53–6.73) |
| Other HSS occupations | 3367 (16%) | 118 (3%) | 3249 (20%) | 6.85 (6.77–6.92) | 6.85 (6.41–7.28) | 6.85 (6.77–6.93) |
| N | 22,247 | 4276 | 17,971 | 6.36 (6.33–6.39) | 5.86 (5.79–5.94) | 6.48 (6.44–6.51) |
| Step1 | Step2 | Step3 | Step4 | Step5 | |
|---|---|---|---|---|---|
| Eldercare (ref. = other HSS employees) | −0.10 *** | −0.02 ** | 0.01 | 0.03 | 0.00 |
| Gender (ref. = females) | 0.07 *** | 0.04 *** | 0.04 *** | 0.04 *** | |
| Age | 0.10 *** | 0.09 *** | 0.10 *** | 0.10 *** | |
| Supervisory position (ref. = yes) | −0.02 ** | −0.01 * | −0.03 *** | −0.03 *** | |
| Shift work (ref. = yes) | 0.16 *** | 0.10 *** | 0.10 *** | 0.10 *** | |
| Perceived health (ref. = poor) | 0.34 *** | 0.26 *** | 0.25 *** | 0.26 *** | |
| Occupation (ref. = other HSS occupations) | |||||
| Administration and clerical | 0.02 * | 0.02 * | 0.02 * | 0.02 ** | |
| Nutrition and cleaning | −0.00 | −0.00 | 0.00 | 0.00 | |
| Practical nurse | −0.04 *** | −0.01 | −0.01 | −0.01 | |
| Nurse | −0.10 *** | −0.03 ** | −0.03 ** | −0.03 *** | |
| Social workers and social counselors | −0.01 | −0.02 ** | −0.02 ** | −0.02 *** | |
| Job strain | −0.39 *** | −0.35 *** | −0.35 *** | ||
| Moral distress | −0.10 *** | −0.09 *** | −0.09 *** | ||
| Engaging leadership | 0.05 *** | 0.05 *** | |||
| Psychological safety | 0.08 *** | 0.08 *** | |||
| Engaging leadership*Job strain | 0.02 ** | ||||
| Engaging leadership*Moral distress | 0.02 * | ||||
| Psychological safety*Job strain | 0.03 *** | ||||
| Psychological safety*Moral distress | 0.01 | ||||
| F change (df1, df2) | 226.25 (1, 22,077) *** | 446.24 (10, 22,067) *** | 2715.82 (2, 22,065) *** | 195.69 (2, 22,063) *** | 23.33 (4, 22,059) *** |
| Adj. R2 | 0.01 | 0.18 | 0.34 | 0.35 | 0.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selander, K.; Korkiakangas, E.; Toivanen, M.; Yli-Kaitala, K.; Kangas, H.; Nevanperä, N.; Laitinen, J. Engaging Leadership and Psychological Safety as Moderators of the Relationship between Strain and Work Recovery: A Cross-Sectional Study of HSS Employees. Healthcare 2023, 11, 1045. https://doi.org/10.3390/healthcare11071045
Selander K, Korkiakangas E, Toivanen M, Yli-Kaitala K, Kangas H, Nevanperä N, Laitinen J. Engaging Leadership and Psychological Safety as Moderators of the Relationship between Strain and Work Recovery: A Cross-Sectional Study of HSS Employees. Healthcare. 2023; 11(7):1045. https://doi.org/10.3390/healthcare11071045
Chicago/Turabian StyleSelander, Kirsikka, Eveliina Korkiakangas, Minna Toivanen, Kirsi Yli-Kaitala, Hilpi Kangas, Nina Nevanperä, and Jaana Laitinen. 2023. "Engaging Leadership and Psychological Safety as Moderators of the Relationship between Strain and Work Recovery: A Cross-Sectional Study of HSS Employees" Healthcare 11, no. 7: 1045. https://doi.org/10.3390/healthcare11071045