
Effects of Digital Learning and Virtual Reality in Port-A Catheter Training Course for Oncology Nurses: A Mixed-Methods Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Setting
2.3. Intervention
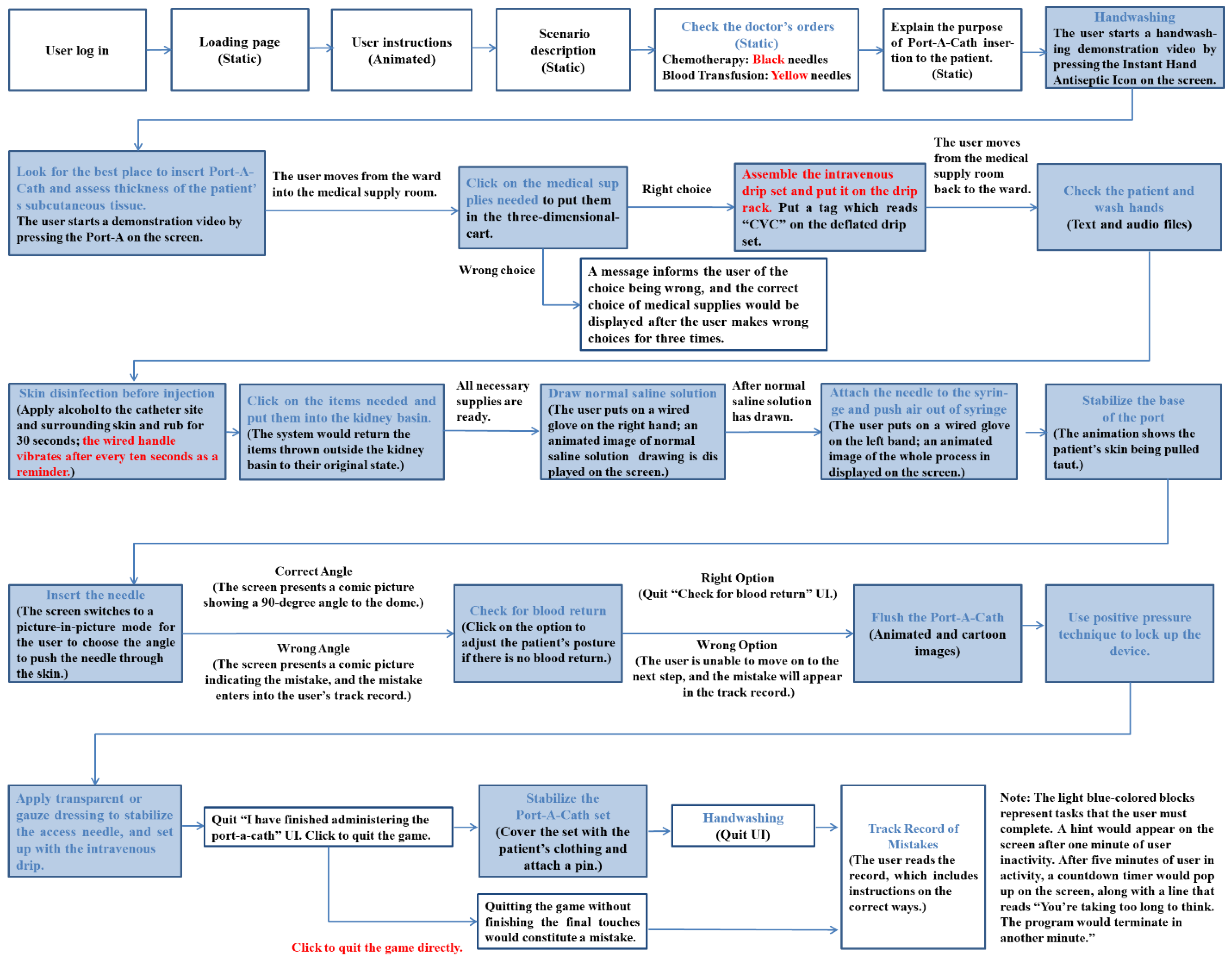
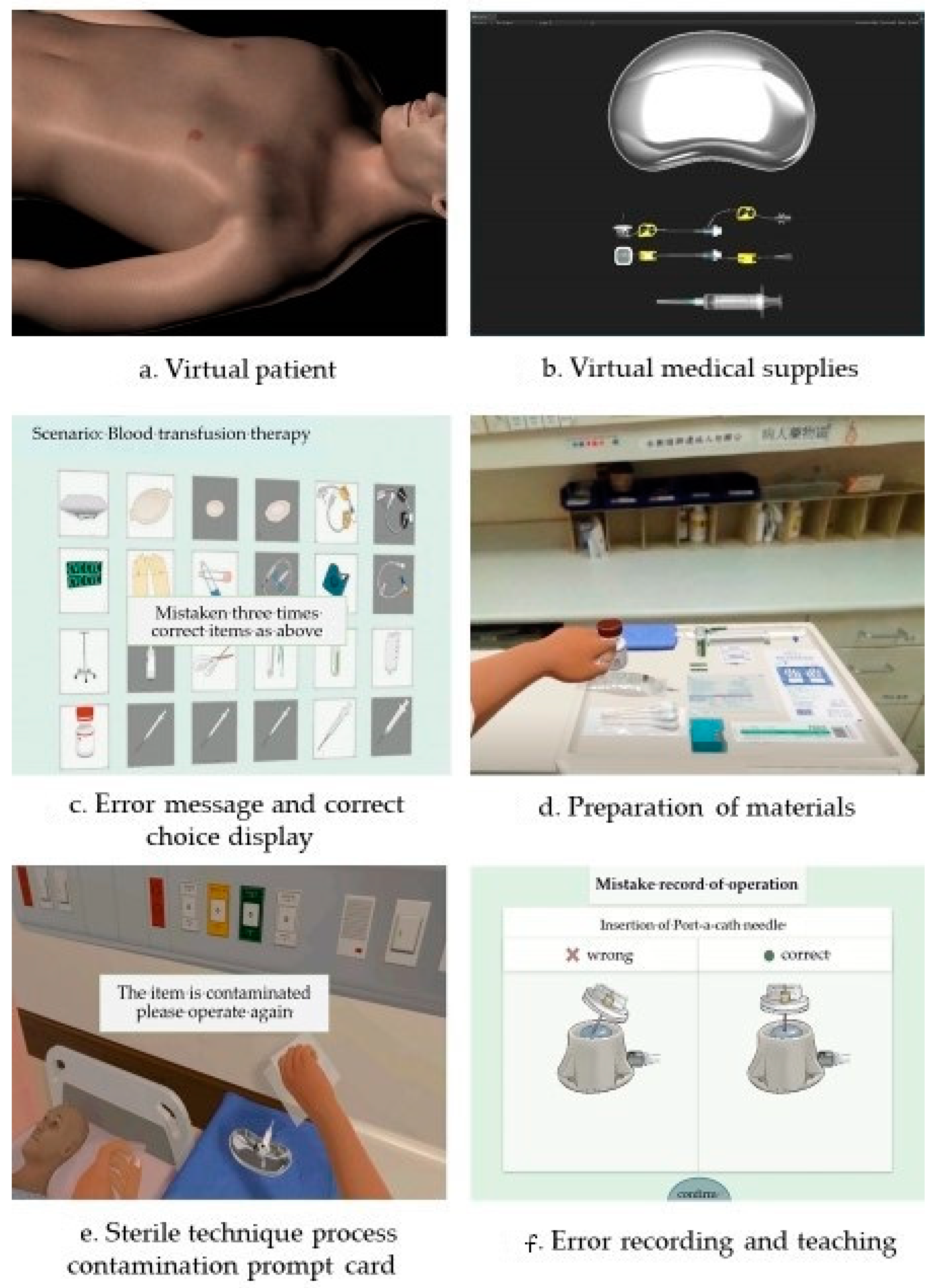
2.3.1. VR Intervention of a Real-Situated Teaching System on Implanted Port-A Catheter Care
Development of the Virtual Reality Teaching System
Digital Course of “Implanted Port-A Abnormality Management and Preventive Care”
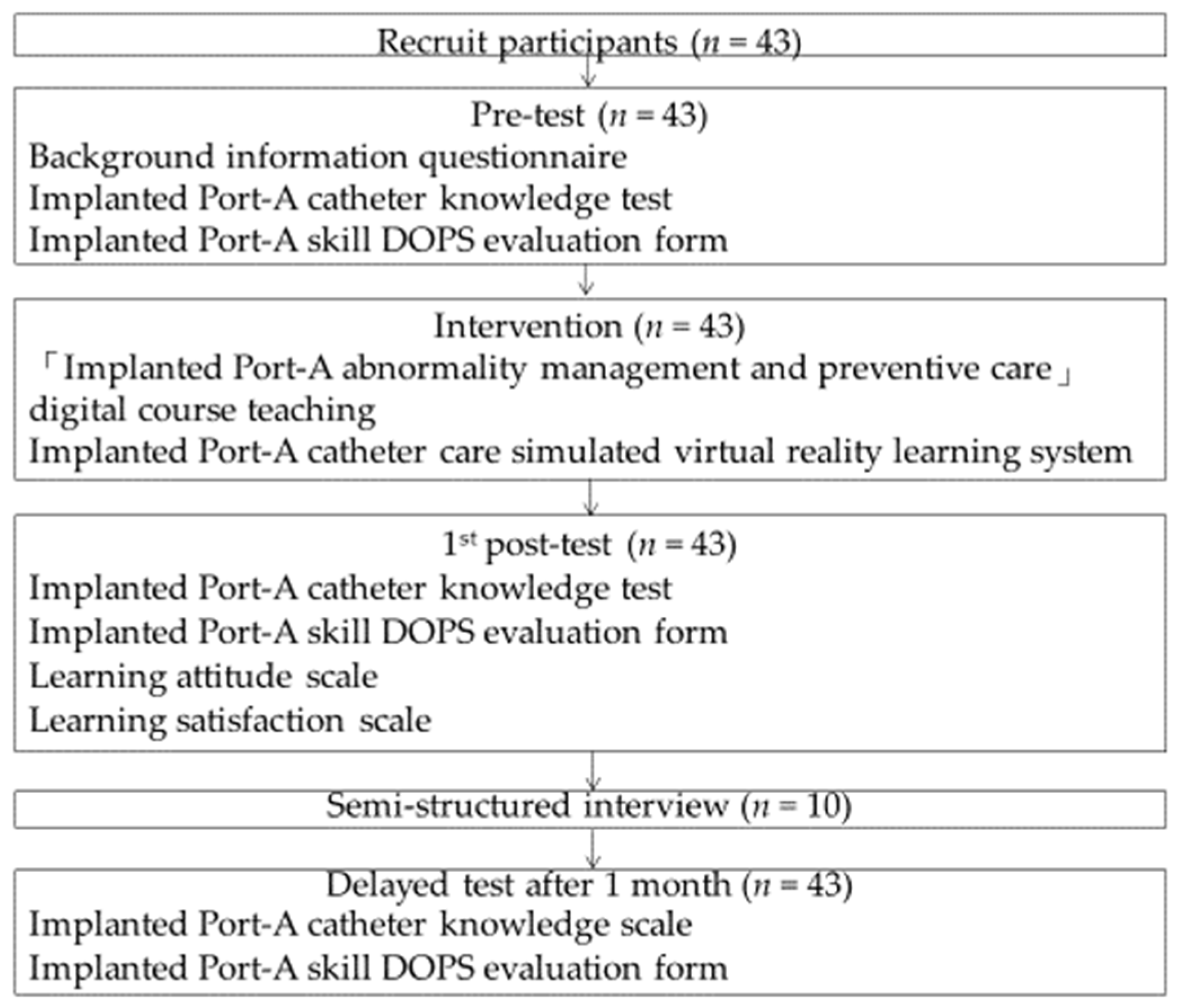
2.3.2. Interventional Procedures
2.4. Instruments
2.4.1. Background Information Questionnaire
2.4.2. Port-A DOPS Evaluation Form
2.4.3. Virtual Reality Teaching System Knowledge Scale of Implanted Port-A Catheter
2.4.4. Virtual Reality Teaching System: Learning Attitude Scale for Implanted Port-A Catheter
2.4.5. Virtual Reality Teaching System Satisfaction Questionnaire for Implanted Port-A Catheter
2.4.6. Interview
2.5. Procedure
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Background Information
3.2. Use Status of Virtual Reality Teaching Intervention Learning System on Implanted Port-A Catheter Care
3.3. Within-Subjects Effects on Knowledge and Skills
3.3.1. Knowledge Test of Implanted Port-A Catheter
3.3.2. Port-A Catheter Curved Needle Injection Skill
3.4. Learning Attitude
3.5. Satisfaction
3.6. Use Experience from an Interview
3.6.1. Impressive and Realistic Virtual Reality (VR) Scenario
S1: “In the past, we learned from books or slide presentations, but this time we learned through VR. We got immediate feedback such as incorrect or inappropriate operation of particular steps. It’s very impressive.”;
S8: “It reduces the waste of consumables. If we practice like we used to, the repeated opening of sterile consumables made our management of sterile technique less accurate, and the fluency of wearing gloves is not as good as in VR.”;
S10: “The experience of push/stop is quite impressive. It is carried out by pressing a flat disc, which is similar to the amount I push during actual clinical practice. Therefore, I can know whether the amount I push each time is OK or not for tube washing. It helps me to know whether the amount I push during actual clinical practice is OK or not.”
3.6.2. Virtual Reality Practice Is Helpful
S1: “It’s helpful. There were vibration reminders for some movements. I am worried about not going through a certain point, so I am more attentive, more careful, and more precise when performing each movement. I am very afraid of making mistakes.”;
S3: “It’s helpful because it allows me to self-evaluate while self-learning.”;
S6: “It’s helpful, especially for getting familiar with the preparation and the initial treatment when there is no blood return.”
3.6.3. Willing to Learn with Virtual Reality in the Future
S1: “If there are continued VR courses in the future, I will be willing to learn because passing them successfully will give me a great sense of accomplishment.”;
S2: “I think it’s pretty fun, and the experience is quite fresh. If there are continued VR courses in the future, I will continue to learn.”;
S8: “I am willing to learn because I think this will save a lot of time. The preceptor may not even need to be there. I can keep practicing without any problems.”
3.6.4. Limitations of Virtual Reality Systems
S2: “Overall, this system is good, however, there was no real sense while inserting the needle. In addition, the sensation in this system is somehow not friendly for the shorter learners.”;
S5: “I think it’s more accurate to say that this is a limitation of current VR technology rather than a drawback to handle fine motor skills in VR experience. And it still needs to be combined with actual clinical practice.”;
S7: “It’s better to have the VR experience in a wider area, so it is less likely to collide. It is difficult to simulate actual conditions when it comes to fixed needle insertion force.”
3.6.5. Direction for the Planning of Future Curriculum
S6: “I suggest using VR for pre-job training. I can practice repeatedly on my own, which would better prepare me with more complete prior knowledge before I carry out real clinical operations on patients. I will have more confidence, and it will be very helpful.”;
S10: “I think the preceptor can first demonstrate the VR operation during pre-job training, and then let them practice on their own. I think it will be very effective. It will allow new students to focus on learning the technical process, rather than being confused by too much information from the preceptor during pre-job training. After we have mastered the technical skills, the preceptor can guide us on how to deal with other problems in the clinical setting, which I think will be better.”
4. Discussion
4.1. Learning Theory of Virtual Reality Teaching
4.2. Effectiveness of the Knowledge Test on Implantable Port-A Catheter
4.3. Effectiveness of Implantable Port-A DOPS Assessment
4.4. Evaluation of Learning Attitude
4.5. Learning System Satisfaction
4.6. Learning Experience with Virtual Reality Teaching Materials
The Learning Experience of Virtual Reality Materials Using an Interview
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T1 | T2 | T3 | RM-ANOVA | Post Hoc Analysis | |||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Mean (SD) | Mean (SD) | Mean (SD) | F Value | p Value | Partial η2 | F Test | F Value | p Value |
| Total knowledge test scores (13 items) | |||||||||
| T1-T2-T3 | 9.53 (2.23) | 10.79 (1.47) | 10.84 (1.46) | 17.14 | <0.0001 | 0.290 | T2 > T1 | 25.85 | <0.0001 |
| Total DOPS scores (8 items) | |||||||||
| T1-T2-T3 | 29.35 (6.54) | 36.93 (4.66) | 39.26 (3.49) | 90.45 | <0.0001 | 0.683 | T2 > T1 | 65.27 | <0.0001 |
| Overall, DOPS performance | |||||||||
| T1-T2-T3 | 3.65 (0.87) | 4.63 (0.66) | 4.91 (0.53) | 94.59 | <0.0001 | 0.693 | T2 > T1 | 68.98 | <0.0001 |
| Dissatisfied | Common | Satisfied | ||||
|---|---|---|---|---|---|---|
| No | Item | n (%) | n (%) | n (%) | Mean (SD) | Rank |
| 1 | The virtual reality teaching system’s difficulty is at moderate level | 1 (2.3) | 4 (9.3) | 38 (88.4) | 4.19 (0.70) | 6 |
| 2 | The virtual reality teaching system covers appropriate scopes | 1 (2.3) | 2 (4.7) | 40 (93.0) | 4.35 (0.69) | 3 |
| 3 | The learning process for the virtual reality teaching system is sequential and logical | 1 (2.3) | 4 (9.3) | 38 (88.4) | 4.35 (0.75) | 2 |
| 4 | The virtual reality teaching system’s process is clear | 0 (0.0) | 5 (11.6) | 38 (88.4) | 4.30 (0.67) | 4 |
| 5 | The virtual reality teaching system aligns with real-world curriculum | 0 (0.0) | 3 (7.0) | 40 (93.0) | 4.42 (0.63) | 1 |
| 6 | I am satisfied with the overall effectiveness of learning using the virtual reality teaching system | 1 (2.3) | 3 (7.0) | 39 (90.7) | 4.23 (0.68) | 5 |
| Grand mean of percent/mean (SD) | 1.53 | 8.15 | 90.32 | 4.31 (0.58) |
References
- Ministry of Health and Welfare. 2021 National Statiatical Results of National Death Causes. 2022. Available online: https://www.mohw.gov.tw/cp-16-70314-1.html (accessed on 1 January 2023).
- Health Promotion Administration, Ministry of Health and Welfare Taiwan. Canncer Registry Annual Report, 2020 Taiwan. 2020. Available online: https://www.hpa.gov.tw/File/Attach/16434/File_20339.pdf. (accessed on 1 January 2023).
- National Cancer Institute. Types of Cancer Treatment. Available online: https://www.cancer.gov/about-cancer/treatment/types (accessed on 1 January 2023).
- World Cancer Research Fund International. Worldwide Cancer Data. Available online: https://www.wcrf.org/cancer-trends/worldwide-cancer-data/ (accessed on 1 January 2023).
- Conley, S.B.; Buckley, P.; Magarace, L.; Hsieh, C.; Pedulla, L.V. Standardizing Best Nursing Practice for Implanted Ports. J. Infus. Nurs. 2017, 40, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Sharour, L.A. Oncology Nurses’ Knowledge about Central Line Catheter: Caring, Complications, and Applications among Cancer Patients—A Cross-Sectional Study. J. Vasc. Nurs. 2018, 36, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.Y. Reduce the Error Rate of Port-A Injection Performed by New Nurses. In 2016 Oncology Nursing Research Presentation; Taiwan Oncology Nursing Society: Taipei City, Taiwan, 2016. [Google Scholar]
- Chuang, Y.S.; Lee, S.C.; Kao, Y.L.; Huang, H.H.; Li, C.L.; Kao, Y.C.; Hsiang, Y.J.; Chen, Y.H. Use of a Medical Breakthrough Series Technique to Decrease Port-A-Related Bloodstream Infections. Infect. Control J. 2015, 25, 53–61. [Google Scholar] [CrossRef]
- Chiu, L.S.; Lee, H.H.; Chang, H.C. Improving Solutions to Vascular Access Problems with Hemodialysis Patients through Multimedia Teaching Intervention. J. Taiwan Nephrol. Nurses Assoc. 2014, 13, 16–29. [Google Scholar]
- Yeh, L.H.; Lo, F.Y.; Li, W.J.; Kuo, T.L.; Tsai, J.L. Applying Therapeutic Play to Assist a Preschool Child with Leukemia to Reduce the Fear of Port-A Insertion. Chang. Gung. Nurs. 2015, 26, 526–538. [Google Scholar] [CrossRef]
- Lee, Y.C.; Lin, H.H.; Chuang, I.J.; Kuan, H.C.; Chi, C.C.; Lin, Y.C.; Dong, S.X.; Wu, M.J.; Ho, H.Y.; Wu, S.C.; et al. The Reduction of Central Line-Associated Bloodstream Infections in Oncology Wards in a Regional Teaching Hospital. Infect. Control J. 2016, 26, 1–12. [Google Scholar] [CrossRef]
- Bird, S. Risk Management: What Is It? Aust. Fam. Physician 2007, 36, 67–68. [Google Scholar]
- Joint Commission of Taiwan. Guidelines for the Postgraduate Two Years Medical Affairs Training Programs. Available online: https://www.jct.org.tw/cp-172-2800-6d65b-1.html (accessed on 1 January 2023).
- Mennonite Christian Hospital. Mennonite Christian Hospital Two-Year Post Graduate Training Program for Nurses. Available online: https://www.mch.org.tw/UserFiles/20151022042/20151022140706.pdf (accessed on 1 January 2023).
- Cardinal Tien Hospital. Guidelines for the Postgraduate Two Years Medical Affairs Training Programs. Available online: https://www.cth.org.tw/public/dept_aboutus/75/045698a3000258545d67b03c1366d763.pdf (accessed on 1 January 2023).
- Chia-Yi Christian Hospital. Training Program for New Medical Staff. Available online: https://www.cych.org.tw/ndsec/doc/%E6%95%99%E8%82%B2%E8%A8%93%E7%B7%B4/%E6%96%B0%E4%BA%BA%E8%81%B7%E8%A8%93%E8%A8%88%E5%8A%83%E6%9B%B8.pdf (accessed on 1 January 2023).
- Taiwan Nurses Association. Basic Oncology Nursing Training Course. Available online: http://www.onst.org.tw/active/side_info.asp?id=395 (accessed on 1 January 2023).
- Lai, C.M.; Huang, H.M.; Liaw, S.S.; Huang, W.W. A Study of User’s Acceptance on Three-Dimensional Virtual Reality Applied in Medical Education. Bull. Educ. Psychol. 2009, 40, 341–361. [Google Scholar] [CrossRef]
- Chang, S.Y. Problems That May Be Faced in the Application of Virtual Reality in the Field of Education. Taiwan Educ. Rev. Mon. 2018, 7, 120–125. [Google Scholar]
- Chen, F.Q.; Leng, Y.F.; Ge, J.F.; Wang, D.W.; Li, C.; Chen, B.; Sun, Z.L. Effectiveness of Virtual Reality in Nursing Education: Meta-Analysis. J. Med. Internet Res. 2020, 22, e18290. [Google Scholar] [CrossRef]
- Padilha, J.M.; Machado, P.P.; Ribeiro, A.; Ramos, J.; Costa, P. Clinical Virtual Simulation in Nursing Education: Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, e11529. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Chen, C.H. Wayfinding Experience in a Virtual Environment with 2D Wedge Design Supports. J. Des. 2015, 20, 63–77. [Google Scholar]
- Tsai, S.L.; Chai, S.K.; Hsieh, L.F.; Lin, S.; Taur, F.M.; Sung, W.H.; Doong, J.L. The Use of Virtual Reality Computer Simulation in Learning Port-A Cath Injection. Adv. Health Sci. Educ. Theory Pract. 2008, 13, 71–87. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.R.; Park, E.A. The Effectiveness of Learning to Use HMD-Based VR Technologies on Nursing Students: Chemoport Insertion Surgery. Int. J. Environ. Res. Public Health 2022, 19, 4823. [Google Scholar] [CrossRef]
- Patel, C. An Analysis of Jean Lave and Etienne Wenger’s: Situated Learning: Legitimate Peripheral Participation; CRC Press: New York, NY, USA, 2017. [Google Scholar]
- Endacott, R.; Scholes, J.; Buykx, P.; Cooper, S.; Kinsman, L.; McConnell-Henry, T. Final-Year Nursing Students’ Ability to Assess, Detect and Act on Clinical Cues of Deterioration in a Simulated Environment. J. Adv. Nurs. 2010, 66, 2722–2731. [Google Scholar] [CrossRef]
- Yung, H.I.; Lee, C.C. Problem-Based Learning on the Problem-Solving Ability and Self-Directed Learning of Undergraduate Students. J. Res. Educ. Sci. 2015, 60, 131–155. [Google Scholar]
- Ekstrand, C.; Jamal, A.; Nguyen, R.; Kudryk, A.; Mann, J.; Mendez, I. Immersive and Interactive Virtual Reality to Improve Learning and Retention of Neuroanatomy in Medical Students: A Randomized Controlled Study. CMAJ Open 2018, 6, E103–E109. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Koo Foundation Sun Yat-Sen Cancer Center. Subcutaneous Port—A Injection, Flushing and Blood Drawing Techniques; Koo Foundation Sun Yat-Sen Cancer Center: Taipei City, Taiwan, 2022. [Google Scholar]
- Martin, F.; Ertzberger, J. Here and Now Mobile Learning: An Experimental Study on the Use of Mobile Technology. Comput. Educ. 2013, 68, 76–85. [Google Scholar] [CrossRef]
- Li, S.Z. Guideline of Clinical Competence Assessment; Elsevier Taiwan Limited Liability Company: Taipei City, Taiwan, 2013. [Google Scholar]
- Taiwan Nurses Association. Teaching Plan Design Guidelines for Nurse Preceptors. Available online: https://www.twna.org.tw/WebUploadFiles/DocFiles/1698_1021211.pdf (accessed on 1 January 2023).
- Tsao, P.S. Examples of Applying the Revison of Bloom’s Taxonomy of Educational Objectives to Mathematics Assessment Items. SE 2012, 63, 38–65. [Google Scholar] [CrossRef]
- Yu, C.; Chen, L.Y.; Huang, C.K. Implementation of the Simulation Training during the Clerkship of Medical Training. J. Innov. Bus Manag. 2010, 1, 51–65. [Google Scholar] [CrossRef]
- Kuo, M.C.; Chang, P. A Total Design and Implementation of an Intelligent Mobile Chemotherapy Medication Administration. Stud. Health Technol. Inform. 2014, 201, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Fletcher-Watson, B.; Crompton, C.J.; Hutchison, M.; Lu, H. Strategies for Enhancing Success in Digital Tablet Use by Older Adults: A Pilot Study. Gerontechnology 2016, 15, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Maytin, M.; Daily, T.P.; Carillo, R.G. Virtual Reality Lead Extraction as a Method for Training New Physicians: A Pilot Study. Pacing. Clin. Electrophysiol. 2015, 38, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.J.; Farra, S.; Ulrich, D.L.; Hodgson, E.; Nicely, S.; Matcham, W. Learning and Retention Using Virtual Reality in a Decontamination Simulation. Nurs. Educ. Perspect. 2016, 37, 210–214. [Google Scholar] [CrossRef]
- Murre, J.M.J.; Dros, J. Replication and Analysis of Ebbinghaus’ Forgetting Curve. PLoS ONE 2015, 10, e0120644. [Google Scholar] [CrossRef]
- Jung, E.Y.; Park, D.K.; Lee, Y.H.; Jo, H.S.; Lim, Y.S.; Park, R.W. Evaluation of Practical Exercises Using an Intravenous Simulator Incorporating Virtual Reality and Haptics Device Technologies. Nurse Educ. Today 2012, 32, 458–463. [Google Scholar] [CrossRef]




| O1 | X | O2 | O3 | |
|---|---|---|---|---|
| Measure | Two Weeks before the Intervention | Within 1 Week after the Intervention | One Month after the Intervention | |
| Background information | √ | |||
| Knowledge of implanted Port-A catheter | √ | √ | √ | |
| DOPS evaluation of implanted Port-A catheter | √ | √ | √ | |
| Virtual reality teaching system learning attitude toward implanted Port-A catheter care | √ | |||
| Virtual reality teaching system satisfaction of implanted Port-A catheter care | √ |
| Item | Content |
|---|---|
| Theoretical framework | Situated learning theory |
| Duration | Around 1 h 10 min |
| Intervention | Implanted Port-A abnormality management, preventive care and Implanted Port-A catheter care simulated virtual reality operation instruction |
| Teaching strategies | 1. TMS digital course teaching 1.1 Port-A care course (30 min) 1.2 Port-A abnormality management course (35 min) 2. Implanted Port-A catheter care virtual reality operation instruction (5 min) |
| Number of participants | 43 |
| Learning objectives | 1. Can you really implement the Port-A catheter skill step and care procedure? 2. Distinguish the patient’s Port-A catheter care problems based on the patient’s signs and symptoms? 3. Select the correct clinical decision-making based on clinical Port-A catheter care problems? |
| Evaluation methods | Virtual reality teaching system knowledge scale for implanted Port-A catheter Evaluation form for implanted Port-A catheter DOPS Virtual reality teaching system for learning attitude scale for implanted Port-A catheter care Virtual reality teaching system satisfaction scale for implanted Port-A catheter care |
| Unit | Number of learners (n = 43) | Pre-test | Intervention | Post-test | Interview (n = 10) | Delayed post-test | |
| 1. Background information 2. Knowledge test 3. DOPS | Digital course | VR practice | 1. Knowledge test 2. Learning attitude 3. Satisfaction scale 4. DOPS | 1. Knowledge test 2. DOPS | |||
| Date | Date of course | VR date of intervention | Date | Date | Date | ||
| 5N | 8 | 6–10 Jan | 11–15 Jan | 15–19 Jan | 12–16 Mar | 19–23 Mar | 16–20 Apr |
| 5S | 6 | 22–26 Jan | |||||
| 6N | 13 | 29 Jan–2 Feb | |||||
| 4N | 2 | 05–09 Feb | |||||
| 6S | 3 | 19–23 Feb | |||||
| 4S | 7 | 26 Feb–02 Mar | |||||
| ICU | 4 | 05–09 Mar | |||||
| Total | 43 | 5 days | 5 days | 5 days, respectively | 5 days | 7 days | 5 days |
| Interview Guidelines |
|---|
|
| Variable | n (%) | Range | Mean (SD) |
|---|---|---|---|
| Female | 43 (100.0) | ||
| Age in years | 20–29 | 22.88 (1.68) | |
| Education | |||
| 5 year diploma | 3 (7.0) | ||
| 2 year college | 24 (55.8) | ||
| 4 year college | 7 (16.3) | ||
| University | 8 (18.6) | ||
| Master’s | 1 (2.3) | ||
| On-the-job training | |||
| No | 41 (95.3) | ||
| Yes | 2 (4.7) | ||
| Work experience in this hospital | 3–25 | 9.86 (6.27) | |
| Total nursing work experience | 3–43 | 12.19 (9.60) | |
| Nursing clinical ladder | |||
| Probation | 1 (2.3) | ||
| N1 | 39 (90.7) | ||
| N2 | 3 (7.0) | ||
| Source of information about VR system | |||
| None | 14 (32.6) | ||
| Yes (multiple choice) | 29 (67.4) | ||
| Newspaper | 8 (18.6) | ||
| Television | 20 (46.5) | ||
| Exhibition | 5 (11.6) | ||
| Others (supervisors, school, friends, and courses) | 5 (11.6) | ||
| VR experience | |||
| None | 30 (69.8) | ||
| Yes (multiple choice) | 13 (30.2) | ||
| Participated in related exhibition | 6 (14.0) | ||
| Place for learning | 1 (2.3) | ||
| Other (entertainment, exhibition, movie, PS4, and games) | 8 (18.6) |
| Frequency | Number of Nurses | Total Practice Time | Grand Mean of Hint Frequency | Grand Mean of Error Frequency |
|---|---|---|---|---|
| T1 | 43 | 0:12:20 | 1.23 | 7.37 |
| T2 | 43 | 0:09:52 | 0.79 | 6.40 |
| T3 | 43 | 0:08:32 | 0.28 | 3.98 |
| T4 | 40 | 0:07:36 | 0.10 | 2.85 |
| T5 | 35 | 0:07:07 | 0.18 | 1.68 |
| T6 | 15 | 0:06:46 | 0.27 | 1.60 |
| T7 | 8 | 0:06:55 | 0.25 | 1.50 |
| T8 | 6 | 0:06:59 | 0.00 | 0.83 |
| T9 | 4 | 0:07:04 | 0.00 | 0.75 |
| T10 | 3 | 0:06:44 | 0.00 | 0.67 |
| T11 | 2 | 0:06:27 | 0.00 | 0.50 |
| T12 | 1 | 0:05:49 | 0.00 | 1.00 |
| T13 | 1 | 0:05:41 | 0.00 | 0.00 |
| Disagree | Neutral | Agree | Mean | |||
|---|---|---|---|---|---|---|
| No | Item | n (%) | n (%) | n (%) | (SD) | Rank |
| 1 | The virtual reality teaching system provides clear instructions on how to operate the system. | 0 (0.0) | 3 (7.0) | 40 (93.0) | 4.35 (0.61) | |
| 2 | The virtual reality teaching system is presented in an easy-to-understand way. | 0 (0.0) | 6 (14.0) | 37 (86.0) | 4.35 (0.72) | |
| 3 | The length of the content in the virtual reality teaching system is appropriate. | 2 (4.7) | 5 (11.6) | 36 (83.7) | 4.19 (0.82) | Low 3 |
| 4 | The content of the virtual reality teaching system increases my interest in learning. | 0 (0.0) | 5 (11.6) | 38 (88.4) | 4.40 (0.70) | High 3 |
| 5 | The virtual reality teaching system provides accurate information. | 0 (0.0) | 3 (7.0) | 40 (93.0) | 4.42 (0.63) | High 2 |
| 6 | I can easily click on the content of the virtual reality teaching system. | 1 (2.3) | 3 (7.0) | 39 (90.7) | 4.23 (0.68) | |
| 7 | The virtual reality teaching system is a realistic and uncluttered scene that is easy to identify | 0 (0.0) | 2 (4.7) | 41 (95.3) | 4.49 (0.59) | High 1 |
| 8 | I can experience the virtual reality teaching system without constantly moving or changing my posture. | 0 (0.0) | 4 (9.3) | 39 (90.7) | 4.23 (0.61) | |
| 9 | The use and operation of the virtual reality teaching system is helpful to me. | 0 (0.0) | 4 (9.3) | 39 (90.7) | 4.26 (0.62) | |
| 10 | I enjoy learning with virtual reality (VR) devices. | 0 (0.0) | 9 (20.9) | 34 (79.1) | 4.14 (0.74) | Low 1 |
| 11 | I believe that this type of virtual reality (VR) learning is effective. | 0 (0.0) | 5 (11.6) | 38 (88.4) | 4.33 (0.68) | |
| 12 | In the future, I will be interested in learning using this method. | 0 (0.0) | 9 (20.9) | 34 (79.1) | 4.16 (0.75) | Low 2 |
| Grand mean of percent/mean (SD) | 0.58 | 11.24 | 88.18 | 4.29 (0.46) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, S.-F.; Hsu, L.-L.; Hsieh, S.-I. Effects of Digital Learning and Virtual Reality in Port-A Catheter Training Course for Oncology Nurses: A Mixed-Methods Study. Healthcare 2023, 11, 1017. https://doi.org/10.3390/healthcare11071017
Shih S-F, Hsu L-L, Hsieh S-I. Effects of Digital Learning and Virtual Reality in Port-A Catheter Training Course for Oncology Nurses: A Mixed-Methods Study. Healthcare. 2023; 11(7):1017. https://doi.org/10.3390/healthcare11071017
Chicago/Turabian StyleShih, Shu-Feng, Li-Ling Hsu, and Suh-Ing Hsieh. 2023. "Effects of Digital Learning and Virtual Reality in Port-A Catheter Training Course for Oncology Nurses: A Mixed-Methods Study" Healthcare 11, no. 7: 1017. https://doi.org/10.3390/healthcare11071017