
Collateral Victims of Defensive Medical Practice

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
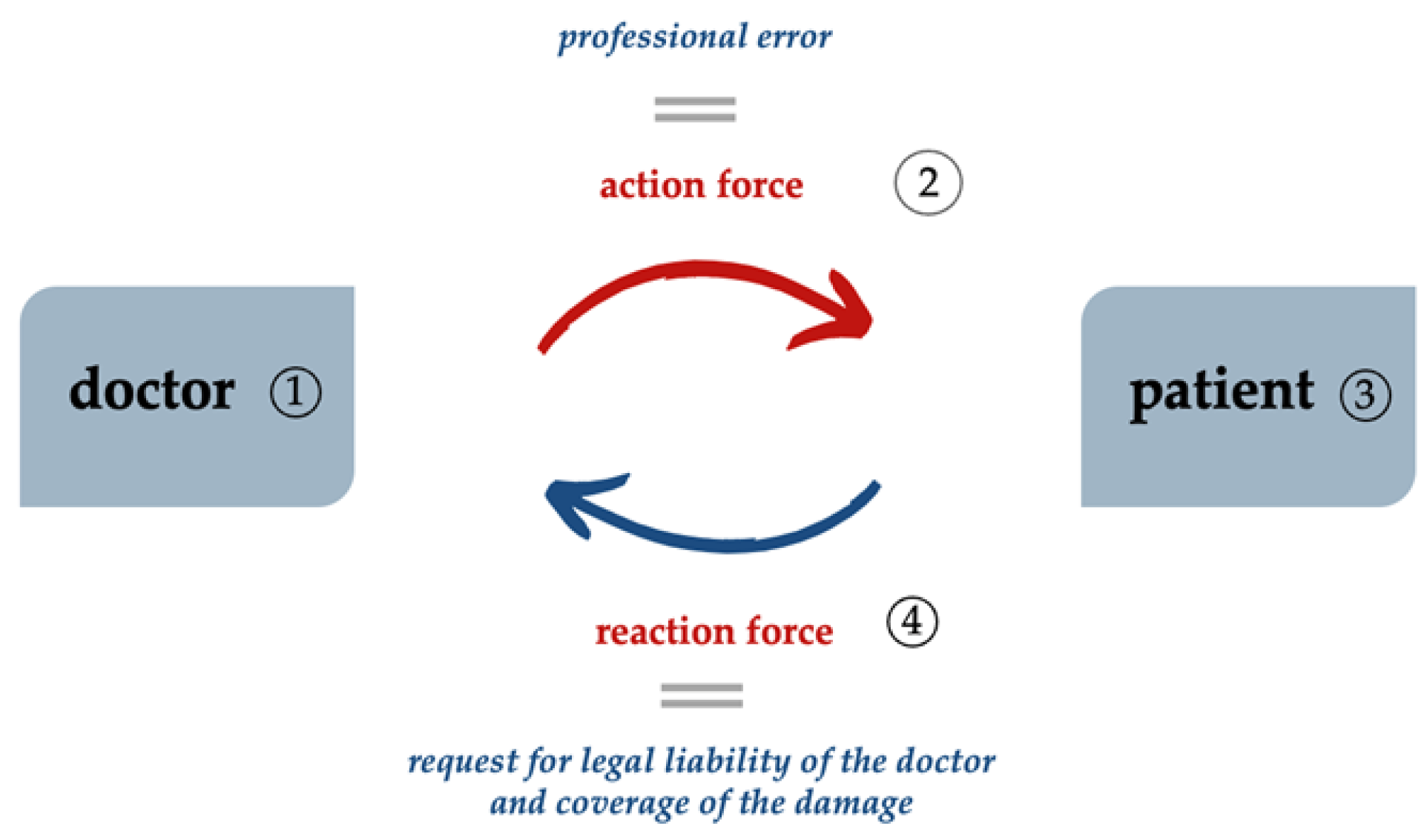
2.1. Malpractice in the Healthcare System Context
2.2. Defensive Medicine—History
- Do not perform any surgery, do not prescribe or administer medicines, do not touch the patient, do not perform any manipulation, and pray a lot, or
- Practice medicine defensively [34].
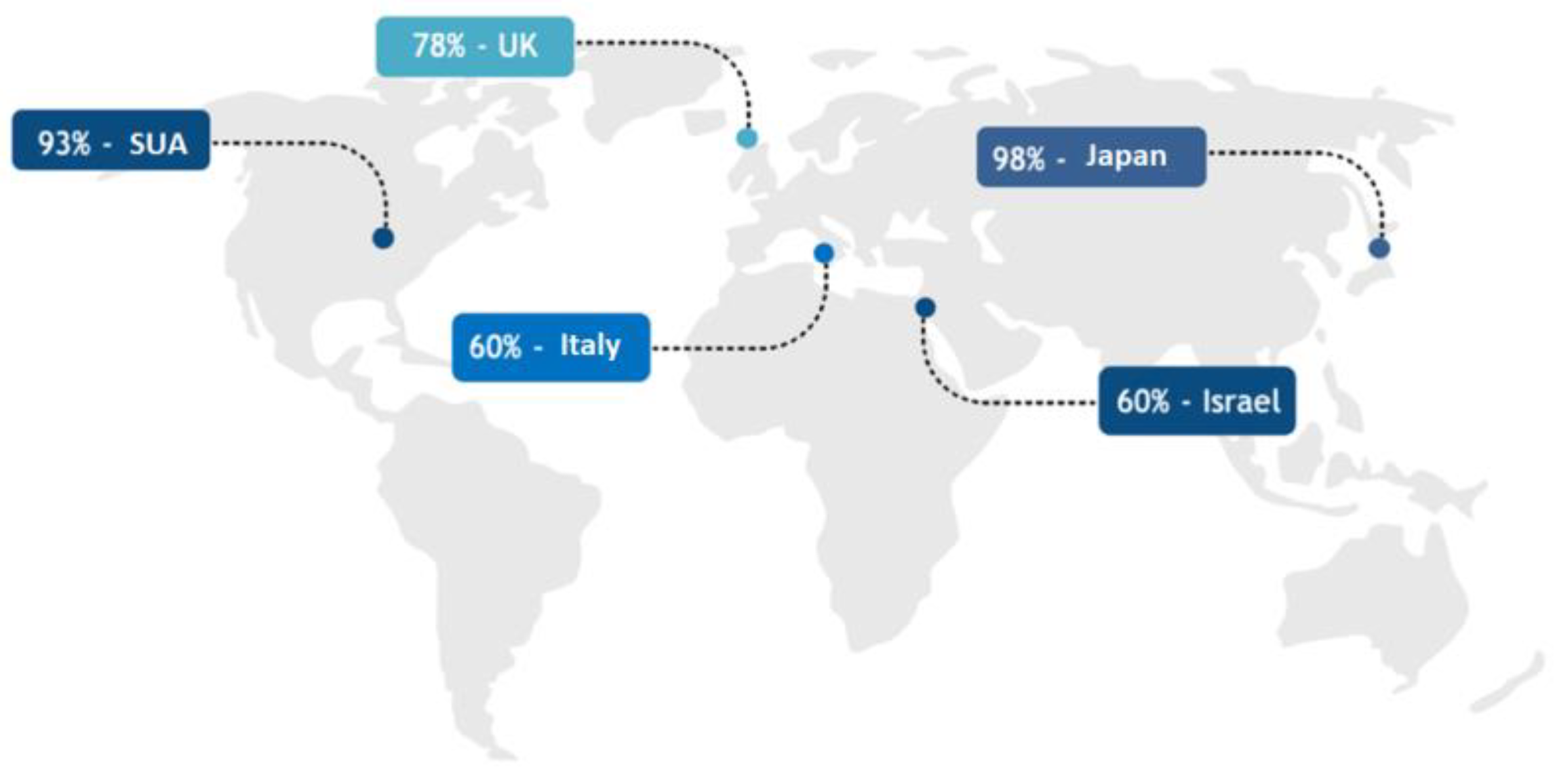
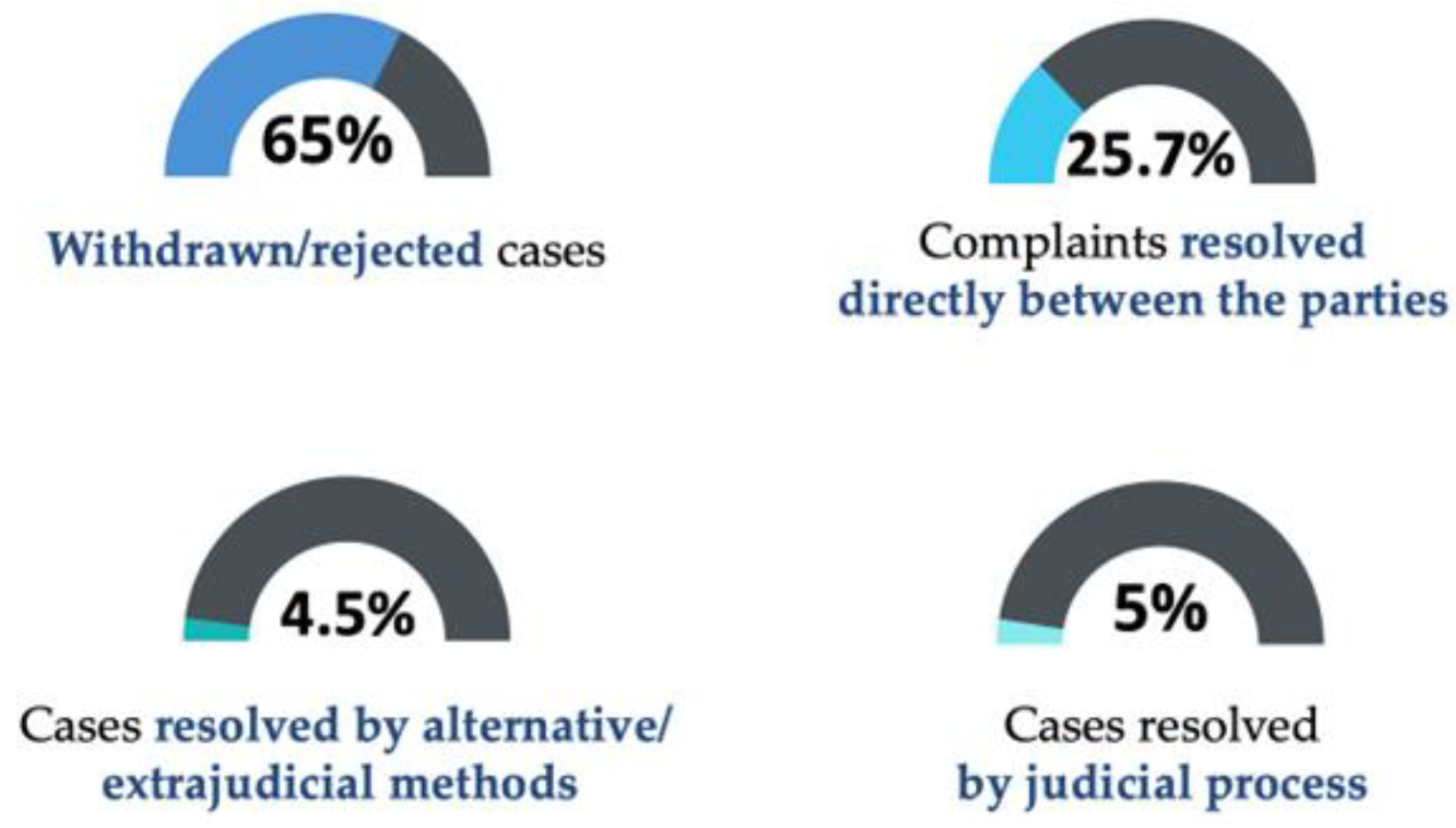
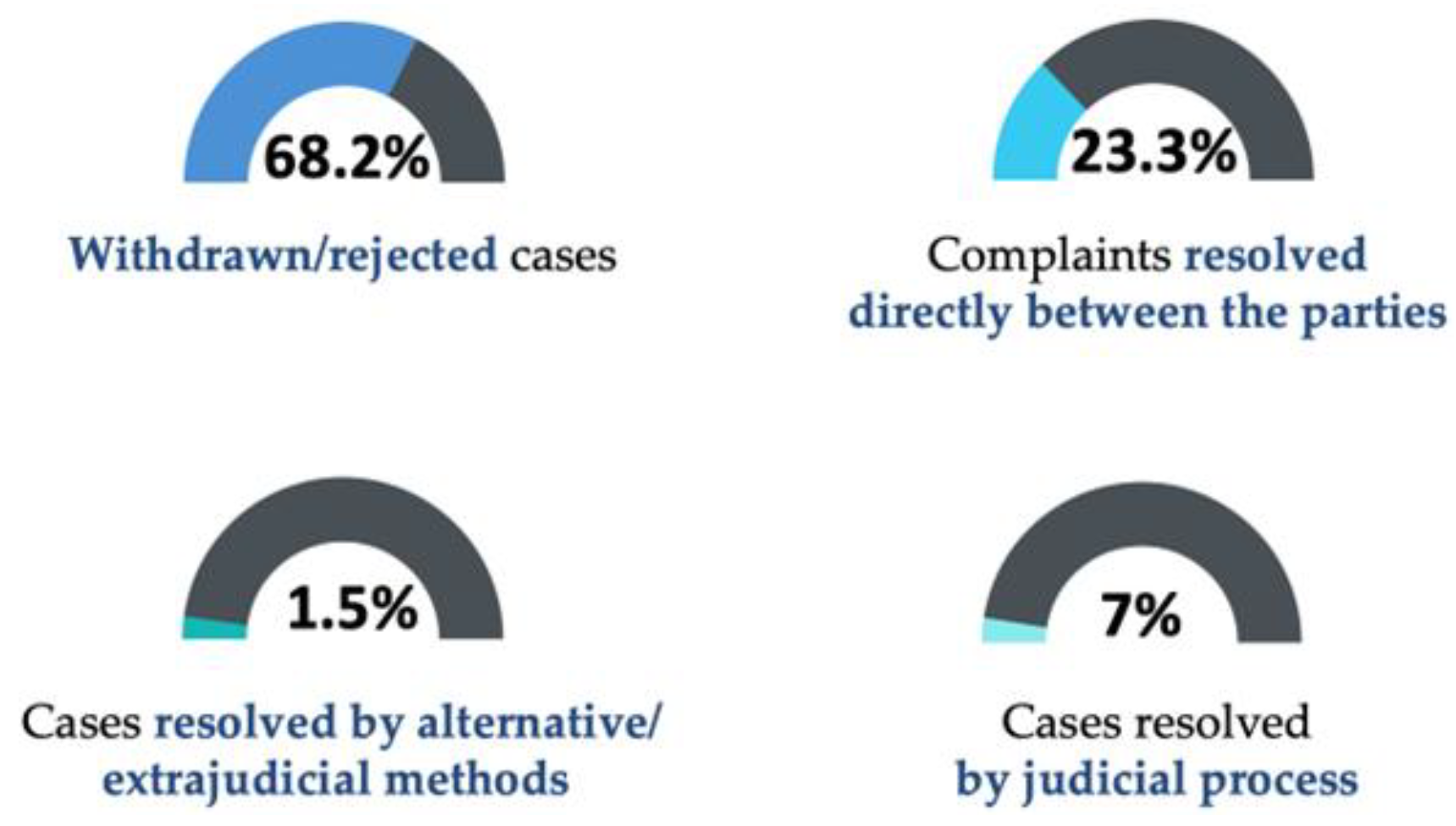
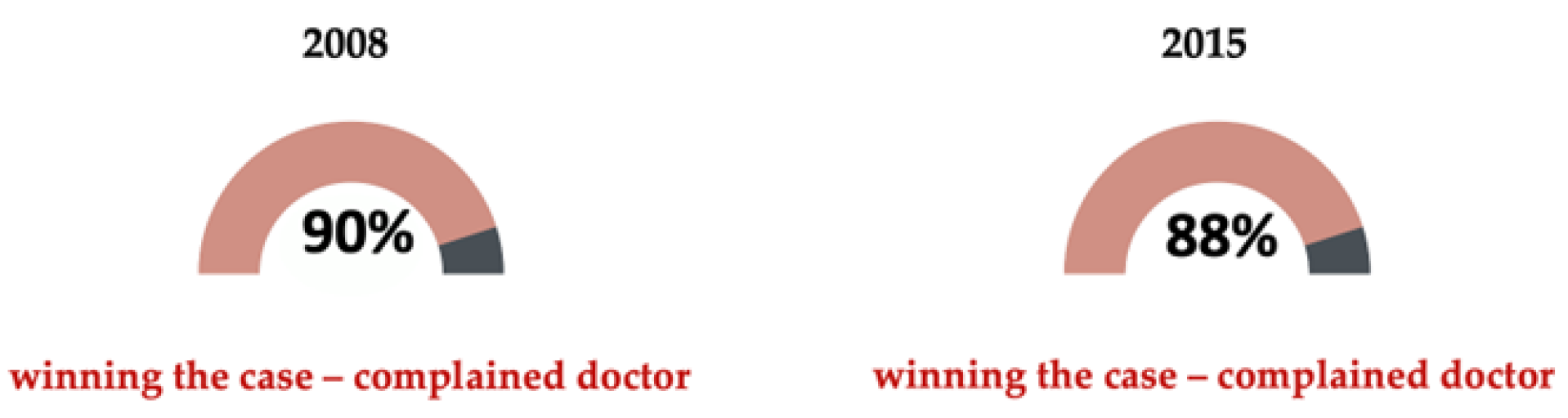
2.3. DMP Statistics
3. Results and Discussions
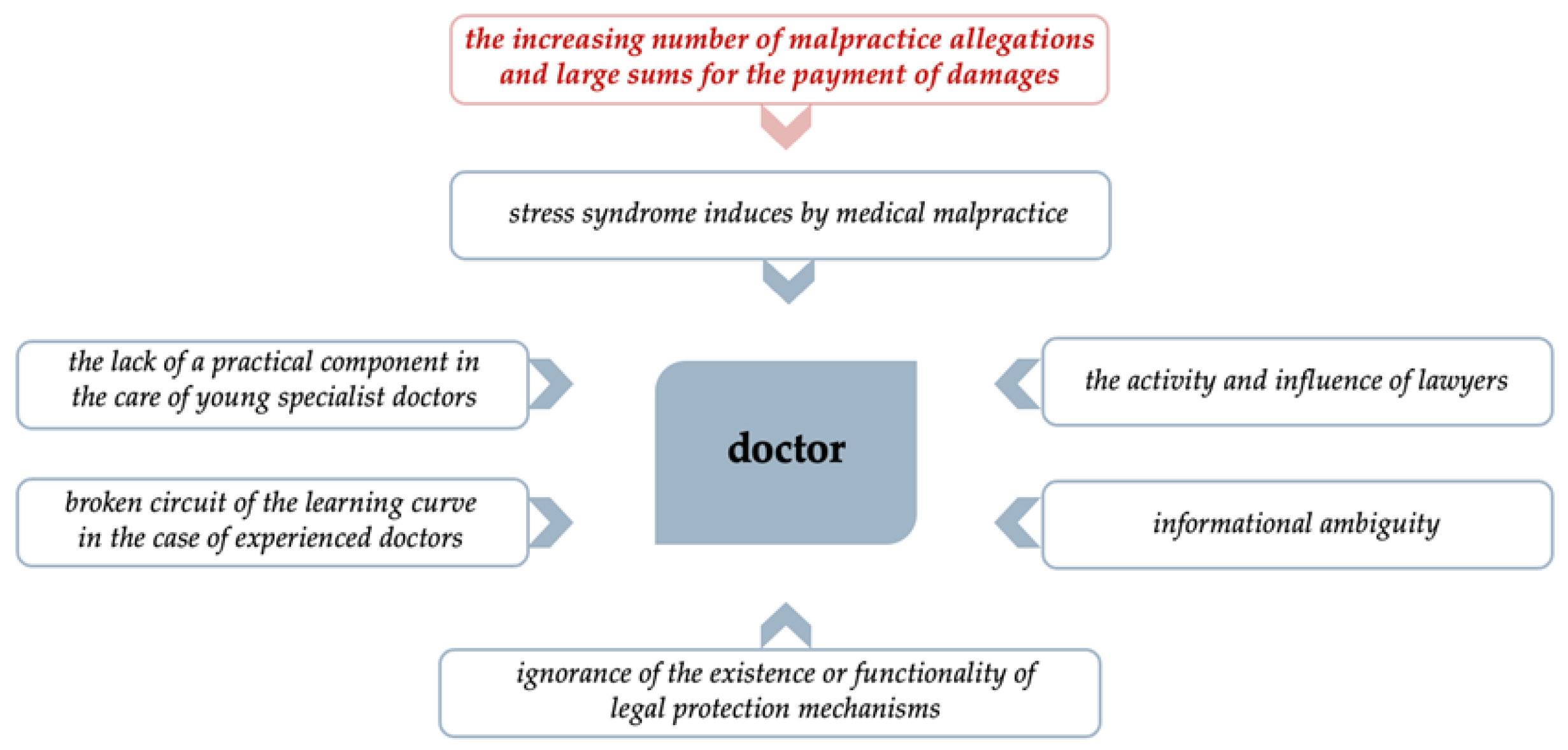
3.1. A Cascade of Factors Justifying DMP
- the lack of a practical component in the case of young specialist doctors—in accordance with the “learning curve” concept, young specialists are the quadrant characterized by “awareness of the competence” they have, as a result of the studies they have carried out and the testing and certification of their acquired knowledge. However, their lack of extensive practical experience may increase their need for extra caution, due to fear of possible error;
- the broken circuit of the learning curve in the case of experienced doctors—the era in which we live, learn, and work professionally is defined by continuous technological and informational progress, which “forces professionals”, through the complexity of the world, to be updated to present requirements in anticipation of the rigors expected in the near future. This circuit of the learning curve places highly experienced doctors in the category of “competency unaware”, which is characterized by a high level of automatism in the professional activity they carry out. The interruption of the learning curve is caused by reluctance to adapt to the new [4].
- ignorance of the existence or functionality of legal protection mechanisms—among legal protection mechanisms, we include informed patient consent, which provides protection for both doctors and patients, ensuring the implementation of doctors’ legal obligation to communicate and provide information and respecting the principle of patient autonomy. Another legal protection mechanism is professional civil liability insurance for medical malpractice, which provides a safety net for doctors by covering damages caused by medical errors, as well as a safety net for patients by ensuring recovery for the damage caused.
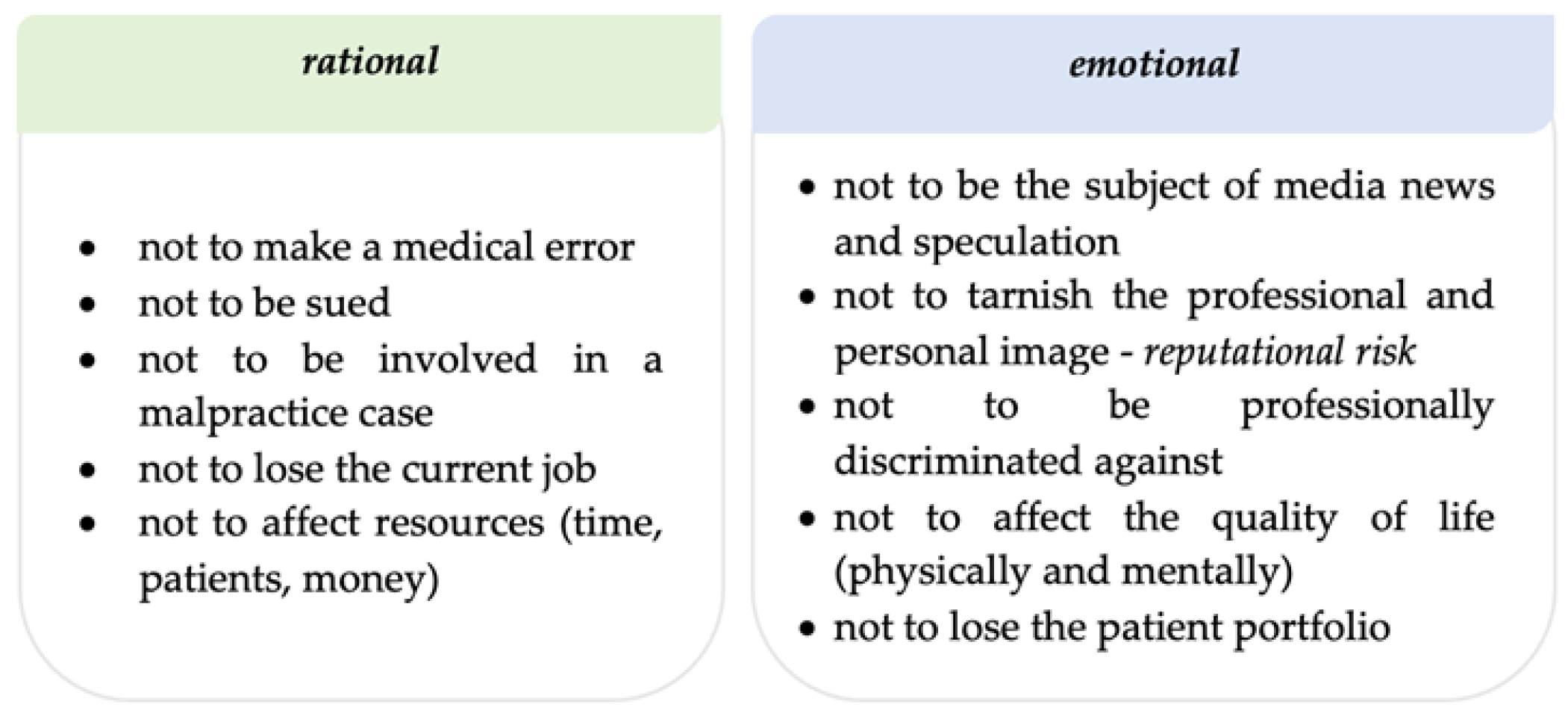
- informational ambiguity—the medical profession needs to build and maintain a good reputation. The press, through its existing means of communication, can significantly affect professional reputations. For this reason, doctors practice defensively to avoid negative publicity, staying in a reputational safety zone. The media can also have a very important impact on patients by increasing their tendency to see themselves as victims of medical malpractice and by presenting the most extreme cases in newspapers and on TV [47]. Thus, in the absence of specialized medical knowledge, patients can be easily influenced by articles without scientific and statistical data pertaining to correct medical practice, and be stimulated to blame medical staff unjustifiably.
- the activity and influence of lawyers—legal professionals can significantly affect the normal course of medical activity, first by supporting proceedings before courts to prove the guilt of a doctor, and second by promoting patients’ sense of victimization and their belief in the success of cases in court. In addition, an important element is the growing number of lawyers who expand their practices to areas with high economic potential based on the importance of protected values.

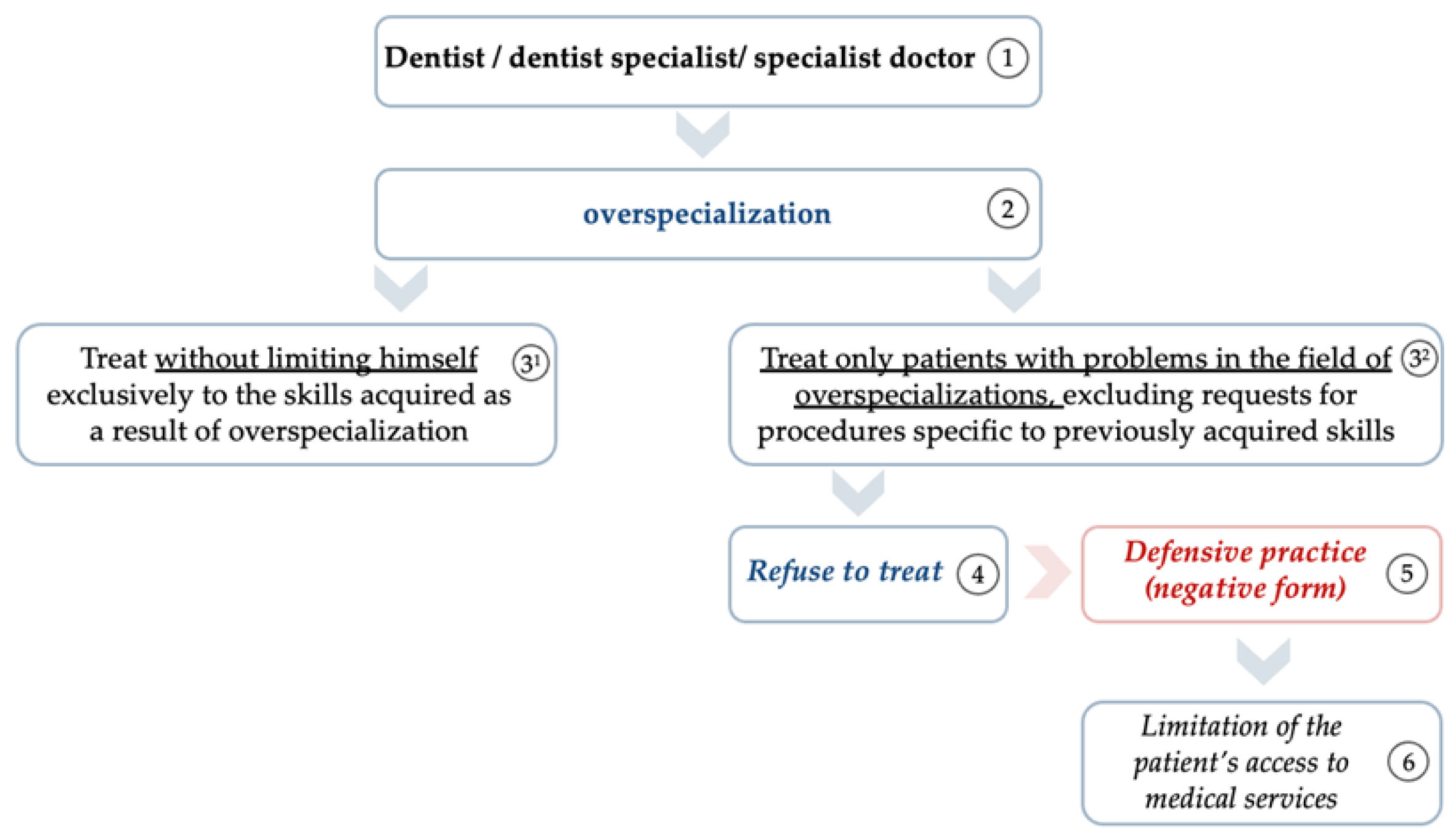
3.2. Overspecialization—A Possible Form of DMP
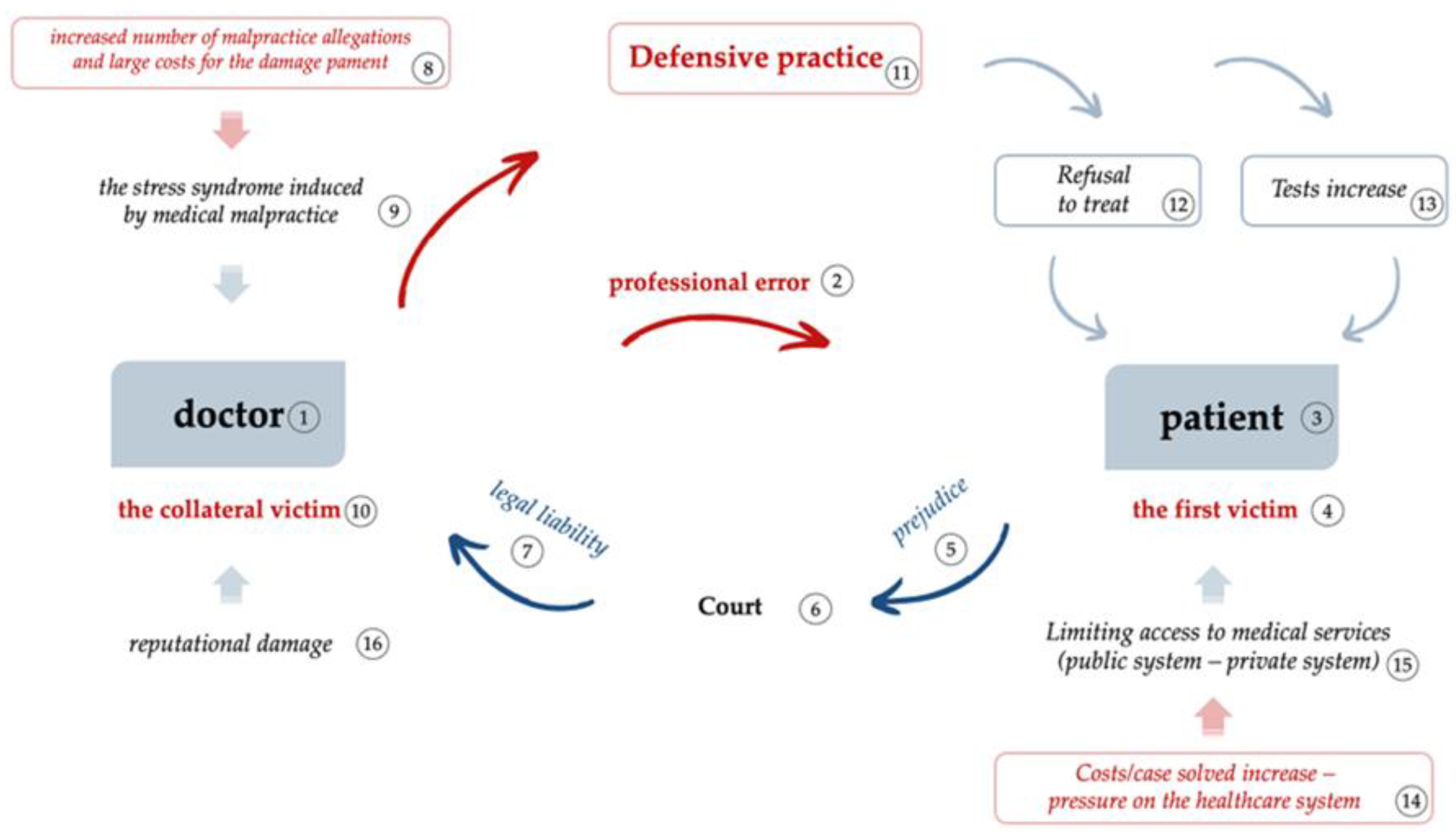
3.3. The Consequences of DMP
- ▪
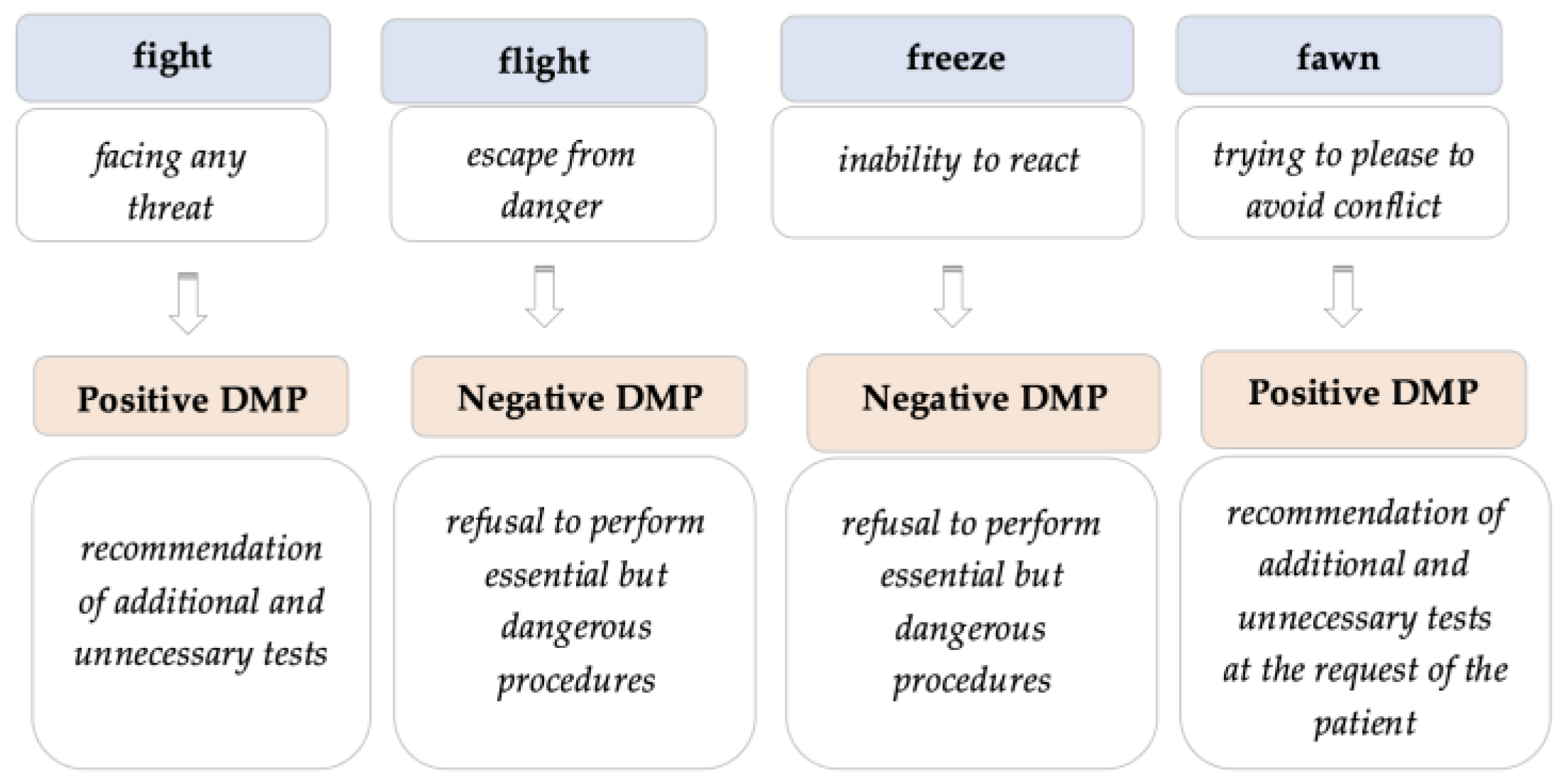
- Limiting the patient’s access to medical services by the doctor’s refusal to perform essential but dangerous procedures—practicing negative defensive medicine.
- ▪
- Being dominated by feelings of distrust and insecurity about medical decisions due to the doctor’s actions in recommending additional and unnecessary tests (positive defensive practice). Thus, the costs of carrying out treatment increase significantly, thereby increasing the risk of abandoning a proposed treatment and leading to possible degradation of the patient’s health and requiring greater financial resources in the future for the patient’s recovery.
- ▪
- The continuous increase in fear of malpractice allegations generates the doctor’s instability and insecurity, which influences and diminishes the doctor’s reputational safety. Doctors can cover payments for damages caused by a medical error by purchasing a professional liability insurance policy, but such a document tht does not have the capacity to ensure the doctor against the psychological costs and the stress caused by involvement in litigation or the reputational effects of a lawsuit (reduced income, damaged status) [26].
- ▪
- Decreasing the efficiency of the medical actions performed by the doctor through positive defensive practice, in terms of increasing the complexity of medical interventions.
- ▪
- Degradation of the doctor’s relationship with the patient by increasing the time needed to identify and resolve the patient’s needs, requiring additional specialist investigations and consultations.
- ▪
- Increasing pressure on the system due to its inability to ensure the correct management of the relationship between the doctor and the patient.
- ▪
- The continued increase in costs of resolving medical cases as a result of the need to protect the doctor by requesting additional specialist investigations and consultations. The impact that defensive medicine has in terms of increased costs has been analyzed in the specialized literature—US 12 billion 1987 and a doubling of these costs in 1997 [48]. In 2008, a Harvard University study showed estimated costs of US 45.6 billion associated with defensive medicine [26].
- ▪
- Decreased patient access to medical services as a result of increased costs. From the perspective of financing health services via funds allocated from national budgets, defensive practices treat a smaller number of patients with the same financial resource. In private healthcare systems, in which the patients contribute from their own income to pay for necessary treatment, fewer and fewer patients will be able to afford certain treatments as a result of the continuous increase in costs. The increase in the costs of resolving medical cases as a result of the unjustified use of health services leads to the blocking of human resources by involving a larger number of medical personnel and the rapid consumption of allocated financial resource. These two elements, which are commonly found due to defensive medical practice, limit the access to medical services by patients who have a great need for medical assistance [12].
3.4. Solutions to Diminish the DMP
- ▪
- the role of the doctor to treat the patient is fulfilled by the doctor’s mission to contribute to the correct education of the patient by promoting a positive attitude regarding prevention and an approach to a healthy lifestyle, ensuring continuous information that enables the patient to be aware of the characteristics and components of appropriate medical care as a complex medical process [49,50].
- ▪
- realizing the connection between education and treatment, the doctor will have the ability to build a correct relationship with the patient, based on trust in the doctor’s professional skills [50].
- ▪
- in order to reduce any conflictual tendency of a patient, there must be certainty regarding damage recovery following an act of malpractice, with an understanding by the patient of the legal mechanisms that cover the damage caused, including professional civil liability insurance.
- ▪
- the need to amplify the doctor’s role in the process of educating patients, starting from the youngest ages.
- ▪
- reducing the reputational risk by developing and increasing the doctor’s reputational mentality. The increase in reputational safety can be achieved by training the doctor’s critical thinking, which represents the fusion of the doctor’s optimism in continuing to practice and the ability to analyze the pitfalls, in terms of being aware of the certainty and the extent of risks that influence the doctor’s activities (as most malpractice cases absolve the doctors of liability).
- ▪
- transforming the negative approach into a need to be aware of the circumstances in which an error occurred, analyzed from the perspective of the learning opportunity [5].
- ▪
- the need for clarity and vision regarding the complexity of professional activity. This can be achieved by ensuring a perpetual circuit of the learning curve [3,4], which would allow the periodic adaptation of the professional in response to new demands of the profession. Doctors need to understand and interpret legislative norms, acquire of soft skills (communication, emotional intelligence, time management, etc.), master digitization, understand cost-efficiency-based management, etc. It is recommended that the defensive, self-protective behavior be replaced with continuous learning [2,3], regardless of the speciality and the accumulated work experience, supplementing such learning with an important component of interpersonal empathy, which would increase the safety of patients [48].
- ▪
- the redistribution of “legislative attention” from the severity of punishment for professional error to the satisfaction of the injured patient, relying on the replacement of the punitive attitude with a need to identify and correct the errors [51], specifically within the no-fault system.
- ▪
- Exchanging legislative and informational uncertainty for clarity and understanding of the system level’s steps taken, in terms of orienting the social mentality toward eliminating the concept of blaming someone who made a mistake [52] and supporting that person in order to report the error immediately.
- ▪
- A possible solution to the treatment of defensive practice is the use of artificial intelligence as a second opinion tool, functioning as an element of social proof based on statistics, thereby diminishing the reputational competition of doctors as medical services providers. Artificial intelligence, from the perspective of providing a second opinion, would provide an ally for doctors in terms of the correctness of diagnoses and proposed treatment options based on information and statistical data, thus reducing the tendency of doctors to practice defensively by adding tests or refusing patients.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bester, J.C. Defensive practice is indefensible: How defensive medicine runs counter to the ethical and professional obligations of clinicians. Med. Health Care Philos. 2020, 23, 413–420. [Google Scholar] [CrossRef]
- Delgado Bolton, R.C.; San-Martín, M.; Vivanco, L. Role of Empathy and Lifelong Learning Abilities in Physicians and Nurses Who Work in Direct Contact with Patients in Adverse Working Conditions. Int. J. Environ. Res. Public Health 2022, 19, 3012. [Google Scholar] [CrossRef] [PubMed]
- Babenko, O.; Koppula, S.; Daniels, L.; Nadon, L.; Daniels, V. Lifelong learning along the education and career continuum: Meta-analysis of studies in health professions. J. Adv. Med. Educ. Prof. 2017, 5, 157–163. [Google Scholar]
- Howard, N.M.; Cook, D.A.; Hatala, R.; Pusic, M.V. Learning Curves in Health Professions Education Simulation Research: A Systematic Review. Simul. Healthc. 2021, 16, 128–135. [Google Scholar] [CrossRef]
- Shepherd, L.; LaDonna, K.A.; Cristancho, S.M.; Chahine, S. How Medical Error Shapes Physicians’ Perceptions of Learning: An Exploratory Study. Acad. Med. 2019, 94, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Bari, A.; Khan, R.A.; Rathore, A.W. Medical errors; causes, consequences, emotional response and resulting behavioral change. Pak. J. Med. Sci. 2016, 32, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Ortashi, O.; Virdee, J.; Hassan, R.; Mutrynowski, T.; Abu-Zidan, F. The practice of defensive medicine among hospital doctors in the United Kingdom. BMC Med. Ethics 2019, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Lyu, H.; Xu, T.; Brotman, D.; Mayer-Blackwell, B.; Cooper, M.; Daniel, M.; Wick, E.C.; Saini, V.; Brownlee, S.; Makary, M.A. Overtreatment in the United States. PLoS ONE 2017, 12, e0181970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, M.K.; Hvidt, E.A.; Pedersen, K.M.; Lykkegaard, J.; Waldorff, F.B.; Munck, A.P.; Pedersen, L.B. Defensive medicine in Danish general practice. Types of defensive actions and reasons for practicing defensively. Scand. J. Prim. Health Care 2021, 39, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Pellino, I.M.; Pellino, G. Consequences of defensive medicine, second victims, and clinical-judicial syndrome on surgeons’ medical practice and on health service. Updates Surg. 2015, 67, 331–337. [Google Scholar] [CrossRef]
- Hvidt, E.A.; Lykkegaard, J.; Pedersen, L.B.; Pedersen, K.M.; Munck, A.; Andersen, M.K. How is defensive medicine understood and experienced in a primary care setting? A qualitative focus group study among Danish general practitioners. BMJ Open 2017, 7, e019851. [Google Scholar] [CrossRef] [Green Version]
- Adwok, J.; Kearns, E.H. Defensive medicine: Effect on cost, quality and access to healthcare. J. Biol. Agric. Healthc. 2013, 3, 29–35. [Google Scholar]
- Universal Declaration of Human Rights. Available online: https://www.un.org/sites/un2.un.org/files/2021/03/udhr.pdf (accessed on 21 January 2023).
- Law 95/2006 on health reform, Romania. Available online: https://legislatie.just.ro/Public/DetaliiDocument/71139 (accessed on 13 January 2023).
- Law nr. 46/2003 patients right, Romania. Available online: https://legislatie.just.ro/Public/DetaliiDocument/41483 (accessed on 13 January 2023).
- Romanian Civil Code. Available online: https://legislatie.just.ro/Public/DetaliiDocument/255190 (accessed on 19 December 2022).
- Ferrara, S.D.; Boscolo-Berto, R.; Viel, G. Malpractice and Medical Liability: European State of the Art and Guidelines; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar] [CrossRef] [Green Version]
- Vandersteegen, T.; Marneffe, W.; Cleemput, I.; Vereeck, L. The impact of no-fault compensation on health care expenditures: An empirical study of OECD countries. Health Policy 2015, 119, 367–374. [Google Scholar] [CrossRef] [Green Version]
- “NHS Resolution Claims Covering the Period 2006/07 to 2021/22,” 26 October 2022. Available online: https://resolution.nhs.uk/resources/annual-report-statistics/ (accessed on 22 January 2023).
- Leflar, R.B. The Regulation of Medical Malpractice in Japan. Clin. Orthop. Relat. Res. 2008, 467, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berlin, L. Medical errors, malpractice, and defensive medicine: An ill-fated triad. Diagnosis 2017, 4, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Guardado, J.R.; Policy Research Perspectives. Medical Professional Liability Insurance Indemnity Payments, Expenses and Claim Disposition, 2006–2015. Available online: https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/government/advocacy/policy-research-perspective-liability-insurance-claim.pdf (accessed on 12 November 2022).
- Wiley, M.; Lotterer, P. National Practitioner Data Bank, Medical Malpractice Payment Reports 9 April 2019. Available online: https://www.npdb.hrsa.gov/community_n_education/2019presentations/MedicalMalpracticePaymentReportsEdForum.pdf (accessed on 24 January 2023).
- Pallocci, M.; Treglia, M.; Passalacqua, P.; Tittarelli, R.; Zanovello, C.; De Luca, L.; Caparrelli, V.; De Luna, V.; Cisterna, A.M.; Quintavalle, G.; et al. Informed Consent: Legal Obligation or Cornerstone of the Care Relationship? Int. J. Environ. Res. Public Health 2023, 20, 2118. [Google Scholar] [CrossRef] [PubMed]
- Treglia, M.; Pallocci, M.; Passalacqua, P.; Giammatteo, J.; De Luca, L.; Mauriello, S.; Cisterna, A.M.; Marsella, L.T. Medical Liability: Review of a Whole Year of Judgments of the Civil Court of Rome. Int. J. Environ. Res. Public Health 2021, 18, 6019. [Google Scholar] [CrossRef] [PubMed]
- Mello, M.M.; Chandra, A.; Gawande, A.A.; Studdert, D.M. National costs of the medical liability system. Health Aff. 2010, 29, 1569–1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, S.D. Medical malpractice and legal medicine. Int. J. Leg. Med. 2013, 127, 541–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Gregorio, V.; Ferriero, A.M.; Specchia, M.L.; Capizzi, S.; Damiani, G.; Ricciardi, W. Defensive medicine in Europe: Which solutions? Vincenzo Di Gregorio. Eur. J. Public Health 2015, 25, ckv171043. [Google Scholar] [CrossRef] [Green Version]
- Johansson, H. The Swedish system for compensation of patient injuries. Upsala J. Med. Sci. 2010, 115, 88–90. [Google Scholar] [CrossRef]
- Geneviève Helleringer, Medical Malpractice and Compensation in France, Part II: Compensation Based on National Solidarity, 86 Chi.-Kent L. Rev. 1125. 2011. Available online: https://scholarship.kentlaw.iit.edu/cklawreview/vol86/iss3/6 (accessed on 12 November 2022).
- Watson, K.; Kottenhagen, R. Patients’ Rights, Medical Error and Harmonisation of Compensation Mechanisms in Europe. Eur. J. Health Law 2018, 25, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Office National d’Indemnisation des Accidents Médicaux (Oniam), “Rapport d’activité 2021”. 2021. Available online: https://www.oniam.fr/indemnisation-accidents-medicaux/rapport-d-activite (accessed on 25 January 2023).
- Garattini, L.; Padula, A. Defensive medicine in Europe: A ‘full circle’? Eur. J. Health Econ. 2020, 21, 477–482. [Google Scholar] [CrossRef] [Green Version]
- Bergen, R. Protection against Malpractice Litigation. Arch. Otolaryngol.-Head Neck Surg. 1975, 101, 182–184. [Google Scholar] [CrossRef] [PubMed]
- Reuveni, I.; Pelov, I.; Reuveni, H. Cross-sectional survey on defensive practices and defensive behaviours among Israeli psychiatrists. BMJ Open 2017, 7, e014153. [Google Scholar] [CrossRef] [PubMed]
- Studdert, D.M.; Mello, M.M.; Sage, W.M.; DesRoches, C.M.; Peugh, J.; Zapert, K.; Brennan, T.A. Defensive medicine among high-risk specialist physicians in a volatile malpractice environment. JAMA 2005, 293, 2609–2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sethi, M.K.; Obremskey, W.T.; Natividad, H.; Mir, H.R.; Jahangir, A.A. Incidence and costs of defensive medicine among orthopedic surgeons in the United States: A national survey study. Am. J. Orthop. 2012, 41, 69–73. [Google Scholar]
- Asher, E.; Greenberg-Dotan, S.; Halevy, J.; Glick, S.; Reuveni, H. Defensive medicine in Israel—A nationwide survey. PLoS ONE 2012, 7, e42613. [Google Scholar] [CrossRef] [Green Version]
- “Agenzia Nazionale per i Servizi Sanitari Regionali,” 2014. Available online: http://www.agenas.it/images/agenas/In%20primo%20piano/medicina difensiva/risultati ricerca medicina difensiva.pdf (accessed on 23 May 2022).
- Hiyama, T.; Yoshihara, M.; Tanaka, S.; Urabe, Y.; Ikegami, Y.; Fukuhara, T.; Chayama, K. Defensive medicine practices among gastroenterologists in Japan. World J. Gastroenterol. 2006, 12, 7671–7675. [Google Scholar] [CrossRef]
- Hurtado, H.E.; Gutiérrez, Z.H.; Iraola, N.; Rodríguez, A. Judicial Clinical Syndrome. Rev. Asoc. Med. Argent. 2006, 119, 8–16. [Google Scholar]
- Paterick, Z.R.; Patel, N.; Chandrasekaran, K.; Tajik, J.; Paterick, T.E. Medical Malpractice Stress Syndrome: A “Forme Fruste” of Posttraumatic Stress Disorder. J. Med. Pract. Manag. 2017, 32, 283–287. [Google Scholar]
- Quick, J.C.; Spielberger, C.D. Walter Bradford Cannon: Pioneer of stress research. Int. J. Stress Manag. 1994, 1, 141–143. [Google Scholar] [CrossRef]
- Mia Belle Frothingham Fight, Flight, Freeze, or Fawn: What This Response Means. Published 6 October 2021. Available online: https://www.simplypsychology.org/fight-flight-freeze-fawn.html (accessed on 23 January 2023).
- Kane, C.K. Policy Research Perspectives Medical Liability Claim Frequency: A 2007–2008 Snapshot of Physicians. Available online: https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/health-policy/prp-201001-claim-freq.pdf (accessed on 13 November 2022).
- Available online: https://ro.wikipedia.org/wiki/Principiul_Pareto (accessed on 22 October 2022).
- Toraldo, D.M.; Vergari, U.; Toraldo, M. Medical malpractice, defensive medicine and role of the “media” in Italy. Multidiscip. Respir. Med. 2015, 10, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osti, M.; Steyrer, J. A perspective on the health care expenditures for defensive medicine. Eur. J. Health Econ. 2017, 18, 399–404. [Google Scholar] [CrossRef] [Green Version]
- Thompson, M.S.; King, C.P. Physician perceptions of medical malpractice and defensive medicine. Eval. Program Plan. 1984, 7, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Lester, G.W.; Smith, S.G. Listening and talking to patients. A remedy for malpractice suits? West. J. Med. 1993, 158, 268–272. [Google Scholar]
- Vento, S.; Cainelli, F.; Vallone, A. Defensive medicine: It is time to finally slow down an epidemic. World J. Clin. Cases 2018, 6, 406–409. [Google Scholar] [CrossRef]
- Rodziewicz, T.L.; Houseman, B.; Hipskind, J.E. Medical Error Reduction and Prevention; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fault System | No-Fault System |
|---|---|
| System applied in most countries of the world (the United States of America, member states of the European Union, Romania). | System implemented in the Scandinavian countries, in Sweden since 1975, in France since 2002 (mixed system). |
| System focused on the search for the mistake and proof. | It is not necessary to prove the error in order for the injured party to receive compensation. |
| System focused on the causal links among act—damage—guilt. | System focused on the direct satisfaction of the injured patient. |
| Conflict character prevails, specific to a judicial procedure. | Settlement through extrajudicial administrative procedures. |
| High procedural costs. | Low procedural costs. |
| Long settlement terms. | Fast resolution. |
| Publicity for malpractice cases. | Increased confidentiality for malpractice cases. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cernega, A.; Meleșcanu Imre, M.; Ripszky Totan, A.; Arsene, A.L.; Dimitriu, B.; Radoi, D.; Ilie, M.-I.; Pițuru, S.-M. Collateral Victims of Defensive Medical Practice. Healthcare 2023, 11, 1007. https://doi.org/10.3390/healthcare11071007
Cernega A, Meleșcanu Imre M, Ripszky Totan A, Arsene AL, Dimitriu B, Radoi D, Ilie M-I, Pițuru S-M. Collateral Victims of Defensive Medical Practice. Healthcare. 2023; 11(7):1007. https://doi.org/10.3390/healthcare11071007
Chicago/Turabian StyleCernega, Ana, Marina Meleșcanu Imre, Alexandra Ripszky Totan, Andreea Letiția Arsene, Bogdan Dimitriu, Delia Radoi, Marina-Ionela Ilie, and Silviu-Mirel Pițuru. 2023. "Collateral Victims of Defensive Medical Practice" Healthcare 11, no. 7: 1007. https://doi.org/10.3390/healthcare11071007