
Factors Influencing the Use of Walking Aids by Frail Elderly People in Senior Day Care Centers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
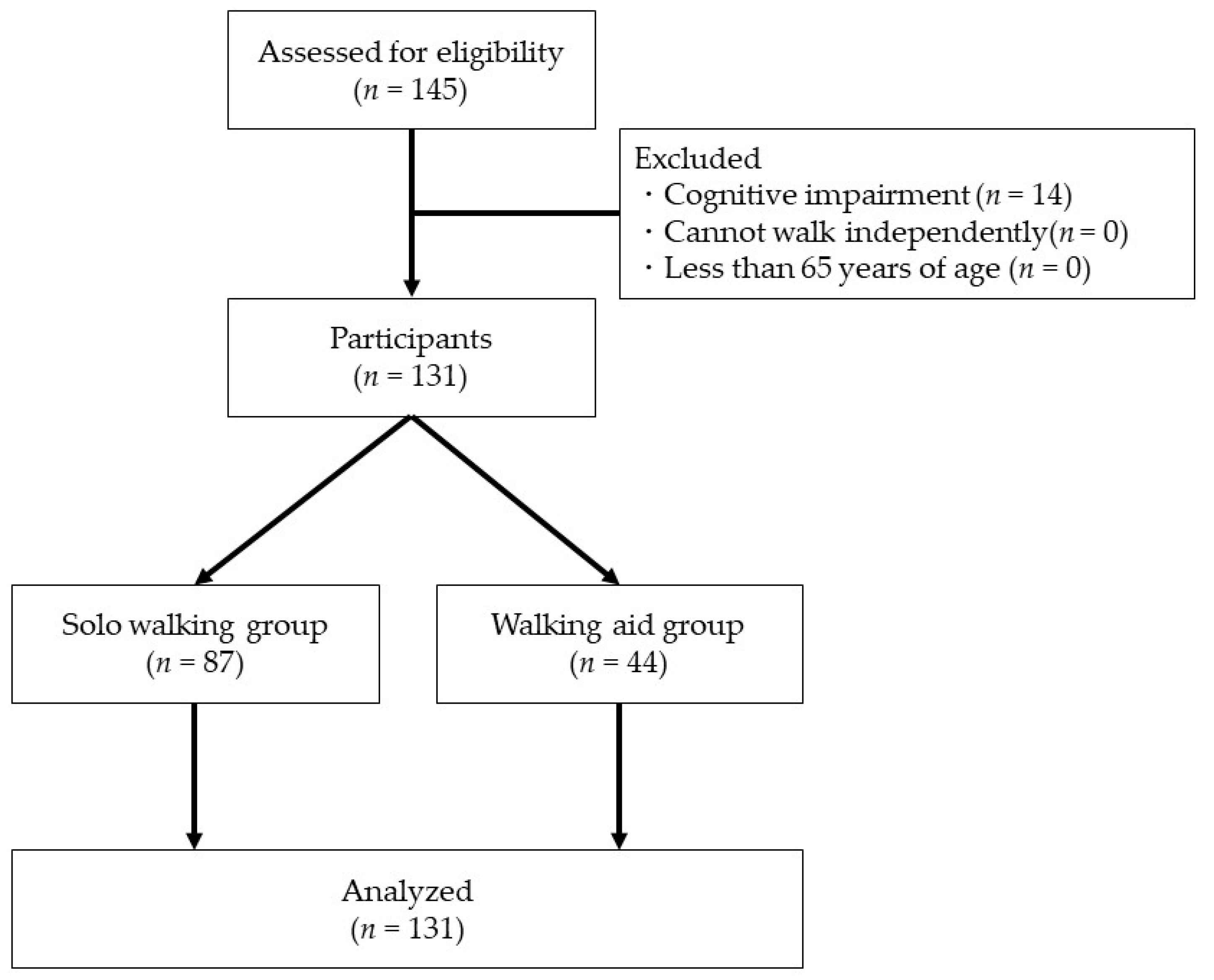
2.2. Study Participants
2.3. Measurements
2.4. Statistical Analysis
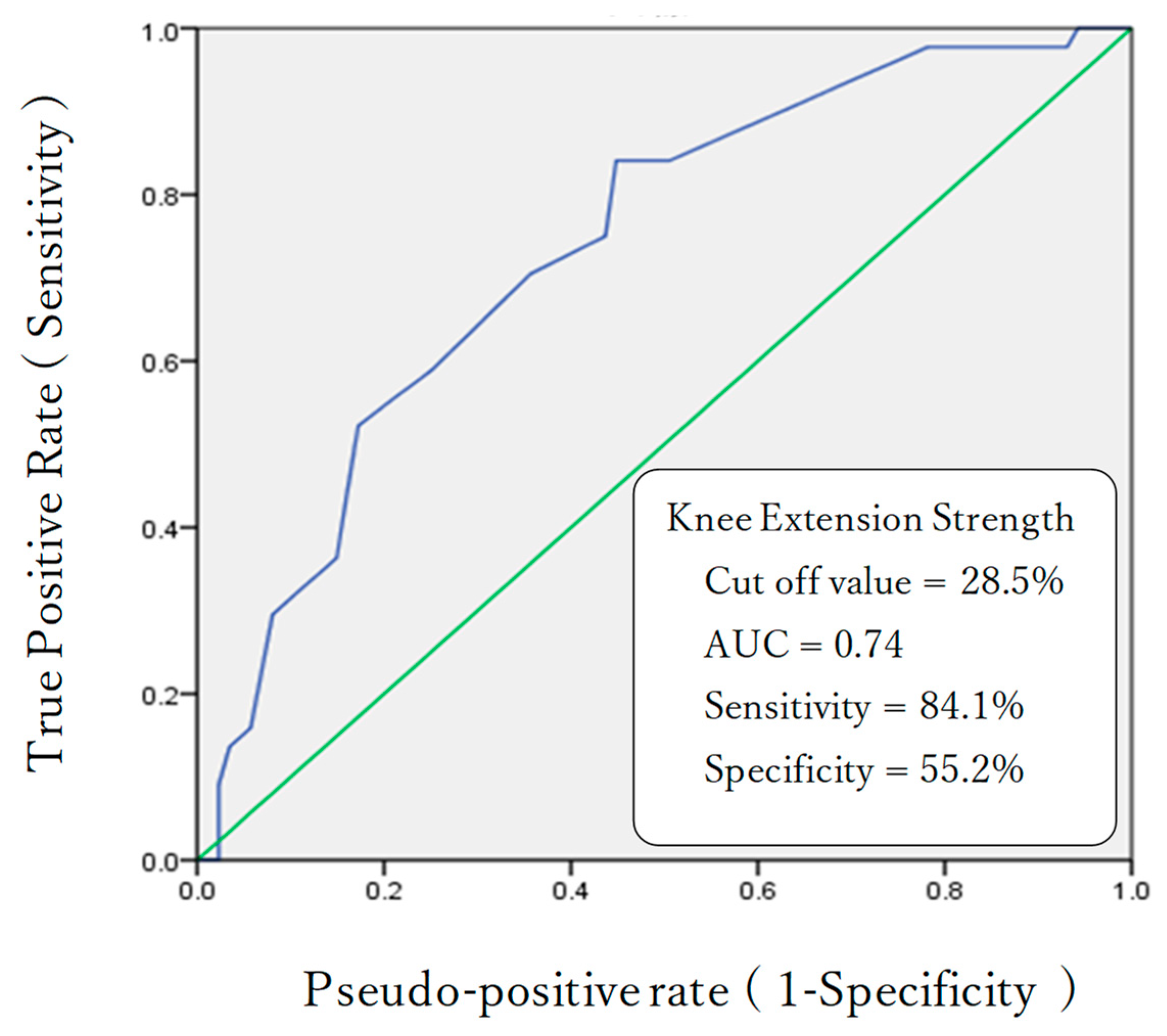
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seungmoon, S.; Hartmut, G. Predictive neuromechanical simulations indicate why walking performance declines with ageing. J. Physiol. 2018, 596, 1199–1210. [Google Scholar] [CrossRef]
- Ronthal, M. Gait Disorders and Falls in the Elderly. Med. Clin. N. Am. 2019, 103, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Damulin, I.V. Changes in walking in the elderly. Zhurnal Nevrol. I Psikhiatrii Im. S.S. Korsakova 2018, 118, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Whipple, M.O.; Hamel, A.V.; Talley, K.M.C. Fear of falling among community-dwelling older adults: A scoping review to identify effective evidence-based interventions. Geriatr. Nurs. 2018, 39, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Jahn, K.; Zwergal, A.; Schniepp, R. Gait disturbances in old age: Classification, diagnosis, and treatment from a neurological perspective. Dtsch. Arztebl. Int. 2010, 107, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Peel, N.M. Epidemiology of falls in older age. Can. J. Aging Rev. Can. Vieil. 2011, 30, 7–19. [Google Scholar] [CrossRef]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Miyasike-daSilva, V.; Tung, J.Y.; Zabukovec, J.R.; McIlroy, W.E. Use of mobility aids reduces attentional demand in challenging walking conditions. Gait Posture 2013, 37, 287–289. [Google Scholar] [CrossRef]
- Lyu, Z.; Wang, L.; Gao, X.; Ma, Y. The Identification of Elderly People with High Fall Risk Using Machine Learning Algorithms. Healthcare 2022, 11, 47. [Google Scholar] [CrossRef]
- Pfortmueller, C.A.; Lindner, G.; Exadaktylos, A.K. Reducing fall risk in the elderly: Risk factors and fall prevention, a systematic review. Minerva Med. 2014, 105, 275–281. [Google Scholar]
- Patcharawan, S.; Candidate; Thiwabhorn, T.; Supapon, K.; Lugkana, M.; Sugalya, A. Walking devices used by community dwelling elderly: Proportion, types, and associated factors. Hong Kong Physiother. J. 2015, 33, 34–41. [Google Scholar]
- Omana, H.A.; Madou, E.; Divine, A.; Wittich, W.; Hill, K.D.; Johnson, A.M.; Holmes, J.D.; Hunter, S.W. The effect of first-time 4-wheeled walker use on the gait of younger and older adults. PM&R 2022, 14, 1333–1342. [Google Scholar] [CrossRef]
- Bradley, S.M.; Hernandez, C.R. Geriatric assistive devices. Am. Fam. Physician. 2011, 84, 405–411. [Google Scholar]
- Thies, S.B.; Bates, A.; Costamagna, E.; Kenney, L.; Granat, M.; Webb, J.; Howard, D.; Baker, R.; Dawes, H. Are older people putting themselves at risk when using their walking frames? BMC Geriatr. 2020, 20, 90. [Google Scholar] [CrossRef]
- Liu, H.H. Assessment of rolling walkers used by older adults in senior-living communities. Geriatr. Gerontol. Int. 2009, 9, 124–130. [Google Scholar] [CrossRef]
- Iolascon, G.; Michini, C.; Sentinella, R.K.; Aulicino, M.; Moretti, A. The role of assistive devices in frail elderly people with fragility fractures: A narrative review. Int. J. Bone Frag. 2021, 1, 53–55. [Google Scholar] [CrossRef]
- Bateni, H.; Maki, E.B. Assistive devices for balance and mobility: Benefits, demands, and adverse consequences. Arch. Phys. Med. Rehabil. 2005, 86, 134–145. [Google Scholar] [CrossRef]
- Li, C.; Su, M.; Xu, J.; Jin, H.; Sun, L. A between-subject fNIRS-BCI study on detecting self-regulated intention during walking. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Hazra, S.; Dutta, S.; Nandy, A. A study on understanding cognitive states through gait analysis. Cogn. Syst. Res. 2021, 69, 41–49. [Google Scholar] [CrossRef]
- Nishijima, T.; Koyama, R.; Naito, I.; Hatakeyama, S.; Yamasaki, H.; Oku, T. Relationship between knee extension muscle strength and walking ability in the elderly patients. Rigakuryoho Kagaku 2004, 19, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health. Labour and Welfare: Overview of Actual Statistics on Nursing Care Benefit Expenses. ETC. 2021. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kaigo/kyufu/21/dl/02.pdf (accessed on 3 December 2022).
- Yamada, M.; Arai, H. Long-term care system in Japan. Ann. Geriatr. Med. Res. 2020, 24, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Shimada, H.; Tsutsumimoto, K.; Makino, K.; Nakakubo, S.; Ishii, H.; Suzuki, T.; DOI, T. Physical frailty and future costs of long-term care in older adults: Results from the NCGG-SGS. Gerontology 2021, 67, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Park, K.W.; Pavlik, V.N.; Rountree, S.D.; Darby, E.J.; Doody, R.S. Is functional decline necessary for a diagnosis of Alzheimer’s disease? Dement. Geriatr. Cogn. Disord. 2007, 24, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef]
- Pachet, A.; Astner, K.; Brown, L. Clinical utility of the mini-mental status examination when assessing decision-making capacity. J. Geriatr. Psychiatry Neurol. 2010, 23, 3–8. [Google Scholar] [CrossRef]
- Fusco-Gessick, B.; Cournan, M. Using Functional Independence Measure Subscales to Predict Falls-Rapid Assessment. Rehabil. Nurs. 2019, 44, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Education, Culture, Sports, Science and Technology. Japan’s Education at a Glance. 2006. Available online: https://www.mext.go.jp/component/english/__icsFiles/afieldfile/2011/03/07/1303013_000.pdf (accessed on 16 November 2022).
- Kamide, N.; Kamiya, R.; Nakazono, T.; Ando, M. Reference values for hand grip strength in Japanese community-dwelling elderly: A meta-analysis. Environ. Health Prev. Med. 2015, 20, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Iwase, H.; Murata, S.; Anami, K.; Matsuo, N.; Sato, H.; Harada, J.; Imanishi, K.; Fukunaga, K.; Madoba, K. Examination of a Simple Lower Limb Function Assessment Method: The 10-second Chair-standing Test. Rigakuryoho Kagaku 2013, 28, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Murata, S.; Goda, A.; Nakano, H.; Yasui, M.; Takaya, M.; Hanashiro, A.; Kamijo, K. Relationships between different stand-up test and physical functions among elderly day-care users. Jpn. J. Health Prom. Phys. Ther. 2020, 10, 67–71. [Google Scholar] [CrossRef]
- Murata, S.; Otao, H.; Murata, J.; Horie, J.; Onituka, M.; Yokoyama, T.; Hara, H. Relationship between the 10-second chair stand test (frail CS−10) and physical function among the frail elderly. Rigakuryoho Kagaku 2010, 25, 431–435. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.J.; Chang, Y.S.; Yang, S.W. Using single leg standing time to predict the fall risk in elderly. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2013, 2013, 7456–7458. [Google Scholar] [CrossRef] [PubMed]
- Owada, H.; Otomo, A.; Suzuki, Y.; Suto, A.; Murakami, K.; Kishikawa, Y. The relationship between frailty and motor function among living in the community elderly females. J. Phys. Ther. Sci. 2023, 35, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Kamide, N.; Takahashi, K.; Shiba, Y. Reference values for the Timed Up and Go test in healthy Japanese elderly people: Determination using the methodology of meta-analysis. Geriatr. Gerontol. Int. 2011, 11, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Hughes, G. Youden’s index and the weight of evidence. Methods Inf. Med. 2015, 54, 198–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forrest, G.; Chen, E. Efficient Assessment of Risk of Fall. Rehab. Nurs. 2016, 41, 320–325. [Google Scholar] [CrossRef]
- Singhal, S.; Bansal, R.; Dewangan, G.C.; Upadhyay, A.D.; Dwivedi, S.N.; Chatterjee, P.; Chakrawarty, A.; Dey, A.B. Low one-repetition-maximum knee extension is significantly associated with poor grip strength, female sex, and various aging-related syndromes. Aging Med. 2020, 3, 125–131. [Google Scholar] [CrossRef]
- Lee, Y.; Chang, S.; Kao, C.; Tsai, H.C. Muscle Strength, Physical Fitness, Balance, and Walking Ability at Risk of Fall for Prefrail Older People. Biomed Res. Int. 2022, 2022, 4581126. [Google Scholar] [CrossRef]
- Avin, K.G.; Hanke, T.A.; Kirk-Sanchez, N.; McDonough, C.M.; Shubert, T.E.; Hardage, J.; Hartley, G.; Academy of Geriatric Physical Therapy of the American Physical Therapy Association. Management of falls in community-dwelling older adults: Clinical guidance statement from the Academy of Geriatric Physical Therapy of the American Physical Therapy Association. Phys. Ther. 2015, 95, 815–834. [Google Scholar] [CrossRef] [Green Version]
- Zarei, H.; Norasteh, A.A.; Koohboomi, M. The relationship between muscle strength and range of motion in lower extremity with balance and risk of falling in Elderl. Physical Treatments—Specific. Phys. Ther. 2020, 10, 33–40. [Google Scholar]
- Uematsu, A.; Tsuchiya, K.; Kadono, N.; Kobayashi, H.; Kaetsu, T.; Hortobágyi, T.; Suzuki, S. A behavioral mechanism of how increases in leg strength improve old adults’ gait speed. PLoS ONE 2014, 9, 10–1371. [Google Scholar] [CrossRef]
- Ding, L.; Yang, F. Muscle weakness is related to slip-initiated falls among community-dwelling older adults. J. Biomech. 2016, 49, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, S.; Morishita, S.; Honda, Y.; Nagase, M.; Tsuda, K.; Mabuchi, S.; Kodama, N.; Domen, K. Examination of related factors and cut-off values for determining walking Independence of inpatients with medical disease in acute care hospitals. Rigaku Ryohogaku 2015, 42, 237–245. [Google Scholar]
- Rantanen, T.; Guralnik, J.M.; Ferrucci, L.; Penninx, B.W.; Leveille, S.; Sipilä, S.; Fried, L.P. Coimpairments as predictors of severe walking disability in older women. J. Am. Geriatr. Soc. 2001, 49, 21–27. [Google Scholar] [CrossRef]
- Bento, P.C.; Pereira, G.; Ugrinowitsch, C.; Rodacki, A.L. Peak torque and rate of torque development in elderly with and without fall history. Clin. Biomech. 2010, 25, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Karabin, M.J.; Sparto, P.J.; Rosano, C.; Redfern, M.S. Impact of strength and balance on Functional Gait Assessment performance in older adults. Gait Posture 2022, 91, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Faruqui, S.R.; Jaeblon, T. Ambulatory assistive devices in orthopaedics: Uses and modifications. J. Am. Acad. Orthop. Surg. 2010, 18, 41–50. [Google Scholar] [CrossRef]
- Youdas, J.W.; Kotajarvi, B.J.; Padgett, D.J.; Kaufman, K.R. Partial weight-bearing gait using conventional assistive devices. Arch. Phys. Med. Rehabil. 2005, 86, 394–398. [Google Scholar] [CrossRef]
- Aragaki, D.R.; Nasmyth, M.C.; Schultz, S.C.; Nguyen, G.M.; Yentes, J.M.; Kao, K.; Perell, K.; Fang, M.A. Immediate effects of contralateral and ipsilateral cane use on normal adult gait. PM&R 2009, 1, 208–213. [Google Scholar] [CrossRef]
- Arnold, P.; Bautmans, I. The influence of strength training on muscle activation in elderly persons: A systematic review and meta-analysis. Exp. Gerontol. 2014, 58, 58–68. [Google Scholar] [CrossRef]
- Lippi, L.; de Sire, A.; Mezian, K.; Curci, C.; Perrero, L.; Turco, A.; Andaloro, S.; Ammendolia, A.; Fusco, N.; Invernizzi, M. Impact of exercise training on muscle mitochondria modifications in older adults: A systematic review of randomized controlled trials. Aging Clin. Exp. Res. 2022, 34, 1495–1510. [Google Scholar] [CrossRef]
- Aranda-Reneo, I.; Albornos-Muñoz, L.; Rich-Ruiz, M.; Cidoncha-Moreno, M.Á.; Pastor-López, Á.; Moreno-Casbas, T.; Otago Project Working Group. Cost-Effectiveness of an Exercise Programme That Provided Group or Individual Training to Reduce the Fall Risk in Healthy Community-Dwelling People Aged 65–80: A Secondary Data Analysis. Healthcare 2021, 9, 714. [Google Scholar] [CrossRef] [PubMed]
- Usmani, S.; Saboor, A.; Haris, M.; Khan, M.A.; Park, H. Latest Research Trends in Fall Detection and Prevention Using Machine Learning: A Systematic Review. Sensors 2021, 21, 5134. [Google Scholar] [CrossRef] [PubMed]
- Grootswagers, P.; Vaes, A.M.M.; Hangelbroek, R.; Tieland, M.; van Loon, L.J.C.; de Groot, L.C.P.G.M. Relative Validity and Reliability of Isometric Lower Extremity Strength Assessment in Older Adults by Using a Handheld Dynamometer. Sport. Health 2022, 14, 899–905. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All | Solo Walking Group | Walking Aid Group | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||||
| Male (n) | 49 | 33 | 16 | 0.86 | ||||||
| Female (n) | 82 | 54 | 28 | |||||||
| Mean | ± | SD | Mean | ± | SD | Mean | ± | SD | ||
| Age (years) | 82.7 | ± | 6.4 | 82.6 | ± | 6.1 | 82.9 | ± | 6.7 | 0.80 |
| MMSE (points) | 24.3 | ± | 2.5 | 24.5 | ± | 2.5 | 24.1 | ± | 2.3 | 0.42 |
| Main disease | ||||||||||
| Bone fracture (n) | 37 | 22 | 15 | 0.66 | ||||||
| Osteoarthritis (n) | 25 | 16 | 9 | |||||||
| Cerebrovascular disease (n) | 20 | 13 | 7 | |||||||
| Aging (n) | 15 | 10 | 5 | |||||||
| Other (n) | 34 | 26 | 8 | |||||||
| Solo Walking Group | Walking Aid Group | p-Value | |||||
| Mean | ± | SD | Mean | ± | SD | ||
| FIM-M (points) | 76.9 | ± | 7.3 | 73.7 | ± | 6.1 | 0.00 * |
| Grip strength (kg) | 15.7 | ± | 4.6 | 14.8 | ± | 4.4 | 0.21 |
| Knee extension strength (%) | 29.2 | ± | 5.4 | 25.0 | ± | 4.0 | 0.00 * |
| Frail CS-10 (times) | 3.4 | ± | 1.3 | 2.6 | ± | 1.3 | 0.00 * |
| SLS (s) | 2.9 | ± | 3.7 | 1.5 | ± | 1.1 | 0.00 * |
| TUG (s) | 14.2 | ± | 4.2 | 17.4 | ± | 4.0 | 0.00 * |
| MMSE (points) | 24.5 | ± | 2.5 | 24.1 | ± | 2.3 | 0.48 |
| B | SD | Wald | p-Value | Exp (B) | 95% CI | |
|---|---|---|---|---|---|---|
| FIM-M | 0.03 | 0.04 | 0.40 | 0.53 | 1.03 | 0.95–1.11 |
| Knee extension strength | −0.14 | 0.06 | 6.25 | 0.00 * | 0.87 | 0.78–0.97 |
| Frail CS-10 | −0.10 | 0.21 | 0.22 | 0.64 | 0.91 | 0.61–1.36 |
| SLS | −0.27 | 0.18 | 2.26 | 0.13 | 0.76 | 0.54–1.09 |
| TUG | 0.05 | 0.07 | 0.69 | 0.40 | 1.06 | 0.93–1.20 |
| Constant | 1.11 | 3.58 | 0.10 | 0.76 | 3.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakano, Y.; Murata, S.; Goda, A.; Nakano, H. Factors Influencing the Use of Walking Aids by Frail Elderly People in Senior Day Care Centers. Healthcare 2023, 11, 858. https://doi.org/10.3390/healthcare11060858
Sakano Y, Murata S, Goda A, Nakano H. Factors Influencing the Use of Walking Aids by Frail Elderly People in Senior Day Care Centers. Healthcare. 2023; 11(6):858. https://doi.org/10.3390/healthcare11060858
Chicago/Turabian StyleSakano, Yuya, Shin Murata, Akio Goda, and Hideki Nakano. 2023. "Factors Influencing the Use of Walking Aids by Frail Elderly People in Senior Day Care Centers" Healthcare 11, no. 6: 858. https://doi.org/10.3390/healthcare11060858