
Quality Indicators during Delivery and the Immediate Postpartum Period: A Modified Delphi Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
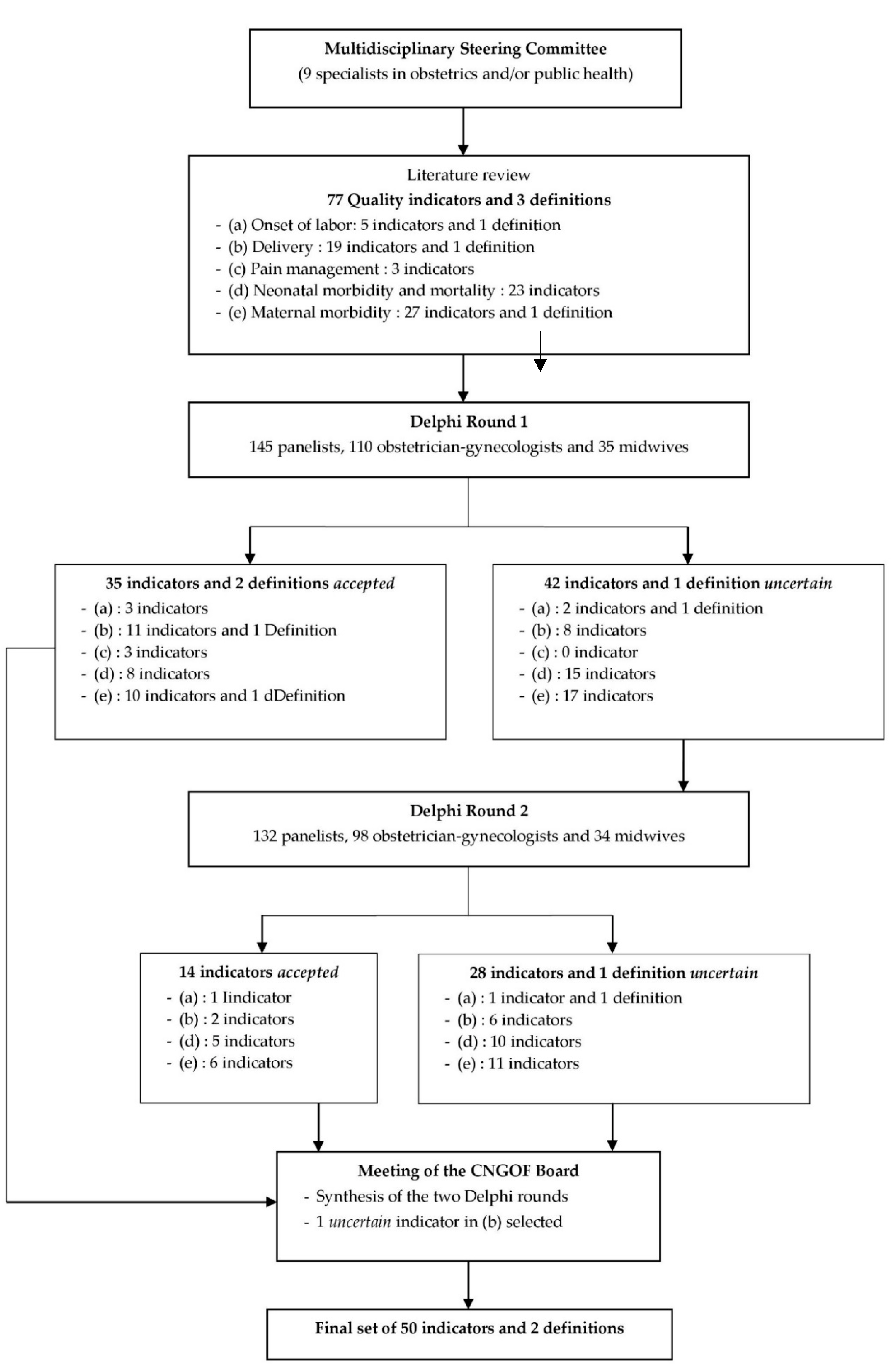
2.2. Literature Review
2.3. Modified Delphi Process
2.3.1. Participants
2.3.2. Data Collection
2.3.3. Data Analysis
2.4. External Validity
3. Results
3.1. Modified Delphi Survey Questionnaire
3.2. Description of the Modified Delphi Survey Panel
3.3. Modified Delphi Survey Analysis
3.4. External Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization—Millennium Development Goals (MDGs). Available online: https://www.who.int/news-room/fact-sheets/detail/millennium-development-goals-(mdgs) (accessed on 9 February 2023).
- Talungchit, P.; Liabsuetrakul, T.; Lindmarck, G. Development and assessment of indicators for quality of care in severe preeclampsia/eclampsia and postpartum hemorrhage. J. Healthc. Qual. 2013, 35, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.; Mainz, J.; Bartels, P. Selection of indicators for continuous monitoring of patient safety: Recommendations of the project ’safety improvement for patients in Europe’. Int. J. Qual. Health Care 2009, 21, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Bonfill, X.; Roqué, M.; Aller, M.B.; Osorio, D.; Foradada, C.; Vives, A.; Rigau, D. Development of quality of care indicators from systematic reviews: The case of hospital delivery. Implement. Sci. 2013, 8, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesmodel, U.S.; Jolving, L.R. Measuring and improving quality in obstetrics—The implementation of national indicators in Denmark. Acta Obstet. Gynecol. Scand. 2011, 90, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Korst, L.M.; Gregory, K.D.; Lu, M.C.; Reyes, C.; Hobel, C.J.; Chavez, G.F. A framework for the development of maternal quality of care indicators. Matern. Child Health J. 2005, 9, 317–341. [Google Scholar] [CrossRef]
- Sibanda, T.; Fox, R.; Draycott, T.J.; Mahmood, T.; Richmond, D.; Simms, R.A. Intrapartum care quality indicators: A systematic approach for achieving consensus. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 166, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, A.; Gissler, M.; Bolumar, F.; Rasmussen, S. The availability of perinatal health indicators in Europe. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 111, S15–S32. [Google Scholar] [CrossRef]
- Wildman, K.; Blondel, B.; Nijhuis, J.; Defoort, P.; Bakoula, C. European indicators of health care during pregnancy, delivery and the postpartum period. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 111, S53–S65. [Google Scholar] [CrossRef]
- Melman, S.; Schoorel, E.C.N.; de Boer, K.; Burggraaf, H.; Derks, J.B.; van Dijk, D.; van Dillen, J.; Dirksen, C.D.; Duvekot, J.J.; Franx, A.; et al. Development and measurement of guidelines-based quality indicators of caesarean section care in the Netherlands: A Rand-modified Delphi procedure and retrospective chart review. PLoS ONE 2016, 11, e0145771. [Google Scholar] [CrossRef] [Green Version]
- Zeitlin, J.; Wildman, K.; Bréart, G.; Alexander, S.; Barros, H.; Blondel, B.; Buitendijk, S.; Gissler, M.; Macfarlane, A. Selecting an indicator set for monitoring and evaluating perinatal health in Europe: Criteria, methods and results from the PERISTAT project. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 111, S5–S14. [Google Scholar] [CrossRef]
- Bailit, J.L. Measuring the quality of inpatient care. Obstet. Gynecol. Surv. 2007, 62, 207–213. [Google Scholar] [CrossRef]
- Alkema, L.; Chou, D.; Hogan, D.; Zhang, S.; Moller, A.B.; Gemmill, A.; Fat, D.M.; Boerma, T.; Temmerman, M.; Mathers, C.; et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: A systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet 2016, 38, 462–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haller, G.; Camparini-Righini, N.; Kern, C.; Pfister, R.E.; Morales, M.; Berner, M.; Clergue, F.; Irion, O. Patient safety indicators for obstetrics: A Delphi based study. J. Gynecol. Obstet. Biol. Reprod. 2010, 39, 371–378. [Google Scholar] [CrossRef]
- Bunch, K.J.; Allin, B.; Jolly, M.; Hardie, T.; Knight, M. Developing a set of consensus indicators to support maternity service quality improvement: Using Core Outcome Set methodology including a Delphi process. BJOG 2018, 125, 1612–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulkedid, R.; Sibony, O.; Goffinet, F.; Fauconnier, A.; Branger, B.; Alberti, C. Quality indicators for continuous monitoring to improve maternal and infant health in maternity departments: A modified Delphi survey of an international multidisciplinary panel. PLoS ONE 2013, 8, e60663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauvegrain, P.; Chantry, A.A.; Chiesa-Dubruille, C.; Keita, H.; Goffinet, F.; Deneux-Tharaux, C. Monitoring quality of obstetric care from hospital discharge databases: A Delphi survey to propose a new set of indicators based on maternal health outcomes. PLoS ONE 2019, 14, e0211955. [Google Scholar] [CrossRef]
- Deneux-Tharaux, C.; Morau, E.; Dreyfus, M. Maternal mortality in France 2013–2015: An evolving profile. Gynecol. Obstet. Fertil. Senol. 2021, 49, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Zeitlin, J.; Alexander, S.; Barros, H.; Blondel, B.; Delnord, M.; Durox, M.; Gissler, M.; Hindori-Mohangoo, A.D.; Hocquette, A.; Szamotulska, K.; et al. Perinatal health monitoring through a European lens: Eight lessons from the Euro-Peristat report on 2015 births. BJOG 2019, 126, 1518–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondel, B.; Durox, M.; Zeitlin, J. How perinatal health in France compared with other European countries in 2015: Some progress but also some concerns about newborn health. Arch. Pediatr. 2019, 26, 249–251. [Google Scholar] [CrossRef]
- European Perinatal Health Report—Core Indicators of the Health and Care of Pregnant Women and Babies in Europe from 2015 to 2019. Available online: https://www.europeristat.com/images/Euro-Peristat_Fact_sheets_2022_for_upload.pdf (accessed on 9 February 2023).
- Corallo, A.N.; Croxford, R.; Goodman, D.C.; Bryan, E.L.; Srivastava, D.; Stukel, T.A. A systematic review of medical practice variation in OECD countries. Health Policy 2014, 114, 5–14. [Google Scholar] [CrossRef]
- The Royal College of Obstetricians and Gynaecologists. Patterns of Maternity Care in English NHS Hospitals, 2011–2012; RCOG Press: London, UK, 2013. [Google Scholar]
- Vendittelli, F.; Tassié, M.C.; Gerbaud, L.; Lémery, D. Appropriateness of elective casarean deliveries in a perinatal network: A cross-sectional study. BMC Pregnancy Childbirth 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vendittelli, F.; Rivière, O.; Crenn-Hébert, C.; Giraud-Roufast, A.; Audipog Sentinel Network. Do perinatal guidelines have an impact on obstetric practices? Rev. Epidemiol. Sante Publique 2012, 60, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé—Indications de la Césarienne Programmée à Terme. Méthode Recommandations pour la Pratique Clinique. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2012-03/indications_cesarienne_programme_-_argumentaire.pdf (accessed on 9 February 2023).
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and Reporting the Delphi Method for Selecting Healthcare Quality Indicators: A Systematic Review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef] [PubMed]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R.; Lazaro, P.; van het Loo, M.; McDonnell, J.; Vader, J.; Kahan, J.P. The RAND/UCLA Appropriateness Method User’s Manual; RAND Corporation: Santa Monica, CA, USA, 2001. [Google Scholar]
- Jones, J.; Hunter, D. Consensus methods for medical and health services research. BMJ 1995, 311, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.S. Can we reduce the cesarean section rate? Best Pract. Res. Clin. Obstet. Gynaecol. 2001, 15, 179–194. [Google Scholar] [CrossRef] [PubMed]
- FIGO Working Group on Challenges in Care of Mothers and Infants during Labour and Delivery. Best practice advice on the 10-Group Classification System for cesarean deliveries. Int. J. Gynecol. Obstet. 2016, 135, 232–233. [Google Scholar] [CrossRef]
- Jorm, A.F. Using the Delphi expert consensus method in mental health research. Aust. N.Z.J. Psychiatry 2015, 49, 887–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Dalkey, N.C. The Delphi Method: An Experimental Study of Group Opinion; RAND Corporation: Santa Monica, CA, USA, 1969. [Google Scholar]
- Murphy, M.K.; Black, N.A.; Lamping, D.L.; McKee, C.M.; Sanderson, C.F.; Askham, J.; Marteau, T. Consensus development methods, and their use in clinical guideline development. Health Technol. Assess. 1998, 2, 1–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumsion, T. The Delphi technique: An adaptive research tool. Br. J. Occup. Ther. 1998, 61, 153–156. [Google Scholar] [CrossRef]
- République Française, Santé Publique France, Inserm—Enquête Nationale Périnatale. Rapport 2021. Les naissances, le suivi à deux mois et les établissements. Situation et évolution depuis 2016. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-de-la-mere-et-de-l-enfant/surdite-permanente-neonatale/documents/enquetes-etudes/enquete-nationale-perinatale.-rapport-2021.-les-naissances-le-suivi-a-deux-mois-et-les-etablissements (accessed on 9 February 2023).
- David, S.; Mamelle, N.; Riviere, O. Estimation of an expected caesarean section rate, taking into account the case mix of a maternity hospital. Analysis from the AUDIPOG Sentinelle Network (France). Obstetricians of AUDIPOG. Association of Users of Computerised Files in Perinatalogy, Obstetrics and Gynaecology. BJOG 2001, 108, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Pratt, S.; Gluck, P.; Nielsen, P.; Risser, D.; Greenberg, P.; Marcus, R.; Goldman, M.; Shapiro, D.; Pearlman, M.; et al. Assessing quality obstetrical care: Development of standardized measures. Jt. Comm. J. Qual. Patient Saf. 2006, 32, 497–505. [Google Scholar] [CrossRef]
- Foglia, L.M.; Nielsen, P.E.; Hemann, E.A.; Walker, S.; Pates, J.A.; Napolitano, P.G.; Deering, S. Accuracy of the Adverse Outcome Index: An Obstetrical Quality Measure. Jt. Comm. J. Qual. Patient Saf. 2015, 41, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Main, E.K.; Moore, D.; Farrell, B.; Schimmel, L.D.; Altman, R.J.; Abrahams, C.; Campbell Bliss, M.; Polivy, L.; Sterling, J. Is there a useful cesarean birth measure? Assessment of the nulliparous term singleton vertex cesarean birth rate as a tool for obstetric quality improvement. Am. J. Obstet. Gynecol. 2006, 194, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- Bertillot, H. How quality indicators take hold in French hospital: Mechanisms of a soft institutionalization. Sociologies 2020, 1–15. (In French) [Google Scholar] [CrossRef]
- Ministère des Solidarités et de la Santé—Décret n° 2021-1613 du 9 décembre 2021 portant modification De dispositions réglementaires du code de la sécurité sociale relatives à l’amélioration de la qualité et de la sécurité des soins. Available online: https://www.legifrance.gouv.fr/download/file/k9J4QampA_S_KWuxcrXD3mPztg_RyZO4BL7nbsvBufc=/JOE_TEXTE (accessed on 9 February 2023).
- Abelhauser, A.; Gori, R.; Sauret, M.J. La Folie Évaluation. Les Nouvelles Fabriques De La Servitude; Edition Fayard/Mille et Une Nuits: Paris, France, 2011. [Google Scholar]
- Todd, R. The End of Average: How We Succeed in A World That Values Sameness; HarperCollins: Toronto, ON, Canada, 2016. [Google Scholar]
- Dumesnil, J. Art Médical Et Normalisation Du Soin; Presse Universitaire de France: Paris, France, 2011. [Google Scholar]
- Wennberg, J. Which rate is right? N. Engl. J. Med. 1986, 314, 310–311. [Google Scholar] [CrossRef]
- Vendittelli, F.; Barasinski, C.; Rivière, O.; Da Costa Correia, C.; Crenn-Hébert, C.; Dreyfus, M.; Legrand, A.; Gerbaud, L. Does the Quality of Postpartum Hemorrhage Local Protocols Improve the Identification and Management of Blood Loss after Vaginal Deliveries? A Multicenter Cohort Study. Healthcare 2022, 10, 992. [Google Scholar] [CrossRef] [PubMed]
- Saturno-Hernández, P.J.; Martínez-Nicolás, I.; Moreno-Zegbe, E.; Fernández-Elorriaga, M.; Poblano-Verástegui, O. Indicators for monitoring maternal and neonatal quality care: A systematic review. BMC Pregnancy Childbirth 2019, 19, 25. [Google Scholar] [CrossRef] [Green Version]
- Lazzaretto, E.; Nespoli, A.; Fumagalli, S.; Colciago, E.; Perego, S.; Locatelli, A. Intrapartum care quality indicators: A literature review. Minerva Ginecol. 2018, 70, 346–356. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Rounds of Modified Delphi Survey | Variables | Obstetrician-Gynecologists | Midwives | Total |
|---|---|---|---|---|
| First Round | N of participants | 110 | 35 | 145 |
| Age (years), mean ± SD | 51.5 ± 9.6 | 45.4 ± 11.6 | 49.7 ± 10.6 | |
| Sex, n (%) | ||||
| Female | 32 (29.1) | 34 (97.1) | 66 (45.5) | |
| Male | 78 (70.9) | 1 (2.9) | 79 (54.5) | |
| Professional experience (years), n (%) | ||||
| <10 | 19 (17.3) | 8 (22.9) | 27 (18.6) | |
| ≥10–<20 | 30 (27.3) | 4 (11.4) | 34 (23.4) | |
| ≥20–<30 | 37 (33.6) | 12 (34.3) | 49 (33.8) | |
| ≥30 | 24 (21.8) | 11 (31.4) | 35 (24.1) | |
| Current place of work 1, n (%) | ||||
| Academic hospital | 37 (33.6) | 13 (37.1) | 50 (34.5) | |
| General public hospital | 43 (39.1) | 17 (48.6) | 60 (41.4) | |
| Private hospital | 30 (27.3) | 5 (14.3) | 35 (24.1)) | |
| Maternity unit level 2, n (%) | ||||
| Level I | 27 (24.5) | 3 (8.6) | 30 (20.7) | |
| Level II | 41 (37.3) | 18 (51.4) | 59 (40.7) | |
| Level III | 42 (38.2) | 14 (40.0) | 56 (38.6) | |
| Mean number of annual deliveries, n (%) | ||||
| <500 | 3 (2.7) | 0 | 3 (2.1) | |
| ≥500–<1500 | 29 (26.4) | 10 (28.6) | 39 (26.9) | |
| ≥1500 | 78 (70.9) | 25 (71.4) | 103 (71.0) | |
| Second Round | N of participants | 98 | 34 | 132 |
| Age (years), mean ± SD | 51.5 ± 9.6 | 46.3 ± 11.7 | 50.2 ± 10.4 | |
| Sex, n (%) | ||||
| Female | 29 (29.6) | 1 (2.9) | 62 (47.0) | |
| Male | 69 (70.4) | 33 (97.1) | 70 (53.0) | |
| Professional experience (years), n (%) | ||||
| <10 | 17 (17.3) | 7 (20.6) | 24 (18.2) | |
| ≥10–<20 | 27 (27.6) | 5 (14.7) | 32 (24.2) | |
| ≥20–<20 | 31 (31.6) | 10 (29.4) | 41 (31.1) | |
| ≥30 | 23 (23.5) | 12 (35.3) | 35 (26.5) | |
| Current place of work 1, n (%) | ||||
| Academic hospital | 35 (35.7) | 13 (38.2) | 48 (36.4) | |
| General public hospital | 37 (37.8) | 16 (47.1) | 53 (40.2) | |
| Private hospital | 26 (26.5) | 5 (14.7) | 31 (23.5) | |
| Maternity unit level 2, n (%) | ||||
| Level I | 21 (21.4) | 3 (8.8) | 24 (18.2) | |
| Level II | 37 (37.8) | 17 (50.0) | 54 (40.9) | |
| Level III | 40 (40.8) | 14 (41.2) | 54 (40.9) | |
| Mean number of annual deliveries, n (%) | ||||
| <500 | 1 (1.0) | 0 | 1 (0.8) | |
| ≥500–<1500 | 25 (25.5) | 10 (29.4) | 35 (26.5) | |
| ≥1500 | 72 (73.5) | 24 (70.6) | 96 (72.7) |
| Category | Quality Indicators 1 or Definition | First Round (n = 145) | Second Round 2 (n = 132) | ||||
|---|---|---|---|---|---|---|---|
| Median Score 3 | Disagreement Index | Accepted, Rejected, or Uncertain 4 | Median Score 3 | Disagreement Index | Accepted, Rejected, or Uncertain 4 | ||
| Onset of labor | Spontaneous labor | 8 | 2.3 | Uncertain | 8 | 1.6 | Uncertain |
| Inductions of labor | 8 | 0.7 | Accepted | ||||
| Planned cesarean deliveries | 9 | 0.5 | Accepted | ||||
| Planned cesareans ≥ 39 wk | 8 | 0.7 | Accepted | ||||
| Definition of a planned cesarean delivery | 8 | 1.6 | Uncertain | 8 | 1.6 | Uncertain | |
| Cesarean deliveries before labor | 8 | 1.1 | Uncertain | 8 | 0.7 | Accepted | |
| Delivery | Vaginal deliveries | 9 | 0.3 | Accepted | |||
| Spontaneous vaginal deliveries (non-operative) | 9 | 0.5 | Accepted | ||||
| Instrumental vaginal deliveries | 9 | 0.3 | Accepted | ||||
| Global cesarean deliveries | 9 | 0.3 | Accepted | ||||
| Global cesarean deliveries ≥ 37 wk with a singleton pregnancy and a breech presentation | 9 | 0.7 | Accepted | ||||
| Cesarean deliveries in nulliparas | 9 | 0.7 | Accepted | ||||
| Cesareans in primiparas with one previous cesarean 5 | 8 | 2.3 | Uncertain | 8 | 2.3 | Uncertain | |
| Cesarean deliveries during labor | 8 | 0.7 | Accepted | ||||
| Adjusted proportion of cesarean deliveries | 7 | 1.1 | Uncertain | 7 | 1.1 | Uncertain | |
| Cesareans ≥37 wk in nulliparas women with a singleton pregnancy and a cephalic presentation | 9 | 1.1 | Uncertain | 9 | 0.7 | Accepted | |
| Cesarean deliveries after one previous cesarean | 9 | 0.5 | Accepted | ||||
| Cesarean deliveries in twin pregnancy | 9 | 0.5 | Accepted | ||||
| Planned cesarean deliveries ≥ 39 wk | 8 | 0.7 | Accepted | ||||
| Cesarean deliveries < 32 wk | 8 | 2.3 | Uncertain | 8 | 1.6 | Uncertain | |
| Unplanned cesareans after failure of labor induction | 9 | 0.7 | Accepted | ||||
| Unplanned cesareans after spontaneous onset of labor | 8 | 1.6 | Uncertain | 8 | 1.6 | Uncertain | |
| Definition of low risk at the end of pregnancy | 8 | 0.7 | Accepted | ||||
| Cesarean deliveries in women at low risk | 8 | 1.6 | Uncertain | 8 | 0.7 | Accepted | |
| Maternity Unit Performance Index | 5 | 4.4 | Uncertain | 5 | 4.4 | Uncertain | |
| Cesarean deliveries according to Robson classification | 6 | 1.6 | Uncertain | 7 | 1.6 | Uncertain | |
| Pain management | General anesthesia for cesarean delivery | 9 | 0.7 | Accepted | |||
| Epidural analgesia for vaginal delivery | 9 | 0.3 | Accepted | ||||
| Spinal analgesia for cesarean delivery | 9 | 0.7 | Accepted | ||||
| Neonatal morbidity and mortality | Apgar score < 7 at 5 min | 8 | 1.1 | Uncertain | 8 | 0.7 | Accepted |
| Apgar score < 5 at 5 min | 8 | 1.1 | Uncertain | 8 | 1.6 | Uncertain | |
| Births ≥37 wk with Apgar score <7 at 5 min | 8 | 0.7 | Accepted | ||||
| Live-born preterm infants < 37 wk | 9 | 0.7 | Accepted | ||||
| Live-born infants, preterm birth < 34 wk | 8 | 0.7 | Accepted | ||||
| Live-born infants, preterm birth < 33 wk | 7 | 3.4 | Uncertain | 7 | 3.4 | Uncertain | |
| Live-born infants, preterm birth < 32 wk | 8 | 1.1 | Uncertain | 8 | 0.7 | Accepted | |
| Live-born infants, preterm birth < 28 wk | 9 | 0.7 | Accepted | ||||
| Arterial pH < 7.10 | 8 | 1.6 | Uncertain | 8 | 0.7 | Accepted | |
| Arterial pH < 7.0 | 8 | 1.1 | Uncertain | 8 | 0.5 | Accepted | |
| Birth weight < 5th percentile for gestational age | 8 | 1.6 | Uncertain | 8 | 1.6 | Uncertain | |
| Birth weight < 3rd percentile for gestational age | 8 | 0.7 | Accepted | ||||
| Birth weight < 2750 g with birth ≥ 40 wk | 6 | 3.4 | Uncertain | 6 | 3.4 | Uncertain | |
| Birth weight < 2500 g | 7 | 3.4 | Uncertain | 7 | 3.4 | Uncertain | |
| Infant discharged from delivery unit with mother and birth ≥ 37 wk | 8 | 2.3 | Uncertain | 8 | 1.6 | Uncertain | |
| Neonatal transfers in resuscitation or intensive care or neonatology unit | 9 | 0.7 | Accepted | ||||
| Neonatal transfers in intensive care unit | 9 | 1.1 | Uncertain | 9 | 0.7 | Accepted | |
| Neonatal transfers in intensive care unit with birth weight > 2500 g | 7 | 1.6 | Uncertain | 7 | 1.6 | Uncertain | |
| Neonatal transfers to any neonatal units for inborn infants with birth ≥ 37 wk | 9 | 0.7 | Accepted | ||||
| Neonatal transfers to any neonatal units for inborn infants with birth ≥ 22 wk | 7 | 2.3 | Uncertain | 7 | 3.4 | Uncertain | |
| Uncomplicated births with a healthy infant | 8 | 1.1 | Uncertain | 8 | 1.6 | Uncertain | |
| Stillbirths | 9 | 0.7 | Accepted | ||||
| Stillbirths ≥ 28 wk | 8 | 1.1 | Uncertain | 8 | 1.6 | Uncertain | |
| Maternal morbidity | Postpartum hemorrhages > 500 mL (regardless of mode of delivery) | 9 | 1.6 | Uncertain | 9 | 1.6 | Uncertain |
| Postpartum hemorrhages > 500 mL for vaginal delivery | 9 | 0.7 | Accepted | ||||
| Postpartum hemorrhages > 1000 mL (regardless of mode of delivery) | 9 | 1.1 | Uncertain | 9 | 0.7 | Accepted | |
| Postpartum hemorrhages > 1000 mL for vaginal delivery | 9 | 1.1 | Uncertain | 9 | 0.7 | Accepted | |
| Postpartum hemorrhages > 1000 mL for cesarean delivery | 9 | 0.7 | Accepted | ||||
| Postpartum hemorrhages > 1500 mL (regardless of mode of delivery) | 8 | 2.3 | Uncertain | 8 | 2.3 | Uncertain | |
| Postpartum hemorrhages > 1500 mL for cesareans | 7 | 2.3 | Uncertain | 8 | 2.3 | Uncertain | |
| Blood transfusions in delivery or operating rooms | 9 | 0.5 | Accepted | ||||
| Hemostatic hysterectomy | 9 | 0.3 | Accepted | ||||
| Hemostatic surgery (other than hysterectomy) | 9 | 0.3 | Accepted | ||||
| Uterine rupture | 9 | 1.1 | Uncertain | 9 | 0.7 | Accepted | |
| Discharge from delivery unit by transfer to intensive care unit | 9 | 0.7 | Accepted | ||||
| Maternal morbidity | Intact perineum (without perineal suture) | 9 | 0.7 | Accepted | |||
| Intact perineum in spontaneous delivery | 8 | 3.4 | Uncertain | 8 | 1.6 | Uncertain | |
| Intact perineum in primiparas | 8 | 2.3 | Uncertain | 8 | 2.3 | Uncertain | |
| Episiotomies | 9 | 0.3 | Accepted | ||||
| Episiotomies in primiparas | 8 | 1.6 | Uncertain | 8 | 0.5 | Accepted | |
| Perineal lacerations (perineal tears and/or episiotomy) | 8 | 1.6 | Uncertain | 8 | 3.4 | Uncertain | |
| Perineal lacerations without episiotomy | 8 | 1.6 | Uncertain | 8 | 1.6 | Uncertain | |
| First-degree perineal tears 6 | 7 | 3.4 | Uncertain | 7 | 3.4 | Uncertain | |
| Second-degree perineal tears 7 | 7 | 2.3 | Uncertain | 8 | 2.3 | Uncertain | |
| Severe perineal tears (3rd- or 4th-degree) 8 | 9 | 0.3 | Accepted | ||||
| Severe perineal tears in instrumental vaginal delivery | 9 | 0.7 | Accepted | ||||
| Severe perineal tears in non-instrumental vaginal delivery | 9 | 1.1 | Uncertain | 9 | 0.3 | Accepted | |
| Severe perineal tears in forceps delivery | 8 | 2.3 | Uncertain | 8 | 0.7 | Accepted | |
| Severe perineal tears in vacuum delivery | 8 | 2.3 | Uncertain | 8 | 1.6 | Uncertain | |
| Adjusted proportion of severe perineal lacerations | 8 | 3.4 | Uncertain | 8 | 3.4 | Uncertain | |
| International definition of perineal tears 6,7,8 (first, second, third, and fourth degree) | 9 | 0.3 | Accepted | ||||
| Category | Quality Indicators 1 or Definitions | Numerator | Denominator |
|---|---|---|---|
| Onset of labor | Inductions of labor | Number of inductions of labor 2 | Total number of deliveries 2 |
| Planned cesarean deliveries | Number of planned cesarean deliveries performed on or before the scheduled due date (surgical indication recorded ≥ 48 h before performance) 2 | Total number of cesarean deliveries 2 | |
| Planned cesareans ≥ 39 wk | Number of planned cesarean deliveries ≥ 39 wk performed on or before the scheduled due date (surgical indication recorded ≥ 48 h before performance) 2 | Total number of planned cesarean deliveries 2 | |
| Cesareans before labor | Number of cesarean deliveries before labor 2 | Total number of cesarean deliveries 2 | |
| Delivery | Vaginal deliveries | Number of vaginal deliveries 2 | Total number of deliveries 2 |
| Spontaneous vaginal deliveries (non-instrumental) | Number of non-instrumental spontaneous vaginal deliveries 2 | Total number of vaginal deliveries 2 | |
| Instrumental vaginal deliveries | Number of instrumental vaginal deliveries 2,3 | Total number of vaginal deliveries 2 | |
| Global cesarean deliveries | Number of cesareans 2 | Total number of deliveries 2 | |
| Global cesareans ≥ 37 wk with a singletonpregnancy in breech presentation | Number of cesareans ≥ 37 wk with a singleton pregnancy in breech presentation 2 | Total number of deliveries ≥ 37 wk with a singleton pregnancy in breech presentation 2 | |
| Cesareans among nulliparas | Number of cesareans among nulliparas 2 | Total number of deliveries for nulliparas 2 | |
| Cesareans during labor | Number of cesareans during labor (among planned cesareans or planned vaginal deliveries) 2 | Total number of cesarean deliveries 2 | |
| Cesareans ≥ 37 wk for nulliparas with a singleton pregnancy in cephalic presentation | Number of cesareans ≥ 37 wk for nulliparas with a singleton pregnancy in cephalic presentation 2 | Total number of deliveries ≥ 37 wk for nulliparas with a singleton pregnancy in cephalic presentation 2 | |
| Cesareans after one previous cesarean | Number of cesareans after only one previous cesarean delivery 2 | Total number of deliveries with only oneprevious cesarean delivery 2 | |
| Cesareans in non-singleton pregnancy | Number of cesareans in non-singleton pregnancy 2 | Total number of non-singleton deliveries 2 | |
| Planned cesareans ≥ 39 wk | Number of planned cesareans ≥ 39 wk 2 | Total number of cesarean deliveries 2 | |
| Unplanned cesareans after failure of induction | Number of unplanned cesareans after induction of labor 2 | Total number of inductions of labor 2 | |
| Definition of low risk at the endof pregnancy | Low-risk women at the end of pregnancy defined as initially at low risk at the beginning of pregnancy (1), and at low risk during pregnancy (2), without placenta previa or other obstacle for a vaginal delivery, with a fetus in cephalic presentation. | ||
(1) Initially (at first consultation) at low risk:
| (2) Low-risk women during pregnancy:
| ||
| Cesareans in women at low risk | Number of cesareans in women at low risk 2,4 | Total number of deliveries in women at low risk 2 | |
| Cesarean sections according to Robson 10-group classification | Number of cesareans 2 in:
| Total number of deliveries 2 according to the description of each group (for example, for group 1: total number of deliveries in nulliparas, with a singleton cephalic fetus, ≥37 wk, in spontaneous labor) | |
| Pain management | General anesthesia for cesarean delivery | Number of women receiving general anesthesia for cesareans 2 | Total number of cesarean deliveries 2 |
| Epidural analgesia for vaginal delivery | Number of women receiving epidural analgesia for vaginal delivery 2 | Total number of vaginal deliveries 2 | |
| Spinal analgesia for cesareans | Number of women receiving spinal analgesia for cesareans 2 | Total number of cesarean deliveries 2 | |
| Neonatal morbidity and mortality | Apgar score < 7 at 5 min | Number of live-born infants with Apgar score < 7 at 5 min 2 | Total number of live-born infants (stillborn infants excluded) 2 |
| Births ≥ 37 wk with Apgar score < 7 at 5 min | Number of live-born infants with a birth ≥ 37 wk and an Apgar score < 7 at 5 min 2 | Total number of live-born infants ≥ 37 wk (stillborn infants excluded) 2 | |
| Live-born preterm neonate | Number of live-born infants before < 37 wk gestation 2 | Total number of live-born infants 2 | |
| Live-born infants before < 34 wk gestation | Number of live-born infants before < 34 wk gestation 2 | Total number of live-born infants 2 | |
| Live-born infants before < 32 wk gestation | Number of live-born infants before < 32 wk gestation 2 | Total number of live-born infants 2 | |
| Live-born infants before < 28 wk gestation | Number of live-born infants before < 28 wk gestation 2 | Total number of live-born infants 2 | |
| Arterial pH < 7.10 | Number of live-born infants with umbilical artery pH < 7.10 2 | Total number of live-born infants with umbilical artery pH measured 2 | |
| Arterial pH < 7.0 | Number of live-born infants with umbilical artery pH < 7.0 2 | Total number of live-born infants with umbilical artery pH measured 2 | |
| Birth weights < 3rd percentile for gestational age | Number of infants with a birth weight < 3rd percentile for gestational age 2 | Total number of newborns 2 | |
| Neonatal transfers to intensive care or neonatology unit | Number of live-born infants transferred to an intensive care or neonatology unit 2 | Total number of live-born infants (admissions for congenital malformations and transfer to kangaroo care unit excluded) 2 | |
| Neonatal transfers to intensive care unit | Number of live-born infants transferred to intensive care unit 2 | Total number of live-born infants (admissions for congenital malformations excluded) 2 | |
| Immediate transfers to any neonatal unit for infants born ≥ 37 wk | Number of infants born ≥37 wk transferred to any neonatal unit 2 | Total number of live-born infants ≥ 37 wk (admissions for congenital malformations excluded) 2 | |
| Stillbirths | Number of fetal or immediate neonatal deaths (including fetal deaths in utero, medical terminations of pregnancy, and intrapartum deaths) 2 | Total number of births (live-born or stillborn infants) 2 | |
| Maternal morbidity | Postpartum hemorrhages >500 mL for vaginal delivery | Number of postpartum hemorrhages > 500 mL for vaginal delivery 2 | Total number of vaginal deliveries 2 |
| Postpartum hemorrhages > 1000 mL (regardless of mode of delivery) | Number of postpartum hemorrhages > 1000 mL for delivery 2 | Total number of deliveries 2 | |
| Postpartum hemorrhage > 1000 mL for vaginal delivery | Number of postpartum hemorrhages > 1000 mL for vaginal delivery 2 | Total number of vaginal deliveries 2 | |
| Postpartum hemorrhages > 1000 mL for cesarean deliveries | Number of postpartum hemorrhages > 1000 mL for cesareans 2 | Total number of cesarean deliveries 2 | |
| Blood transfusions in delivery or operating room | Number of blood transfusions in the delivery or operating room 2 | Total number of deliveries 2 | |
| Hemostatic hysterectomies | Number of hemostatic hysterectomies 2 | Total number of deliveries 2 | |
| Hemostatic surgery (other than hysterectomy) | Number of hemostatic surgeries other than hysterectomies 2 | Total number of deliveries 2 | |
| Uterine ruptures | Number of complete or subperitoneal uterine ruptures (dehiscences excluded) 2 | Total number of deliveries 2 | |
| Discharge from delivery unit by transfer to adult intensive care unit | Number of women discharged from the delivery unit by a transfer to an intensive care unit 2 | Total number of deliveries 2 | |
| Intact perineum | Number of women with an intact perineum (without suture) 2 | Total number of deliveries 2 | |
| Episiotomies | Number of women with an episiotomy for vaginal delivery 2 | Total number of vaginal deliveries 2 | |
| Episiotomies in primiparas | Number of primiparas with an episiotomy in vaginal delivery 2 | Total number of vaginal deliveriesin primiparas 2 | |
| Severe perineal tears | Number of women with 3rd- and 4th-degree perineal tears 5 in vaginal delivery 2 | Total number of vaginal deliveries 2 | |
| Severe perineal tears for instrumental vaginal delivery | Number of women with 3rd- and 4th-degree perineal tears 5 for instrumental vaginal delivery 2 | Total number of instrumental vaginal deliveries (forceps, vacuum, spatula) 2 | |
| Severe perineal tears for non-instrumental vaginal delivery | Number of women with 3rd- and 4th-degree perineal tears 5 in non-instrumental vaginal delivery 2 | Total number of non-instrumental vaginal deliveries 2 | |
| Severe perineal tears for forceps delivery | Number of women with 3rd- and 4th-degree perineal tears 5 ininstrumental vaginal delivery using forceps 2 | Total number of instrumental vaginal deliveries using forceps 2 | |
| International definition of perineal tears (first, second, third, and fourth degrees) |
| ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guiguet-Auclair, C.; Rivière, O.; Gerbaud, L.; Vendittelli, F. Quality Indicators during Delivery and the Immediate Postpartum Period: A Modified Delphi Study. Healthcare 2023, 11, 848. https://doi.org/10.3390/healthcare11060848
Guiguet-Auclair C, Rivière O, Gerbaud L, Vendittelli F. Quality Indicators during Delivery and the Immediate Postpartum Period: A Modified Delphi Study. Healthcare. 2023; 11(6):848. https://doi.org/10.3390/healthcare11060848
Chicago/Turabian StyleGuiguet-Auclair, Candy, Olivier Rivière, Laurent Gerbaud, and Françoise Vendittelli. 2023. "Quality Indicators during Delivery and the Immediate Postpartum Period: A Modified Delphi Study" Healthcare 11, no. 6: 848. https://doi.org/10.3390/healthcare11060848