
Detection of Drug-Related Problems through a Clinical Decision Support System Used by a Clinical Pharmacy Team
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design
2.3. Creation and Optimization of Clinical Rules
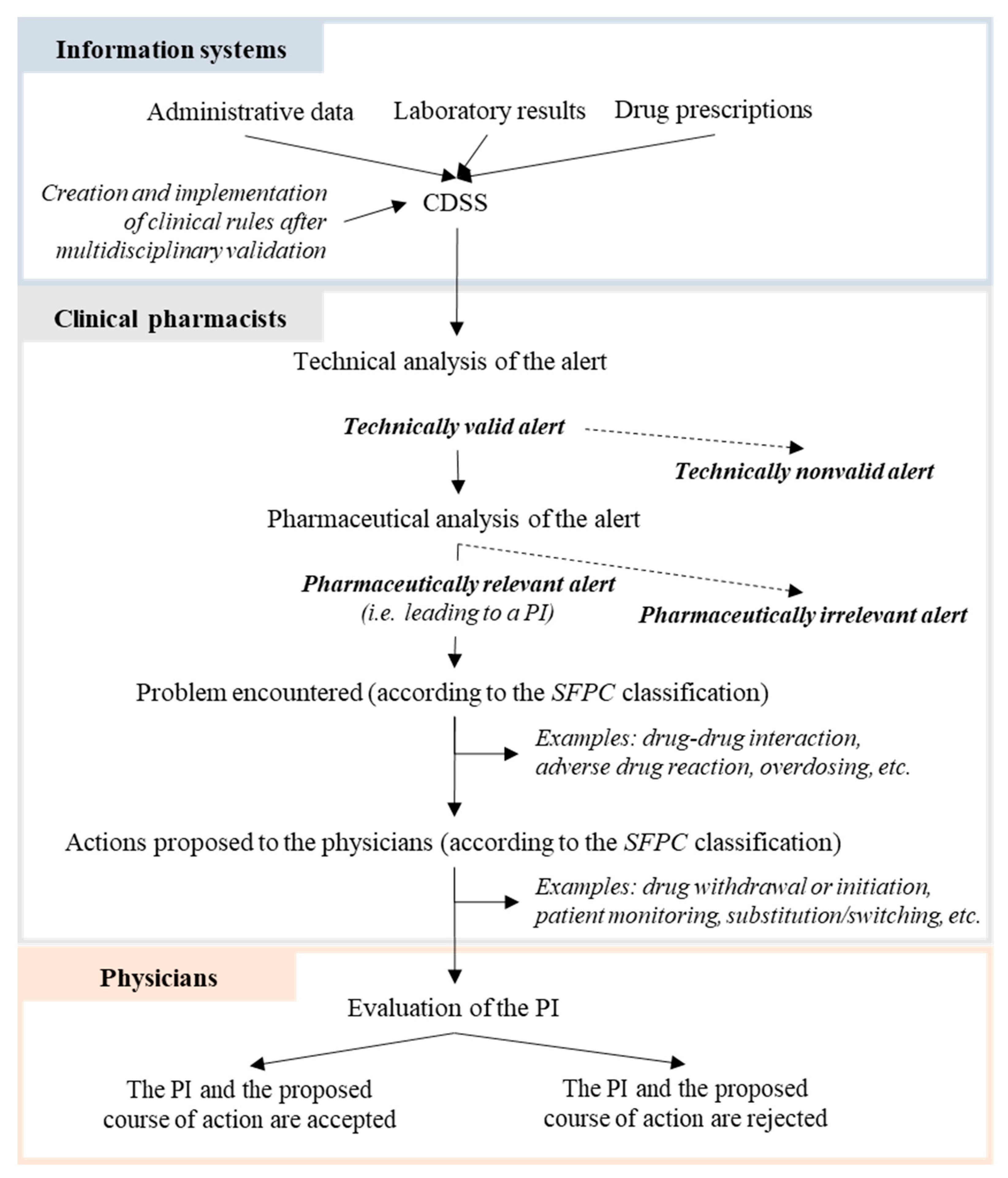
- Rule criteria were based on data collected by the CDSS: laboratory results (e.g., a threshold of 5 mM for blood potassium), drug prescriptions, drug dose levels (e.g., the prescription of more than 1000 mg of metformin three times a day) and the patient’s administrative data (e.g., age over 75).
- Criticality of the alert was based on the validated French classification of clinical, health, economic, and organizational impacts of PIs developed by the French Society of Clinical Pharmacy (Société Française de Pharmacie Clinique (SFPC)) (see Suppl. Data Table S1) [21]. Criticality is based on the addition of these various weighted impacts. The establishment of criticality rules allowed us to distinguish between critical and noncritical alerts. Critical alerts were defined as those with a criticality score of 7 or more (e.g., maintaining an antivitamin K with an INR ≥ 6). This criticality threshold of 7 corresponds to a threshold where rapid intervention was deemed necessary according to the project committee and the clinical pharmacy team. Noncritical alerts were defined as those with a criticality score below 7 (e.g., prescription of hypoglycemic sulfonamide among elderly patients).
- Pharmacist interventions (PIs) and the course of action were proposed for each rule by the project committee and the clinical pharmacy team, based on guidelines or clinical expertise. The PI could recommend definitive discontinuation, temporary discontinuation or the modification of drug treatment, patient monitoring, or laboratory assays. The course of action was also proposed in order to provide to the clinical pharmacy team the process of what to do when an alert was triggered. This course of action was validated by the entire clinical pharmacy team.
2.4. Organization of the Clinical Pharmacy Team following Implementation of the CDSS
2.5. Analysis of Alerts/Monitoring of Indicators
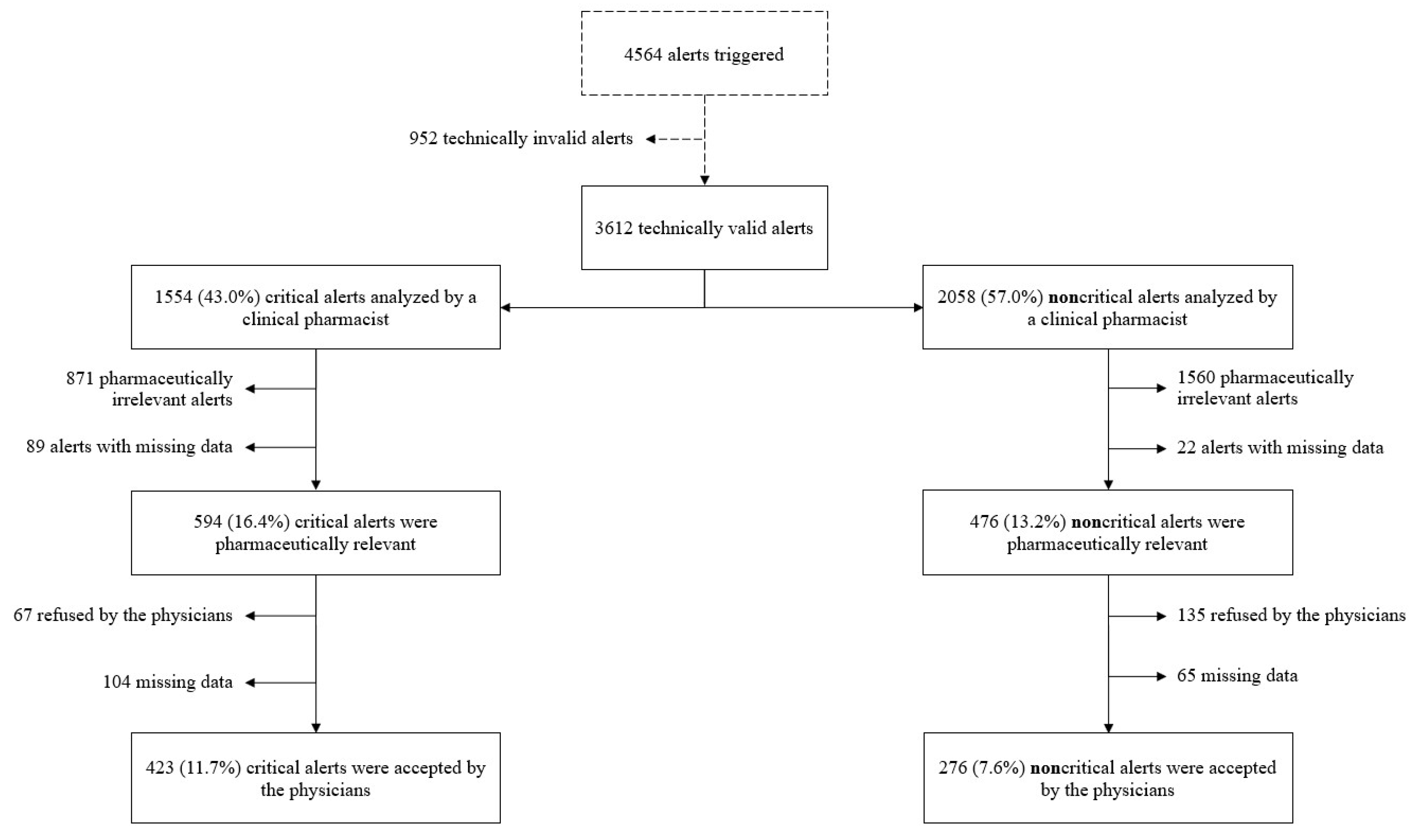
- The alert’s technical validity: an alert was deemed to be valid when criteria required to trigger the rule were met (administrative, laboratory and treatment-related data). If the terms of the rule were met, the alert was qualified as “technically valid”. Technically invalid alerts were alerts that did not meet exactly the criteria of the rule, due to data integration issues (long reception time, lack of data integration …). For example, it was alerts that detected at-risk situations in which medication was already suspended or discontinued.
- The alert’s pharmaceutical relevance: only a technically valid alert could prompt the clinical pharmacist to issue a PI. However, a PI was issued only if the clinical pharmacist considered that the prescription or change was relevant for medical care. If a PI was issued, the problem and the action suggested by the pharmacist were noted. The transmission channel for the PI, the type of problem and action suggested following an alert were based on the SFPC’s classification [22,23]. An alert prompting a PI is referred to hereafter as “pharmaceutically relevant”.
- Physician acceptance of a PI: a PI (a suggestion for treatment or monitoring by the pharmacist) could be accepted or not by the prescribing physician.
2.6. Data Sources and Extraction
2.7. Statistical Analysis
3. Results
3.1. Analysis of Critical vs. Noncritical Alerts
3.2. Characteristics of the PIs

3.3. Categories of Rules Triggered
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skjøt-Arkil, H.; Lundby, C.; Kjeldsen, L.J.; Skovgårds, D.M.; Almarsdottir, A.B.; Kjølhede, T.; Duedahl, T.H.; Pottegård, A.; Graabaek, T. Multifaceted Pharmacist-led Interventions in the Hospital Setting: A Systematic Review. Basic Clin. Pharmacol. Toxicol. 2018, 123, 363–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammenwerth, E.; Schnell-Inderst, P.; Machan, C.; Siebert, U. The effect of electronic prescribing on medication errors and adverse drug events: A systematic review. J. Am. Med. Inform. Assoc. 2008, 15, 585–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedouch, P.; Tessier, A.; Baudrant, M.; Labarere, J.; Foroni, L.; Calop, J.; Bosson, J.L.; Allenet, B. Computerized physician order entry system combined with on-ward pharmacist: Analysis of pharmacists’ interventions. J. Eval. Clin Pract. 2012, 18, 911–918. [Google Scholar] [CrossRef]
- Pontefract, S.K.; Coleman, J.J.; Vallance, H.K.; Hirsch, C.A.; Shah, S.; Marriott, J.F.; Redwood, S. The Impact of Computerised Physician Order Entry and Clinical Decision Support on Pharmacist-Physician Communication in the Hospital Setting: A Qualitative Study. PLoS ONE 2018, 13, e0207450. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6239308/ (accessed on 7 March 2023). [CrossRef] [PubMed] [Green Version]
- Robertson, J.; Walkom, E.; Pearson, S.-A.; Hains, I.; Williamsone, M.; Newby, D. The impact of pharmacy computerised clinical decision support on prescribing, clinical and patient outcomes: A systematic review of the literature. Int. J. Pharm. Pract. 2010, 18, 69–87. [Google Scholar] [CrossRef] [PubMed]
- Curtain, C.; Peterson, G.M. Review of computerized clinical decision support in community pharmacy. J. Clin. Pharm. Ther. 2014, 39, 343–348. [Google Scholar] [CrossRef]
- Jaspers, M.W.M.; Smeulers, M.; Vermeulen, H.; Peute, L.W. Effects of clinical decision-support systems on practitioner performance and patient outcomes: A synthesis of high-quality systematic review findings. J. Am. Med. Inform. Assoc. 2011, 18, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Schnipper, J.L.; Kirwin, J.L.; Cotugno, M.C.; Wahlstrom, S.A.; Brown, B.A.; Tarvin, E.; Kachalia, A.; Horng, M.; Roy, C.L.; McKean, S.C.; et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern. Med. 2006, 166, 565–571. [Google Scholar] [CrossRef]
- English, D.; Ankem, K.; English, K. Acceptance of clinical decision support surveillance technology in the clinical pharmacy. Inform. Health Soc. Care 2017, 42, 135–152. [Google Scholar] [CrossRef]
- Beuscart, J.-B.; Pelayo, S.; Robert, L.; Thevelin, S.; Marien, S.; Dalleur, O. Medication review and reconciliation in older adults. Eur. Geriatr. Med. 2021, 12, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Schmiedl, S.; Rottenkolber, M.; Szymanski, J.; Drewelow, B.; Siegmund, W.; Hippius, M.; Farker, K.; Guenther, I.R.; Hasford, J.; Thuermann, P.A.; et al. Preventable ADRs leading to hospitalization—Results of a long-term prospective safety study with 6,427 ADR cases focusing on elderly patients. Expert Opin. Drug Saf. 2018, 17, 125–137. [Google Scholar] [CrossRef]
- McDonnell, P.J.; Jacobs, M.R. Hospital admissions resulting from preventable adverse drug reactions. Ann. Pharmacother. 2002, 36, 1331–1336. [Google Scholar] [CrossRef]
- Bouvy, J.C.; De Bruin, M.L.; Koopmanschap, M.A. Epidemiology of Adverse Drug Reactions in Europe: A Review of Recent Observational Studies. Drug Saf. 2015, 38, 437–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, L.M. Comparative epidemiology of hospital-acquired adverse drug reactions in adults and children and their impact on cost and hospital stay—A systematic review. Eur. J. Clin. Pharmacol. 2013, 69, 1985–1996. [Google Scholar] [CrossRef] [PubMed]
- Calloway, S.; Akilo, H.A.; Bierman, K. Impact of a Clinical Decision Support System on Pharmacy Clinical Interventions, Documentation Efforts, and Costs. Hosp. Pharm. 2013, 48, 744–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, L.; Reese, T.; Nelson, S.D. A Narrative Review of Clinical Decision Support for Inpatient Clinical Pharmacists. Appl. Clin. Inform. 2021, 12, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Kane-Gill, S.L.; Achanta, A.; Kellum, J.A.; Handler, S.M. Clinical decision support for drug related events: Moving towards better prevention. World J. Crit. Care Med. 2016, 5, 204–211. [Google Scholar] [CrossRef]
- Ancker, J.S.; Edwards, A.; Nosal, S.; Hauser, D.; Mauer, E.; Kaushal, R.; With the HITEC Investigators. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med. Inform. Decis. Mak. 2017, 17, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, A.E. Averting Alert Fatigue to Prevent Adverse Drug Reactions. JAMA 2019, 322, 601. [Google Scholar] [CrossRef]
- Cuvelier, E.; Robert, L.; Musy, E.; Rousseliere, C.; Marcilly, R.; Gautier, S.; Odou, P.; Beuscart, J.B.; Décaudin, B. The clinical pharmacist’s role in enhancing the relevance of a clinical decision support system. Int. J. Med. Inf. 2021, 155, 104568. [Google Scholar] [CrossRef] [PubMed]
- Vo, H.T.; Charpiat, B.; Chanoine, S.; Juste, M.; Roubille, R.; Rose, F.X.; Conort, O.; Allenet, B.; Bedouch, P. CLEO: A multidimensional tool to assess clinical, economic and organisational impacts of pharmacists’ interventions. Eur. J. Hosp. Pharm. 2021, 28, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Allenet, B.; Bedouch, P.; Rose, F.X.; Escofier, L.; Roubille, R.; Charpiat, B.; Juste, M.; Conort, O. Validation of an instrument for the documentation of clinical pharmacists’ interventions. Pharm. World Sci. 2006, 28, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Charpiat, B.; Conort, O.; Juste, M.; Rose, F.X.; Roubille, R.; Bedouch, P.; Allenet, B. The French Society of Clinical Pharmacy ACT-IP© project: Ten years onward, results and prospects. Pharm. Hosp Clin. 2015, 50, e15–e24. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2017. Available online: https://www.R-project.org/ (accessed on 7 March 2023).
- Olakotan, O.; Mohd Yusof, M.; Ezat Wan Puteh, S. A Systematic Review on CDSS Alert Appropriateness. Stud. Health Technol. Inform. 2020, 906, 10. [Google Scholar]
- Chin, D.L.; Wilson, M.H.; Trask, A.S.; Johnson, V.T.; Neaves, B.I.; Gojova, A.; Hogarth, M.A.; Bang, H.; Romano, P.S. Repurposing Clinical Decision Support System Data to Measure Dosing Errors and Clinician-Level Quality of Care. J. Med. Syst. 2020, 44, 1–16. [Google Scholar] [CrossRef]
- Hussain, M.I.; Reynolds, T.L.; Zheng, K. Medication safety alert fatigue may be reduced via interaction design and clinical role tailoring: A systematic review. J. Am. Med. Inform. Assoc. 2019, 26, 1141–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranji, S.R.; Rennke, S.; Wachter, R.M. Computerised provider order entry combined with clinical decision support systems to improve medication safety: A narrative review. BMJ Qual. Saf. 2014, 23, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Segal, G.; Segev, A.; Brom, A.; Lifshitz, Y.; Wasserstrum, Y.; Zimlichman, E. Reducing drug prescription errors and adverse drug events by application of a probabilistic, machine-learning based clinical decision support system in an inpatient setting. J. Am. Med. Inform. Assoc. 2019, 26, 1560–1565. [Google Scholar] [CrossRef]
- Corny, J.; Rajkumar, A.; Martin, O.; Dode, X.; Lajonchère, J.P.; Billuart, O.; Bézie, Y.; Buronfosse, A. A machine learning–based clinical decision support system to identify prescriptions with a high risk of medication error. J. Am. Med. Inform. Assoc. JAMIA 2020, 27, 1688–1694. [Google Scholar] [CrossRef]
- Díaz, A.S.; de la Fuente, J.S.; Esteva, L.; Pardo, A.M.A.; Barrueco, N.; Esteban, C.; Rodríguez, I.E. Drug prescribing in patients with renal impairment optimized by a computer-based, semi-automated system. Int. J. Clin. Pharm. 2013, 35, 1170–1177. [Google Scholar] [CrossRef]
- Rommers, M.K.; Zwaveling, J.; Guchelaar, H.-J.; Teepe-Twiss, I.M. Evaluation of rule effectiveness and positive predictive value of clinical rules in a Dutch clinical decision support system in daily hospital pharmacy practice. Artif. Intell. Med. 2013, 59, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Lagreula, J.; Maes, F.; Wouters, D.; Quennery, S.; Dalleur, O. Optimizing pharmacists’ detection of prescribing errors: Comparison of on-ward and central pharmacy services. J. Clin. Pharm. Ther. 2021, 46, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Quintens, C.; De Rijdt, T.; Van Nieuwenhuyse, T.; Simoens, S.; Peetermans, W.E.; Van den Bosch, B.; Casteels, M.; Spriet, I. Development and implementation of “Check of Medication Appropriateness” (CMA): Advanced pharmacotherapy-related clinical rules to support medication surveillance. BMC Med. Inform. Decis. Mak. 2019, 19, 29. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Reason | Critical Alerts n = 871 | Noncritical Alerts n = 1560 |
|---|---|---|
| Poor performance by the CDSS, n (%) | 539 (61.9%) | 1004 (64.4%) |
| Pharmacist’s decision to monitor the patient, n (%) | 136 (15.6%) | 254 (16.3%) |
| Irrelevant alert for the ward in question, n (%) | 70 (8.0%) | 208 (13.3%) |
| Other, n (%) | 122 (14.0%) | 60 (3.8%) |
| Missing data, n (%) | 4 (0.5%) | 34 (2.2%) |
| Categories of Rule | All Alerts | Critical Alerts | Noncritical Alerts | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Tech. Valid | Pharm. Relevant n (%) * | PI Accepted n (%) ** | Tech. Valid | Pharm. Relevant n (%) * | PI Accepted n (%) ** | Tech. Valid | Pharm. Relevant n (%) * | PI Accepted n (%) ** | |
| Adverse drug reaction | 84 | 24 (28.6%) | 11 (45.8%) | 29 | 13 (44.8%) | 6 (46.2%) | 55 | 11 (20.0%) | 5 (45.5%) |
| Untreated indication | 74 | 20 (27.0%) | 11 (55.0%) | 32 | 9 (28.1%) | 5 (55.6%) | 42 | 11 (26.2%) | 6 (54.5%) |
| Drug interaction | 341 | 169 (49.6%) | 122 (72.2%) | 332 | 165 (49.7%) | 120 (72.7%) | 9 | 4 (44.4%) | 2 (50.0%) |
| Nonindicated drug | 149 | 46 (30.9%) | 27 (58.7%) | 123 | 33 (26.8%) | 19 (57.6%) | 26 | 13 (50.0%) | 8 (61.5%) |
| Monitoring | 181 | 37 (20.4%) | 27 (73.0%) | 0 | 0 | 0 | 181 | 37 (20.4%) | 27 (73.0%) |
| Noncompliance with guidelines/contraindication | 1474 | 449 (30.5%) | 270 (60.1%) | 554 | 227 (41.0%) | 166 (73.1%) | 920 | 222 (24.1%) | 104 (46.8%) |
| Underdosing | 128 | 23 (18.0%) | 11 (47.8%) | 128 | 23 (20.0%) | 11 (47.8%) | 0 | 0 | 0 |
| Overdosing | 1156 | 279 (24.1%) | 201 (72.0%) | 353 | 121 (34.3%) | 95 (78.5%) | 803 | 158 (19.7%) | 106 (67.1%) |
| Inappropriate administration route/mode | 25 | 23 (92.0%) | 19 (82.6%) | 3 | 3 (100.0%) | 1 (33.3%) | 22 | 20 (90.9%) | 18 (90.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robert, L.; Cuvelier, E.; Rousselière, C.; Gautier, S.; Odou, P.; Beuscart, J.-B.; Décaudin, B. Detection of Drug-Related Problems through a Clinical Decision Support System Used by a Clinical Pharmacy Team. Healthcare 2023, 11, 827. https://doi.org/10.3390/healthcare11060827
Robert L, Cuvelier E, Rousselière C, Gautier S, Odou P, Beuscart J-B, Décaudin B. Detection of Drug-Related Problems through a Clinical Decision Support System Used by a Clinical Pharmacy Team. Healthcare. 2023; 11(6):827. https://doi.org/10.3390/healthcare11060827
Chicago/Turabian StyleRobert, Laurine, Elodie Cuvelier, Chloé Rousselière, Sophie Gautier, Pascal Odou, Jean-Baptiste Beuscart, and Bertrand Décaudin. 2023. "Detection of Drug-Related Problems through a Clinical Decision Support System Used by a Clinical Pharmacy Team" Healthcare 11, no. 6: 827. https://doi.org/10.3390/healthcare11060827