
Long-Term Spasticity Management in Post-Stroke Patients: Issues and Possible Actions—A Systematic Review with an Italian Expert Opinion

 , , ,
, , ,  and
and
Abstract
:1. Introduction
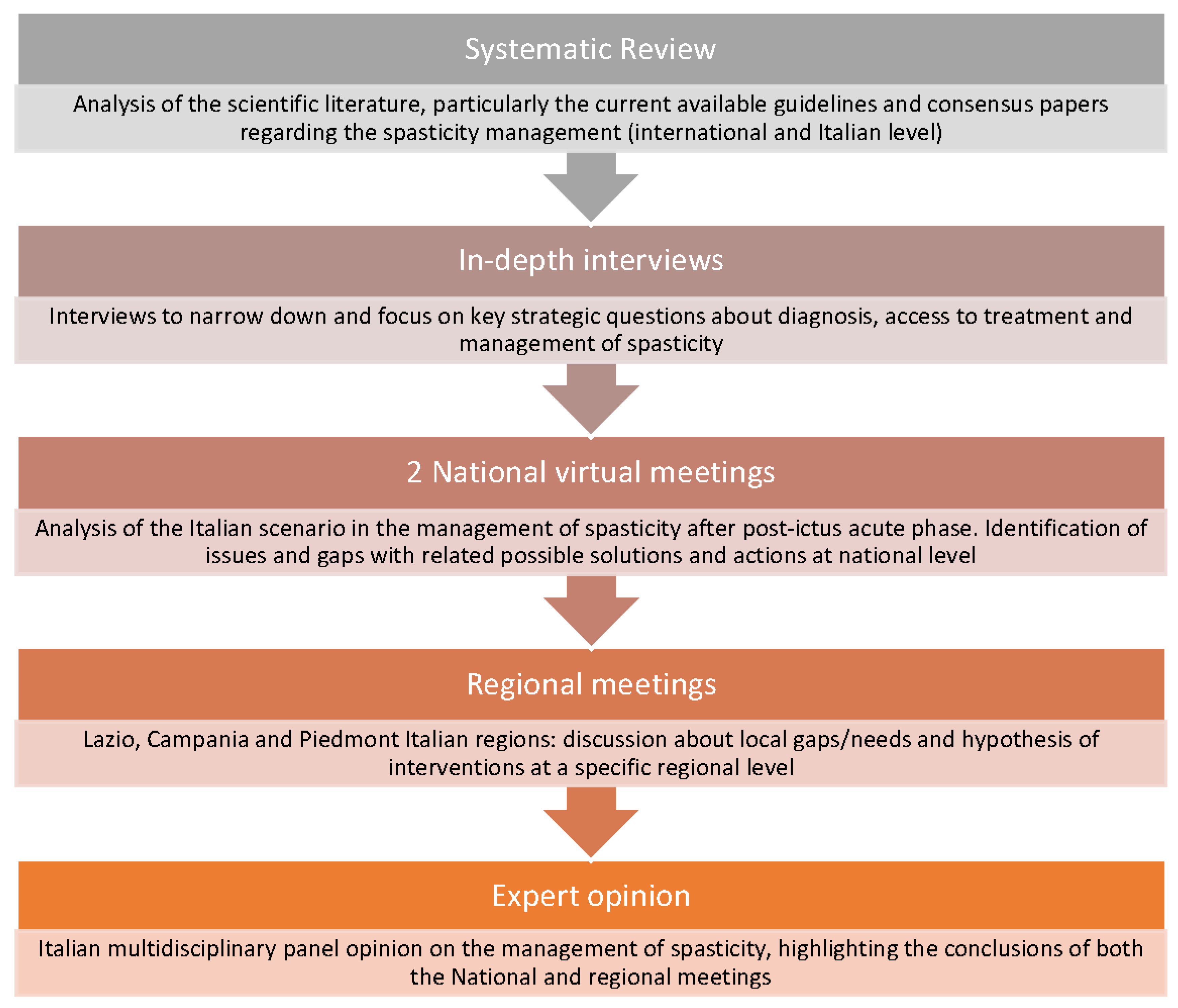
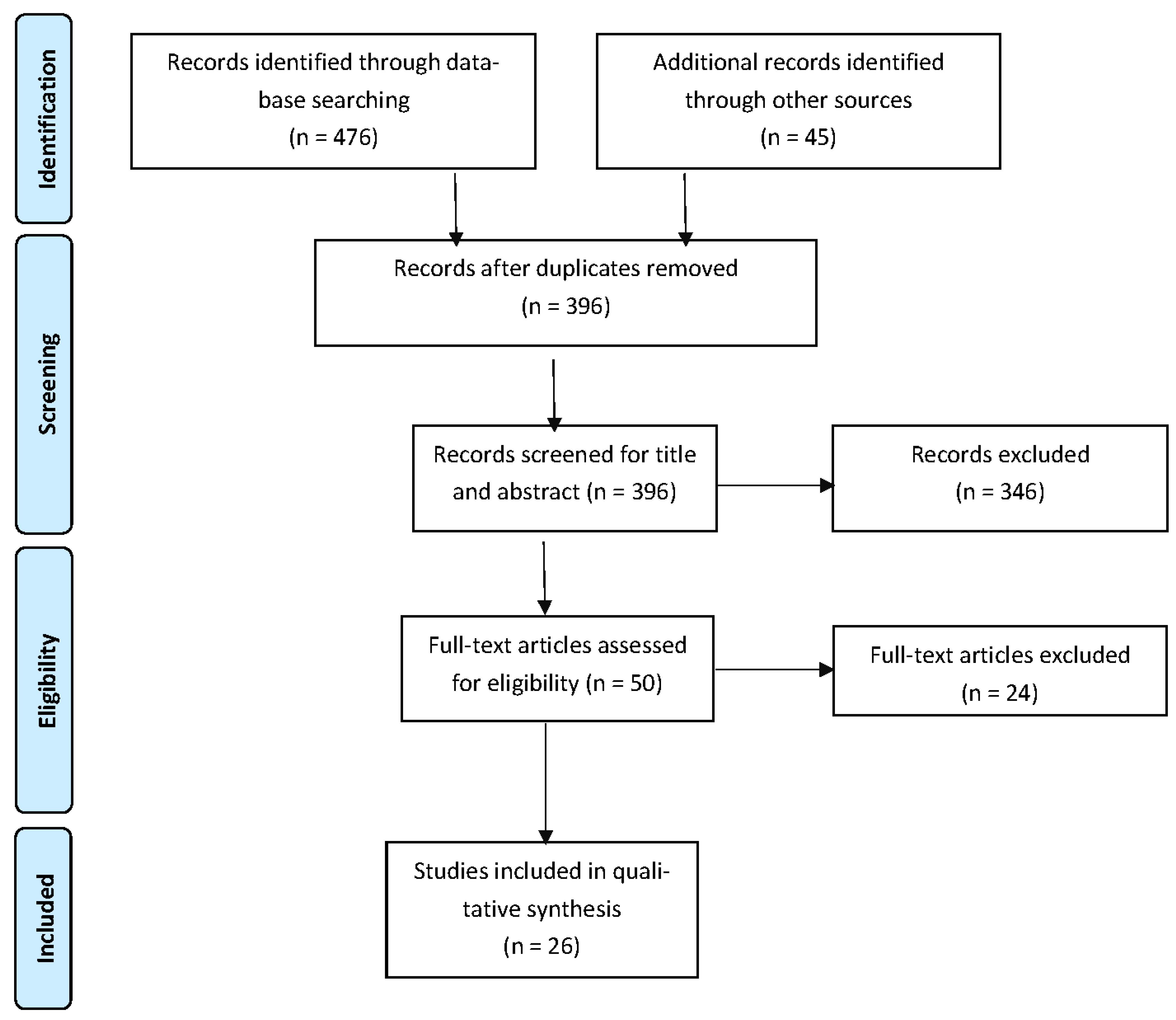
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Bavikatte, G.; Subramanian, G.; Ashford, S.; Allison, R.; Hicklin, D. Early Identification, Intervention and Management of Post-stroke Spasticity: Expert Consensus Recommendations. J. Cent. Nerv. Syst. Dis. 2021, 13, 11795735211036576. [Google Scholar] [CrossRef] [PubMed]
- Christofi, G.; Ashford, S.; Birns, J.; Dalton, C.; Duke, L.; Madsen, C.; Salam, S. Improving the Management of Post-Stroke Spasticity: Time for Action. J. Rehabil. Med. Clin. Commun. 2018, 1, 1000004. [Google Scholar] [CrossRef]
- Gupta, A.D.; Visvanathan, R.; Cameron, I.; Koblar, S.A.; Howell, S.; Wilson, D. Efficacy of botulinum toxin in modifying spasticity to improve walking and quality of life in post-stroke lower limb spasticity-a randomized double-blind placebo-controlled study. BMC Neurol. 2019, 19, 96. [Google Scholar]
- Dong, Y.; Wu, T.; Hu, X.; Wang, T. Efficacy and safety of botulinum toxin type A for upper limb spasticity after stroke or traumatic brain injury: A systematic review with meta-analysis and trial sequential analysis. Eur. J. Phys. Rehabil. Med. 2017, 53, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Nair, K.P.; Marsden, J. The management of spasticity in adults. BMJ 2014, 349, g4737. [Google Scholar] [CrossRef] [Green Version]
- Francisco, G.E.; Balbert, A.; Bavikatte, G.; Bensmail, D.; Carda, S.; Deltombe, T.; Draulans, N.; Escaldi, S.; Gross, R.; Jacinto, J.; et al. A practical guide to optimizing the benefits of post-stroke spasticity interventions with botulinum toxin A: An international group consensus. J. Rehabil. Med. 2021, 53, jrm00134. [Google Scholar] [CrossRef]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Physicians; British Society of Rehabilitation Medicine; The Chartered Society of Physiotherapy; Association of Chartered Physiotherapists in Neurology; the Royal College of Occupational Therapists. Spasticity in adults: Management using botulinum toxin. National Guidelines; RCP: London, UK, 2018. [Google Scholar]
- Cox, A.P.; Raluy-Callado, M.; Wang, M.; Bakheit, A.M.; Moore, A.P.; Dinet, J. Predictive analysis for identifying potentially undiagnosed post-stroke spasticity patients in United Kingdom. J. Biomed. Inform. 2016, 60, 328–333. [Google Scholar] [CrossRef]
- Wissel, J.; Olver, J.; Sunnerhagen, K.S. Navigating the poststroke continuum of care. J. Stroke Cerebrovasc. Dis. 2013, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Global Action Plan for the Prevention and Control of NCDs 2013–2020. Available online: https://www.who.int/publications/i/item/9789241506236 (accessed on 2 January 2023).
- Zeng, H.; Chen, J.; Guo, Y.; Tan, S. Prevalence and Risk Factors for Spasticity After Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 11, 616097. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.-L.; Hu, G.-C. Post-stroke spasticity: A review of epidemiology, pathophysiology, and treatments. Int. J. Gerontol. 2018, 12, 280–284. [Google Scholar] [CrossRef]
- Picelli, A.; Baricich, A.; Cisari, C.; Paolucci, S.; Smania, N.; Sandrini, G. The Italian real-life post-stroke spasticity survey: Unmet needs in the management of spasticity with botulinum toxin type A. Funct. Neurol. 2017, 32, 89–96. [Google Scholar] [CrossRef]
- Smania, N.; Colosimo, C.; Bentivoglio, A.R.; Sandrini, G.; Picelli, A. Use of botulinum toxin type A in the management of patients with neurological disorders: A national survey. Funct. Neurol. 2013, 28, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Baricich, A.; Wein, T.; Cinone, N.; Bertoni, M.; Picelli, A.; Chisari, C.; Molteni, F.; Santamato, A. BoNT-A for Post-Stroke Spasticity: Guidance on Unmet Clinical Needs from a Delphi Panel Approach. Toxins 2021, 13, 236. [Google Scholar] [CrossRef]
- Wein, T.; Esquenazi, A.; Jost, W.H.; Ward, A.B.; Pan, G.; Dimitrova, R. OnabotulinumtoxinA for the Treatment of Poststroke Distal Lower Limb Spasticity: A Randomized Trial. PMR 2018, 10, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Gracies, J.M.; Esquenazi, A.; Brashear, A.; Banach, M.; Kocer, S.; Jech, R.; Khatkova, S.; Benetin, J.; Vecchio, M.; McAllister, P.; et al. International AbobotulinumtoxinA Adult Lower Limb Spasticity Study Group. Efficacy and safety of abobotulinumtoxinA in spastic lower limb: Randomized trial and extension. Neurology 2017, 89, 2245–2253. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.C.; Chen, R.; Fu, C.; Chen, Y.; Wu, Q.; Chen, R.; Lin, X.; Luo, S. Efficacy and Safety of Botulinum Toxin Type A for Limb Spasticity after Stroke: A Meta-Analysis of Randomized Controlled Trials. Biomed. Res. Int. 2019, 2019, 8329306. [Google Scholar] [CrossRef] [Green Version]
- Ghroubi, S.; Alila, S.; Elleuch, W.; Ayed, H.B.; Mhiri, C.; Elleuch, M.H. Efficacy of botulinum toxin A for the treatment of hemiparesis in adults with chronic upper limb spasticity. Pan. Afr. Med. J. 2020, 35, 55. [Google Scholar] [CrossRef]
- Picelli, A.; Santamato, A.; Cosma, M.; Baricich, A.; Chisari, C.; Millevolte, M.; Prete, C.; Mazzù, I.; Girardi, P.; Smania, N. Early Botulinum Toxin Type A Injection for Post-Stroke Spasticity: A Longitudinal Cohort Study. Toxins 2021, 13, 374. [Google Scholar] [CrossRef] [PubMed]
- Magon, A.; Conte, G.; Arrigoni, C.; Dellafiore, F.; de Maria, M.; Pittella, F.; Rocco, G.; Stievano, A.; Ghizzardi, G.; Caruso, R. Development and Psychometric Validation of the Nursing Self-Efficacy Scale for Managing Cancer Treatment-Induced Cardiotoxicity: An Exploratory Mixed-Method Study. Semin. Oncol. Nurs. 2022, 151367, Advance online publication. [Google Scholar] [CrossRef]
- Mediratta, S.; Chari, A.; DOLPHIN-UK Collaborators. A standardised protocol for neuro-endoscopic lavage for post-haemorrhagic ventricular dilatation: A Delphi consensus approach. Child’s Nerv. Syst. Off. J. Int. Soc. Pediatr. Neurosurg. 2022, 38, 2181–2187. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence. Available online: https://www.cebm.net/wp-content/uploads/2014/06/CEBM-Levels-of-Evidence-2.1.pdf (accessed on 2 January 2023).
- Lazzaro, C.; Baricich, A.; Picelli, A.; Caglioni, P.M.; Ratti, M.; Santamato, A. AbobotulinumtoxinA and rehabilitation vs rehabilitation alone in post-stroke spasticity: A cost-utility analysis. J. Rehabil. Med. 2020, 52, jrm00016. [Google Scholar] [CrossRef]
- Rychlik, R.; Kreimendahl, F.; Schnur, N.; Lambert-Baumann, J.; Dressler, D. Quality of life and costs of spasticity treatment in German stroke patients. Health Econ. Rev. 2016, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Forsmark ARosengren, L.; Ertzgaard, P. Inequalities in pharmacologic treatment of spasticity in Sweden–health economic consequences of closing the treatment gap. Health Econ. Rev. 2020, 10, 4. [Google Scholar] [CrossRef] [Green Version]
- Sandrini, G.; Baricich, A.; Cisari, C.; Paolucci, S.; Smania, N.; Picelli, A. Management of spasticity with onabotulinumtoxinA: Practical guidance based on the Italian real-life post-stroke spasticity survey. Funct. Neurol. 2018, 33, 37–43. [Google Scholar] [CrossRef]
- Demetrios, M.; Khan, F.; Turner-Stokes, L.; Brand, C.; McSweeney, S. Multidisciplinary rehabilitation following botulinum toxin and other focal intramuscular treatment for post-stroke spasticity. Cochrane Database Syst. Rev. 2013, 6, CD009689. [Google Scholar] [CrossRef] [Green Version]
- Wissel, J.; Ri, S. Assessment, goal setting, and botulinum neurotoxin a therapy in the management of post-stroke spastic movement disorder: Updated perspectives on best practice. Expert Rev. Neurother. 2022, 22, 27–42. [Google Scholar] [CrossRef]
- Williams, G.; Singer, B.J.; Ashford, S.; Hoare, B.; Hastings-Ison, T.; Fheodoroff, K.; Berwick, S.; Sutherland, E.; Hill, B. A synthesis and appraisal of clinical practice guidelines, consensus statements and Cochrane systematic reviews for the management of focal spasticity in adults and children. Disabil. Rehabil. 2022, 44, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Cinone, N.; Santoro, L.; Spina, S.; Facciorusso, S.; Battaglia, M.; Baricich, A.; Marcogiuseppe, P.; Santamato, A. Reasons and Determinants of BoNT-A Treatment Discontinuation in Patients Living with Spasticity: A 10-Year Retrospective Analysis. Toxins 2022, 14, 675. [Google Scholar] [CrossRef] [PubMed]
- Raluy-Callado, M.; Cox, A.; MacLachlan, S.; Bakheit, A.M.; Moore, A.P.; Dinet, J.; Gabriel, S. A retrospective study to assess resource utilization and costs in patients with post-stroke spasticity in the United Kingdom. Curr. Med. Res. Opin. 2018, 34, 1317–1324. [Google Scholar] [CrossRef]
- Turner-Stokes, L.; Ashford, S.; Esquenazi, A.; Wissel, J.; Ward, A.B.; Francisco, G.; Lains, J.; Suputtitada, A.; Serrano, S.; Baguley, I.J.; et al. A comprehensive person-centered approach to adult spastic paresis: A consensus-based framework. Eur. J. Phys. Rehabil. Med. 2018, 54, 605–617. [Google Scholar] [CrossRef]
- Sunnerhagen, K.S.; Francisco, G.E. Enhancing patient-provider communication for long-term post-stroke spasticity management. Acta Neurol. Scand. 2013, 128, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Santamato, A.; Facciorusso, S.; Spina, S.; Cinone, N.; Avvantaggiato, C.; Santoro, L.; Ciritella, C.; Smania, N.; Picelli, A.; Gasperini, G.; et al. Discontinuation of botulinum neurotoxin type-A treatment during COVID-19 pandemic: An Italian survey in post stroke and traumatic brain injury patients living with spasticity. Eur. J. Phys. Rehabil. Med. 2021, 57, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Jacinto, J.; Varriale, P.; Pain, E.; Lysandropoulos, A.; Esquenazi, A. Patient Perspectives on the Therapeutic Profile of Botulinum Neurotoxin Type A in Spasticity. Front. Neurol. 2020, 11, 388. [Google Scholar] [CrossRef]
- Makino, K.; Tilden, D.; Guarnieri, C.; Mudge, M.; Baguley, I.J. Cost Effectiveness of Long-Term Incobotulinumtoxin-A Treatment in the Management of Post-stroke Spasticity of the Upper Limb from the Australian Payer Perspective. Pharm. –Open 2019, 3, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Fheodoroff, K.; Danchenko, N.; Whalen, J.; Balcaitiene, J.; Magalhães, B.; Szulc, E.; Zaffalon, A.; Burchakova, M.; Nechiporenko, D.; Robbins, S. Modelling Long-Term Outcomes and Risk of Death for Patients with Post-Stroke Spasticity Receiving Abobotulinumtoxina Treatment and Rehabilitation Therapy. J. Rehabil. Med. 2022, 54, jrm00303. [Google Scholar] [CrossRef]
- Lindsay, C.; Humphreys, I.; Phillips, C.; Pandyan, A. Estimating the cost consequence of the early use of botulinum toxin in post-stroke spasticity: Secondary analysis of a randomised controlled trial. Clin. Rehabil. 2023, 37, 373–380. [Google Scholar] [CrossRef]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Quality of Care and Outcomes Research; et al. Guidelines for adult stroke rehabilitation and recovery: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Hebert, D.; Lindsay, M.P.; McIntyre, A.; Kirton, A.; Rumney, P.G.; Bagg, S.; Bayley, M.; Dowlatshahi , D.; Dukelow, S.; Garnhum, M.; et al. Canadian stroke best practice recommendations: Stroke rehabilitation practice guidelines, update 2015. Int. J. Stroke 2016, 11, 459–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, L. Management of patients with stroke: Rehabilitation, prevention and management of complications, and discharge planning: A national clinical guideline. SIGN 2010, 118. Available online: https://www.sign.ac.uk/media/1056/sign118.pdf (accessed on 2 June 2022).
- Stroke Foundation of New Zealand; New Zealand Guidelines Group. Clinical Guidelines for Stroke Management 2010; Stroke Foundation of New Zealand: Wellington, FL, USA, 2010. [Google Scholar]
- Schnitzler, A.; Ruet, A.; Baron, S.; Buzzi, J.C.; Genet, F. Botulinum toxin A for treating spasticity in adults: Costly for French hospitals? Ann. Phys. Rehabil. Med. 2015, 58, 265–268. [Google Scholar] [CrossRef] [Green Version]
- Iosa, M.; Lupo, A.; Morone, G.; Baricich, A.; Picelli, A.; Panza, G.; Smania, N.; Cisari, C.; Sandrini, G.; Paolucci, S. Post Soft Care: Italian implementation of a post-stroke checklist software for primary care and identification of unmet needs in community-dwelling patients. Neurol. Sci. 2018, 39, 135–139. [Google Scholar] [CrossRef]
- Kim, K.T.; Chang, W.K.; Jung, Y.S.; Jee, S.; Sohn, M.K.; Ko, S.H.; Shin, Y.I.; Leigh, J.H.; Kim, W.S.; Paik, N.J. Unmet Needs for Rehabilitative Management in Common Health-Related Problems Negatively Impact the Quality of Life of Community-Dwelling Stroke Survivors. Front. Neurol. 2021, 12, 758536. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Key Questions to the Expert Panel |
|---|
| (1) To date, what are the main critical points and barriers that limit the correct diagnosis? |
| (2) To date, what are the main critical points and barriers to access to treatment? |
| (3) In the current scenario, how is the outpatient service of botulinum toxin injection remunerated? |
| (4) In the light of the analysis in the above questions, how do we ensure that patients with post-stroke spasticity are diagnosed and have access to continuous (chronic) appropriate treatment? |
| (5) In the current scenario, what characteristics an organizational network should have to efficiently taking care of patients suffering from post-stroke spasticity (roles and responsibilities). |
| (6) How can the actual performance of the take-over system be measured? |
| Selected Papers | Title | Type of Study | OCBM Scale | Objective | Main Findings |
|---|---|---|---|---|---|
| Christofi G et al., 2018 [4] | Improving the Management of Post-Stroke Spasticity: Time for Action. | Consensus report | Level 5 | To identify barriers to appropriate referral and treatment for patients with PSS and present solutions that address these in a pragmatic way. | Key barriers, throughout the patient journey prioritized by the panel, broadly related to lack of awareness and knowledge of spasticity, insufficient access to spasticity services, and a lack of standardized processes/pathways. |
| Bavikatte G et al., 2021 [3] | Early Identification, Intervention and Management of Post-stroke Spasticity: Expert Consensus Recommendations. | Consensus report | Level 5 | The proposed system, based on clinical evidence, expert consensus, and recent clinical guidelines, provides simple and straightforward criteria for management, multidisciplinary consultation, and referral to specialist spasticity services. | The Expert Consensus, through several rules, concludes that effective and timely intervention aims to increase functional abilities, improve personal care, and impact quality of life. |
| Picelli A et al., 2017 [16] | The Italian real-life post-stroke spasticity survey: unmet needs in the management of spasticity with botulinum toxin type A. | Survey | Level 5 | The main aim of this national survey was to provide an overview of some important issues concerning the use of BoNT-A to treat patients with PSS, and to highlight related unmet needs. | The management of PSS has several unmet needs that, were they addressed, might improve these patients’ clinical outcomes and quality of life. These needs concern patient follow-up, where a clearly defined pathway is lacking; furthermore, there is a need to use maximum doses per BoNT-A treatment and to ensure early intervention on PSS. |
| Francisco GE et al., 2021 [8] | A practical guide to optimizing the benefits of post-stroke spasticity interventions with botulinum toxin A: An international group consensus. | Consensus report | Level 5 | This consensus paper from the international group of experts does not replicate information published elsewhere, but instead aims to provide practical advice to help optimize the use of BoNT-A and maximize clinical outcomes. | The use of BoNT-A and innovative techniques have facilitated a more individualized approach to the treatment of PSS, which provides physicians with the opportunity to optimize outcomes and address multiple goals. |
| Picelli A et al., 2021 [23] | Early Botulinum Toxin Type A Injection for Post-Stroke Spasticity: A Longitudinal Cohort Study. | Multicenter, longitudinal, cohort study | Level 3 | The aim was of the study to determine whether the length of time between stroke onset and initial BoNT-A injection has an effect on outcomes after PSS treatment. | The study findings suggest that BoNT-A treatment for PSS should be initiated within 3 months after stroke onset in order to obtain a greater reduction in muscle tone at 1 and 3 months afterward. |
| Lazzaro C et al., 2020 [28] | Abobotulinum toxin A and rehabilitation vs. rehabilitation alone in post-stroke spasticity: A cost-utility analysis. | Cost-utility study | Level 3 | This is the first Italian economic evaluation aimed at investigating the costs and QALYs of rehabilitation + BoNT-A (rehab/aboBoNT-A) vs. rehabilitation (rehab) in Italy, via a 2-year, model-based cost-utility analysis (CUA) in post-stroke spasticity in Italy. | Rehabilitation combined with abobotulinum toxin A is a cost-effective healthcare program for treating patients with post-stroke spasticity in Italy, for both the Italian National Health Service and society. |
| Rychlik R et al., 2016 [29] | Quality of life and costs of spasticity treatment in German stroke patients. | Prospective, multicenter, non-interventional parallel-group study | Level 3 | To gather routine clinical practice data on post-stroke spasticity patients and their treatments in Germany. Efficacy, impact on quality of life and costs over a one-year treatment period were analyzed. | In this study, incobotulinum toxin A treatment demonstrated superior results in muscle tone reduction compared to conventional therapy and significantly improved functional impairment as well as quality of life. In the investigator’s view, the results underline the level A recommendation of national and international guidelines for the treatment of post-stroke spasticity with botulinum toxin. |
| Forsmark A et al., 2020 [30] | Inequalities in the pharmacologic treatment of spasticity in Sweden—health economic consequences of closing the treatment gap. | Comprehensive overview | Level 5 | Sweden lacks national treatment guidelines regarding the management of spasticity, leaving room for local variations in clinical practice: a marked variation in BoNT-A treatment of adult spasticity was observed. | The results from the current study show marked regional differences regarding BoNT-A spasticity treatment in Sweden, which also apply to other pharmacological treatments. The emerging explanation of the observed variation seems to be a lack of evidence-based central guidelines, training in spasticity care, and up-to date clinical expertise. |
| Sandrini G et al., 2018 [31] | Management of spasticity with onabotulinumtoxinA: practical guidance based on the Italian real-life post-stroke spasticity survey. | Survey | Level 5 | The aim of the paper is to provide practical guidance on the management of adult spasticity based on the unmet needs in the management of spasticity with botulinum toxin type A identified by the Italian Real-Life Post-Stroke Spasticity Survey. | All the members of the stroke care team should be aware of the early predictors of post-stroke spasticity; early predictors of spasticity should be evaluated within a few days of the onset of the stroke, and reported in the letter of discharge from the Stroke Unit. Stroke patients should be referred to spasticity services that have adequate facilities and multidisciplinary teams with the necessary training, competence, and expertise. |
| Demetrios M et al., 2013 [32] | Multidisciplinary rehabilitation following botulinum toxin and other focal intramuscular treatment for post-stroke spasticity. | Systematic review | Level 1 | To assess the effectiveness of multidisciplinary rehabilitation, following BoNT and other focal intramuscular treatments such as phenol. To explore what settings, types, and intensities of rehabilitation programs are effective. | There was ‘low level’ evidence for the effectiveness of outpatient MD rehabilitation in improving active function and impairments following BoNT for upper limb spasticity in adults with chronic stroke. Settings, modalities, and therapy approaches are unclear. |
| Wissel J et al., 2022 [33] | Assessment, goal setting, and botulinum neurotoxin a therapy in the management of post-stroke spastic movement disorder: updated perspectives on best practice. | Non-systematic review | Level 5 | The aim of the review is to discuss predictors, early identification, clinical assessments, goal setting, and management in a multi-professional team for early and chronic management of PS-SMD | BoNT-A to manage emerging and establishing post-stroke spastic movement disorder is recommended, safe, and dose-dependent effective local therapy. BoNT-A treatment improves activities of daily living and quality of life, especially when patient-centered goal setting in a multi-professional team and adjunctive treatment to BoNT-A is applied. |
| Williams G et al., 2022 [34] | A synthesis and appraisal of clinical practice guidelines, consensus statements and Cochrane systematic re-views for the management of focal spasticity in adults and children. | Systematic review | Level 2 | To review the existing clinical practice guidelines, consensus statements and Cochrane systematic reviews for the PSS and to generate a single synthesized guideline | PSS management should be provided by a multi-disciplinary team; therapy should be goal-directed; PSS goals should be developed in conjunction with the patient and family; in PSS treatment follow-up evaluations are of great importance. |
| Cinone N et al., 2022 [35] | Reasons and Determinants of BoNT-A Treatment Discontinuation in Patients Living with Spasticity: A 10-Year Retrospective Analysis. | Retrospective Study | Level 3 | to evaluate the reasons and determinants of BoNT-A discontinuation. | For stroke patients’ logistics reasons and clinical worsening were the most important causes of discontinuation. |
| Raluy-Callado M et al., 2018 [36] | A retrospective study to assess resource utilization and costs in patients with post-stroke spasticity in the United Kingdom. | Retrospective study | Level 3 | To assess the differences in healthcare resource utilization between patients who do and do not develop PSS in the UK. | Stroke patients who develop spasticity use twice as much economic resources as patients who do not develop it, particularly for hospital readmissions. |
| Turner-Stokes L et al., 2018 [37] | A comprehensive person-centered approach to adult spastic paresis: a consensus-based framework. | Consensus report | Level 5 | To develop a consensus-based framework towards “person-centered” medicine for the complex management of spastic paresis and to include an educative process that engages care providers and patients and encourages them to participate actively in the long-term management of spasticity. | Care focused on patient priorities. Definition of objectives, negotiation, and measurability of the same are priorities. The family’s ability to carry out self-rehabilitation must be considered and the cognitive, neuropsychological, and behavioral issues of rehabilitation must be taken into consideration. |
| Sunnerhagen KS et al., 2013 [38] | Enhancing patient-provider communication for long-term post-stroke spasticity management. | Non-systematic review | Level 5 | To discuss patient-provider communication and its role in PSS rehabilitation within the context of patient-centered health care. | Areas to be improved: involving family members; educating patients and family members on stroke and rehabilitation and establishing a common definition for long-term goals. Increased communication among physicians, patients, and payers may bridge some of the gaps and increase the effectiveness of PSS rehabilitation and management. |
| Santamato A et al., 2021 [39] | Discontinuation of botulinum neurotoxin type-A treatment during COVID-19 pandemic: an Italian survey in post stroke and traumatic brain injury patients living with spasticity. | Survey | Level 5 | To evaluate the impact of discontinuation of BoNT-A treatment on spasticity during the COVID-19 quarantine. | The discontinuation of BoNT-A treatment was associated with a worsening of perceived spasticity and associated loss of independence. |
| Jacinto J et al., 2020 [40] | Patient Perspectives on the Therapeutic Profile of Botulinum Neurotoxin Type A in Spasticity. | Survey | Level 5 | To evaluate patient perceptions of the impact of spasticity and the waning of BoNT-A therapeutic effects | Symptom re-emergence is common and has a significant impact on quality of life. Greater patient/clinician awareness of this therapeutic profile should lead to a better level of overall satisfaction with treatment, informed therapeutic discussions, and treatment schedule planning. |
| Makino K et al., 2019 [41] | Cost Effectiveness of Long-Term Incobotulinum toxin-A Treatment in the Management of Post-stroke Spasticity of the Upper Limb from the Australian Payer Perspective. | Retrospective study | Level 3 | Pharmacoeconomics study on BoNT-A treatment duration in Australia. | In Australia, BoNT-A treatment is restricted to four cycles of BoNT treatment irrespective of the subject’s response or clinical needs. This study demonstrated that in well-selected subjects more than four cycles can be cost-effective. |
| Fheodoroff K et al., 2022 [42] | Modelling Long-Term Outcomes and Risk of Death for Patients with Post-Stroke Spasticity Receiving Abobotulinum toxin A Treatment and Rehabilitation Therapy. | Non-systematic review | Level 5 | To model the long-term clinical and economic outcomes of post-stroke spasticity. | BoNT-A plus rehabilitation therapy led to a risk reduction of 8.8% for all-cause mortality, and an increase of 13% in life-years and 59% in quality-adjusted life-years compared with rehabilitation therapy alone. |
| Lindsay C et al., 2023 [43] | Estimating the cost consequence of the early use of botulinum toxin in post-stroke spasticity: Secondary analysis of a randomised controlled trial. | Randomized controlled trial | Level 2 | To evaluate the cost-consequence of an early BoNT-A treatment in the acute stroke unit. | An early spasticity treatment in stroke patients at risk of contractures with botulinum toxin leads to a significant reduction in contracture costs. |
| Guideline | Society/Association, Year | Main Recommendations/Statements |
|---|---|---|
| Royal College of Physicians, 2018 [10] | Royal College of Physicians, 2018 | The purpose of these guidelines is to provide clinicians with the knowledge and tools to use BoNT-A appropriately in focal spasticity. The principles for successful intervention are:
|
| Winstein CJ, et al., 2016 [44] | American Heart Association (AHA), American Stroke Association (ASA), 2016 | Botulinum toxin injection can be useful to reduce severe hypertonicity in hemiplegic shoulder muscles. Targeted injection of botulinum toxin into localized upper limb muscles is recommended to reduce spasticity, improve passive or active range of motion, and improve dressing, hygiene, and limb positioning. Targeted injection of botulinum toxin into lower limb muscles is recommended to reduce spasticity that interferes with gait function. |
| Hebert D, et al., 2015. [45] | Canadian stroke best practice recommendations | Chemodenervation using botulinum toxin can be used to reduce spasticity, increase range of motion, and improve gait, for patients with focal and/or symptomatically distressing spasticity |
| Smith L. 2010 [46] | SIGN Guidelines, Scotland | A Clostridium botulinum toxin type A may be considered for use to relieve spasticity following stroke where it is causing pain or interfering with physical function and the ability to maintain hand hygiene; injections may need to be repeated every three to four months and should be discontinued if lack of efficacy; botulinum toxin should only be used by those with appropriate training and care is required with the administration as the unit dosage of botulinum toxin differs between manufacturers. |
| Stroke Foundation of New Zealand and New Zealand Guidelines Group. 2010 [47] | Stroke Foundation of New Zealand and New Zealand Guidelines Group | Botulinum toxin A should be trialed in conjunction with rehabilitation therapy which includes setting clear goals. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morone, G.; Baricich, A.; Paolucci, S.; Bentivoglio, A.R.; De Blasiis, P.; Carlucci, M.; Violi, F.; Levato, G.; Pani, M.; Carpagnano, L.F.; et al. Long-Term Spasticity Management in Post-Stroke Patients: Issues and Possible Actions—A Systematic Review with an Italian Expert Opinion. Healthcare 2023, 11, 783. https://doi.org/10.3390/healthcare11060783
Morone G, Baricich A, Paolucci S, Bentivoglio AR, De Blasiis P, Carlucci M, Violi F, Levato G, Pani M, Carpagnano LF, et al. Long-Term Spasticity Management in Post-Stroke Patients: Issues and Possible Actions—A Systematic Review with an Italian Expert Opinion. Healthcare. 2023; 11(6):783. https://doi.org/10.3390/healthcare11060783
Chicago/Turabian StyleMorone, Giovanni, Alessio Baricich, Stefano Paolucci, Anna Rita Bentivoglio, Paolo De Blasiis, Matilde Carlucci, Francesco Violi, Gabriella Levato, Marcello Pani, Lucia Federica Carpagnano, and et al. 2023. "Long-Term Spasticity Management in Post-Stroke Patients: Issues and Possible Actions—A Systematic Review with an Italian Expert Opinion" Healthcare 11, no. 6: 783. https://doi.org/10.3390/healthcare11060783