Long-Term Evolution of Activities of Daily Life (ADLs) in Critically Ill COVID-19 Patients, a Case Series

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Performance Evaluation
2.2. Outcomes
2.3. Statistical Analysis
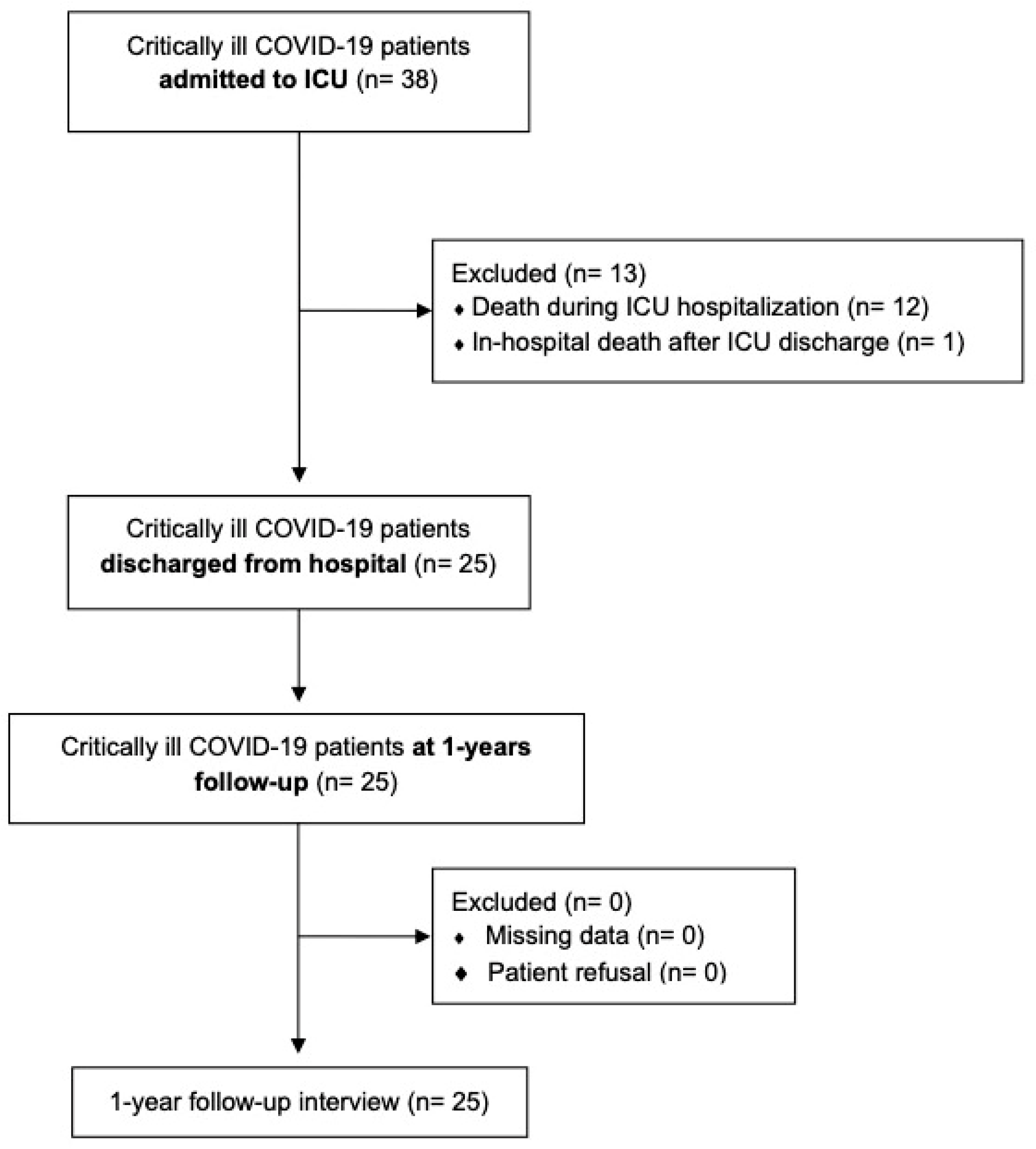
3. Results
3.1. Primary Outcome
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phelan, A.L.; Katz, R.; Gostin, L.O. The Novel Coronavirus Originating in Wuhan, China: Challenges for Global Health Governance. JAMA J. Am. Med. Assoc. 2020, 323, 709–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy: Early Experience and Forecast during an Emergency Response. JAMA J. Am. Med. Assoc. 2020, 323, 1545–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns Hopkins Coronavirus Resource Center Cumulative Cases-Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/data/cumulative-cases (accessed on 1 June 2022).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA J. Am. Med. Assoc. 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.R.E.; Hastie, J.; et al. Epidemiology, Clinical Course, and Outcomes of Critically Ill Adults with COVID-19 in New York City: A Prospective Cohort Study. Available online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31189-2/fulltext (accessed on 1 June 2021).
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Aranda, J.; Oriol, I.; Martín, M.; Feria, L.; Vázquez, N.; Rhyman, N.; Vall-Llosera, E.; Pallarés, N.; Coloma, A.; Pestaña, M.; et al. Long-term impact of COVID-19 associated acute respiratory distress syndrome. J. Infect. 2021, 83, 581–588. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Del Rio, C.; Collins, L.F.; Malani, P. Long-term Health Consequences of COVID-19. JAMA J. Am. Med. Assoc. 2020, 324, 1723–1724. [Google Scholar] [CrossRef]
- Frija-Masson, J.; Debray, M.P.; Boussouar, S.; Khalil, A.; Bancal, C.; Motiejunaite, J.; Galarza-Jimenez, M.A.; Benzaquen, H.; Penaud, D.; Laveneziana, P.; et al. Residual ground glass opacities three months after COVID-19 pneumonia correlate to alteration of respiratory function: The post COVID M3 study. Respir. Med. 2021, 184, 106435. [Google Scholar] [CrossRef] [PubMed]
- Qin, W.; Chen, S.; Zhang, Y.; Dong, F.; Zhang, Z.; Hu, B.; Zhu, Z.; Li, F.; Wang, X.; Wang, Y.; et al. Diffusion capacity abnormalities for carbon monoxide in patients with COVID-19 at 3-month follow-up. Eur. Respir. J. 2021, 58, 2003677. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.-m.; Shang, Y.-m.; Song, W.-b.; Li, Q.-q.; Xie, H.; Xu, Q.-f.; Jia, J.-l.; Li, L.-m.; Mao, H.-l.; Zhou, X.-m.; et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine 2020, 25, 100463. [Google Scholar] [CrossRef] [PubMed]
- Boutou, A.K.; Georgopoulou, A.; Pitsiou, G.; Stanopoulos, I.; Kontakiotis, T.; Kioumis, I. Changes in the respiratory function of COVID-19 survivors during follow-up: A novel respiratory disorder on the rise? Int. J. Clin. Pract. 2021, 75, e14301. [Google Scholar] [CrossRef] [PubMed]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Alsina-Restoy, X.; Solis-Navarro, L.; Burgos, F.; Puppo, H.; Vilaró, J. Respiratory function in patients post-infection by COVID-19: A systematic review and meta-analysis. Pulmonology 2021, 27, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Baricich, A.; Patrucco, F.; Zeppegno, P.; Gramaglia, C.; Balbo, P.E.; Carriero, A.; Amico, C.S.; Avanzi, G.C.; Barini, M.; et al. Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19. Sci. Rep. 2021, 11, 22666. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir. Med. 2021, 9, 747–754. [Google Scholar] [CrossRef]
- Steinbeis, F.; Thibeault, C.; Doellinger, F.; Ring, R.M.; Mittermaier, M.; Ruwwe-Glösenkamp, C.; Alius, F.; Knape, P.; Meyer, H.J.; Lippert, L.J.; et al. Severity of respiratory failure and computed chest tomography in acute COVID-19 correlates with pulmonary function and respiratory symptoms after infection with SARS-CoV-2: An observational longitudinal study over 12 months. Respir. Med. 2022, 191, 106709. [Google Scholar] [CrossRef]
- Van Zeller, C.; Anwar, A.; Ramos-Bascon, N.; Barnes, N.; Madden, B. Pulmonary function, computerized tomography features and six-minute walk test at three months in severe COVID-19 patients treated with intravenous pulsed methylprednisolone: A preliminary report. Monaldi Arch. Chest Dis. 2021, 91, e1811. [Google Scholar] [CrossRef]
- González, J.; Benítez, I.D.; Carmona, P.; Santisteve, S.; Monge, A.; Moncusí-Moix, A.; Gort-Paniello, C.; Pinilla, L.; Carratalá, A.; Zuil, M.; et al. Pulmonary Function and Radiologic Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort. Chest 2021, 160, 187–198. [Google Scholar] [CrossRef]
- Hazarika, A.; Mahajan, V.; Kajal, K.; Ray, A.; Singla, K.; Sehgal, I.S.; Bhalla, A.; Singh, S.M.; Naik, N.B.; Kaloria, N.; et al. Pulmonary Function, Mental and Physical Health in Recovered COVID-19 Patients Requiring Invasive Versus Non-invasive Oxygen Therapy: A Prospective Follow-Up Study Post-ICU Discharge. Cureus 2021, 13, e17756. [Google Scholar] [CrossRef]
- Compagnone, N.; Palumbo, D.; Cremona, G.; Vitali, G.; De Lorenzo, R.; Calvi, M.R.; Del Prete, A.; Baiardo Redaelli, M.; Calamarà, S.; Belletti, A.; et al. Residual lung damage following ARDS in COVID-19 ICU survivors. Acta Anaesthesiol. Scand. 2022, 66, 223–231. [Google Scholar] [CrossRef] [PubMed]
- McGroder, C.F.; Zhang, D.; Choudhury, M.A.; Salvatore, M.M.; D’Souza, B.M.; Hoffman, E.A.; Wei, Y.; Baldwin, M.R.; Garcia, C.K. Pulmonary fibrosis 4 months after COVID-19 is associated with severity of illness and blood leucocyte telomere length. Thorax 2021, 76, 1242–1245. [Google Scholar] [CrossRef] [PubMed]
- Herridge, M.S.; Cheung, A.M.; Tansey, C.M.; Matte-Martyn, A.; Diaz-Granados, N.; Al-Saidi, F.; Cooper, A.B.; Guest, C.B.; Mazer, C.D.; Mehta, S.; et al. One-Year Outcomes in Survivors of the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2003, 348, 683–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceravolo, M.G.; De Sire, A.; Andrenelli, E.; Negrini, F.; Negrini, S. Systematic rapid “living” review on rehabilitation needs due to COVID-19: Update to March 31st, 2020. Eur. J. Phys. Rehabil. Med. 2020, 56, 347–353. [Google Scholar] [CrossRef]
- LI, J. Rehabilitation management of patients with COVID-19: Lessons learned from the first experience in China. Eur. J. Phys. Rehabil. Med. 2020, 56, 335–338. [Google Scholar] [CrossRef]
- Lew, H.L.; Lew, H.L.; Oh-Park, M.; Oh-Park, M.; Cifu, D.X.; Cifu, D.X.; Cifu, D.X. The War on COVID-19 Pandemic: Role of Rehabilitation Professionals and Hospitals. Am. J. Phys. Med. Rehabil. 2020, 99, 571–572. [Google Scholar] [CrossRef]
- Ahmed, H.; Patel, K.; Greenwood, D.C.; Halpin, S.; Lewthwaite, P.; Salawu, A.; Eyre, L.; Breen, A.; O’Connor, R.; Jones, A.; et al. Long-term clinical outcomes in survivors of severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) coronavirus outbreaks after hospitalisation or ICU admission: A systematic review and meta-analysis. J. Rehabil. Med. 2020, 52, 1–11. [Google Scholar] [CrossRef]
- Quah, P.; Li, A.; Phua, J. Mortality rates of patients with COVID-19 in the intensive care unit: A systematic review of the emerging literature. Crit. Care 2020, 24, 285. [Google Scholar] [CrossRef]
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Decreasing mortality rates in ICU during the COVID-19 pandemic. Anaesthesia 2021, 76, 10. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected: Interim Guidance 28 January 2020; WHO: Geneva, Switzerland, 2020.
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Sinoff, G.; Ore, L. The Barthel activities of daily living index: Self-reporting versus actual performance in the old-old (≤ 75 years). J. Am. Geriatr. Soc. 1997, 45, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Galeoto, G.; Lauta, A.; Palumbo, A.; Sf, C.; Mollica, R.; Santilli, V.; Sacchetti, M.; Galeoto, G. International Journal of Neurology and Neurotherapy The Barthel Index: Italian Translation, Adaptation and Validation. Int. Libr. Cit. Int. J. Neurol. Neurother. 2015, 2, 2378–3001. [Google Scholar] [CrossRef]
- Mor, V.; Laliberte, L.; Morris, J.N.; Wiemann, M. The Karnofsky performance status scale: An examination of its reliability and validity in a research setting. Cancer 1984, 53, 2002–2007. [Google Scholar] [CrossRef] [PubMed]
- Schag, C.C.; Heinrich, R.L.; Ganz, P.A. Karnofsky performance status revisited: Reliability, validity, and guidelines. J. Clin. Oncol. 1984, 2, 187–193. [Google Scholar] [CrossRef]
- Parry, I. Physical Rehabilitation. In Burn Care for General Surgeons and General Practitioners; Springer International Publishing: Cham, Switzerland, 2016; pp. 137–150. ISBN 9783319291611. [Google Scholar]
- Gill, T.M. Assessment of function and disability in longitudinal studies. J. Am. Geriatr. Soc. 2010, 58, 783–787. [Google Scholar] [CrossRef]
- Yates, J.W.; Chalmer, B.; McKegney, F.P. Evaluation of patients with advanced cancer using the karnofsky performance status. Cancer 1980, 45, 2220–2224. [Google Scholar] [CrossRef]
- Friendlander, A.H.; Ettinger, R.L. Editorial: Karnofsky performance status scale. Spec. Care Dent. 2009, 29, 147–148. [Google Scholar] [CrossRef]
- Nicholson, C.; Davies, J.M.; George, R.; Smith, B.; Pace, V.; Harris, L.; Ross, J.; Noble, J.; Hansford, P.; Murtagh, F.E.M. What are the main palliative care symptoms and concerns of older people with multimorbidity?-A comparative cross-sectional study using routinely collected phase of illness, Australia-modified karnofsky performance status and integrated palliative care out. Ann. Cardiothorac. Surg. 2018, 7, S164–S175. [Google Scholar] [CrossRef]
- Tandon, P.; Reddy, K.R.; O’Leary, J.G.; Garcia-Tsao, G.; Abraldes, J.G.; Wong, F.; Biggins, S.W.; Maliakkal, B.; Fallon, M.B.; Subramanian, R.M.; et al. A Karnofsky performance status–based score predicts death after hospital discharge in patients with cirrhosis. Hepatology 2017, 65, 217–224. [Google Scholar] [CrossRef]
- De Haan, R.; Aaronson, N.; Limburg, M.; Langton Hewer, R.; Van Crevel, H. Measuring quality of life in stroke. Stroke 1993, 24, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Fortini, A.; Torrigiani, A.; Sbaragli, S.; Lo Forte, A.; Crociani, A.; Cecchini, P.; Innocenti Bruni, G.; Faraone, A. COVID-19: Persistence of symptoms and lung alterations after 3–6 months from hospital discharge. Infect 2021, 49, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Faverio, P.; Luppi, F.; Rebora, P.; D’Andrea, G.; Stainer, A.; Busnelli, S.; Catalano, M.; Modafferi, G.; Franco, G.; Monzani, A.; et al. One-year pulmonary impairment after severe COVID-19: A prospective, multicenter follow-up study. BioMed Central Ltd. 2022, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of Antibody Immunity to SARS-CoV-2. Available online: https://pubmed.ncbi.nlm.nih.gov/33461210/ (accessed on 1 June 2022).
- Carmo, A.; Pereira-Vaz, J.; Mota, V.; Mendes, A.; Morais, C.; da Silva, A.C.; Camilo, E.; Pinto, C.S.; Cunha, E.; Pereira, J.; et al. Clearance and Persistence of SARS-CoV-2 RNA in Patients with COVID-19. Available online: https://pubmed.ncbi.nlm.nih.gov/32484958/ (accessed on 1 June 2022).
- Kandetu, T.B.; Dziuban, E.J.; Sikuvi, K.; Beard, R.S.; Nghihepa, R.; van Rooyen, G.; Shiningavamwe, A.; Katjitae, I. Persistence of Positive RT-PCR Results for over 70 Days in Two Travelers with COVID-19. Available online: https://pubmed.ncbi.nlm.nih.gov/33208199/ (accessed on 1 June 2022).
- Vibholm, L.K.; Nielsen, S.S.; Pahus, M.H.; Frattari, G.S.; Olesen, R.; Andersen, R.; Monrad, I.; Andersen, A.H.; Thomsen, M.M.; Konrad, C.V.; et al. SARS-CoV-2 Persistence Is Associated with Antigen-Specific CD8 T-Cell Responses. Available online: https://pubmed.ncbi.nlm.nih.gov/33530000/ (accessed on 1 June 2022).
- Wang, X.; Huang, K.; Jiang, H.; Hua, L.; Yu, W.; Ding, D.; Wang, K.; Li, X.; Zou, Z.; Jin, M.; et al. Long-Term Existence of SARS-CoV-2 in COVID-19 Patients: Host Immunity, Viral Virulence, and Transmissibility. Virol. Sin. 2020, 35, 793–802. [Google Scholar] [CrossRef]
- Hirotsu, Y.; Maejima, M.; Shibusawa, M.; Amemiya, K.; Nagakubo, Y.; Hosaka, K.; Sueki, H.; Hayakawa, M.; Mochizuki, H.; Tsutsui, T.; et al. Analysis of a Persistent Viral Shedding Patient Infected with SARS-CoV-2 by RT-qPCR, FilmArray Respiratory Panel v2.1, and Antigen Detection. Available online: https://pubmed.ncbi.nlm.nih.gov/33183963/ (accessed on 1 June 2022).
- Wu, Y.; Guo, C.; Tang, L.; Hong, Z.; Zhou, J.; Dong, X.; Yin, H.; Xiao, Q.; Tang, Y.; Qu, X.; et al. Prolonged Presence of SARS-CoV-2 Viral RNA in Faecal Samples. Available online: https://pubmed.ncbi.nlm.nih.gov/32199469/ (accessed on 1 June 2022).
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.Y.; Huang, C.C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients–An MRI-based 3-month Follow-up Study: A brief title: Cerebral Changes in COVID-19. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The Emerging Spectrum of COVID-19 Neurology: Clinical, Radiological and Laboratory Findings. Available online: https://pubmed.ncbi.nlm.nih.gov/32637987/ (accessed on 1 June 2022).
- Rajpal, S.; Tong, M.S.; Borchers, J.; Zareba, K.M.; Obarski, T.P.; Simonetti, O.P.; Daniels, C.J. Cardiovascular Magnetic Resonance Findings in Competitive Athletes Recovering from COVID-19 Infection. Available online: https://pubmed.ncbi.nlm.nih.gov/32915194/ (accessed on 12 June 2021).
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered from Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-COVID Syndrome in Individuals Admitted to Hospital with COVID-19: Retrospective Cohort Study. Available online: https://www.bmj.com/content/372/bmj.n693 (accessed on 1 June 2022).
- Eberst, G.; Claudé, F.; Laurent, L.; Meurisse, A.; Roux-Claudé, P.; Barnig, C.; Vernerey, D.; Paget-Bailly, S.; Bouiller, K.; Chirouze, C.; et al. Result of One-Year, Prospective Follow-Up of Intensive Care Unit Survivors after SARS-CoV-2 Pneumonia. Available online: https://annalsofintensivecare.springeropen.com/articles/10.1186/s13613-022-00997-8 (accessed on 1 June 2022).
- Marando, M.; Fusi-Schmidhauser, T.; Tamburello, A.; Grazioli Gauthier, L.; Rigamonti, E.; Argentieri, G.; Puligheddu, C.; Pagnamenta, A.; Valenti, A.; Pons, M.; et al. 1-year radiological, functional and quality-of-life outcomes in patients with SARS-CoV-2 pneumonia-A prospective observational study. npj Prim. Care Respir. Med. 2022, 32, 8. [Google Scholar] [CrossRef]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Tansey, C.M.; Louie, M.; Loeb, M.; Gold, W.L.; Muller, M.P.; De Jager, J.A.; Cameron, J.I.; Tomlinson, G.; Mazzulli, T.; Walmsley, S.L.; et al. One-year outcomes and health care utilization in survivors of severe acute respiratory syndrome. Arch. Intern. Med. 2007, 167, 1312–1320. [Google Scholar] [CrossRef] [Green Version]
- Herridge, M.S.; Tansey, C.M.; Matté, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional Disability 5 Years after Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [Green Version]
- Rawal, G.; Yadav, S.; Kumar, R. Post-intensive care syndrome: An overview. J. Transl. Intern. Med. 2017, 5, 90–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Needham, D.M.; Davidson, J.; Cohen, H.; Hopkins, R.O.; Weinert, C.; Wunsch, H.; Zawistowski, C.; Bemis-Dougherty, A.; Berney, S.C.; Bienvenu, O.J.; et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care Med. 2012, 40, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Vanhorebeek, I.; Latronico, N.; Van den Berghe, G. ICU-acquired weakness. Intensive Care Med. 2020, 46, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Needham, D.M.; Wozniak, A.W.; Hough, C.L.; Morris, P.E.; Dinglas, V.D.; Jackson, J.C.; Mendez-Tellez, P.A.; Shanholtz, C.; Ely, E.W.; Colantuoni, E.; et al. Risk factors for physical impairment after acute lung injury in a national, multicenter study. Am. J. Respir. Crit. Care Med. 2014, 189, 1214–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, E.; Dowdy, D.W.; Colantuoni, E.; Mendez-Tellez, P.A.; Sevransky, J.E.; Shanholtz, C.; Himmelfarb, C.R.D.; Desai, S.V.; Ciesla, N.; Herridge, M.S.; et al. Physical complications in acute lung injury survivors: A two-year longitudinal prospective study. Crit. Care Med. 2014, 42, 849–859. [Google Scholar] [CrossRef] [Green Version]
- Ceruti, S.; Glotta, A.; Galli, A.; Biggiogero, M.; Bona, G.; Mauri, R.; Saporito, A.; Capdevila, X. Dysphagic disorder in a cohort of COVID-19 patients: Evaluation and evolution. Ann. Med. Surg. 2021, 69, 102837. [Google Scholar] [CrossRef]
- Biehl, M.; Kashyap, R.; Ahmed, A.H.; Reriani, M.K.; Ofoma, U.R.; Wilson, G.A.; Li, G.; Malinchoc, M.; Sloan, J.A.; Gajic, O. Six-month quality-of-life and functional status of acute respiratory distress syndrome survivors compared to patients at risk: A population-based study. Crit. Care 2015, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Shinar, D.; Gross, C.R.; Bronstein, K.S.; Licata-Gehr, E.E.; Eden, D.T.; Cabrera, A.R.; Fishman, I.G.; Roth, A.A.; Barwick, J.A.; Kunitz, S.C. Reliability of the Activities of Daily Living Scale and Its Use in Telephone Interview. Available online: https://pubmed.ncbi.nlm.nih.gov/3662782/ (accessed on 1 June 2022).
- Moore, K.; Merritt, B.; Doble, S.E. ADL skill profiles across three psychiatric diagnoses. Scand. J. Occup. Ther. 2010, 17, 77–85. [Google Scholar] [CrossRef]
- Nielsen, K.T.; Guidetti, S.; von Bülow, C.; Klokker, L.; Wæhrens, E.E. Feasibility of ABLE 1.0—A program aiming at enhancing the ability to perform activities of daily living in persons with chronic conditions. Pilot Feasibility Stud. 2021, 7, 52. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unit | Values | |
|---|---|---|
| Demographics data | ||
| Age | yrs | 59 ± 12 (29–76) |
| Male sex | n (%) | 21 (84%) |
| BMI | Kg/m2 | 29 ± 5 (20.1–40.1) |
| HTA | n (%) | 11 (44%) |
| DM | n (%) | 8 (32%) |
| OSAS | n (%) | 3 (12%) |
| COPD | n (%) | 1 (4%) |
| Pulmonary embolism | n (%) | 1 (4%) |
| ICU Data | ||
| SAPS II (first 24 h in ICU) | 39 ± 15 (13–70) | |
| SOFA * | 6 ± 2 (2–11) | |
| NEMS | 33 ± 9 (18–42) | |
| Temperature * | °C | 37.2 ± 0.9 (35.9–39.0) |
| Systolic arterial blood pressure * | mmHg | 133 ± 21 (100–180) |
| Diastolic arterial blood pressure * | mmHg | 70 ± 16 (50–110) |
| Heart rate * | bpm | 91 ± 25 (55–160) |
| Oro-tracheal intubation | n (%) | 20 (80%) |
| Tracheostomy | n (%) | 4 (16%) |
| CRRT | n (%) | 4 (16%) |
| Ventilation-associated pneumonia | n (%) | 4 (16%) |
| Other ICU infections | n (%) | 5 (20%) |
| ICU LOS | days | 12 ± 8 (2–41) |
| MV days | days | 11.8 ± 9 (0–41) |
| Laboratory Data | ||
| White cells * | G/L | 8.2 ± 3.5 (3.5–14.9) |
| Lymphocytes * | G/L | 0.9 ± 0.7 (0.2–4.1) |
| Lactate * | mmol/L | 1.1 ± 0.4 (0.5–2.1) |
| ASAT * | U/L | 66 ± 30 (22–131) |
| ALAT * | U/L | 53 ± 26 (25–123) |
| CRP max | mg/L | 241 ± 128 (57–534) |
| LDH max | U/L | 671 ± 390 (184–2291) |
| Ferritin max | ng/mL | 2354 ± 2307 (455–11,000) |
| Creatinine max | μmol/L | 124 ± 117 (50–521) |
| Thrombocytes min | G/L | 245 ± 84 (111–458) |
| Bilirubin max | μmol/L | 13.2 ± 12.5 (3.8–52) |
| CK max | U/L | 424 ± 386 (33–1680) |
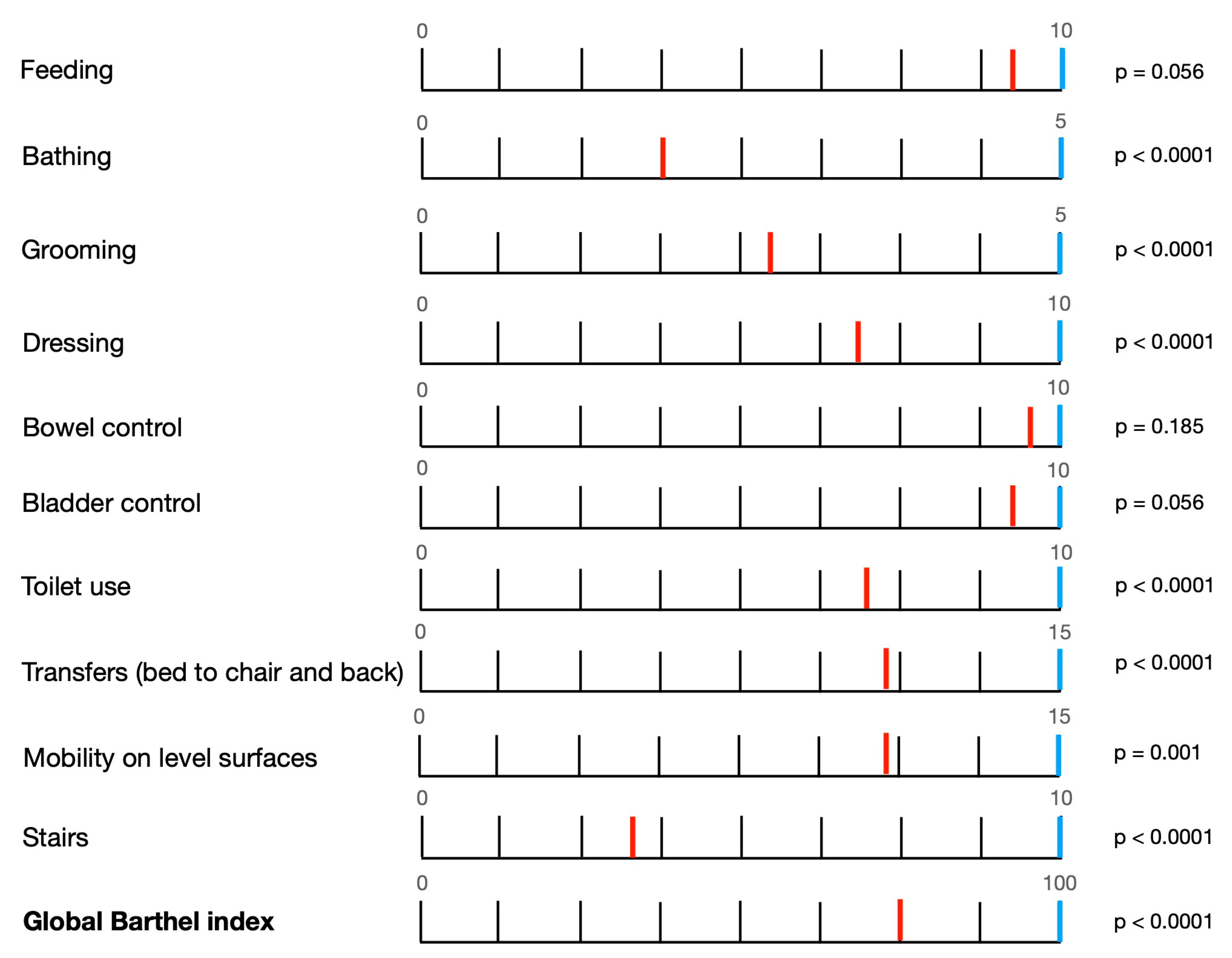
| Acute ADLs | Chronic ADLs | t | dF | p Value | |
|---|---|---|---|---|---|
| Feeding | 8.8 ± 2.9 | 10.0 ± 0 | 0.056 | ||
| Bathing | 2.0 ± 2.5 | 5.0 ± 0 | −6.0 | 24 | <0.0001 * |
| Grooming | 2.6 ± 2.5 | 5.0 ± 0 | −4.707 | 24 | <0.0001 * |
| Dressing | 6.8 ± 3.8 | 10.0 ± 0 | −4.226 | 24 | <0.0001 * |
| Bowel control | 9.4 ± 2.2 | 10.0 ± 0 | 0.185 | ||
| Bladder control | 8.8 ± 3 | 10.0 ± 0 | 0.056 | ||
| Toilet use | 7.0 ± 3.5 | 10.0 ± 0 | −4.243 | 24 | <0.0001 * |
| Transfers (bed to chair and back) | 11.2 ± 4.6 | 15 ± 0 | −4.106 | 24 | <0.0001 * |
| Mobility on level surfaces | 11.4 ± 4.9 | 15 ± 0 | −3.674 | 24 | 0.001 * |
| Stairs | 3.4 ± 4.2 | 10.0 ± 0 | −7.742 | 24 | <0.0001 * |
| Global Barthel index | 75 (55–97.5) | 100 (100–100) | −5.211 | 24 | <0.0001 * |
| Correlation | p Value | |
|---|---|---|
| Demographics Data | ||
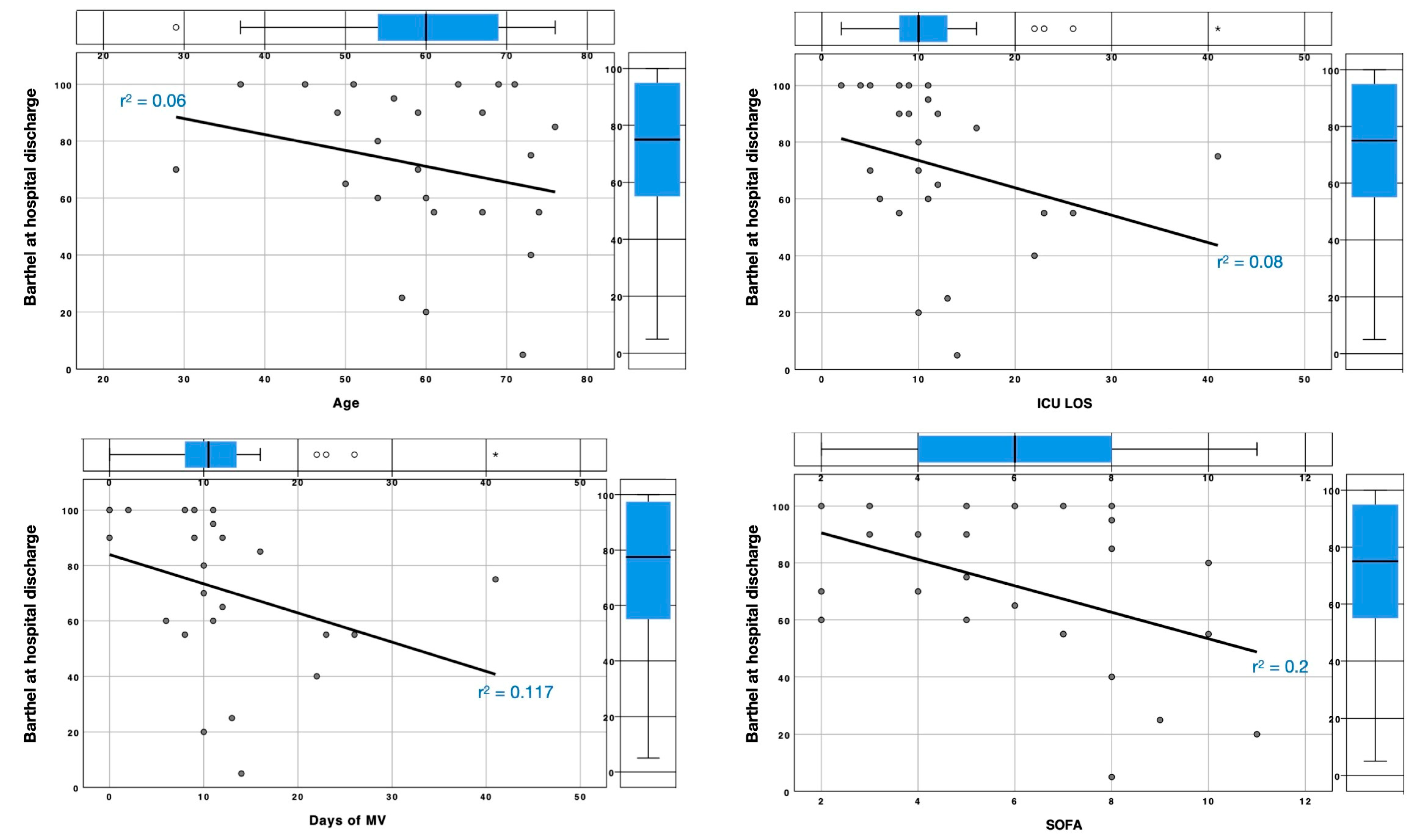
| Age | −0.219 | 0.158 |
| BMI | −0.167 | 0.223 |
| AHT | −0.497 | 0.619 |
| DM | −0.294 | 0.769 |
| OSAS | −0.886 | 0.376 |
| COPD | −0.979 | 0.327 |
| Pulmonary embolism | −0.146 | 0.884 |
| ICU Data | ||
| SAPS II (first 24 h in ICU) | 0.070 | 0.376 |
| SOFA * | −0.473 | 0.01 * |
| Systolic arterial blood pressure * | −0.03 | 0.446 |
| Diastolic arterial blood pressure * | 0.004 | 0.492 |
| Heart rate * | 0.04 | 0.428 |
| Temperature * | −0.031 | 0.444 |
| Oro-tracheal intubation | −1.473 | 0.141 |
| Tracheostomy | −0.935 | 0.35 |
| CRRT | −0.187 | 0.852 |
| Ventilation-associated pneumonia | −0.336 | 0.737 |
| Other ICU infections | −0.206 | 0.837 |
| Days of symptoms before admission | 0.235 | 0.14 |
| ICU LOS | −0.275 | 0.102 |
| MV days | −0.322 | 0.067 |
| Pronation sessions | 0.071 | 0.373 |
| Laboratory Data | ||
| White cells | −0.353 | 0.05 * |
| Lymphocytes | −0.042 | 0.425 |
| Lactate | −0.322 | 0.067 |
| ASAT | 0.004 | 0.493 |
| ALAT | 0.119 | 0.294 |
| CRP max | 0.033 | 0.441 |
| LDH max | −0.238 | 0.137 |
| Ferritin max | 0.102 | 0.322 |
| Creatinine max | 0.163 | 0.229 |
| Thrombocytes min | 0.213 | 0.165 |
| Bilirubin max | −0.184 | 0.2 |
| CK max | −0.142 | 0.258 |
| Sex | HTA | DM | OSAS | COPD | PE | IMV | Trach | CRRT | VAP | Inf | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Feeding | −0.407 0.684 | −0.429 0.668 | −0.228 0.819 | −0.983 0.326 | −0.435 0.664 | −0.445 0.656 | −1.065 0.287 | −0.639 0.523 | −0.639 0.523 | −0.639 0.523 | 0.373 0.709 |
| Bathing | −0.436 0.663 | −0.322 0.747 | −0.171 0.864 | −0.246 0.806 | −0.816 0.414 | −0.845 0.398 | −1.0 0.317 | −1.746 0.081 | −0.436 0.663 | −0.655 0.513 | −1.0 0.317 |
| Grooming | −0.984 0.325 | −0.569 0.569 | −0.975 0.329 | −0.676 0.499 | −1.041 0.298 | −1.0 0.317 | −1.373 0.17 | −1.155 0.248 | −0.086 0.932 | −0.086 0.932 | −0.588 0.588 |
| Dressing | −0.245 0.806 | −1.538 0.124 | −0.385 0.7 | −1.382 0.167 | −0.688 0.492 | −0.881 0.378 | −1.46 0.144 | −1.102 0.27 | −0.245 0.806 | −0.245 0.806 | −0.561 0.575 |
| Bowel control | −0.63 0.529 | −1.628 0.103 | −0.619 0.536 | −1.599 0.11 | −0.295 0.768 | −0.301 0.763 | −0.722 0.47 | −1.417 0.156 | −1.26 0.208 | −1.26 0.208 | −1.155 0.248 |
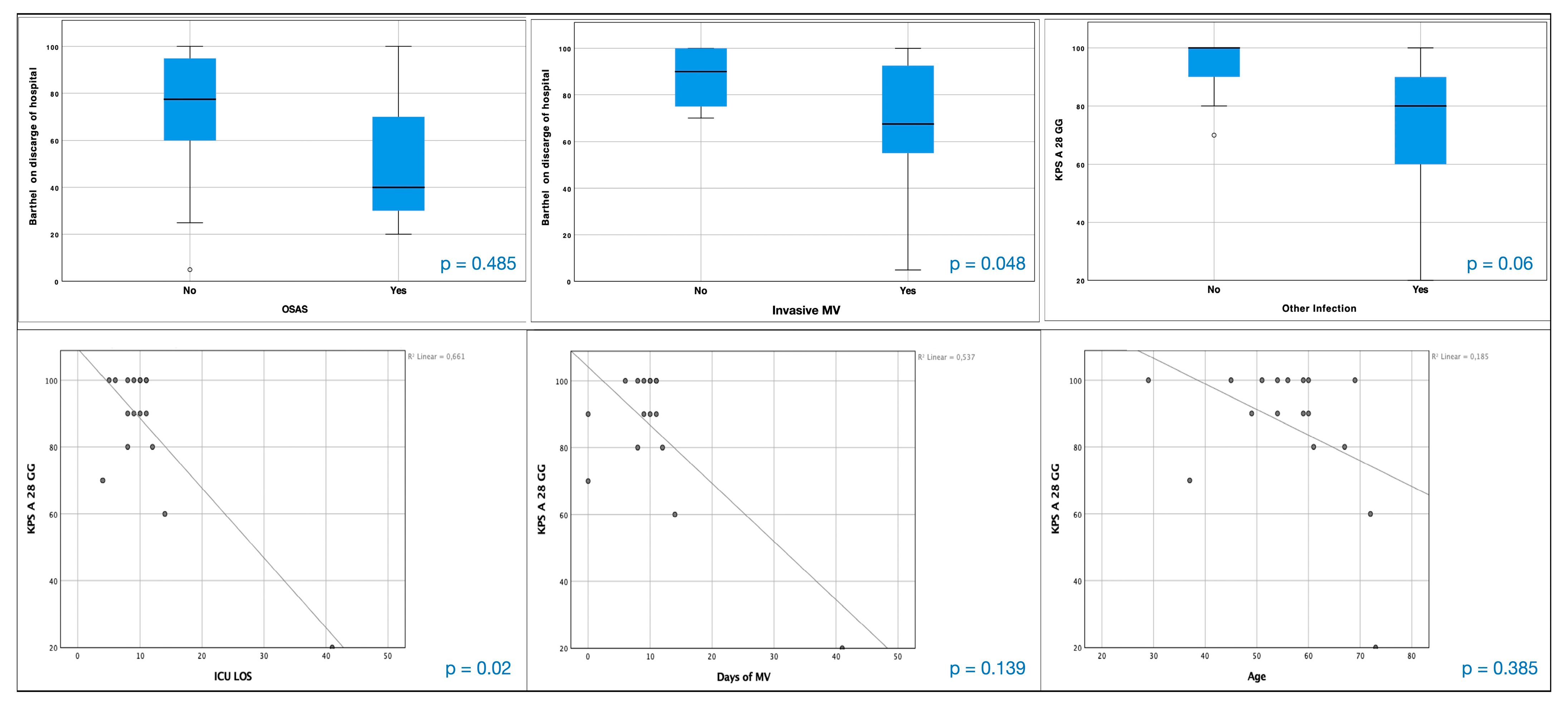
| Bladder control | −0.407 0.684 | −1.416 0.157 | −1.005 0.315 | −0.983 0.326 | −0.435 0.664 | −0.445 0.656 | −0.16 0.873 | −1.975 0.048 * | −0.93 0.353 | −0.93 0.353 | −1.597 0.11 |
| Toilet use | −0.164 0.869 | −0.729 0.466 | −0.129 0.897 | −0.928 0.353 | −0.769 0.442 | −0.717 0.473 | −1.432 0.152 | −0.329 0.742 | −0.329 0.742 | −0.329 0.742 | −0.151 0.88 |
| Transfers | −0.405 0.686 | −0.777 0.437 | −0.413 0.679 | −1.096 0.273 | −1.363 0.173 | −0.47 0.639 | −1.521 0.128 | −0.04 0.968 | −0.486 0.627 | −0.486 0.627 | −0.408 0.683 |
| Mobility on level surfaces | −0.164 0.869 | −0.729 0.466 | −0.129 0.897 | −0.928 0.353 | −0.769 0.442 | −0.717 0.473 | −1.432 0.152 | −0.329 0.742 | −0.329 0.742 | −0.329 0.742 | −0.151 0.88 |
| Stairs | −1.033 0.301 | −1.13 0.259 | −0.325 0.745 | −0.14 0.889 | −0.851 0.395 | −0.816 0.414 | −0.909 0.363 | −0.248 0.804 | −0.207 0.836 | −0.207 0.836 | −0.493 0.622 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceruti, S.; Glotta, A.; Biggiogero, M.; Marzano, M.; Bona, G.; Previsdomini, M.; Saporito, A.; Capdevila, X. Long-Term Evolution of Activities of Daily Life (ADLs) in Critically Ill COVID-19 Patients, a Case Series. Healthcare 2023, 11, 650. https://doi.org/10.3390/healthcare11050650
Ceruti S, Glotta A, Biggiogero M, Marzano M, Bona G, Previsdomini M, Saporito A, Capdevila X. Long-Term Evolution of Activities of Daily Life (ADLs) in Critically Ill COVID-19 Patients, a Case Series. Healthcare. 2023; 11(5):650. https://doi.org/10.3390/healthcare11050650
Chicago/Turabian StyleCeruti, Samuele, Andrea Glotta, Maira Biggiogero, Martino Marzano, Giovanni Bona, Marco Previsdomini, Andrea Saporito, and Xavier Capdevila. 2023. "Long-Term Evolution of Activities of Daily Life (ADLs) in Critically Ill COVID-19 Patients, a Case Series" Healthcare 11, no. 5: 650. https://doi.org/10.3390/healthcare11050650