
Healthcare Resource Utilization in Patients with Newly Diagnosed Atrial Fibrillation: A Global Analysis from the GARFIELD-AF Registry

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Outcomes Measures and Definitions
2.3. Statistical Analysis
3. Results
3.1. Baseline Sample Characteristics
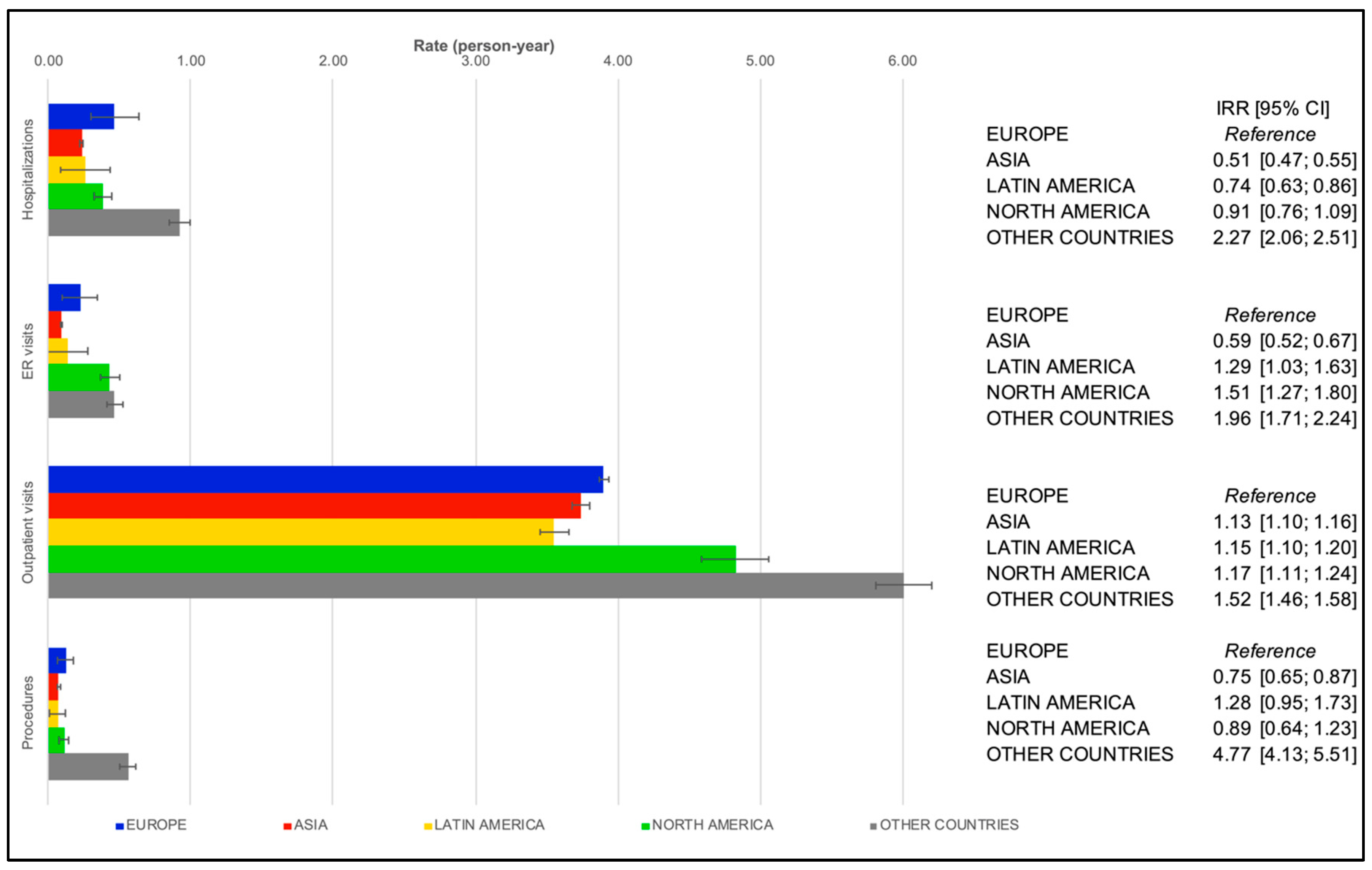
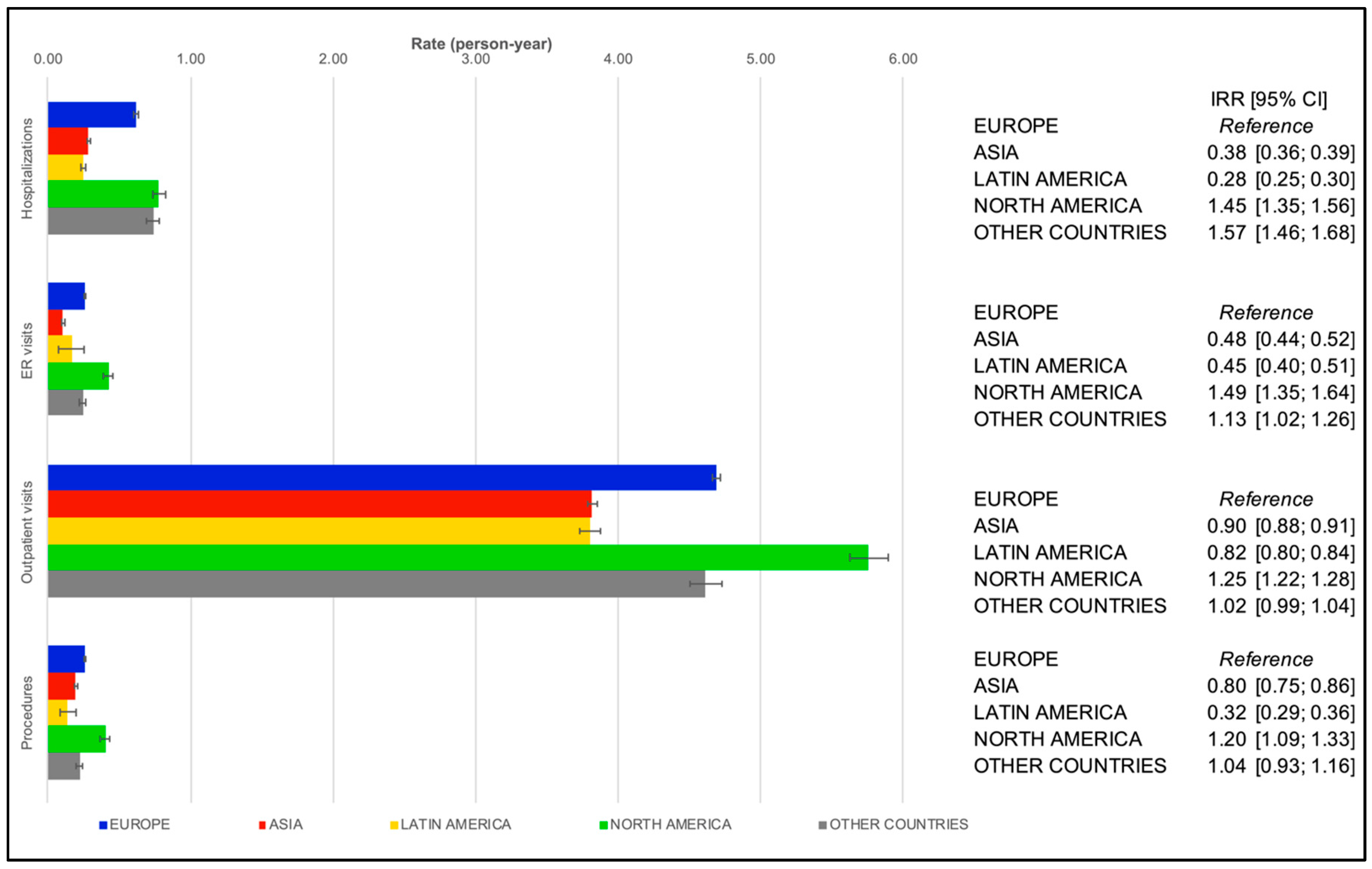
3.2. Healthcare Resource Utilization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.Z.; Benzinger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990 to 2019: Update from the Global Burden of Disease 2019 Study. JACC J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Patel, N.J.; Atti, V.; Mitrani, R.D.; Viles-Gonzalez, J.F.; Goldberger, J.J. Global rising trends of atrial fibrillation: A major public health concern. Heart 2018, 104, 1989–1990. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Song, X.; Liang, Y.; Bai, X.; Liu-Huo, W.S.; Tang, C.; Chen, W.; Zhao, L. Global, regional, and national burden of disease study of atrial fibrillation/flutter, 1990-2019: Results from a global burden of disease study, 2019. BMC Public Health 2022, 22, 2015. [Google Scholar] [CrossRef] [PubMed]
- Borschel, C.S.; Schnabel, R.B. The imminent epidemic of atrial fibrillation and its concomitant diseases—Myocardial infarction and heart failure—A cause for concern. Int. J. Cardiol. 2019, 287, 162–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, K.; Kamal, K.M. Impact of atrial fibrillation on inpatient cost for ischemic stroke in the USA. Int. J. Stroke 2019, 14, 159–166. [Google Scholar] [CrossRef]
- Ball, J.; Carrington, M.J.; McMurray, J.J.; Stewart, S. Atrial fibrillation: Profile and burden of an evolving epidemic in the 21st century. Int. J. Cardiol. 2013, 167, 1807–1824. [Google Scholar] [CrossRef]
- Burdett, P.; Lip, G.Y.H. Atrial Fibrillation in the United Kingdom: Predicting Costs of an Emerging Epidemic Recognising and Forecasting the Cost Drivers of Atrial Fibrillation-related costs. Eur. Heart J. Qual. Care Clin. Outcomes 2020, 8, 187–194. [Google Scholar] [CrossRef]
- Mittal, S.V.; Wu, B.; Song, J.; Milentijevic, D.; Ashton, V.; Mahajan, D. Healthcare resource utilization and costs among nonvalvular atrial fibrillation patients initiating rivaroxaban or warfarin in skilled nursing facilities: A retrospective cohort study. Curr. Med. Res. Opin. 2020, 36, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Sobhy, M.A.; Khoury, M.; Almahmeed, W.A.; Sah, J.; Di Fusco, M.; Mardekian, J.; Kherraf, S.A.; Lopes, R.D.; Hersi, A. The atrial FibriLlatiOn real World management registry in the Middle East and Africa: Design and rationale. J. Cardiovasc. Med. 2020, 21, 704–710. [Google Scholar] [CrossRef]
- Patel, N.J.; Deshmukh, A.; Pant, S.; Singh, V.; Singh, V.; Patel, N.; Arora, S.; Shah, N.; Chothani, A.; Savani, G.T.; et al. Contemporary trends of hospitalization for atrial fibrillation in the United States, 2000 through 2010: Implications for healthcare planning. Circulation 2014, 129, 2371–2379. [Google Scholar] [CrossRef] [Green Version]
- Le Heuzey, J.V.; Bassand, J.P.; Berneau, J.B.; Cozzolino, P.; D’Angiolella, L.; Doucet, B.; Mantovani, L.G.; Mertelet, M.; Mouallem, J.; Muller, J.J.; et al. Stroke prevention, 1-year clinical outcomes and healthcare resource utilization in patients with atrial fibrillation in France: Data from the GARFIELD-AF registry. Arch. Cardiovasc. Dis. 2018, 111, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.R.; Essebag, V.; Zimetbaum, P.; Cohen, D.J. Healthcare resource utilization and costs associated with recurrent episodes of atrial fibrillation: The FRACTAL registry. J. Cardiovasc. Electrophysiol. 2007, 18, 628–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakkar, A.K.; Mueller, I.; Bassand, J.P.; Fitzmaurice, D.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Hacke, W.; Lip, G.Y.; Mantovani, L.G.; et al. International longitudinal registry of patients with atrial fibrillation at risk of stroke: Global Anticoagulant Registry in the FIELD (GARFIELD). Am. Heart J. 2012, 163, 13–19.e1. [Google Scholar] [CrossRef]
- Kakkar, A.K.; Mueller, I.; Bassand, J.P.; Fitzmaurice, D.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Hacke, W.; Lip, G.Y.H.; Mantovani, L.G.; et al. Risk profiles and antithrombotic treatment of patients newly diagnosed with atrial fibrillation at risk of stroke: Perspectives from the international, observational, prospective GARFIELD registry. PLoS ONE 2013, 8, e63479. [Google Scholar] [CrossRef] [Green Version]
- Ambrosio, G.; Camm, A.J.; Bassand, J.P.; Corbalan, R.; Kayani, G.; Carlucio, E.; Mantivani, L.G.; Virdone, S.; Kakkar, A.K. Characteristics, treatment, and outcomes of newly diagnosed atrial fibrillation patients with heart failure: GARFIELD-AF. ESC Heart Fail. 2021, 8, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Cools, F.; Virdone, S.; Bassand, J.-P.; Fitzmaurice, D.A.; Fox, K.A.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Mantovani, L.G.; et al. Mortality in Patients with Atrial Fibrillation Receiving Nonrecommended Doses of Direct Oral Anticoagulants. J. Am. Coll. Cardiol. 2020, 76, 1425–1436. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Accetta, G.; Ambrosio, G.; Atar, D.; Bassand, J.-P.; Berge, E.; Cools, F.; A Fitzmaurice, D.; Goldhaber, S.Z.; Goto, S.; et al. Evolving antithrombotic treatment patterns for patients with newly diagnosed atrial fibrillation. Heart 2017, 103, 307–314. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LLC: College Station, TX, USA, 2013. [Google Scholar]
- Apenteng, P.N.; Gao, H.; Hobbs, R.; Fitzmaurice, D.A.; UK GARFIELD-AF Investigators; GARFIELD-AF Steering Committee. Temporal trends in antithrombotic treatment of real-world UK patients with newly diagnosed atrial fibrillation: Findings from the GARFIELD-AF registry. BMJ Open 2018, 8, e018905. [Google Scholar] [CrossRef]
- Fox, K.A.A.; Accetta, G.; Pieper, K.S.; Bassand, J.-P.; Camm, A.J.; Fitzmaurice, D.A.; Kayani, G.; Kakkar, A.K. Why are outcomes different for registry patients enrolled prospectively and retrospectively? Insights from the global anticoagulant registry in the FIELD-Atrial Fibrillation (GARFIELD-AF). Eur. Heart J. Qual. Care Clin. Outcomes 2018, 4, 27–35. [Google Scholar]
- Klarenbach, S.W.; Jacobs, P. International Comparison of Health Resource Utilization in Subjects with Diabetes. An analysis of Canadian and American national health surveys. Diabetes Care 2003, 26, 1116–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerjes-Sanchez, C.; Corbalan, R.; Barretto, A.C.P.; Luciardi, H.L.; Allu, J.; Illingworth, L.; Pieper, K.S.; Kayani, G. Stroke prevention in patients from Latin American countries with non-valvular atrial fibrillation: Insights from the GARFIELD-AF registry. Clin. Cardiol. 2019, 42, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Rush, K.L.; Burton, L.; Van Der Merwe, F.; Hatt, L.; Galloway, C. Atrial fibrillation care in rural communities: A mixed methods study of physician and patient perspectives. BMC Fam. Pract. 2019, 20, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frohlich, N.; Carriere, K.C.; Potvin, L.; Black, C. Assessing socioeconomic effects on different sized populations: To weight or not to weight? J. Epidemiol. Community Health 2001, 55, 913–920. [Google Scholar] [CrossRef] [Green Version]
- Santos, I.S.; Goulart, A.C.; Olmos, R.D.; Thomas, G.N.; Lip, G.Y.H.; A Lotufo, P.; Benseñor, I.M.; Arasalingam, A.; Brocklehurst, P.; Cheng, K.K.; et al. Atrial fibrillation in low- and middle-income countries: A narrative review. Eur. Heart J. 2020, 22, O61–O77. [Google Scholar] [CrossRef]
- Bassand, J.P.; Virdone, S.; Goldhaber, S.Z.; Camm, A.J.; Fitzmaurice, D.A.; Fox, K.A.; Goto, S.; Haas, S.; Hacke, W.; Kayani, G.; et al. Early Risks of Death, Stroke/Systemic Embolism, and Major Bleeding in Patients with Newly Diagnosed Atrial Fibrillation. Circulation 2019, 139, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, B.A.; Kim, S.; Fonarow, G.C.; Thomas, L.; Ansell, J.; Kowey, P.R.; Mahaffey, K.W.; Gersh, B.J.; Hylek, E.; Naccarelli, G.; et al. Drivers of hospitalization for patients with atrial fibrillation: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Am. Heart J. 2014, 167, 735–742.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhat, A.; Khanna, S.; Chen, H.H.L.; Gan, G.C.H.; MacIntyre, C.R.; Tan, T.C. Drivers of hospitalization in atrial fibrillation: A contemporary review. Heart Rhythm 2020, 17, 1991–1999. [Google Scholar] [CrossRef]
- Bumpus, S.; Krallman, R.; McMahon, C.; Gupta, A.; Montgomery, D.; Kline-Rogers, E.; Vaishnava, P. Insights into hospital readmission patterns of atrial fibrillation patients. Eur. J. Cardiovasc. Nurs. 2020, 19, 545–550. [Google Scholar] [CrossRef]
- Tripathi, B.; Atti, V.; Kumar, V.; Naraparaju, V.; Sharma, P.; Arora, S.; Wojtaszek, E.; Gopalan, R.; Siontis, K.C.; Gersh, B.J.; et al. Outcomes and Resource Utilization Associated with Readmissions After Atrial Fibrillation Hospitalizations. J. Am. Heart Assoc. 2019, 8, e013026. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Asia | Europe | Latin America | North America | Other GARFIELD–AF Countries | |
|---|---|---|---|---|---|---|
| N (%) | 49,574 (100.00) | 14,059 (28.36) | 27,987 (56.45) | 4004 (8.08) | 1554 (3.13) | 1970 (3.97) |
| Cohort | ||||||
| Group A (C2-3) | 16,459 (33.20) | 3711 (26.40) | 10,449 (37.34) | 1390 (34.72) | 331 (21.30) | 578 (29.34) |
| Group B (C4-6) | 33,115 (66.80) | 10,348 (73.60) | 17,538 (62.66) | 2614 (65.28) | 1223 (78.70) | 1392 (70.66) |
| Sex | ||||||
| Male | 27,586 (55.65) | 8251 (58.69) | 15,293 (54.64) | 2106 (52.60) | 849 (54.63) | 1087 (55.18) |
| Female | 21,988 (44.35) | 5808 (41.31) | 12,694 (45.36) | 1898 (47.40) | 705 (45.37) | 883 (44.82) |
| Age | ||||||
| Mean (SD) | 69.62 (11.48) | 67.54 (12.00) | 70.73 (10.90) | 69.77 (11.92) | 71.05 (11.84) | 67.32 (12.04) |
| Median (IQR) | 71 (63–78) | 69 (60–76) | 72 (64–79) | 71 (63–78.5) | 72 (64–80) | 68 (60–76) |
| Comorbid conditions | ||||||
| Diabetes | ||||||
| No | 38,458 (77.58) | 10,903 (77.55) | 21,975 (78.52) | 3011 (75.20) | 1143 (73.55) | 1426 (72.39) |
| Yes | 11,116 (22.42) | 3156 (22.45) | 6012 (21.48) | 993 (24.80) | 411 (26.45) | 544 (27.61) |
| Chronic kidney disease | ||||||
| No | 22,753 (45.90) | 7941 (56.48) | 11,055 (39.50) | 1876 (46.85) | 926 (59.59) | 955 (48.48) |
| I | 9994 (20.16) | 2702 (19.22) | 6034 (21.56) | 809 (20.20) | 164 (10.55) | 285 (14.47) |
| II | 5896 (11.89) | 1020 (7.26) | 4314 (15.41) | 192 (4.80) | 112 (7.21) | 258 (13.10) |
| III/IV | 4918 (9.92) | 960 (6.83) | 3387 (12.10) | 241 (6.02) | 125 (8.04) | 205 (10.41) |
| V | 226 (0.46) | 108 (0.77) | 74 (0.26) | 26 (0.65) | 11 (0.71) | 7 (0.36) |
| Unknown | 5786 (11.67) | 1328 (9.45) | 3123 (11.16) | 859 (21.45) | 216 (13.90) | 260 (13.20) |
| Missing | 1 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.02) | 0 (0.00) | 0 (0.00) |
| Hypercholesterolemia | ||||||
| No | 27,841 (56.16) | 9751 (69.36) | 14,317 (51.16) | 2327 (58.12) | 623 (40.09) | 823 (41.78) |
| Yes | 20,257 (40.86) | 4020 (28.59) | 12,778 (45.66) | 1468 (36.66) | 904 (58.17) | 1087 (55.18) |
| Unknown | 1476 (2.98) | 288 (2.05) | 892 (3.19) | 209 (5.22) | 27 (1.74) | 60 (3.05) |
| Cirrhosis | ||||||
| No | 48,647 (98.13) | 13,784 (98.04) | 27,541 (98.41) | 3912 (97.7) | 1505 (96.85) | 1905 (96.70) |
| Yes | 272 (0.55) | 92 (0.65) | 134 (0.48) | 14 (0.35) | 14 (0.90) | 18 (0.91) |
| Unknown | 655 (1.32) | 183 (1.30) | 312 (1.11) | 78 (1.95) | 35 (2.25) | 47 (2.39) |
| Congestive Heart Failure | ||||||
| No | 39,688 (80.06) | 11,274 (80.19) | 22,237 (79.45) | 3200 (79.92) | 1323 (85.14) | 1654 (83.96) |
| Yes | 9886 (19.94) | 2785 (19.81) | 5750 (20.55) | 804 (20.08) | 231 (14.86) | 316 (16.04) |
| Vascular Disease | ||||||
| No | 42,209 (85.14) | 12,400 (88.20) | 23,553 (84.16) | 3425 (85.54) | 1285 (82.69) | 1546 (78.48) |
| Yes | 7365 (14.86) | 1659 (11.80) | 4434 (15.84) | 579 (14.46) | 269 (17.31) | 424 (21.52) |
| Type of atrial fibrillation | ||||||
| Permanent | 6285 (12.68) | 1195 (8.50) | 4193 (14.98) | 643 (16.06) | 35 (2.25) | 219 (11.12) |
| Persistent | 7427 (14.98) | 2438 (17.34) | 4104 (14.66) | 597 (14.91) | 97 (6.24) | 191 (9.70) |
| Paroxysmal | 13,739 (27.71) | 5169 (36.77) | 6933 (24.77) | 1050 (26.22) | 332 (21.36) | 255 (12.94) |
| New onset (unclassified) | 22,123 (44.63) | 5257 (37.39) | 12,757 (45.58) | 1714 (42.81) | 1090 (70.14) | 1305 (66.24) |
| Stroke prophylaxis | ||||||
| AP or none | 15,933 (32.14) | 6013 (42.77) | 7431 (26.55) | 1484 (37.06) | 500 (32.18) | 505 (25.63) |
| VKA ± AP | 19,352 (39.04) | 4140 (29.45) | 12,396 (44.29) | 1580 (39.46) | 341 (21.94) | 895 (45.43) |
| NOACs ± AP | 13,598 (27.43) | 3752 (26.69) | 7733 (27.63) | 874 (21.83) | 694 (44.66) | 545 (27.66) |
| Unknown | 691 (1.39) | 154 (1.10) | 427 (1.53) | 66 (1.65) | 19 (1.22) | 25 (1.27) |
| History of bleeding | ||||||
| No | 48,157 (97.14) | 13,723 (97.61) | 27,230 (97.3) | 3841 (95.93) | 1470 (94.59) | 1893 (96.09) |
| Yes | 1237 (2.50) | 230 (1.64) | 712 (2.54) | 158 (3.95) | 72 (4.63) | 65 (3.30) |
| Unknown | 180 (0.36) | 106 (0.75) | 45 (0.16) | 5 (0.12) | 12 (0.77) | 12 (0.61) |
| Prior transient ischemic attack | ||||||
| No | 47,138 (95.09) | 13,631 (96.96) | 26,460 (94.54) | 3815 (95.28) | 1457 (93.76) | 1775 (90.10) |
| Yes | 2183 (4.40) | 302 (2.15) | 1451 (5.18) | 173 (4.32) | 81 (5.21) | 176 (8.93) |
| Unknown | 253 (0.51) | 126 (0.90) | 76 (0.27) | 16 (0.40) | 16 (1.03) | 19 (0.96) |
| CHA2DS2-VASc score | ||||||
| 0 | 1366 (2.76) | 684 (4.87) | 470 (1.68) | 115 (2.87) | 46 (2.96) | 51 (2.59) |
| 1 | 6072 (12.25) | 2300 (16.36) | 2904 (10.38) | 442 (11.04) | 175 (11.26) | 251 (12.74) |
| 2 | 9950 (20.07) | 3116 (22.16) | 5428 (19.39) | 728 (18.18) | 286 (18.40) | 392 (19.90) |
| 3 | 11,954 (24.11) | 3181 (22.63) | 7010 (25.05) | 933 (23.30) | 366 (23.55) | 464 (23.55) |
| 4 | 10,837 (21.86) | 2584 (18.38) | 6481 (23.16) | 982 (24.53) | 366 (23.55) | 424 (21.52) |
| 5 | 5624 (11.34) | 1356 (9.65) | 3399 (12.14) | 470 (11.74) | 188 (12.10) | 211 (10.71) |
| 6–9 | 3771 (7.61) | 838 (5.96) | 2295 (8.20) | 334 (8.34) | 127 (8.17) | 177 (8.98) |
| Cohort Group A | Cohort Group B | Total | p-Value | |
|---|---|---|---|---|
| N (%) | 16,459 (33.20) | 33,115 (66.80) | 49,574 (100.0) | |
| Sex | 0.316 | |||
| Male | 9211 (55.96) | 18,375 (55.49) | 27,586 (55.65) | |
| Female | 7248 (44.04) | 14,740 (44.51) | 21,988 (44.35) | |
| Age | 0.139 | |||
| Mean (SD) | 69.73 (11.40) | 69.57 (11.52) | 69.62 (11.48) | |
| Median (IQR) | 71 (63-78) | 71 (62–78) | 71 (63–78) | |
| Comorbid conditions | ||||
| Diabetes | 0.247 | |||
| No | 12,819 (77.88) | 25,639 (77.42) | 38,458 (77.58) | |
| Yes | 3640 (22.12) | 7476 (22.58) | 11,116 (22.42) | |
| Chronic kidney disease * | <0.001 | |||
| None | 93 (0.57) | 22,660 (68.43) | 22,753 (45.90) | |
| I | 8099 (49.21) | 1895 (5.72) | 9994 (20.16) | |
| II | 2434 (14.79) | 3462 (10.45) | 5896 (11.89) | |
| III/IV | 1629 (9.90) | 3289 (9.93) | 4918 (9.92) | |
| V | 70 (0.43) | 156 (0.47) | 226 (0.46) | |
| Unknown | 4134 (25.12) | 1652 (4.99) | 5786 (11.67) | |
| Missing | 0 (0.00) | 1 (0.00) | 1 (0.00) | |
| Hypercholesterolemia | <0.001 | |||
| No | 9765 (59.33) | 18,076 (54.59) | 27,841 (56.16) | |
| Yes | 6689 (40.64) | 13,568 (40.97) | 20,257 (40.86) | |
| Unknown | 5 (0.03) | 1471 (4.44) | 1476 (2.98) | |
| Cirrhosis | <0.001 | |||
| No | 16,365 (99.43) | 32,282 (97.48) | 48,647 (98.13) | |
| Yes | 83 (0.50) | 189 (0.57) | 272 (0.55) | |
| Unknown | 11 (0.07) | 644 (1.94) | 655 (1.32) | |
| Congestive Heart Failure | 0.001 | |||
| No | 13,041 (79.23) | 26,647 (80.47) | 39,688 (80.06) | |
| Yes | 3418 (20.77) | 6468 (19.53) | 9886 (19.94) | |
| Vascular Disease | 0.345 | |||
| No | 14,049 (85.36) | 28,160 (85.04) | 42,209 (85.14) | |
| Yes | 2410 (14.64) | 4955 (14.96) | 7365 (14.86) | |
| Type of atrial fibrillation | <0.001 | |||
| Permanent | 2160 (13.12) | 4125 (12.46) | 6285 (12.68) | |
| Persistent | 2556 (15.53) | 4871 (14.71) | 7427 (14.98) | |
| Paroxysmal | 4199 (25.51) | 9540 (28.81) | 13,739 (27.71) | |
| New onset (unclassified) | 7544 (45.84) | 14,579 (44.03) | 22,123 (44.63) | |
| Stroke prophylaxis | <0.001 | |||
| VKA ± AP | 8161 (49.58) | 11,191 (33.79) | 19,352 (39.04) | |
| NOACs ± AP | 1781 (10.82) | 11,817 (35.68) | 13,598 (27.43) | |
| None ± AP | 6232 (37.86) | 9701 (29.29) | 15,933 (32.14) | |
| Unknown | 285 (1.73) | 406 (1.23) | 691 (1.39) | |
| History of bleeding | <0.001 | |||
| No | 15,979 (97.08) | 32,178 (97.17) | 48,157 (97.14) | |
| Yes | 472 (2.87) | 765 (2.31) | 1237 (2.50) | |
| Unknown | 8 (0.05) | 172 (0.52) | 180 (0.36) | |
| Prior transient ischemic attack | <0.001 | |||
| No | 15,582 (94.67) | 31,556 (95.29) | 47,138 (95.09) | |
| Yes | 870 (5.29) | 1313 (3.96) | 2183 (4.40) | |
| Unknown | 7 (0.04) | 246 (0.74) | 253 (0.51) | |
| CHA2DS2-VASc score | <0.001 | |||
| 0 | 386 (2.35) | 980 (2.96) | 1366 (2.76) | |
| 1 | 1951 (11.85) | 4121 (12.44) | 6072 (12.25) | |
| 2 | 3218 (19.55) | 6732 (20.33) | 9950 (20.07) | |
| 3 | 3975 (24.15) | 7979 (24.09) | 11,954 (24.11) | |
| 4 | 3610 (21.93) | 7227 (21.82) | 10,837 (21.86) | |
| 5 | 1947 (11.83) | 3677 (11.10) | 5624 (11.34) | |
| 6–9 | 1372 (8.34) | 2399 (7.24) | 3771 (7.61) | |
| HCRU Events * (N [%]) | Total | Asia | Europe | Latin America | North America | Other GARFIELD–AF Countries |
|---|---|---|---|---|---|---|
| Hospitalizations | 15,046 (30.35) | 2617 (18.61) | 10,412 (37.20) | 607 (15.16) | 582 (37.45) | 828 (42.03) |
| ER admissions | 8129 (16.40) | 1137 (8.09) | 5637 (20.14) | 434 (10.84) | 482 (31.02) | 439 (22.28) |
| Procedures ^ | 7167 (14.46) | 1540 (10.95) | 4527 (16.18) | 302 (7.54) | 390 (25.10) | 408 (20.71) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, L.G.; Cozzolino, P.; Ferrara, P.; Virdone, S.; Camm, A.J.; Verheugt, F.W.A.; Bassand, J.-P.; Turpie, A.G.G.; Hacke, W.; Kayani, G.; et al. Healthcare Resource Utilization in Patients with Newly Diagnosed Atrial Fibrillation: A Global Analysis from the GARFIELD-AF Registry. Healthcare 2023, 11, 638. https://doi.org/10.3390/healthcare11050638
Mantovani LG, Cozzolino P, Ferrara P, Virdone S, Camm AJ, Verheugt FWA, Bassand J-P, Turpie AGG, Hacke W, Kayani G, et al. Healthcare Resource Utilization in Patients with Newly Diagnosed Atrial Fibrillation: A Global Analysis from the GARFIELD-AF Registry. Healthcare. 2023; 11(5):638. https://doi.org/10.3390/healthcare11050638
Chicago/Turabian StyleMantovani, Lorenzo G., Paolo Cozzolino, Pietro Ferrara, Saverio Virdone, A. John Camm, Freek W. A. Verheugt, Jean-Pierre Bassand, Alexander G. G. Turpie, Werner Hacke, Gloria Kayani, and et al. 2023. "Healthcare Resource Utilization in Patients with Newly Diagnosed Atrial Fibrillation: A Global Analysis from the GARFIELD-AF Registry" Healthcare 11, no. 5: 638. https://doi.org/10.3390/healthcare11050638