
Real-World Analysis on the Characteristics, Therapeutic Paths and Economic Burden for Patients Treated for Glaucoma in Italy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
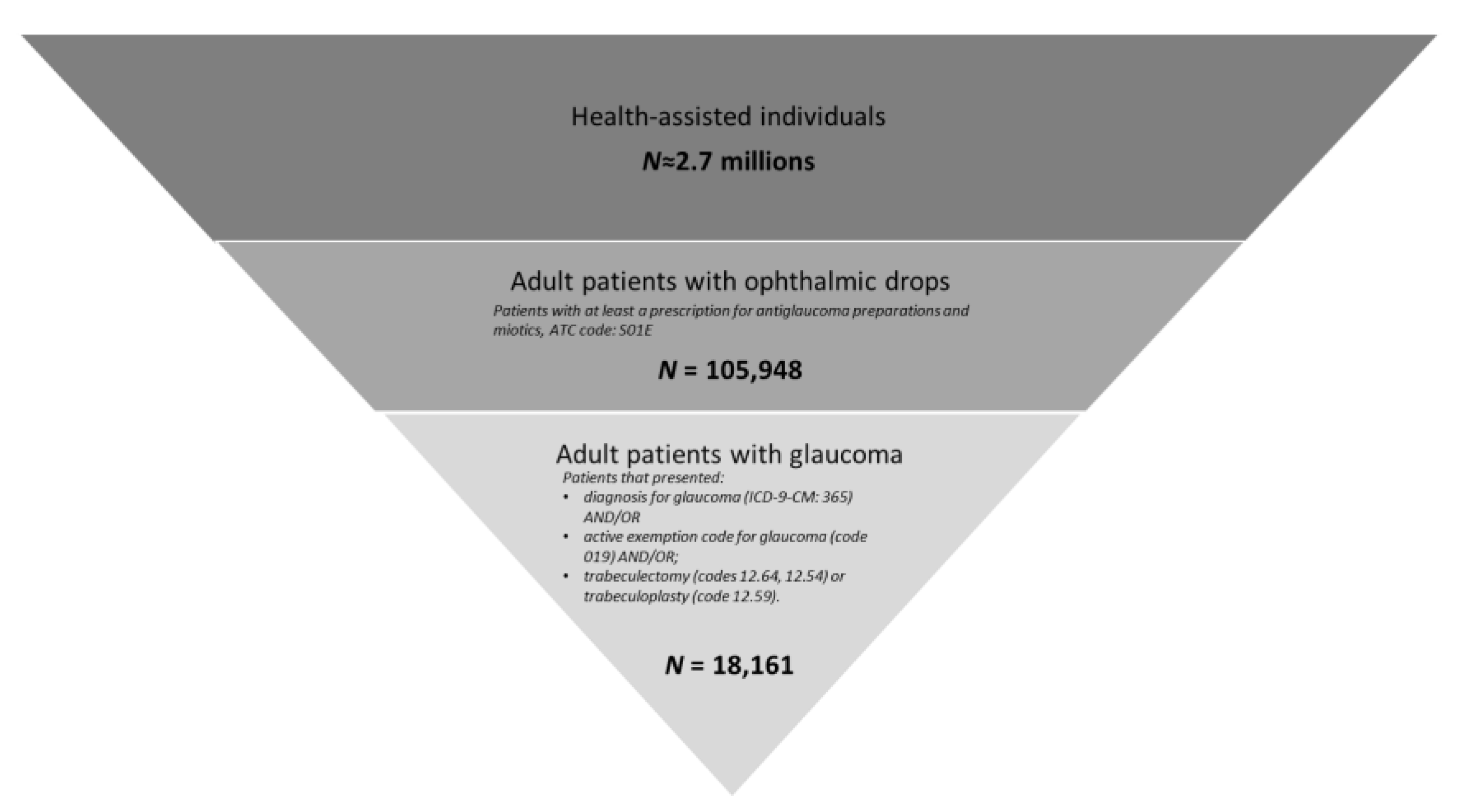
2.2. Patient Population
2.3. Baseline Patient’ Characteristics
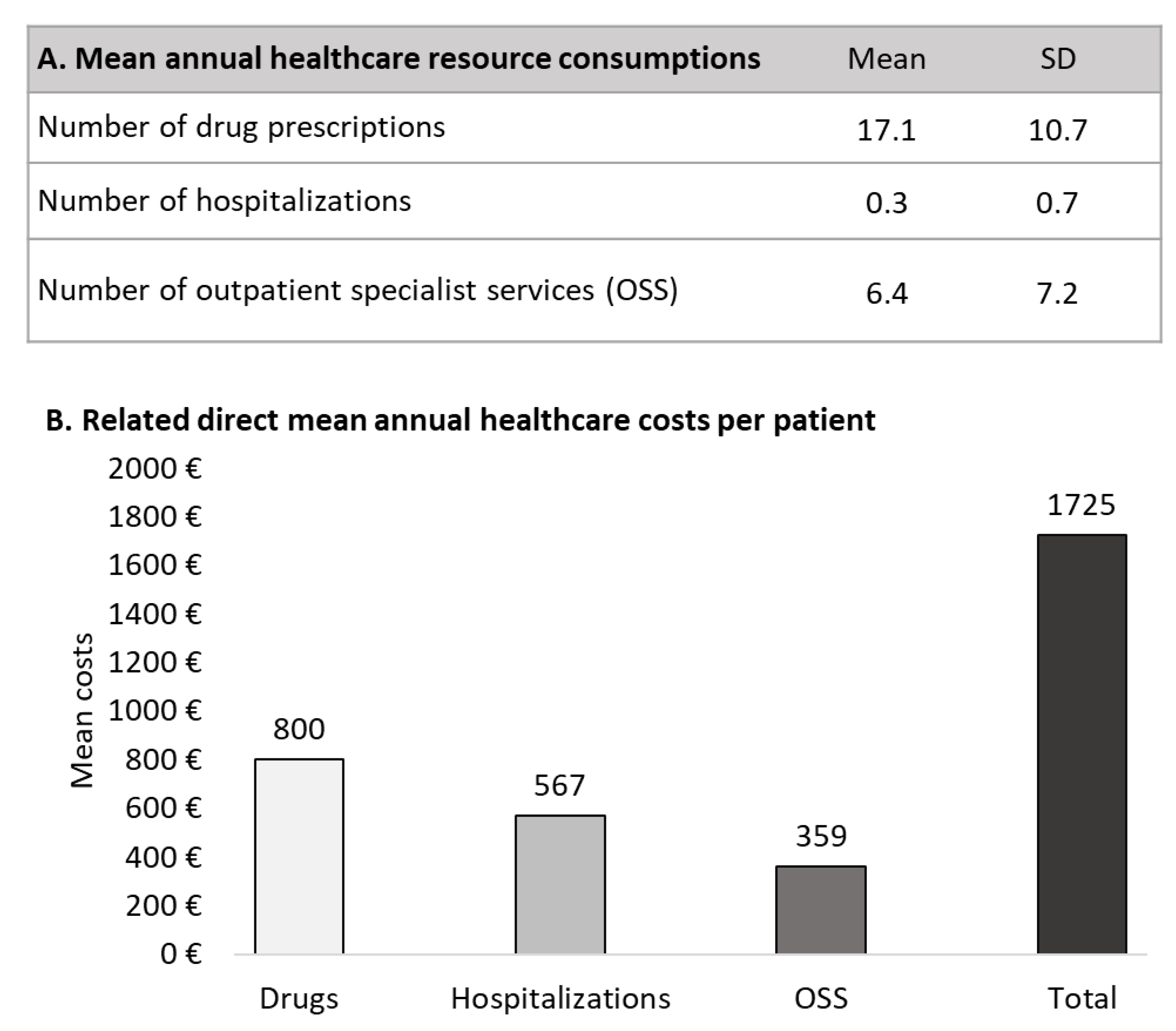
2.4. Healthcare Resource Consumption and Costs
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swenor, B.K.; Ehrlich, J.R. Ageing and vision loss: Looking to the future. Lancet Glob. Health 2021, 9, e385–e386. [Google Scholar] [CrossRef]
- Kreft, D.; Doblhammer, G.; Guthoff, R.F.; Frech, S. Prevalence, incidence, and risk factors of primary open-angle glaucoma—A cohort study based on longitudinal data from a German public health insurance. BMC Public Health 2019, 19, 851. [Google Scholar] [CrossRef] [Green Version]
- Leske, M.C. Open-Angle Glaucoma—An Epidemiologic Overview. Ophthalmic Epidemiol. 2007, 14, 166–172. [Google Scholar] [CrossRef]
- Lee, D.A.; Higginbotham, E.J. Glaucoma and its treatment: A review. Am. J. Health Pharm. 2005, 62, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Coleman, A.L.; Kodjebacheva, G. Risk factors for glaucoma needing more attention. Open Ophthalmol. J. 2009, 3, 38–42. [Google Scholar] [CrossRef]
- Allison, K.; Patel, D.; Alabi, O. Epidemiology of Glaucoma: The Past, Present, and Predictions for the Future. Cureus 2020, 12, e11686. [Google Scholar] [CrossRef]
- Costagliola, C.; Sbordone, M.; Gandolfi, S.; Cesari, L.; Furneri, G.; Fea, A.M. Minimally Invasive Surgery in Mild-to-Moderate Glaucoma Patients in Italy: Is It Time to Change? Clin. Ophthalmol. 2020, 14, 2639–2655. [Google Scholar] [CrossRef]
- Wang, Y.; Alnwisi, S.; Ke, M. The impact of mild, moderate, and severe visual field loss in glaucoma on patients’ quality of life measured via the Glaucoma Quality of Life-15 Questionnaire. Medicine 2017, 96, e8019. [Google Scholar] [CrossRef] [PubMed]
- Floriani, I.; Quaranta, L.; Rulli, E.; Katsanos, A.; Varano, L.; Frezzotti, P.; Rossi, G.C.M.; Carmassi, L.; Rolle, T.; Ratiglia, R.; et al. Health-related quality of life in patients with primary open-angle glaucoma. An Italian multicentre observational study. Acta Ophthalmol. 2015, 94, e278–e286. [Google Scholar] [CrossRef] [Green Version]
- Spaeth, G.L. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br. J. Ophthalmol. 2021, 105 (Suppl. S1), 1–169. [Google Scholar] [CrossRef]
- Li, T.; Lindsley, K.; Rouse, B.; Hong, H.; Shi, Q.; Friedman, D.S.; Wormald, R.; Dickersin, K. Comparative Effectiveness of First-Line Medications for Primary Open-Angle Glaucoma. Ophthalmology 2015, 123, 129–140. [Google Scholar] [CrossRef] [Green Version]
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition—Chapter 3: Treatment principles and options Supported by the EGS Foundation. Br. J. Ophthalmol. 2017, 101, 130–195. [CrossRef] [Green Version]
- Zaharia, A.-C.; Dumitrescu, O.-M.; Radu, M.; Rogoz, R.-E. Adherence to Therapy in Glaucoma Treatment—A Review. J. Pers. Med. 2022, 12, 514. [Google Scholar] [CrossRef]
- Rossi, G.C.; Pasinetti, G.M.; Scudeller, L.; Radaelli, R.; Bianchi, P.E. Do Adherence Rates and Glaucomatous Visual Field Progression Correlate? Eur. J. Ophthalmol. 2011, 21, 410–414. [Google Scholar] [CrossRef]
- Sleath, B.; Blalock, S.; Covert, D.; Stone, J.L.; Skinner, A.C.; Muir, K.; Robin, A.L. The Relationship between Glaucoma Medication Adherence, Eye Drop Technique, and Visual Field Defect Severity. Ophthalmology 2011, 118, 2398–2402. [Google Scholar] [CrossRef] [Green Version]
- Sleath, B.; Blalock, S.J.; Stone, J.L.; Skinner, A.C.; Covert, D.; Muir, K.; Robin, A. Validation of a short version of the glaucoma medication self-efficacy questionnaire. Br. J. Ophthalmol. 2011, 96, 258–262. [Google Scholar] [CrossRef]
- Meichenbaum, D.; Turk, D. Facilitating Treatment Adherence: A Practitioner’s Guidebook; Plenum: New York, NY, USA, 1987; pp. 1–55. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Cedrone, C.; Culasso, F.; Cesareo, M.; Zapelloni, A.; Cedrone, P.; Cerulli, L. Prevalence of glaucoma in Ponza, Italy: A comparison with other studies. Ophthalmic Epidemiology 1997, 4, 59–72. [Google Scholar] [CrossRef]
- Huber, M.; Kölzsch, M.; Stahlmann, R.; Hofmann, W.; Bolbrinker, J.; Dräger, D.; Kreutz, R. Ophthalmic Drugs as Part of Polypharmacy in Nursing Home Residents with Glaucoma. Drugs Aging 2012, 30, 31–38. [Google Scholar] [CrossRef]
- Robin, A.L.; Muir, K.W. Medication adherence in patients with ocular hypertension or glaucoma. Expert Rev. Ophthalmol. 2019, 14, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Rouland, J.-F.; Le Pen, C.; Benhaddi, H.; Piriou, E.; Lilliu, H.; Kenigsberg, P.-A.; Abellan, P.; Arnoux, M.; Attia, A.; Baudouin, C.; et al. Naturalistic, Prospective Study of Glaucoma and Ocular Hypertension Treatment in France: Strategies, Clinical Outcomes, and Costs at 2 Years. Eur. J. Ophthalmol. 2005, 15, 562–580. [Google Scholar] [CrossRef]
- Pöhlmann, J.; Norrbacka, K.; Boye, K.S.; Valentine, W.J.; Sapin, H. Costs and where to find them: Identifying unit costs for health economic evaluations of diabetes in France, Germany and Italy. Eur. J. Health Econ. 2020, 21, 1179–1196. [Google Scholar] [CrossRef]
- Wilensky, J.; Fiscella, R.G.; Carlson, A.M.; Morris, L.S.; Walt, J. Measurement of Persistence and Adherence to Regimens of IOP-Lowering Glaucoma Medications Using Pharmacy Claims Data. Am. J. Ophthalmol. 2006, 141, 28–33. [Google Scholar] [CrossRef]
- Hwang, D.-K.; Liu, C.J.-L.; Pu, C.-Y.; Chou, Y.-J.; Chou, P. Persistence of Topical Glaucoma Medication. JAMA Ophthalmol. 2014, 132, 1446–1452. [Google Scholar] [CrossRef] [Green Version]
- Traverso, C.E.; Walt, J.G.; Kelly, S.P.; Hommer, A.H.; Bron, A.M.; Denis, P.; Nordmann, J.P.; Renard, J.P.; Bayer, A.; Grehn, F.; et al. Direct costs of glaucoma and severity of the disease: A multinational long term study of resource utilisation in Europe. Br. J. Ophthalmol. 2005, 89, 1245–1249. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total Glaucoma Patients (N = 18,161) | Patients with Drop Therapy Only (N = 15,749) | Patients with Trabeculoplasty (N = 354) | p-Valued | |
|---|---|---|---|---|
| Male, n (%) | 8047 (44.3) | 7151 (45.4) | 201 (56.8) | <0.001 |
| Age, mean (SD) | 66.6 (14.7) | 68.6 (13.0) | 70.5 (11.6) | 0.006 |
| Age groups | ||||
| 18−24 years, n (%) | 137 (0.8) | 51 (0.3) | NR | |
| 25−34 years, n (%) | 508 (2.8) | 145 (0.9) | NR | |
| 35−44 years, n (%) | 897 (4.9) | 494 (3.1) | 5 (1.4) | 0.002 |
| 45−54 years, n (%) | 1902 (10.5) | 1661 (10.5) | 24 (6.8) | |
| 55−64 years, n (%) | 3704 (20.4) | 3363 (21.4) | 62 (17.5) | |
| 65−74 years, n (%) | 5091 (28.1) | 4538 (28.8) | 114 (32.2) | |
| 75−84 years, n (%) | 4276 (23.6) | 3923 (24.9) | 117 (33.1) | |
| >85 years, n (%) | 1646 (9.1) | 1574 (10.0) | 29 (8.2) | |
| Charlson index (mean, SD) | 0.9 (1.0) | 0.9 (1.0) | 1.1 (1.1) | <0.001 |
| Charlson index = 0, n (%) | 7743 (42.6) | 6744 (42.8) | 115 (32.5) | <0.001 |
| Charlson index = 1, n (%) | 6481 (35.7) | 5645 (35.8) | 141 (39.8) | |
| Charlson index ≥ 2, n (%) | 3937 (21.7) | 3360 (21.3) | 98 (27.7) | |
| Hypertension, n (%) | 10,935 (60.2) | 9861 (62.6) | 250 (70.6) | 0.002 |
| Dyslipidemia, n (%) | 5385 (29.7) | 4868 (30.9) | 127 (35.9) | 0.046 |
| Diabetes, n (%) | 3091 (17.0) | 2733 (17.4) | 115 (32.5) | <0.001 |
| Cataract, n (%) | 1609 (8.9) | 1398 (8.9) | 53 (15.0) | <0.001 |
| Blindess, n (%) | 126 (0.7) | 99 (0.6) | NR | - |
| Retinal/choroid disorders, n (%) | 301 (1.7) | 222 (1.4) | 16 (4.5) | <0.001 |
| Diabetic retinopathy, n (%) | 72 (0.4) | 57 (0.4) | NR | - |
| Wet age-related macular degeneration, n (%) | 22 (0.1) | 16 (0.1) | NR | - |
| Retinal vein occlusion, n (%) | 24 (0.1) | 15 (0.1) | NR | - |
| Parkinson’s disease, n (%) | 98 (0.5) | 96 (0.6) | NR | - |
| Alzheimer’s disease, n (%) | 24 (0.1) | 23 (0.1) | NR | - |
| Rheumatoid arthritis, n (%) | 168 (0.9) | 158 (1.0) | NR | - |
| First Line | Second Line | N (%) | Third Line | N (%) |
|---|---|---|---|---|
Ophthalmic drops (N = 17,456)
| / | 5407 (31.0) | ||
| Other ophthalmic drops 1st L SA -> 2nd L SA 1st L SA -> 2nd L COMB 1st L COMB -> 2nd L SA 1st L COMB -> 2nd L COMB | 11,490 (65.8) −5644 3231 −1951 −664 | / | 1627 (14.2) | |
Other ophthalmic drops
| 9733 (84.7)
| |||
| Trabeculectomy | 102 (0.9) | |||
| Trabeculoplasty | 28 (0.2) | |||
| Trabeculectomy | 481 (2.8) | / | 276 (57.4) | |
| Other ophthalmic drops | 205 (42.6) (164 SA, 41 COMB) | |||
| Trabeculoplasty | 78 (0.4) | / | 29 (37.2) | |
| Other ophthalmic drops | 48 (61.5) (36 SA, 12 COMB) | |||
| Trabeculectomy | NI | |||
| Trabeculectomy (N = 628) | Ophthalmic drops | 628 (100) (518 SA, 110 COMB) | / | 389 (61.9) |
| Other ophthalmic drops 2nd L SA -> 3rd L SA 2nd L SA -> 3rd L COMB 2nd L COMB -> 3rd L SA 2ndL COMB -> 3rd L COMB | 166 (26.4)
| |||
| Trabeculectomy | 73 (11.6) | |||
| Trabeculoplasty (N = 77) | Other ophthalmic drops | 77 (100) (71 SA, 6 COMB) | / | 39 (50.6) |
| Other ophthalmic drops 2nd L SA -> 3rd L SA 2nd L SA -> 3rd L COMB 2nd L COMB -> 3rd L SA | 28 (36.4)
| |||
| Trabeculoplasty | 10 (13.0) |
| Patients with Glaucoma (N = 18,161) | ||
|---|---|---|
| N | % | |
| Adherence to treatment | ||
| PDC ≥ 80 | 10,581 | 58.3 |
| 40 ≤ PDC < 80 | 4651 | 25.6 |
| PDC < 40 | 2928 | 16.1 |
| Persistence to treatment | 14,179 | 78.1 |
| Discontinuation to treatment | 10,685 | 58.8 |
| Interruption | 3982 | 21.9 |
| Switch | 7605 | 41.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrone, V.; Formica, D.; Piergentili, B.; Rossetti, L.; Degli Esposti, L. Real-World Analysis on the Characteristics, Therapeutic Paths and Economic Burden for Patients Treated for Glaucoma in Italy. Healthcare 2023, 11, 635. https://doi.org/10.3390/healthcare11050635
Perrone V, Formica D, Piergentili B, Rossetti L, Degli Esposti L. Real-World Analysis on the Characteristics, Therapeutic Paths and Economic Burden for Patients Treated for Glaucoma in Italy. Healthcare. 2023; 11(5):635. https://doi.org/10.3390/healthcare11050635
Chicago/Turabian StylePerrone, Valentina, Dario Formica, Benedetta Piergentili, Luca Rossetti, and Luca Degli Esposti. 2023. "Real-World Analysis on the Characteristics, Therapeutic Paths and Economic Burden for Patients Treated for Glaucoma in Italy" Healthcare 11, no. 5: 635. https://doi.org/10.3390/healthcare11050635