
Impact of the COVID-19 Pandemic on Dermatology Care in the Chilean Public Health Sector

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Ethical Considerations
3. Results
3.1. Consultations by Region during 2020
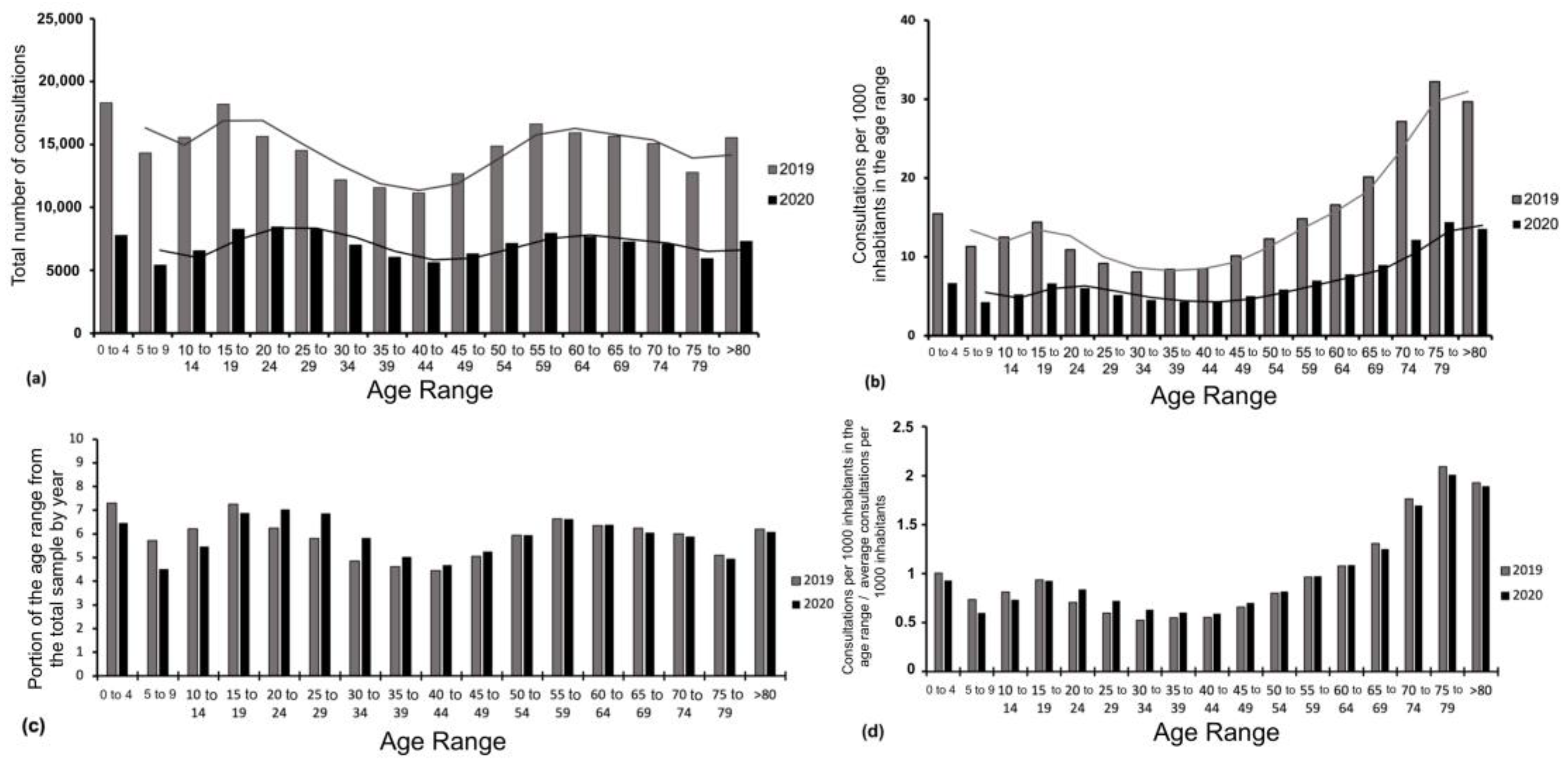
3.2. Consultations by Age Range in 2019 Versus 2020
3.3. Temporal Sequence of Consultations in 2020
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-NCoV). Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 21 August 2021).
- World Health Organization. COVID-19 Weekly Epidemiological Update. Edition 93. Geneva; WHO 25 May 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---25-may-2022 (accessed on 20 June 2022).
- Jara, A.; Undurraga, E.A.; González, C.; Paredes, F.; Fontecilla, T.; Jara, G.; Pizarro, A.; Acevedo, J.; Leo, K.; Leon, F.; et al. Effectiveness of an Inactivated SARS-CoV-2 Vaccine in Chile. N. Engl. J. Med. 2021, 385, 875–884. [Google Scholar] [CrossRef] [PubMed]
- iCOVID Chile. Informe #80: Se Deterioran Sustantivamente los Indicadores de la Pandemia Durante Mayo, Aunque Casos Severos se Mantienen Bajos. Available online: https://uploads.strikinglycdn.com/files/38287195-03a6-48a6-952f-4bd85a9c6ae8/80,%20ICOVID,%20InformeF.pdf?id=3912013 (accessed on 20 June 2022).
- World Health Organization. COVID-19 Strategic Preparedness and Response Plan: Country Preparedness and Response Status for COVID-19. Geneva: WHO; March 16 2020. Available online: https://www.who.int/who-documents-detail/updated-country-preparedness-and-response-status-for-covid-19-as-of-16-march-2020 (accessed on 21 August 2021).
- Grebe, G.; Vélez, J.A.; Tiutiunnyk, A.; Aragón-Caqueo, D.; Fernández-Salinas, J.; Navarrete, M.; Laroze, D. Dynamic quarantine: A comparative analysis of the Chilean public health response to COVID-19. Epidemiol. Infect. 2020, 148, e270. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado, C.; Monsalves, M.J.; Gajardo, J.; Bertoglia, M.P.; Najera, M.; Alfaro, T.; Canals, M.; Kaufman, J.S.; Peña, S. Impact of Small-Area Lockdowns for the Control of the COVID-19 Pandemic. medRxiv. 2020. Available online: http://medrxiv.org/content/early/2020/05/09/2020.05.05.20092106.abstract (accessed on 21 August 2021).
- Ministerio de Salud de la república de Chile (MINSAL). Ministerio de Salud Confirma Primer caso de Coronavirus en Chile. Santiago de Chile, Marzo 3 del 2020. MINSAL. Available online: https://www.minsal.cl/ministerio-de-salud-confirma-primer-caso-de-coronavirus-en-chile/ (accessed on 21 August 2021).
- Ministerio de Salud de la República de Chile (MINSAL). COVID- 19: Subsecretario Alberto Dougnac Anunció Postergación de Cirugías Electivas Santiago de Chile, Marzo 16 del 2021. Available online: https://www.minsal.cl/covid-19-subsecretario-alberto-dougnac-anuncio-postergacion-de-cirugias-electivas/ (accessed on 2 September 2021).
- Nazzaro, G.; Marzano, A.V.; Berti, E. What is the role of a dermatologist in the battle against COVID-19? The experience from a hospital on the frontline in Milan. Int. J. Dermatol. 2020, 59, e238–e239. [Google Scholar] [CrossRef]
- Giacalone, S.; Bortoluzzi, P.; Nazzaro, G. Which are the “emergent” dermatologic practices during COVID-19 pandemic? Report from the lockdown in Milan, Italy. Int. J. Dermatol. 2020, 59, e269–e270. [Google Scholar] [CrossRef]
- Naderi-Azad, S.; Manion, R.; Alhusayen, R. Impact of COVID-19 on Access to Care: A National Patient Survey. J. Cutan. Med. Surg. 2021, 25, 453–455. [Google Scholar] [CrossRef]
- Ministerio de Salud de Chile. Subsecretaría de Redes Asistenciales: División de Gestión y Desarrollo de las Personas y Departamento de Estudios Planificación y Control de Gestión del Área de Personas. Informe Sobre Brechas de Personal de Salud en los Servicios de Salud y Estado de Situación de los Recursos Humanos de Salud en Chile. Santiago de Chile: Ministerio de Salud, Abril 2019. Available online: https://www.minsal.cl/wp-content/uploads/2019/06/Glosa-01-letra-i-ORD-1983.pdf (accessed on 27 August 2021).
- Mena Vergara, L.; Carrasco Cancino, C.; Rojas Pizarro, H.; Saavedra, W. Demografía y distribución de dermatólogos en Chile. Piel 2022, 37, 392–400. [Google Scholar] [CrossRef]
- Aragón-Caqueo, D.; Parrao, F.; Palacios, J.; Mora, F.; Correa, J.; Guglielmetti, A. Consultas a Dermatología en el sector público de salud en Chile en 2019. Rev. Chil. Derm. 2020, 36, 172–177. [Google Scholar] [CrossRef]
- Ministerio de Salud. Departamento de Estadísticas e Información de Salud. Sistema de Reportes REM: Atención de Especialidades Periodo 2020. Available online: https://reportesrem.minsal.cl/?_token=5lM3NvDeT0DvvX3PbfuupkJwuaslnG2PffgQSPTL&serie=1&rem=62&seccion_id=695&tipo=4&tipoReload=4®iones=-1®ionesReload=-1&servicios=0&serviciosReload=0&periodo=2019&mes_inicio=1&mes_final=12 (accessed on 15 December 2021).
- Instituto Nacional de Estadísticas. Síntesis de Resultados CENSO 2017, Junio 2018. Available online: https://www.censo2017.cl/descargas/home/sintesis-de-resultados-censo2017.pdf (accessed on 15 December 2021).
- Ministerio de Salud de Chile. COVID-19 en Chile. Pandemia 2020–2022 . In Hitos de la primera ola|COVID-19; Departamento de Comunicaciones y Relaciones Públicas del Ministerio de Salud: Santiago, Chile, 2022; pp. 96–98. Available online: https://www.minsal.cl/wp-content/uploads/2022/03/2022.03.03_LIBRO-COVID-19-EN-CHILE-1-1.pdf (accessed on 16 July 2022).
- Karadag, A.S.; Aslan Kayıran, M.; Wollina, U. How dermatology has changed in the COVID-19 pandemic. Clin. Dermatol. 2021, 39, 457–460. [Google Scholar] [CrossRef]
- Gisondi, P.; Piaserico, S.; Conti, A.; Naldi, L. Dermatologists and SARS-CoV-2: The impact of the pandemic on daily practice. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1196–1201. [Google Scholar] [CrossRef]
- Aragón-Caqueo, D.; Arceu Ojeda, M.; Aragón-Caqueo, G.; Zamora Aragón, K.; Tom Montalva, D.; Gatica Monsalve, J.L. Comparación del tiempo de espera de atención dermatológica mediante el uso de teledermatología y derivación presencial. Piel 2020, 35, 220–224. [Google Scholar] [CrossRef]
- Wang, R.; Helf, C.; Tizek, L.; Neuhauser, R.; Eyerich, K.; Zink, A.; Eberlein, B.; Biedermann, T.; Brockow, K.; Boehner, A. The impact and consequences of SARS-CoV-2 pandemic on a single university dermatology outpatient clinic in Germany. Int. J. Environ. Res. Public Health 2020, 17, 6182. [Google Scholar] [CrossRef] [PubMed]
- Marin, B.G.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Temiz, S.A.; Dursun, R.; Daye, M.; Ataseven, A. Evaluation of dermatology consultations in the era of COVID-19. Dermatol. Ther. 2020, 33, e13642. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud de la República de Chile (MINSAL). Presidente Declara Estado de Excepción Constitucional de Catástrofe en Todo el Territorio Nacional. Santiago de Chile, Marzo 18 del 2020. Available online: https://www.minsal.cl/presidente-declara-estado-de-excepcion-constitucional-de-catastrofe-en-todo-el-territorio-nacional/ (accessed on 1 September 2021).
- Kwatra, S.G.; Sweren, R.J.; Grossberg, A.L. Dermatology Practices as vectors for COVID-19 transmission: A call for immediate cessation of nonemergent dermatology visits. J. Am. Acad. Dermatol. 2020, 82, e179–e180. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud de la República de Chile (MINSAL). Departamento de Epidemiología. Informe Epidemiológico Nº25 Enfermedad por SARS-CoV-2 (COVID-19). Santiago. 2020. Available online: https://www.minsal.cl/wp-content/uploads/2020/06/Informe_EPI_120620.pdf (accessed on 4 September 2022).
- Goh, C.F.; Ming, L.C.; Wong, L.C. Dermatologic reactions to disinfectant use during the COVID-19 pandemic. Clin. Dermatol. 2021, 39, 314–322. [Google Scholar] [CrossRef]
- Shanshal, M.; Ahmed, H.S.; Asfoor, H.; Salih, R.I.; Ali, S.A.; Aldabouni, Y.K. Impact of COVID-19 on medical practice: A nationwide survey of dermatologists and health care providers in Iraq. Clin. Dermatol. 2021, 39, 500–509. [Google Scholar] [CrossRef]
- Gronbeck, C.; Grant-Kels, J.M.; Lu, J.; Feng, H. Increased Utilization of Teledermatology Among Medicare Part B Beneficiaries During the COVID-19 Pandemic. Clin. Dermatol. 2022, 40, 760–763. [Google Scholar] [CrossRef]
- Subsecretaría de Redes Asistenciales. Programa Nacional de Telesalud. 2018. Available online: http://www.minsal.cl/wp-content/uploads/2018/03/Programa-Nacional-de-Telesalud.pdf (accessed on 4 September 2021).
- Fuenzalida Cruz, H.; Jimeno Ortega, I.; Toso Díaz de la Vega, S.; Sepúlveda Muñoz, A.; Loubies Muñoz, R. Teledermatología: Impacto de una herramienta de gestión informática para zonas remotas de Chile. Piel 2017, 32, 257–262. [Google Scholar] [CrossRef]
- Gatica, J.L.; Bertoló, S.; Morales, E.; Espinoza, M.; Contreras, C. Teledermatología en Chile, un aporte a la atención primaria de salud. Piel 2015, 30, 148–154. [Google Scholar] [CrossRef]
- Aragón-Caqueo, D.; Arceu, M.; Aragón-Caqueo, G.; Zamora, K.; Tom, D.; Gatica, J.L. Teledermatología en Chile: Experiencia de su implementación temprana. Piel 2022, 37, 1–6. [Google Scholar] [CrossRef]
- Lopez-Liria, R.; Lopez-Villegas, A.; Valverde-Martinez, M.A.; Perez-Heredia, M.; Vega-Ramirez, F.A.; Peiro, S.; Leal-Costa, C. Comparative Analysis of Quality of Life of Patients with Dermatological Problems: Teledermatology Versus Face-to-Face Dermatology. Healthcare 2022, 10, 2172. [Google Scholar] [CrossRef] [PubMed]
- Trondsen, M.V. Managing Everyday Life: A Qualitative Study of Patients’ Experiences of a Web-Based Ulcer Record for Home-Based Treatment. Healthcare 2014, 2, 492–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rismiller, K.; Cartron, A.M.; Trinidad, J.C.L. Inpatient Teledermatology During the COVID-19 Pandemic. J. Dermatolog. Treat. 2020, 31, 441–443. [Google Scholar] [CrossRef]
- Elsner, P. Teledermatology in the times of COVID-19—A systematic review. J. Dtsch. Dermatol. Ges. 2020, 18, 841–845. [Google Scholar] [CrossRef]
- Gatica, J.L.; Aedo Inostroza, G.; Letelier, M.; Sabando, V.; Loubies, R.; Fuenzalida, H.; Aragón-Caqueo, D.; Martínez, G. Teledermatology in Chile: Implementation of a Single National System. J. Clin. Exp. Dermatol. Res. 2022, 13, 605. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aragón-Caqueo, D.; Aedo, G.; Suárez, J.; Toloza, C.; Guglielmetti, A. Impact of the COVID-19 Pandemic on Dermatology Care in the Chilean Public Health Sector. Healthcare 2023, 11, 633. https://doi.org/10.3390/healthcare11050633
Aragón-Caqueo D, Aedo G, Suárez J, Toloza C, Guglielmetti A. Impact of the COVID-19 Pandemic on Dermatology Care in the Chilean Public Health Sector. Healthcare. 2023; 11(5):633. https://doi.org/10.3390/healthcare11050633
Chicago/Turabian StyleAragón-Caqueo, Diego, Gabriel Aedo, Javier Suárez, Claudio Toloza, and Antonio Guglielmetti. 2023. "Impact of the COVID-19 Pandemic on Dermatology Care in the Chilean Public Health Sector" Healthcare 11, no. 5: 633. https://doi.org/10.3390/healthcare11050633