
Exploring Occupational Therapists’ Professional Identity: A Q-Method Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Development of the Q Sample
2.3. Selection of the P Set
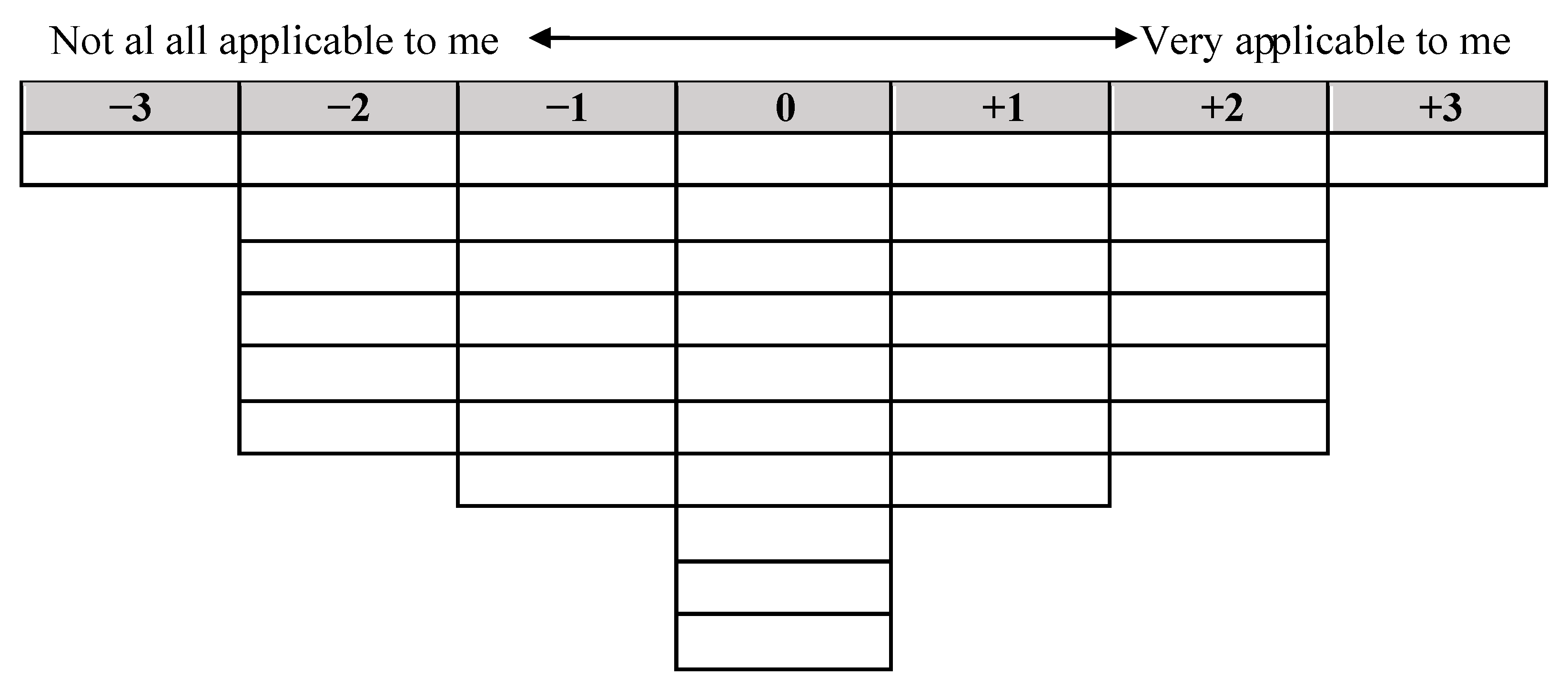
2.4. Q-Sort
2.5. Factor Extraction and Interpretation
- The starting point was the default number of factors extracted by the Ken-Q analysis software, a total of 8 factors.
- Factors with an eigenvalue greater than 1.0 were included.
- At least two significant factor loadings were required for each retained factor.
- The cross-product of the two highest loadings should be greater than twice the standard error (SE) (Humphrey’s rule). SE was calculated using the formula SE = 1/√n, where n = number of statements in the Q-set. Therefore, loadings of 2 × 1/√40 (factor loadings > 0.31623) identified Q-sorts correlated with each factor.
3. Results
3.1. Retained Factor 1: Viewpoint 1—Professional Identity Due to Mentors
3.2. Retained Factor 2: Viewpoint 2—A Grey Field on Professional Identity
3.3. Retained Factor 3: Viewpoint 3—Reaffirming a Common Professional Identity
3.4. Retained Factor 4: Viewpoint 4—The Role of Education and Mentors on the Own Professional Identity
3.5. Retained Factor 5: Viewpoint 5—The Outcome of Ongoing Training in Order to Develop a Professional Identity
4. Discussion
4.1. Before University Training
- (a)
- Personal: Mark et al. [52] described how personal relationships, social class, previous education, and social environmental factors can shape an individual’s professional identity. As a result of the multiplicity and interaction of these factors, it has been suggested that professional identity, even before starting university studies, follows its own path, which is determined by the person who chooses to study occupational therapy over other disciplines [50,53].
- (b)
- Family: As with other disciplines, such as nursing [52], studies included in the research by Mao et al. [54] suggest that family support is closely linked to the selection of a particular degree. Our study confirms that nursing students who have relatives working in the health sector express a higher interest in completing a certain training program [55,56,57].
- (c)
- Professional: Mark et al. [52] noted that clinical experience, role models (e.g., teaching staff, preceptors, and mentors), and exposure to the profession before formal training influence the establishment of a professional identity [5,50,53]. Rituals, rites of passage, and symbols in education and health institutions can also contribute to the creation of a professional identity [50].
- (d)
- (e)
- Gender: Finally, we believe that gender is a core element in the decision to study occupational therapy. Our sample corroborates that only 8% of occupational therapists are men, while 92% are women [58], and 10% are LGBT [59]. This situation is similar to that in other disciplines. Although occupational therapy has traditionally been considered a female-dominated occupation, it is experiencing an increase in the number of male professionals. However, this number is insufficient to achieve professional parity, contributing to the gender inequality present in most professions [60].
4.2. During University Training
4.3. After University Training
4.4. Limitations and Strengths of the Study
4.5. Future Lines
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walder, K.; Bissett, M.; Molineux, M.; Whiteford, G. Understanding professional identity in occupational therapy: A scoping review. Scand. J. Occup. Ther. 2022, 29, 175–197. [Google Scholar] [CrossRef]
- Dige, M. Occupational therapy, professional development, and ethics. Scand. J. Occup. Ther. 2009, 16, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Trede, F.; Macklin, R.; Bridges, D. Professional identity development: A review of the higher education literature. Stud. High. Educ. 2011, 37, 365–384. [Google Scholar] [CrossRef]
- Kahlke, R.M.; McConnell, M.M.; Wisener, K.M.; Eva, K.W. The disconnect between knowing and doing in health professions education and practice. Adv. Health Sci. Educ. 2020, 25, 227–240. [Google Scholar] [CrossRef]
- Ashby, S.E.; Adler, J.; Herbert, L. An exploratory international study into occupational therapy students’ perceptions of professional identity. Aust. Occup. Ther. J. 2016, 63, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Boehm, J.; Tanner, B.; Lowrie, D.; Bonassi, M.; Brown, N.; Thomas, Y.; Cordier, R. Exploring emerging occupational therapy identity and the development of graduate attributes among occupational therapy students. Br. J. Occup. Ther. 2015, 78, 499–507. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, M.; Smith, A.K.; Rehman, N.; Taylor, M. Role Emerging Placements in Undergraduate Occupational Study. Internet J. Allied Health Sci. Pract. 2017, 15, 7. [Google Scholar] [CrossRef]
- Ikiugu, M.N.; Rosso, H.N. Facilitating professional identity in Occupational therapy students. Occup. Ther. Int. 2003, 10, 206–225. [Google Scholar] [CrossRef]
- Herbert, L.; Ashby, S.E. An exploratory study into the formation of professional identity during an occupational therapy entry-level program. Aust. Occup. Ther. J. 2015, 62, 1440–1630. [Google Scholar] [CrossRef] [Green Version]
- Gray, H.; Colthorpe, K.; Ernst, H.; Ainscough, L. Professional Identity of UndergraduateOccupational Therapy Students. J. Occup. Ther. Educ. 2020, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Towns, E.; Ashby, S.E. The influence of practiceeducators on occupational therapy students’ understand-ing of the practical applications of theoretical knowledge: A phenomenological study into student experiences ofpractice education. Aust. Occup. Ther. J. 2014, 61, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Turipin, M.J.; Rodger, S.; Hall, A.R. Occupational therapy students’ perceptions of occupational therapy. Aust. Occup. Ther. J. 2012, 59, 367–374. [Google Scholar] [CrossRef]
- Hurley, J. A qualitative study of mental health nurse identities: Many roles, one profession. Int. J. Ment. Health Nurs. 2009, 18, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.E.; Monrouxe, L.V. Who are you and who do you want to be? Key considerations in developing professional identities in medicine. Med. J. Aust. 2018, 209, 202–203. [Google Scholar] [CrossRef]
- Jenkins, R. Social Identity, 4th ed.; Routeledge: London, UK, 2008; pp. 42–59. [Google Scholar]
- Zubriski, S.; Norman, M.; Shimmell, L.; Gewurtz, R.; Letts, L. Professional identity and emerging occupational therapy practice: An autoethnography. Can. J. Occup. Ther. 2020, 87, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Drolet, M.J.; Desormeaux-Moreau, M. The values of occupational therapy: Perceptions of occupational therapists in Quebec. Scandavian J. Occup. Ther. 2016, 23, 272–285. [Google Scholar] [CrossRef]
- Metaxas, V.A. Eleanor Clarke Slagle & Susan, E. Tracy: Personal and professional identity and the development of occupational therapy in Progressive Era America. Nurs. Hist. Rev. 2000, 8, 39–70. [Google Scholar] [CrossRef]
- Lecours, A.; Baril, N.; Drolet, M.J. What is Professionalism in Occupational Therapy? A Concept Analysis. Can. J. Occup. Ther. 2021, 88, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Hoeve, Y.; Jansen, G.; Roodbol, P. The nursing profession: Public image, self-concept and professional identity. A discussion paper. J. Adv. Nurs. 2014, 70, 295–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arreciado, A.; Isla, M.P. Theory and practice in the construction of professional identity in nursing students: A qualitative study. Nurse Educ. Today 2015, 35, 859–863. [Google Scholar] [CrossRef] [Green Version]
- Eagle, I.T.; Hohneck, S.L.; VanDuine, S.M.; Fitzgerald, M.; Kinney, J.S. Factors Influencing the Professional Identity of Student and Licensed Professional Members of the American Dental Hygienists’ Association. J. Dent. Hyg. 2022, 96, 52–61. Available online: https://jdh.adha.org/content/96/5/52 (accessed on 14 December 2022). [PubMed]
- Dawodu, P.; Rutter, P. How Do Pharmacists Construct, Facilitate and Consolidate Their Professional Identity? Pharmacy 2016, 4, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindquist, I.; Engardt, M.; Garnham, L.; Poland, F.; Richardson, B. Physiotherapy students’ professional identity on the edge of working life. Med. Teach. 2006, 28, 270–276. [Google Scholar] [CrossRef]
- Hammond, R.; Cross, V.; Moore, A. The construction of professional identity by physiotherapists: A qualitative study. Physiotherapy 2016, 102, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.; Knight, J. A debate on the professional identity of occupational therapists. Br. J. Occup. Ther. 2015, 78, 664–673. [Google Scholar] [CrossRef]
- Guru, R.; Siddiqui, M.A.; Rehman, A. Professional identity (role blurring) of occupational therapy in community mental health in India. ISRA Med. J. 2013, 5, 155–159. [Google Scholar]
- Fanshawe, E. The importance of rehabilitiation to disabled people. The Dr Elizabeth Casson Memorial Lecture. Br. J. Occup. Ther. 1981, 44, 194–197. [Google Scholar] [CrossRef]
- Godber, G. Interpretational relationships in the Health Service. The Dr Elizabeth Casson Memorial Lecture. Br. J. Occup. Ther. 1973, 36, 396–403. [Google Scholar] [CrossRef]
- Grant, A. The effect of the use of discretion on occupational therapists’ professional identity. Br. J. Occup. Ther. 2013, 76, 409–417. [Google Scholar] [CrossRef] [Green Version]
- Zambonini, M.C. Terapia ocupacional e Identidade Profissional: É Possível Visualizar Mudanças nas Últimas Décadas? Ph.D. thesis, Instituto de Saúde e Sociedade, Universidade Federal de São Paulo, São Paulo, Brazil, 2022. [Google Scholar]
- Fortune, T. Occupational therapists: Is our therapy truly occupational or are we merely filling gaps? Br. J. Occup. Ther. 2000, 63, 225–230. [Google Scholar] [CrossRef]
- Lundberg, A.; De Leeuw, R.; Aliani, R. Using Q methodology: Sorting out subjectivity in educational research. Educ. Res. Rev. 2020, 31, 100361. [Google Scholar] [CrossRef]
- Brown, S.R. A primer on Q methodology. Operant. Subj. 1993, 16, 91–138. [Google Scholar] [CrossRef]
- Smith, N. Current Systems in Psychology: History, Theory, Research and Application; Wadsworth/Thomson Learning: Belmont, CA, USA, 2001; p. 430. [Google Scholar]
- Garbellini, S.; Randall, M.; Steele, M.; Elliott, C.; Imms, C. Unpacking the application of Q methodology for use in occupational therapy research. Scand. J. Occup. Ther. 2020, 28, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.C.; Xiao, X.; Nkambule, N.; Ngerng, R.; Bullock, A.; Monrouxe, L.V. Exploring emergency physicians’ professional identities: A Q-method study. Adv. Health Sci. Educ. Theory Pract. 2021, 26, 117–138. [Google Scholar] [CrossRef]
- Brown, S.R. Q Methodology and Qualitative Research. Qual. Health Res. 1996, 6, 561–567. [Google Scholar] [CrossRef]
- Alderson, S.; Foy, R.; Bryant, L.; Ahmed, S.; House, A. Using Q-methodology to guide the implementation of new healthcare policies. BMJ Qual. Saf. 2018, 27, 737–742. [Google Scholar] [CrossRef]
- Márquez-Álvarez, L.J.; Calvo-Arenillas, J.I.; Jiménez-Arberas, E.; Talavera-Valverde, M.A.; Souto-Gómez, A.I.; Moruno-Miralles, P. A Q-Method Approach to Perceptions of Professional Reasoning in Occupational Therapy Undergraduates. BMC Med. Educ. 2021, 21, 264. [Google Scholar] [CrossRef]
- Talavera, M.A. Razonamiento Clínico y Diagnostico en Terapia Ocupacional, 1st ed.; Síntesis: Madrid, Spain, 2015; pp. 33–66. [Google Scholar]
- Edwards, H.; Dirette, D. The Relationship between Professional Identity and Burnout among Occupational Therapists. Occup. Ther. Health Care 2010, 24, 119–129. [Google Scholar] [CrossRef]
- Matthews, J.; Bialocerkowski, A.; Molineux, M. Professional identity measures for student health professionals—A systematic review of psychometric properties. BMC Med. Educ. 2019, 19, 308. [Google Scholar] [CrossRef] [Green Version]
- Garbellini, S.; Randall, M.; Steele, M.; Elliott, C.; Imms, C. Prescribing upper limb orthoses for children with cerebral palsy: A Q methodology study of occupational therapists’ decision making. Disabil. Rehabil. 2020, 42, 2600–2610. [Google Scholar] [CrossRef]
- Watts, S.; Stenner, P. Doing Q methodology: Theory, method and interpretation. Qual. Res. Psychol. 2005, 2, 67–91. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.R. Q Methodology. In The SAGE Encyclopedia of Qualitative Research Methods, 1st ed.; Given, L.M., Ed.; Sage: Newcastle, UK, 2008; pp. 699–712. [Google Scholar]
- Chee, D.Y.; Lee, H.C.; Patomella, A.H.; Falkmer, T. Driving Behaviour Profile of Drivers with Autism Spectrum Disorder (ASD). J. Autism Dev. Disord. 2017, 47, 2658–2670. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Elliott, C.; Willis, C.; Ward, R.; Falkmer, M.; Falkmer, T.; Gubbay, A.; Girdler, S. Can, Want and Try: Parents’ Viewpoints Regarding the Participation of Their Child with an Acquired Brain Injury. PLoS ONE 2016, 11, e0157951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, S.; Williams, S. Professional identity in interprofessional teams: Findings from a scoping review. J. Interprof. Care 2018, 33, 170–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monrouxe, L.V. Identity, identification and medical education: Why should we care? Med. Educ. 2010, 44, 40–49. [Google Scholar] [CrossRef]
- Vignoles, V.L.; Schwartz, S.J.; Luyckx, K. Introduction: Toward an integrative view of identity. In Handbook of Identity Theory and Research, 1st ed.; Schwartz, S.J., Luyckx, K., Vignoles, V.L., Eds.; Springer: New York, NY, USA, 2011; pp. 1–27. [Google Scholar]
- Mark, S.; Hunt, M.; Boruff, J.; Zaccagnini, M.; Thomas, A. Exploring professional identity in rehabilitation professions: A scoping review. Adv. Health Sci. Educ. Theory Pract. 2022, 27, 793–815. [Google Scholar] [CrossRef]
- Cruess, S.R.; Cruess, R.L.; Steinert, Y. Supporting the development of a professional identity: General principles. Med. Teach. 2019, 41, 641–649. [Google Scholar] [CrossRef]
- Mao, A.; Lu, S.E.; Lin, Y.; He, M. A scoping review on the influencing factors and development process of professional identity among nursing students and nurses. J. Prof. Nurs. 2020, 37, 391–398. [Google Scholar] [CrossRef]
- Fan, Z.H.; Wang, X.Y.; Hou, R.P. A survey on the professional identity status and influencing factors among baccalaureate nursing students in Henan Province. Health Vocat. Educ. 2018, 36, 126–127. [Google Scholar]
- Gao, H. An exploration on the professional identity levels and influencing factors among 921 clinical nurses from 20 hospitals in Shanghai. J. Nurs. 2013, 20, 27–30. [Google Scholar] [CrossRef]
- Tian, Y.X.; Zhu, J.H.; Zhang, L. Professional identity of nursing students in Ningxia province and its influencing factors. J. Nurs. Sci. 2012, 27, 69–70. [Google Scholar] [CrossRef]
- Workforce Trends in Occupational Therapy. Available online: https://www.aota.org/-/media/corporate/files/educationcareers/prospective/workforce-trends-in-ot.pdf (accessed on 14 December 2022).
- ZIPPIA. Occupational Therapist Demographics and Statistics in the USA. Available online: https://www.zippia.com/occupational-therapist-jobs/demographics/ (accessed on 12 December 2022).
- Collins, J. A Female’s Profession: Gender Disparity in Occupational Therapy. Ph.D. Thesis, Eastern Kentucky University, Richmond, KY, USA, 2019. [Google Scholar]
- Khodaei, A.; Mansourian, M.; Ganjei, S.; Asgari, H. Strategies for decreasing gap between theory & clinical performance from the viewpoints of nursing students in Tabriz university of medical sciences. Res. Med. Educ. 2016, 8, 49–59. [Google Scholar]
- Shaterjalali, M.; Nikoo, Y.; Changiz, T. Who are the right teachers for medical clinical students? Investigating stakeholders’ opinions using modified Delphi approach. Adv. Med. Educ. Pract. 2018, 9, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashby, S.E.; Ryan, S.; Gray, M.; James, C. Factors that influence the professional resilience of occupational therapists in mental health practice. Aust. Occup. Ther. J. 2013, 60, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Hodgetts, S.; Hollis, V.; Triska, O.; Dennis, S.; Madill, H.; Taylor, E. Occupational therapy students’ and graduates’ satisfaction with professional education and preparedness for practice. Can. J. Occup. Ther. 2007, 74, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Pillen, M.; Beijaard, D.; Brok, P.D. Tensions in beginning teachers’ professional identity development, accompanying feelings and coping strategies. Eur. J. Teach. Educ. 2013, 36, 240–260. [Google Scholar] [CrossRef]
- Volkmann, M.J.; Anderson, M.A. Creating professional identity: Dilemmas and metaphors of a first-year chemistry teacher. Sci. Educ. 1998, 82, 293–310. [Google Scholar] [CrossRef]
- Holland, K.E.; Middleton, L.; Uys, L. Professional Confidence: Conceptions Held by Novice Occupational Therapists in South Africa. Occup. Ther. Int. 2013, 20, 105–113. [Google Scholar] [CrossRef]
- Cusick, A.; McIntosh, D.; Santiago, L. New graduate therapists in acute care hospitals: Priorities, problems and strategies for departmental action. Aust. Occup. Ther. J. 2004, 51, 174–184. [Google Scholar] [CrossRef]
- Lee, S.; Mackenzie, L. Starting out in rural New South Wales: The experiences of new graduate occupational therapists. Aust. J. Rural. Health 2003, 11, 36–43. [Google Scholar] [CrossRef]
- Morley, M. Developing a preceptorship programme for newly qualified occupational therapists: Action research. Br. J. Occup. Ther. 2007, 70, 330–338. [Google Scholar] [CrossRef]
- Tryssenaar, J.; Perkins, J. From student to therapist: Exploring the first year of practice. Am. J. Occup. Ther. 2001, 55, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Robertson, L.J.; Griffiths, S. Graduates’ reflections on their preparation for practice. Br. J. Occup. Ther. 2009, 72, 125–132. [Google Scholar] [CrossRef]
- Pang, M. Two faces of variation: On continuity in the phenomenographic movement. Scand. J. Educ. Res. 2003, 47, 145–156. [Google Scholar] [CrossRef]
- Ibarra, H. Provisional selves: Experimenting with image and identity in professional adaptation. Adm. Sci. Q. 1999, 44, 764–791. [Google Scholar] [CrossRef] [Green Version]
- Goldie, J. The formation of professional identity in medical students: Considerations for educators. Med. Teach. 2012, 34, e641–e648. [Google Scholar] [CrossRef] [Green Version]
- Mackey, H. Do not ask me to remain the same: Foucault and the professional identities of occupational therapists. Aust. Occup. Ther. J. 2007, 54, 95–102. [Google Scholar] [CrossRef]
- Sauvageau, A.; Drolet, M.J.; Gohier, C. Le développement identitaire de l’ergothérapeute éclairé par un modèle de construction de l’identité professionnelle de l’enseignant. Ergotherapies 2017, 67, 71–80. [Google Scholar]
- Jung, B.F. The Professional Master’s Occupational Therapist: Developing an Emerging Professional Identity. Ph.D. Thesis, University of Western Ontario, London, ON, Canada, 2010. [Google Scholar]
- Davis, J.L. In Search of an Identity: Occupational Therapy Students’ Images of Practice. Ph.D. Thesis, University of Kansas, Lawrence, KS, USA, 2005. [Google Scholar]
- Hayward, L.M.; Li, L. Promoting and assessing cultural competence, professional identity, and advocacy in doctor of physical therapy (DPT) degree students within a community of practice. J. Phys. Ther. Educ. 2014, 28, 23–36. [Google Scholar] [CrossRef]
- Lahav, O.; Daniely, N.; Yalon-Chamovitz, S. Interpersonal social responsibility model of service learning: A longitudinal study. Scand. J. Occup. Ther. 2018, 25, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Binyamin, G. Strategies for resolving relational dilemmas while developing therapists’ professional identity. Adv. Health Sci. Educ. 2021, 26, 827–845. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.G.; Kim, M. Collaborative reflection through dilemma cases of science practical work during practicum. Int. J. Sci. Educ. 2010, 32, 283–301. [Google Scholar] [CrossRef]
- Glenn, E.K.; Gilbert-Hunt, S. New graduate occupational therapists experience of showering assessments: A phenomenological study. Aust. Occup. Ther. J. 2012, 59, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Schott, C.; Van Kleef, D.D.; Steen, T.P. The combined impact of professional role identity and public service motivation on decision-making in dilemma situations. Int. Rev. Adm. Sci. 2018, 84, 21–41. [Google Scholar] [CrossRef]
- Kielhofner, G. Dimensions of doing. In Model of Human Occupation, 3rd ed.; Kielhofner, G., Ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2002; pp. 124–144. [Google Scholar]
- Unruh, A.M. So… what do you do? Occupation and the construction of identity. Can. J. Occup. Ther. 2004, 5, 291–295. [Google Scholar] [CrossRef]
- Pratt, M.G.; Corley, K.G. Organizational identities: On identity ambiguity, identity conflict and members’ reactions. In On Identity and the Modern Organization, 2nd ed.; Bartel, C., Blader, S.L., Wrzesniewski, A., Eds.; Psychology Press & Routledge Classic Editions: London, UK, 2012; pp. 99–118. [Google Scholar]
- Seah, C.H.; Mackenzie, L.; Gamble, J. Transition of graduates of the Master of Occupational Therapy to practice. Aust. Occup. Ther. J. 2011, 58, 103–110. [Google Scholar] [CrossRef]
- Moores, A.; Fitzgerald, C. New graduate transition to practice: How can the literature inform support strategies? Aust. Health Rev. 2016, 41, 308–312. [Google Scholar] [CrossRef]
- Fortune, T.; Ryan, S.; Adamson, L. Transition to practice in supercomplex environments: Are occupational therapy graduates adequately prepared? Aust. Occup. Ther. J. 2013, 60, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Pilling, S. Supporting the transition from student to professional—A case study in allied health. Aust. Health Rev. 2008, 32, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Warmington, S.; McColl, G. Medical student stories of participation in patient care-related activities: The construction of relational identity. Adv. Health Sci. Educ. 2017, 22, 147–163. [Google Scholar] [CrossRef]
- Bleakley, A.; Bligh, J. Students learning from patients: Let’s get real in medical education. Adv. Health Sci. Educ. 2008, 13, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Dvir, N.; Avissar, I. Constructing a critical professional identity among teacher candidates during service-learning. Prof. Dev. Educ. 2014, 40, 398–415. [Google Scholar] [CrossRef]
- Willetts, G.; Clarke, D. Constructing nurses’ professional identity through social identity theory. Int. J. Nurs. Pract. 2014, 20, 164–169. [Google Scholar] [CrossRef]
- Covell, C.L.; Neiterman, E.; Bourgealut, E. Scoping review about the professional integration of internationally educated health profession. Hum. Resour. Health 2016, 14, 38. [Google Scholar] [CrossRef] [Green Version]
- Wattson, R. Construcción de la identidad profesional. TOG 2008, 5, 48–62. [Google Scholar]
- Benner, P.E. From Novice to Expert: Excellence and Power in Clinical Nursing Practice, 1st ed.; Prentice Hall: Hoboken, NJ, USA, 2000; pp. 62–81. [Google Scholar]
- Schell, B.A.; Schell, J.W. Clinical and Professional Reasoning in Occupational Therapy, 2nd ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2008; pp. 252–300. [Google Scholar]
- Moruno, P. Razonamiento Clínico en Terapia Ocupacional: Un Análisis del Procedimiento Diagnóstico. Ph.D. Thesis, University Autonoma de Madrid, Madrid, Spain, 2022. [Google Scholar]


{kind=link}
| No. | Statement |
|---|---|
| Group 1. Longitudinal statements | |
| 1 | I think professional identity is a relevant factor during the training for professional practice. |
| 2 | I think occupational therapy is too diverse to have a distinctive professional identity |
| 3 | I would prefer that occupational therapy had a clearer definition |
| 4 | I feel confident when describing occupational therapy |
| 5 | I consider that overcoming challenging situations and/or experiences fosters professional growth |
| 6 | Working as an occupational therapist makes me happy |
| 7 | I have developed a clear professional identity |
| 8 | I am still searching for my professional identity |
| 9 | I know whom I am professionally speaking |
| 10 | I still do not know which is my professional identity |
| Group 2. Influences before occupational therapy education | |
| 11 | I knew the nature of the tasks performed in my future career |
| 12 | In most working environments, professionals from different disciplines work together |
| 13 | I personally knew some professionals from my future working field |
| 14 | I followed the updates regarding my professional field in newspapers, TV, social media, events, etc. |
| 15 | My decision to study and become an occupational therapist was influenced |
| 16 | I chose my preferred career regardless of other people’s feedback |
| 17 | My knowledge of the profession of occupational therapy was sourced from a person I knew |
| 18 | I considered I should take into account both my own ideal and my surrounding factors during the election process of my career |
| 19 | I was sure I was successful in occupational therapy |
| 20 | I knew the different skills of the professional categories with which I was going to cooperate |
| Group 3. Influences during occupational therapy studies | |
| 21 | I knew what type of therapies were going to be part of my working activity |
| 22 | I knew what type of environments would be part of my working activity |
| 23 | I knew what type of tasks would be part of my working activity |
| 24 | When working on problems in class, I put myself in the shoes of an occupational therapist professional |
| 25 | During my last years of training, I already applied the professional reasoning of an occupational therapist |
| 26 | I admired the occupational therapists/educators in the areas I thought I was going to work in |
| 27 | I was confident I could carry out an excellent job in occupational therapy |
| 28 | I was positive I mastered all the required skills to be successful in my career |
| 29 | When starting my occupational therapy studies, I had a strong identity of becoming an occupational therapist |
| 30 | I was ashamed to admit I was studying occupational therapy |
| Group 4. Influences while working | |
| 31 | I do not feel sufficiently trained to work as an occupational therapist |
| 32 | I think I will easily perform my tasks as a professional therapist |
| 33 | I like working as a professional therapist |
| 34 | I think I have spent too long training to become a professional therapist |
| 35 | I try to learn about the scene of another professional field to strengthen my professional belief |
| 36 | I feel a member of this professional group |
| 37 | I can positively identify with other occupational therapists |
| 38 | I feel I share some features with other members of this professional group |
| 39 | I feel like giving excuses for belonging to this profession |
| 40 | I take advantage of my skills as an occupational therapist |
| Q-Sort | Age | Genre | YEX | APOT | Field of Expertise |
|---|---|---|---|---|---|
| 2 | 33 | Male | 11 | 0 | Pediatrics |
| 9 | 33 | Female | 11 | 5 | Pediatrics |
| 13 | 26 | Female | 1 | 2 | Pediatrics |
| 29 | 23 | Female | 1 | 0 | Geriatrics |
| 6 | 24 | Female | 1 | 1 | Neurorrehabilitation |
| 7 | 29 | Female | 6 | 1 | Community |
| 11 | 39 | Female | 18 | 17 | Various |
| 25 | 30 | Female | 9 | 0 | Geriatrics |
| 30 | 26 | Female | 4 | 0 | Geriatrics |
| 34 | 35 | Male | 10 | 5 | Geriatrics |
| 4 | 23 | Female | 0 | 1 | Neurorrehabilitation |
| 5 | 40 | Female | 18 | 15 | Geriatrics |
| 8 | 25 | Female | 3 | 0 | Geriatrics |
| 10 | 31 | Female | 8 | 5 | Mental health |
| 18 | 40 | Female | 18 | 2 | Geriatrics |
| 19 | 53 | Female | 17 | 18 | Geriatrics |
| 22 | 38 | Female | 16 | 4 | Various |
| 23 | 23 | Female | 0 | 0 | Geriatrics |
| 26 | 37 | Female | 16 | 0 | Various |
| 27 | 37 | Female | 16 | 16 | Mental health |
| 28 | 24 | Female | 1 | 2 | Geriatrics |
| 31 | 30 | Female | 8 | 9 | Mental health |
| 33 | 38 | Female | 18 | 0 | Mental health |
| 3 | 56 | Female | 29 | 30 | Mental health |
| 15 | 24 | Female | 2 | 3 | Various |
| 17 | 38 | Female | 17 | 2 | Geriatrics |
| 32 | 39 | Female | 13 | 13 | Mental health |
| 35 | 44 | Female | 18 | 18 | Geriatrics |
| 36 | 50 | Female | 25 | 0 | Various |
| 37 | 29 | Female | 7 | 5 | Various |
| 20 | 35 | Female | 12 | 11 | Geriatrics |
| 24 | 42 | Female | 20 | 11 | Various |
| 1 | 53 | Female | 3 | 1 | Geriatrics |
| 14 | 45 | Female | 6 | 6 | Various |
| 12 | 26 | Female | 3 | 4 | Pediatrics |
| 21 | 37 | Female | 13 | 2 | Geriatrics |
| Selection criteria | ||||||||
|---|---|---|---|---|---|---|---|---|
| Default factors | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Eigenvalue (value needed >1.0) | 15.31 | 3.20 | 2.19 | 1.95 | 1.63 | 1.38 | 1.26 | 1.16 |
| % explained variance | 41 | 9 | 6 | 5 | 4 | 4 | 3 | 3 |
| Number of factor loading > 0.31623 | 4 | 6 | 13 | 7 | 2 | 2 | 1 | 2 |
| Humphrey’s rule succeeded | Y | Y | Y | Y | Y | Y | N | Y |
| More than 2 factors with p < 0.05 | Y | Y | Y | Y | Y | N | - | N |
| Statement | V1 | V2 | V3 | V4 | V5 | |
|---|---|---|---|---|---|---|
| 1 | I think professional identity is a relevant factor during the training for professional practice. | +2 | +2 | +2 | +2 | +2 |
| 2 | I think occupational therapy is too diverse to have a distinctive professional identity | 0 | +1 | 0 | −1 b | +1 |
| 3 | I would prefer that occupational therapy had a clearer definition | +2 | +2 | +1 | −2 a | +2 |
| 4 | I feel confident when describing occupational therapy | +1 | 0 | +1 | +1 | 0 |
| 5 | I consider that overcoming challenging situations and/or experiences fosters professional growth | +1 | +2 | +2 | +1 | +2 |
| 6 | Working as an occupational therapist makes me happy | 0 | 0 | +1 e | +1 | 0 |
| 7 | I have developed a clear professional identity | 0 | −2 b | +1 | 0 | 0 |
| 8 | I am still searching for my professional identity | +1 | +2 | 0 | −1 b | +1 |
| 9 | I know whom I am professionally speaking | −1 | 0 | +1 | 0 | +2 |
| 10 | I still do not know which is my professional identity | −1 | +1 | −2 | −1 | 0 |
| 11 | I knew the nature of the tasks performed in my future career | −2 b | 0 | 0 | 0 | −1 |
| 12 | In most working environments, professionals from different disciplines work together | −1 a | +2 | +1 c | +1 | +2 |
| 13 | I personally knew some professionals from my future working field | +2 d | −2 | −1 | −2 | −2 |
| 14 | I followed the updates regarding my professional field in newspapers, TV, social media, events, etc. | +1 | −1 | −2 | −2 | 0 |
| 15 | My decision to study and become an occupational therapist was influenced | +1 c | −3 | −2 | −2 | 1 d |
| 16 | I chose my preferred career regardless of other people’s feedback | +3 | +1 | 0 | +3 | 0 |
| 17 | My knowledge of the profession of occupational therapy was sourced from a person I knew | +2 d | −2 | −1 | −2 | −2 |
| 18 | I considered I should take into account both my own ideal and my surrounding factors during the election process of my career | −2 | +1 | 0 | 0 | −1 |
| 19 | I was sure I was successful in occupational therapy | +2 d | 0 | 0 | −1 | 0 |
| 20 | I knew the different skills of the professional categories with which I was going to cooperate | −1 a | −1 | 0 | −1 | 0 |
| 21 | I knew what type of therapies were going to be part of my working activity | −2 | −1 | −1 | 0 | −1 |
| 22 | I knew what type of environments would be part of my working activity | −2 | −1 | −1 | +1 d | −1 |
| 23 | I knew what type of tasks would be part of my working activity | −1 | 0 | 0 | 0 | −2 |
| 24 | When working on problems in class, I put myself in the shoes of an occupational therapist professional | +1 | +3 e | −1 c | +2 | −2 a |
| 25 | During my last years of training, I already applied the professional reasoning of an occupational therapist | −1 | 0 | −2 | 0 | −1 |
| 26 | I admired the occupational therapists/educators in the areas I thought I was going to work in | +1 | 0 | −1 | +2 | 0 |
| 27 | I was confident I could carry out an excellent job in occupational therapy | 0 | −1 | 0 | +1 | 0 |
| 28 | I was positive I mastered all the required skills to be successful in my career | 0 | −2 | −1 | +1 | 0 |
| 29 | When starting my occupational therapy studies, I had a strong identity of becoming an occupational therapist | 0 | −2 a | −1 f | 0 | +2 d |
| 30 | I was ashamed to admit I was studying occupational therapy | 0 d | −2 | −2 | −3 | −2 |
| 31 | I do not feel sufficiently trained to work as an occupational therapist | 0 | +1 | −2 | −1 | −2 |
| 32 | I think I will easily perform my tasks as a professional therapist | −1 | 0 | 0 | 0 | +1 |
| 33 | I like working as a professional therapist | +1 | +1 | +2 | +2 | +1 |
| 34 | I think I have spent too long training to become a professional therapist | −3 a | 0 | 1 | −1 c | +3 d |
| 35 | I try to learn about the scene of another professional field to strengthen my professional belief | −2 | +1 | +1 | −1 | −1 |
| 36 | I feel a member of this professional group | +2 | −1 | +3 | +2 | −1 |
| 37 | I can positively identify with other occupational therapists | +1 | +1 | +2 e | +1 | −1 |
| 38 | I feel I share some features with other members of this professional group | 0 | +1 | +2 | +2 | +1 |
| 39 | I feel like giving excuses for belonging to this profession | −2 | −1 e | −3 | −2 | −3 |
| 40 | I take advantage of my skills as an occupational therapist | 0 | −1 | +2 | 0 | +1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souto-Gómez, A.-I.; Talavera-Valverde, M.-Á.; García-de-la-Torre, M.-d.-P.; Márquez-Álvarez, L.-J. Exploring Occupational Therapists’ Professional Identity: A Q-Method Study. Healthcare 2023, 11, 630. https://doi.org/10.3390/healthcare11040630
Souto-Gómez A-I, Talavera-Valverde M-Á, García-de-la-Torre M-d-P, Márquez-Álvarez L-J. Exploring Occupational Therapists’ Professional Identity: A Q-Method Study. Healthcare. 2023; 11(4):630. https://doi.org/10.3390/healthcare11040630
Chicago/Turabian StyleSouto-Gómez, Ana-Isabel, Miguel-Ángel Talavera-Valverde, María-del-Pilar García-de-la-Torre, and Luis-Javier Márquez-Álvarez. 2023. "Exploring Occupational Therapists’ Professional Identity: A Q-Method Study" Healthcare 11, no. 4: 630. https://doi.org/10.3390/healthcare11040630