
Clinical Consequences for Individuals Treated with Tocilizumab for Serious COVID-19 Infection
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Subjects and Methods
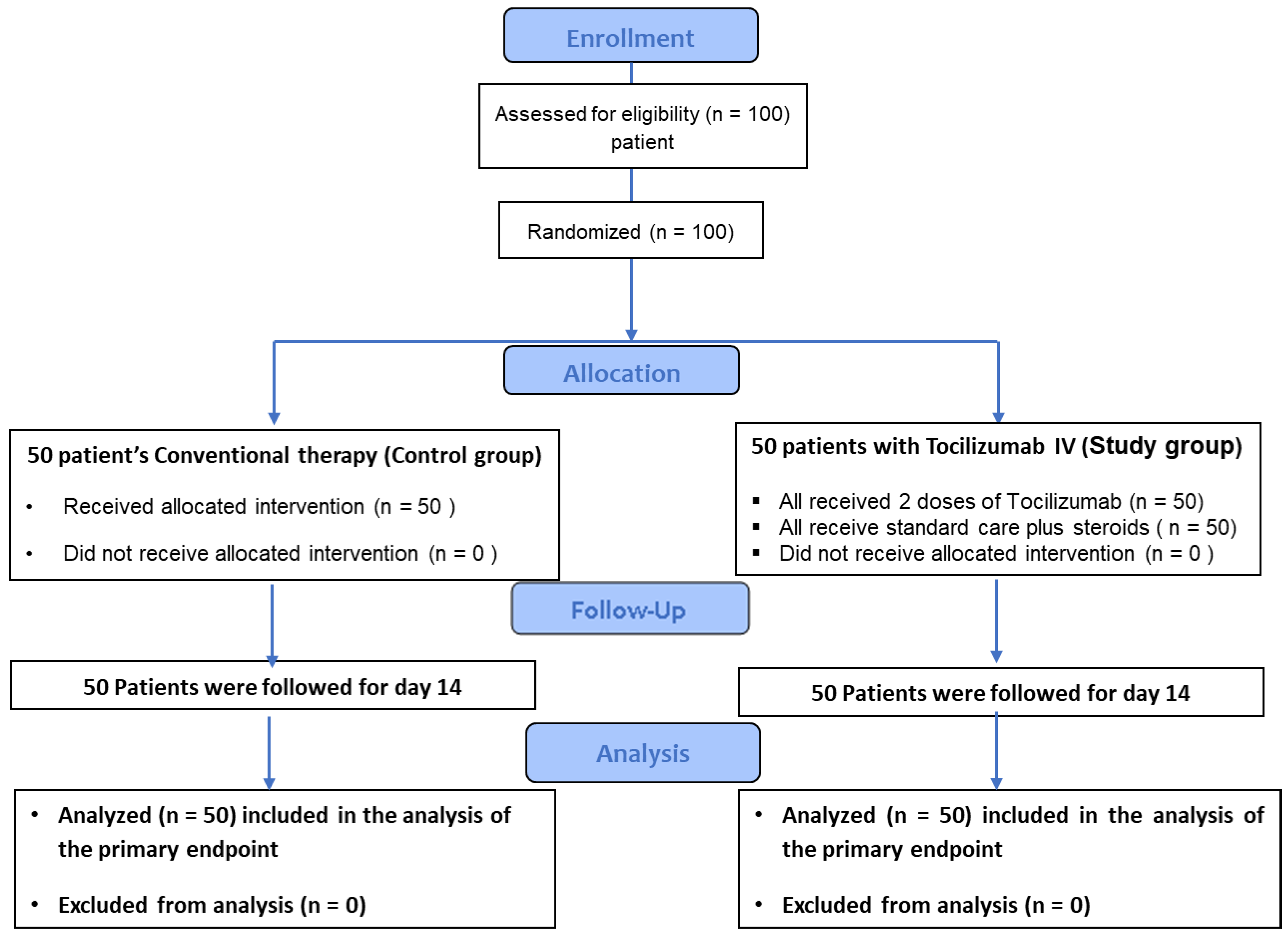
2.1. Study Design
2.2. Participants
2.3. Outcomes
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hussein, R.R.; Shaman, M.B.; Shaaban, A.H.; Fahmy, A.M.; Sofy, M.R.; Lattyak, E.A.; Abuelhana, A.; Naguib, I.A.; Ashour, A.M.; Aldeyab, M.A. Antibiotic consumption in hospitals during COVID-19 pandemic: A comparative study. J. Infect. Dev. Ctries. 2022, 16, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Stratton, C.W.; Tang, Y.W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.-Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Lu, P.; Fan, Y.; Xia, Y.; Liu, M. The clinical characteristics of pneumonia patients coinfected with 2019 novel coronavirus and influenza virus in Wuhan, China. J. Med. Virol. 2020, 92, 1549–1555. [Google Scholar] [CrossRef] [PubMed]
- Sofy, M.R.; Mancy, A.G.; Alnaggar, A.E.A.M.; Refaey, E.E.; Mohamed, H.I.; Elnosary, M.E.; Sofy, A.R. A polishing the harmful effects of Broad Bean Mottle Virus infecting broad bean plants by enhancing the immunity using different potassium concentrations. Not. Bot. Horti Agrobot. Cluj-Napoca 2022, 50, 12654. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe 2020, 27, 992–1000.e1003. [Google Scholar] [CrossRef]
- Aziz, M.; Fatima, R.; Assaly, R. Elevated interleukin-6 and severe COVID-19: A meta-analysis. J. Med. Virol. 2020, 92, 2283–2285. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The vascular endothelium: The cornerstone of organ dysfunction in severe SARS-CoV-2 infection. Crit. Care 2020, 24, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Al-Mokadem, A.Z.; Alnaggar, A.E.-A.M.; Mancy, A.G.; Sofy, A.R.; Sofy, M.R.; Mohamed, A.K.S.; Abou Ghazala, M.M.; El-Zabalawy, K.M.; Salem, N.F.; Elnosary, M.E. Foliar Application of Chitosan and Phosphorus Alleviate the Potato virus Y-Induced Resistance by Modulation of the Reactive Oxygen Species, Antioxidant Defense System Activity and Gene Expression in Potato. Agronomy 2022, 12, 3064. [Google Scholar] [CrossRef]
- Kaur, S.; Bansal, Y.; Kumar, R.; Bansal, G. A panoramic review of IL-6: Structure, pathophysiological roles and inhibitors. Bioorganic Med. Chem. 2020, 28, 115327. [Google Scholar] [CrossRef]
- Nouveau, L.; Buatois, V.; Cons, L.; Chatel, L.; Pontini, G.; Pleche, N.; Ferlin, W.G. Immunological analysis of the murine anti-CD3-induced cytokine release syndrome model and therapeutic efficacy of anti-cytokine antibodies. Eur. J. Immunol. 2021, 51, 2074–2085. [Google Scholar] [CrossRef]
- Li, X.; Shao, M.; Zeng, X.; Qian, P.; Huang, H. Signaling pathways in the regulation of cytokine release syndrome in human diseases and intervention therapy. Signal Transduct. Target. Ther. 2021, 6, 367. [Google Scholar] [CrossRef]
- Burgos-Blasco, B.; Güemes-Villahoz, N.; Santiago, J.L.; Fernandez-Vigo, J.I.; Espino-Paisan, L.; Sarria, B.; Garcia-Feijoo, J.; Martinez-de-la-Casa, J.M. Hypercytokinemia in COVID-19: Tear cytokine profile in hospitalized COVID-19 patients. Exp. Eye Res. 2020, 200, 108253. [Google Scholar] [CrossRef]
- Rubbert-Roth, A.; Furst, D.E.; Nebesky, J.M.; Jin, A.; Berber, E. A review of recent advances using tocilizumab in the treatment of rheumatic diseases. Rheumatol. Ther. 2018, 5, 21–42. [Google Scholar] [CrossRef] [Green Version]
- Urbaniak, G.; Plous, S. Research Randomizer; Version 4.0; Web-based application; Social Psychology Network: Evansville, IN, USA, 2013. [Google Scholar]
- Kang, S.-J.; Jung, S.I. Age-related morbidity and mortality among patients with COVID-19. Infect. Chemother. 2020, 52, 154. [Google Scholar] [CrossRef]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.-A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef] [PubMed]
- Conover, W.J. Practical Nonparametric Statistics; John Wiley & Sons: Hoboken, NJ, USA, 1999; Volume 350. [Google Scholar]
- Fouda, H.; Sofy, M. Effect of biological synthesis of nanoparticles from Penicillium chrysogenum as well as traditional salt and chemical nanoparticles of zinc on canola plant oil productivity and metabolic. Egyp. J. Chem. 2022, 65, 507–516. [Google Scholar] [CrossRef]
- Maksoud, M.A.; Bekhit, M.; El-Sherif, D.M.; Sofy, A.R.; Sofy, M.R. Gamma radiation-induced synthesis of a novel chitosan/silver/Mn-Mg ferrite nanocomposite and its impact on cadmium accumulation and translocation in brassica plant growth. Int. J. Biol. Macrom. 2022, 194, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Stewart, I.; Fabbri, L.; Moss, S.; Robinson, K.; Smyth, A.R.; Jenkins, G. Systematic review and meta-analysis of anakinra, sarilumab, siltuximab and tocilizumab for COVID-19. Thorax 2021, 76, 907–919. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.J.; Raymundo, L.A.M.; Monteforte, M.; Taub, E.M.; Go, R. Tocilizumab in the treatment of critical COVID-19 pneumonia: A retrospective cohort study of mechanically ventilated patients. Int. J. Infect. Dis. 2021, 103, 536–539. [Google Scholar] [CrossRef]
- Vela, D.; Vela-Gaxha, Z.; Rexhepi, M.; Olloni, R.; Hyseni, V.; Nallbani, R. Efficacy and safety of tocilizumab versus standard care/placebo in patients with COVID-19; a systematic review and meta-analysis of randomized clinical trials. Br. J. Clin. Pharmacol. 2022, 88, 1955–1963. [Google Scholar] [CrossRef]
- Yu, S.-Y.; Koh, D.-H.; Choi, M.; Ryoo, S.; Huh, K.; Yeom, J.S.; Yoon, Y.K. Clinical efficacy and safety of interleukin-6 receptor antagonists (tocilizumab and sarilumab) in patients with COVID-19: A systematic review and meta-analysis. Emerg. Microbes Infect. 2022, 11, 1154–1165. [Google Scholar] [CrossRef]
- Zhao, J.; Cui, W.; Tian, B.-p. Efficacy of tocilizumab treatment in severely ill COVID-19 patients. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef]
- Boregowda, U.; Perisetti, A.; Nanjappa, A.; Gajendran, M.; Kutti Sridharan, G.; Goyal, H. Addition of tocilizumab to the standard of care reduces mortality in severe COVID-19: A systematic review and meta-analysis. Front. Med. 2020, 7, 586221. [Google Scholar] [CrossRef]
- Chober, D.; Aksak-Wąs, B.; Bobrek-Lesiakowska, K.; Budny-Finster, A.; Hołda, E.; Mieżyńska-Kurtycz, J.; Jamro, G.; Parczewski, M. Effectiveness of Tocilizumab in Patients with Severe or Critical Lung Involvement in COVID-19: A Retrospective Study. J. Clin. Med. 2022, 11, 2286. [Google Scholar] [CrossRef]
- Aziz, M.; Haghbin, H.; Abu Sitta, E.; Nawras, Y.; Fatima, R.; Sharma, S.; Lee-Smith, W.; Duggan, J.; Kammeyer, J.A.; Hanrahan, J. Efficacy of tocilizumab in COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1620–1630. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Molinero, A.; Pérez-López, C.; Gálvez-Barrón, C.; Miñarro, A.; Macho, O.; López, G.F.; Robles, M.T.; Dapena, M.D.; Martínez, S.; Rodríguez, E. Matched cohort study on the efficacy of tocilizumab in patients with COVID-19. One Health 2021, 12, 100214. [Google Scholar] [CrossRef] [PubMed]
- Vivarelli, E.; Matucci, A.; Lucenteforte, E.; Bormioli, S.; Virgili, G.; Trotta, M.; Spinicci, M.; Bartoloni, A.; Zammarchi, L.; Peris, A. Effectiveness of Tocilizumab in hospitalized moderate-to-severe COVID-19 patients: A real life study. Panminerva Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Morrison, A.R.; Johnson, J.M.; Griebe, K.M.; Jones, M.C.; Stine, J.J.; Hencken, L.N.; To, L.; Bianchini, M.L.; Vahia, A.T.; Swiderek, J. Clinical characteristics and predictors of survival in adults with coronavirus disease 2019 receiving tocilizumab. J. Autoimmun. 2020, 114, 102512. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Wang, W.; Hayek, S.S.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J. Association between early treatment with tocilizumab and mortality among critically ill patients with COVID-19. JAMA Intern. Med. 2021, 181, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Luo, P.; Liu, Y.; Qiu, L.; Liu, X.; Liu, D.; Li, J. Tocilizumab treatment in COVID-19: A single center experience. J. Med. Virol. 2020, 92, 814–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- Cavalli, G.; De Luca, G.; Campochiaro, C.; Della-Torre, E.; Ripa, M.; Canetti, D.; Oltolini, C.; Castiglioni, B.; Din, C.T.; Boffini, N. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e325–e331. [Google Scholar] [CrossRef]
- Horby, P.W.; Pessoa-Amorim, G.; Peto, L.; Brightling, C.E.; Sarkar, R.; Thomas, K.; Jeebun, V.; Ashish, A.; Tully, R.; Chadwick, D. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): Preliminary results of a randomised, controlled, open-label, platform trial. Medrxiv 2021. [Google Scholar]
- Tleyjeh, I.M.; Kashour, Z.; Damlaj, M.; Riaz, M.; Tlayjeh, H.; Altannir, M.; Altannir, Y.; Al-Tannir, M.; Tleyjeh, R.; Hassett, L. Efficacy and safety of tocilizumab in COVID-19 patients: A living systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 215–227. [Google Scholar] [CrossRef]
- Biran, N.; Ip, A.; Ahn, J.; Go, R.C.; Wang, S.; Mathura, S.; Sinclaire, B.A.; Bednarz, U.; Marafelias, M.; Hansen, E. Tocilizumab among patients with COVID-19 in the intensive care unit: A multicentre observational study. Lancet Rheumat 2020, 2, e603–e612. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group A (Conventional) N = 50 | Group B (Tocilizumab) N = 50 | Mann–Whitney U Statistic | p-Value | |
|---|---|---|---|---|
| Age, median (IQR), years | 63.00 (55.75–66.0) | 66.00 (55.0–70.0) | 1140.50 | 0.44 NS |
| Weight, kg | 80.0 (67.00–80.00) | 70.00 (60.00–88.50) | 1020.50 | 0.111 NS |
| Height, (meter) | 1.68 (1.60–1.70) | 1.66 (1.62–1.70) | 1237.50 | 0.932 NS |
| BMI, kg/m2 | 27.68 (26.72–28.89) | 26.64 (23.43–30.65) | 996.50 | 0.080 NS |
| RR median (IQR), breaths/min | 26.00 (24.00–30.00) | 22.00 (21.00–30.65) | 493.00 | <0.001 HS |
| FIO2, mm Hg | 0.21 (0.21–0.21) | 0.21 (0.21–0.21) | 1125.00 | 0.166 NS |
| PAO2, mm Hg | 56.0 (55.00–73.00) | 66.00 (49.25–73.00) | 1239.50 | 0.94 NS |
| Max. temp, median (IQR), °C | 38.00 (38.00–38.00) | 37.90 (37.50–38.00) | 845 | 0.002 s |
| Systolic BP, mm Hg | 120.00 (110.00–132.50) | 130.0 (127.50–140.0) | 841 | 0.004 S |
| Diastolic, mm Hg | 80.00 (70.00–90.00) | 85.00 (80.00–100.00) | 837.000 | 0.003 S |
| HR | 88.00 (85.00–92.00) | 99.00 (90.0–103.00) | 462.50 | <0.001 HS |
| GCS at admission | 15.00 (15.00–15.00) | 15.00 (15.00–15.00) | 1210 | 0.61 NS |
| IL-6, median (IQR), pg/mL | 36.18 (17.25–58.25) | 51.05 (29.25–65.52) | 977.00 | 0.060 NS |
| Comorbidities Diabetes CKD IHD COPD Hypertension | 20(40.0%) 3(6.0%) 6(12.0%) 0(0.0%) 26(52.0%) | 22(44.0%) 0(0.0%) 16(32.0%) 5(10.0%) 22(44.0%) | X2 = 0.164 X2 = 3.093 X2 = 5.828 X2 = 5.263 X2 = 0.641 | 0.685 NS 0.079 NS 0.016 S 0.022 S 0.423 NS |
| Group A (Conventional) N = 50 | Group B (Tocilizumab) N = 50 | Mann–Whitney U Statistic | p-Value | |
|---|---|---|---|---|
| CRP, mg/dL | 103.0 (100.00–120.0) | 104.00 (72.0–108.25) | 913.00 | 0.019 S |
| Creatinine | 1.50 (1.40–1.90) | 1.40 (1.20–1.90) | 1020 | 0.111 NS |
| HB | 13.00 (11.70–15.17) | 12.00 (11.40–13.72) | 999.50 | 0.084 NS |
| TLC/μL | 8400.0 (6000–18,750) | 11450.0 (10,175–14,825) | 1052.50 | 0.174 NS |
| Lymphocyte Count, % | 12.00 (10.00–15.00) | 10.00 (6.00–15.00) | 985.00 | 0.064 NS |
| Neutrophile Count, % | 80.00 (80.00–82.50) | 84.00 (80.00–87.75) | 888.00 | 0.011 S |
| NLR, % | 6.83 (5.33–8.30) | 8.30 (5.39–14.49) | 963 | 0.047 S |
| PLT ×103/μL | 281.0 (187.0–332.5) | 246.5 (186.0–291.50) | 1074.50 | 0.227 NS |
| NA | 141.50 (138.00–143.0) | 140.000 (137.0–143.0) | 1122.50 | 0.379 NS |
| K | 4.00 (3.80–4.30) | 4.20 (3.94–4.43) | 1049.50 | 0.167 Ns |
| Temp, °C | 38.00 (38.00–38.0) | 38.00 (38.00–38.0) | 1250.00 | 1.00 NS |
| Ferritin, ng/mL | 564.00 (500.0–758.0) | 721.0 (486.25–1500) | 997.00 | 0.080 NS |
| AST | 33.50 (25.00–41.75) | 55.00 (45.00–71.00) | 4325.50 | <0.001 HS |
| LDH | 576.50 (441.00–825.75) | 881.00 (718.00–1147.50) | 506.00 | <0.001 HS |
| D-Dimer, ng/mL | 463.50 (283.00–1001.0) | 513.0 (251.0–1014.0) | 1236.50 | 0.928 NS |
| ALT | 37.50 (25.00–40.00) | 55.00 (40.00–88.00) | 568.500 | <0.001 HS |
| O2 saturation at admission | 80.00 (70.00–85.00) | 80.00 (70.00–89.00) | 1135.50 | 0.429 NS |
| Group A (Conventional) N = 50 | Group B (Tocilizumab) N = 50 | Mann–Whitney U Statistic | p-Value | |
|---|---|---|---|---|
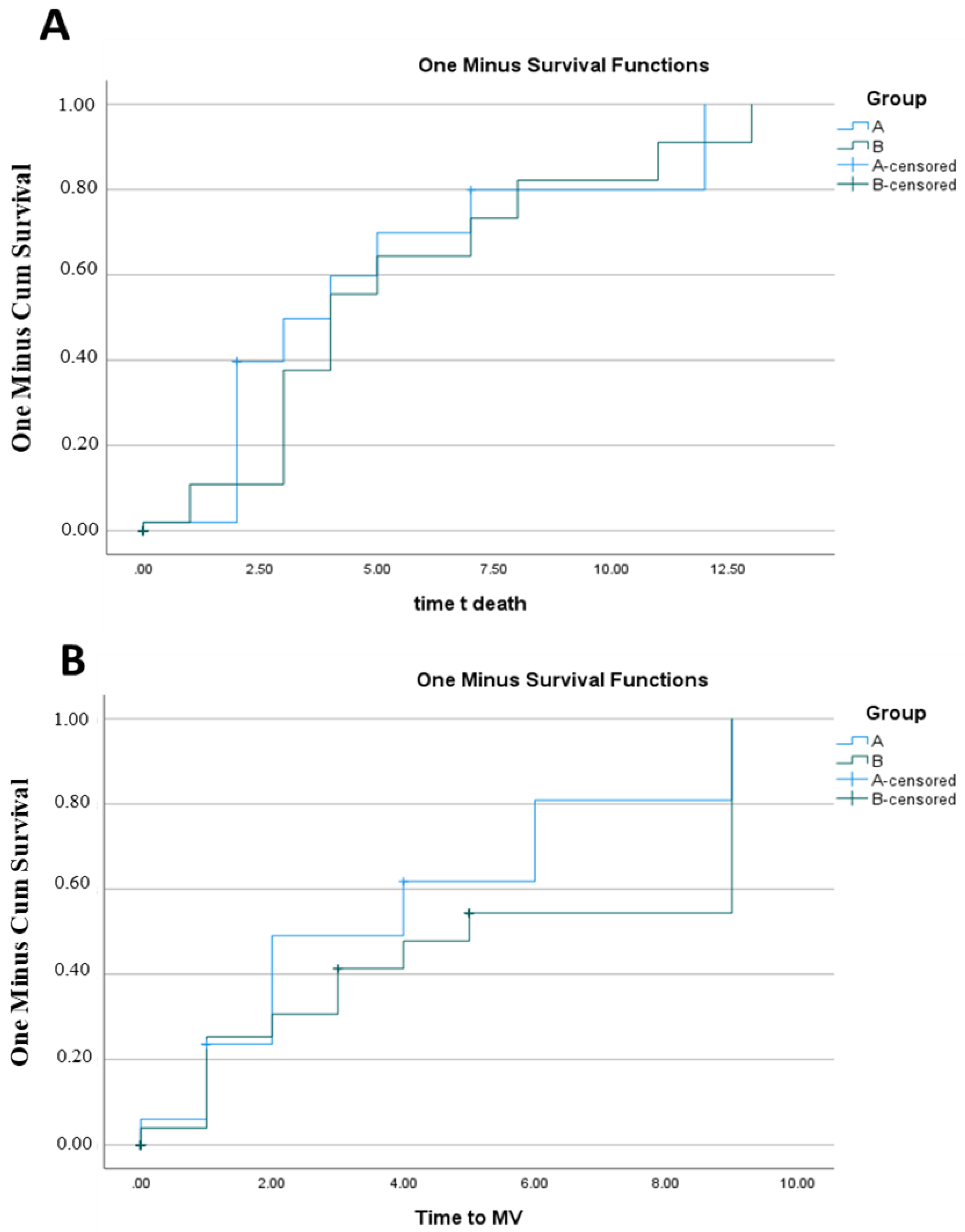
| Time to death | 0.00 (0.00–2.00) | 0.00 (0.00–0.00) | 1225.0 | 0.825 NS |
| Time to MV | 0.00 (0.00–1.00) | 0.00 (0.00–3.00) | 1138.50 | 0.364 NS |
| Duration of MV days | 0.00 (0.00–2.00) | 1.50 (0.00–3.00) | 1027.00 | 0.098 NS |
| Patient hospital days | 4.00 (3.00–6.00) | 7.00 (4.75–10.00) | 564.50 | <0.001 HS |
| Outcomes | Group A (Conventional) N = 50 | Group B (Tocilizumab) N = 50 | Chi-Square | p-Value |
|---|---|---|---|---|
| Clinical worsening (MV) primary endpoint | 17 (34%) | 28 (56%) | 4.889 | 0.027 S |
| Deaths at the end of follow-up | 11 (22%) | 12 (24%) | 0.056 | 0.812 NS |
| Discharges at the end of follow-up | 19 (38%) | 24 (48%) | 25.5 | 0.001 S |
| CRP | Unstandardized Coefficients | Standardized Coefficient | t | Sig. | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| (Constant) | 2256.774 | 813.942 | 2.773 | 0.008 | |
| Time at death | −8.036 | 2.980 | −0.988 | −2.696 | 0.010 |
| Time to MV | 6.762 | 3.162 | 0.620 | 2.139 | 0.038 |
| Duration of MV days | 8.850 | 3.948 | 0.833 | 2.242 | 0.030 |
| Age | Unstandardized Coefficients | Standardized Coefficient | t | Sig. | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| (Constant) | 688.895 | 297.89 | 2.313 | 0.026 | |
| Duration of MV days | −5.172- | 1.406 | −1.094- | −3.677- | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabie, A.S.I.; Salah, H.; Said, A.S.A.; Shaaban, A.H.; Abdou, L.M.; Khalil, D.M.; Kharaba, Z.; Afifi, H.; Sofy, M.R.; Youssef, E.M.I.; et al. Clinical Consequences for Individuals Treated with Tocilizumab for Serious COVID-19 Infection. Healthcare 2023, 11, 607. https://doi.org/10.3390/healthcare11040607
Rabie ASI, Salah H, Said ASA, Shaaban AH, Abdou LM, Khalil DM, Kharaba Z, Afifi H, Sofy MR, Youssef EMI, et al. Clinical Consequences for Individuals Treated with Tocilizumab for Serious COVID-19 Infection. Healthcare. 2023; 11(4):607. https://doi.org/10.3390/healthcare11040607
Chicago/Turabian StyleRabie, Al Shaimaa Ibrahim, Hager Salah, Amira S. A. Said, Ahmed Hassan Shaaban, Lamya Mohamed Abdou, Doaa Mahmoud Khalil, Zelal Kharaba, Hala Afifi, Mahmoud R. Sofy, Eman M. I. Youssef, and et al. 2023. "Clinical Consequences for Individuals Treated with Tocilizumab for Serious COVID-19 Infection" Healthcare 11, no. 4: 607. https://doi.org/10.3390/healthcare11040607