1. Introduction
The World Health Organization (WHO) declared the monkeypox (Mpox) outbreak to be a public health emergency of international concern (PHEIC) on 23 July 2022 [
1]. On 28 November 2022, the WHO recommended using the name Mpox as a new name for the disease to reduce the associated stigma [
2].
As of 18 January 2023, a cumulative total of 84,901 laboratory-confirmed cases of Mpox, including 83 deaths, have been reported from 110 countries spanning the six WHO regions [
3].
The ten countries that reported the most cumulative cases worldwide are the United States of America (USA, n = 30,026), Brazil (n = 10,671), Spain (n = 7513), France (n = 4114), Colombia (n = 4062), the United Kingdom (UK, n = 3730), Peru (n = 3711), Mexico (n = 3696), Germany (n = 3684), and Canada (n = 1460) [
3]. Combined, these countries represent 86% of reported cases worldwide [
3].
Mpox is caused by the monkeypox virus (MPXV), a member of the
Orthopoxvirus genus in the family
Poxviridae, which refers to the first isolation of captive monkeys sent to Denmark from Africa in 1958, which was first identified in humans in 1970 in the Democratic Republic of the Congo [
4,
5]. The MPXV has a zoonotic origin, with multiple reservoirs [
4]. Mpox is a disease of global public health importance as it affects not only countries in west and central Africa, but the rest of the world [
4].
Mpox is transmitted to humans through close contact with an infected person or animal or with material contaminated with the virus [
4].
There has been a significant increase in the recent resurgence of Mpox, which is worrying about the possibility of developing another pandemic similar to that of COVID-19 [
5,
6]. The recent outbreak of Mpox in several countries, with no movement to endemic regions, is certainly of worry [
5,
6], as demonstrated by scientists worldwide [
7].
The recipients of solid organ transplantation may contract Mpox through direct contact with cutaneous lesions, sexual transmission, or respiratory droplets from infected humans or animals [
8,
9]. The American Society of Transplantation (AST) announced that although there were no published data on Mpox in transplant recipients, there was an impending risk to this immunocompromised patient population, especially if the human-to-human transmission continued [
10].
Moreover, it could be transmitted from an infected donor to the recipient of the solid organ during transplantation [
11]. The emergence of Mpox continues to add to the current burden of anxiety experienced by healthcare workers (HCWs) and the public as well [
1]. A recent study revealed that approximately 62% of the general population were more worried about Mpox than coronavirus disease 2019 (COVID-19) [
12]. Another study by Gallè et al. showed that the communication about Mpox was initially ineffective in terms of disease knowledge among adults [
13]. The ongoing COVID-19 pandemic has been associated with stress among HCWs, as well as increased workload and anxiety [
14].
The transplant community is concerned about the potential for more severe outcomes in transplant recipients if they develop Mpox infections. Moreover, transplant healthcare workers are worried about the need for post-exposure prophylaxis for themselves. We conducted this multicenter survey to assess the perceptions and knowledge among solid organ transplants’ HCWs working in Saudi Arabia and their advocacy of the Mpox vaccines.
4. Discussion
The recipients of SOT are among the groups considered at risk for MPXV acquisition with risk of severe disease. This comes in relation to their compromised immune status; therefore, HCWs involved in SOT patient care should be highly knowledgeable regarding this emerging infection.
The current study represented a unique and novel opportunity to analyze Mpox knowledge and awareness as well as the worries of this group towards an emerging infection that was declared as a PHEIC.
The findings of the study indicated several gaps in HCWs’ knowledge and relatively high levels of anxiety regarding Mpox among the study group. The relevance of the study is related to the representativeness of various occupational categories of HCWs involved in SOT and the inclusions of personnel with varying level of experience. Specifically, about half of the study sample comprised nurses or nurse coordinators. Moreover, more than a third of the respondents were physicians. Furthermore, the study sample comprised pharmacists and laboratory technicians having different roles in the care of SOT patients.
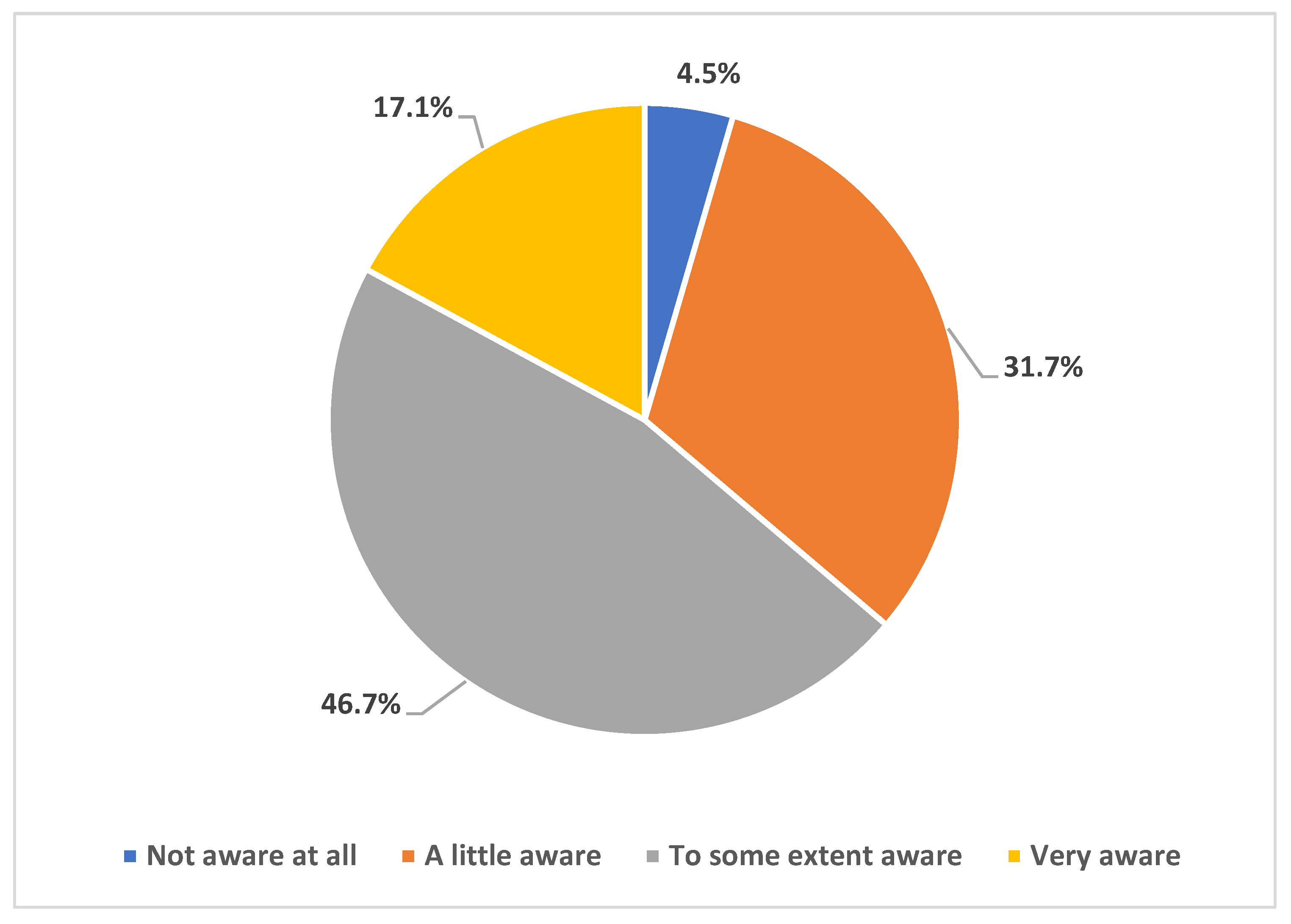
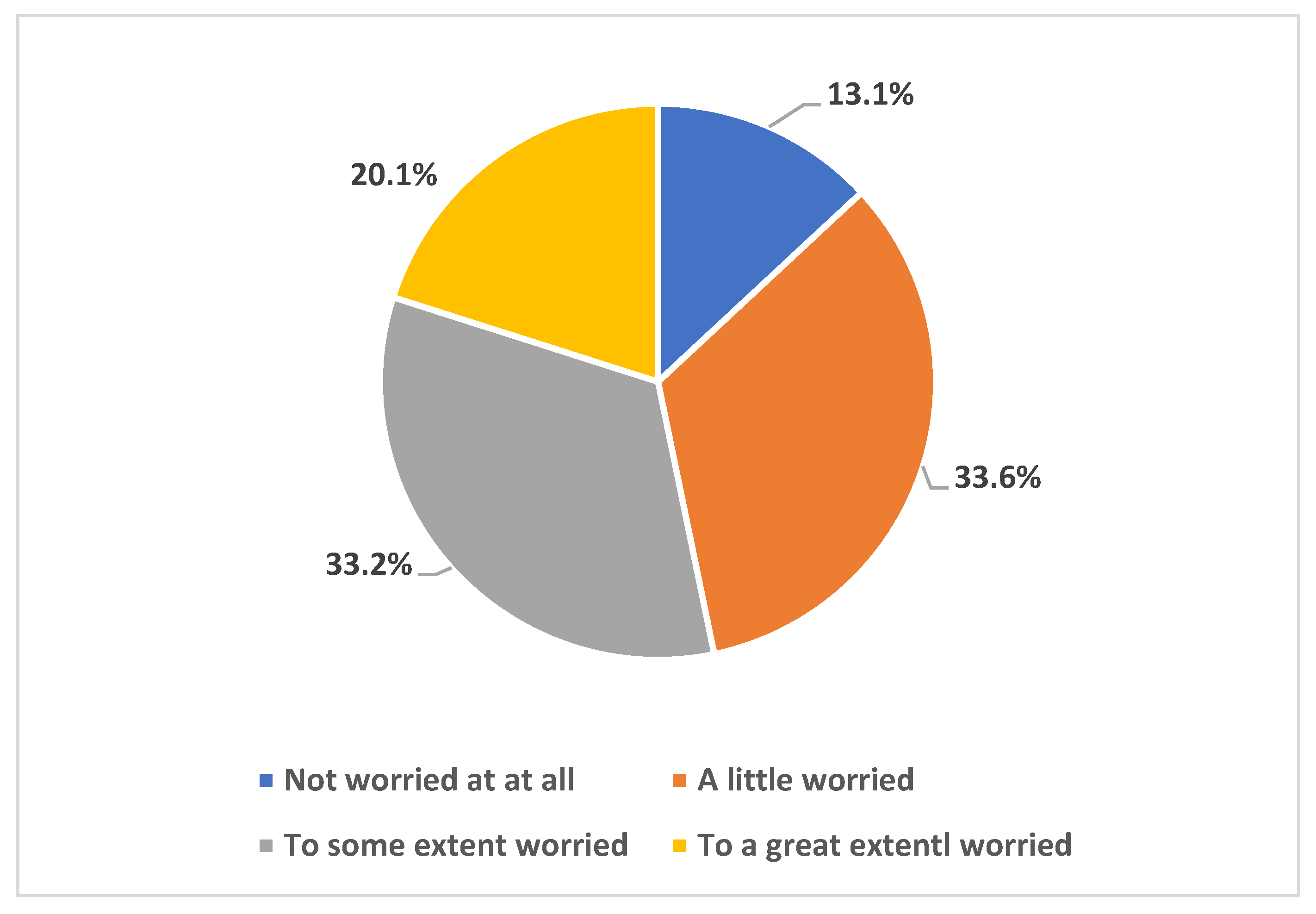
Our results indicated high levels of awareness of the ongoing Mpox multi-country outbreak, with >95% of the participants being either very aware, aware, or at least having a little awareness of the 2022 increase in Mpox cases worldwide that meant its declaration as a PHEIC. This result is conceivable for two reasons: first, the SOT HCWs could have higher levels of worry regarding emergence infectious diseases considering the critical condition of the patients they take care of; second, the timing of the survey (August/September 2022) coincided with intensive and rapid availability of literature regarding Mpox together with intensified media coverage of the new emerging infection following COVID-19. The latest point might explain the finding of high levels of worries that Mpox might turn into a pandemic similar to COVID-19. Specifically, 87% of the respondents were either very worried, worried to some extent, or at least having a little worry that MPXV will cause a pandemic similar to COVID-19. This result is much higher compared to the level of worry previously observed among HCWs in Saudi Arabia, where the level of Mpox worries was observed at a rate of 51% [
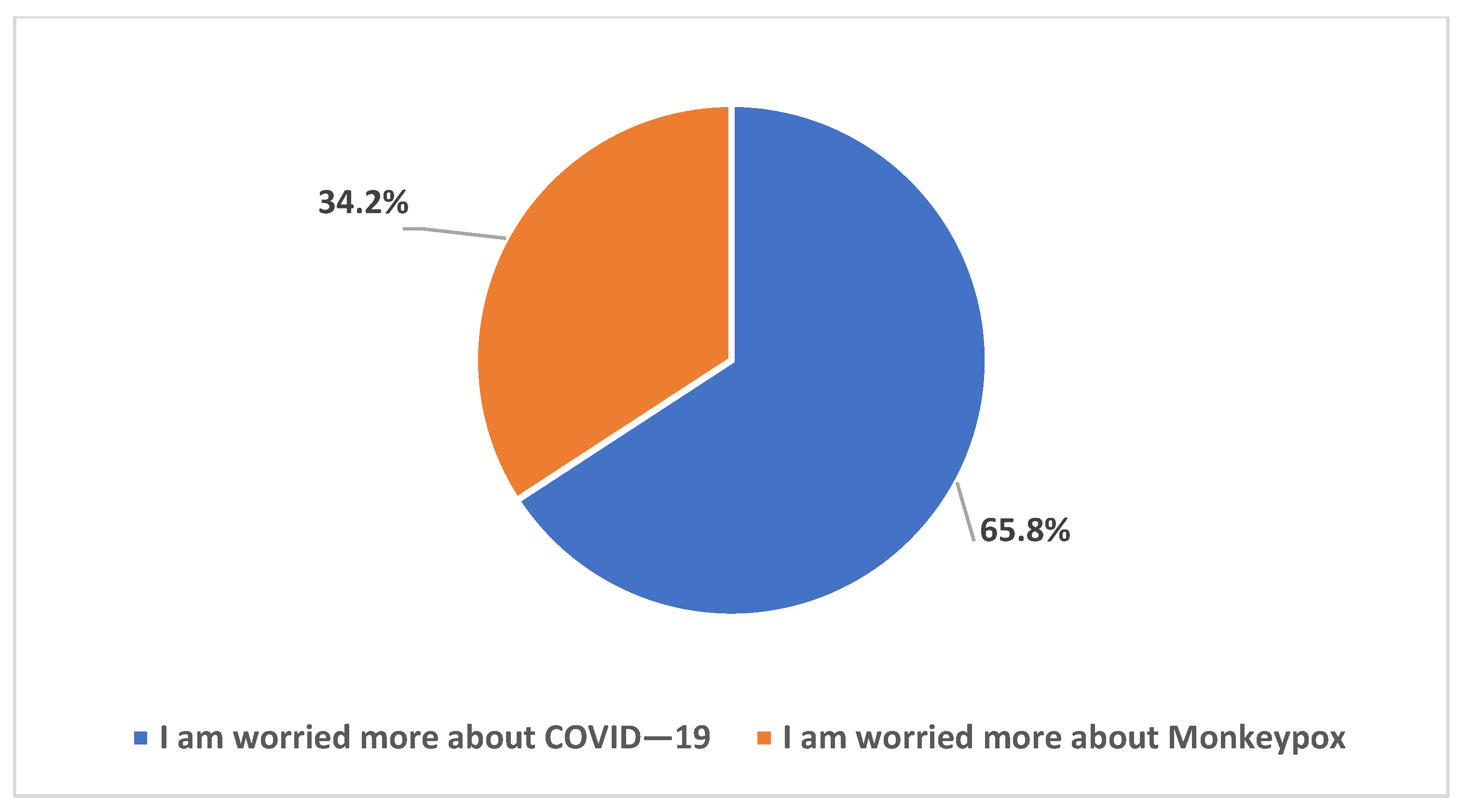
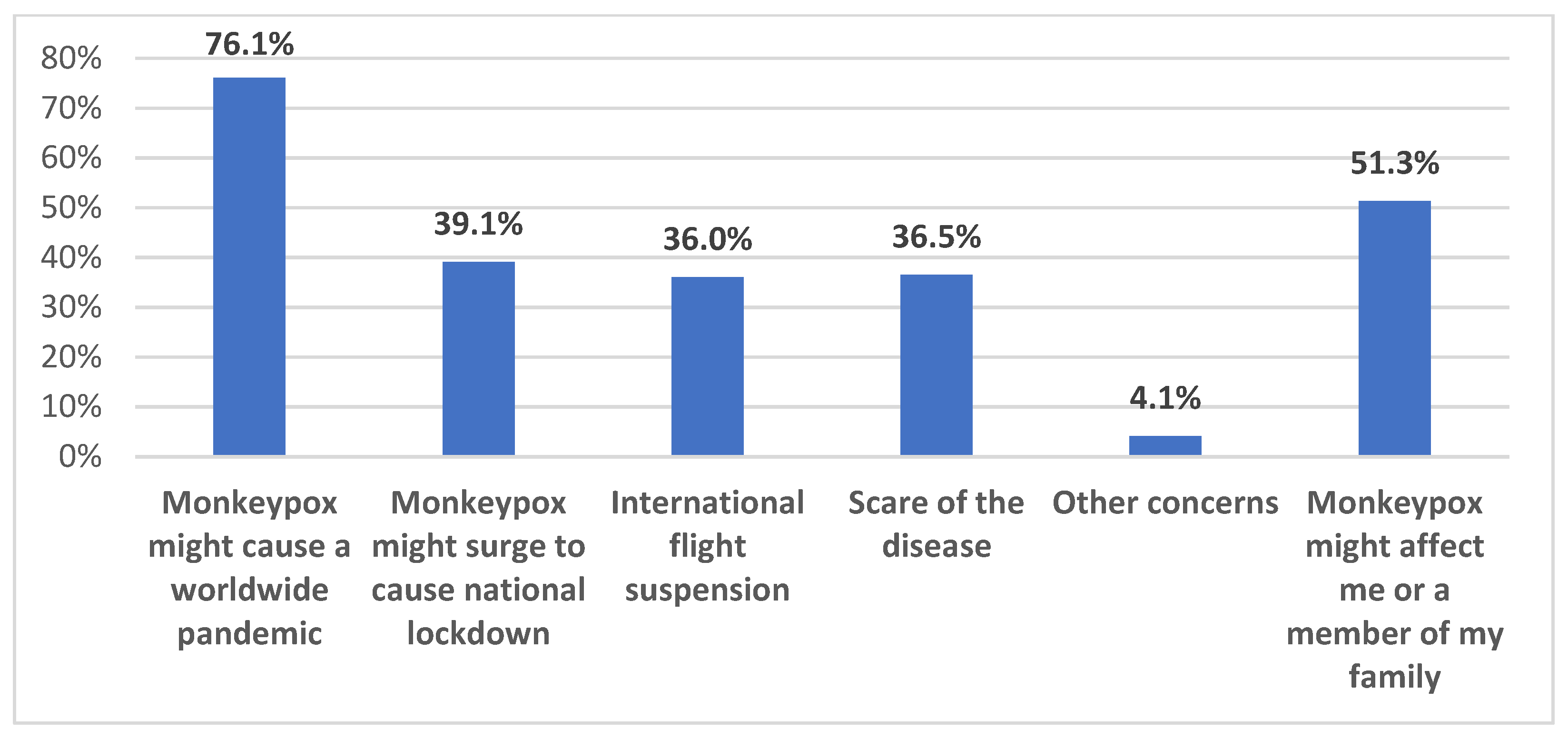
23]. This high level of worry among SOT HCWs is also understandable considering the immune status of the patients to whom they are responsible for providing care. However, the respondents listed other possible causes of such worries including the fear of another pandemic, fear of becoming infected themselves or infection among their families, and worries that Mpox might cause another international flight suspension or wide lockdowns. Despite that, the level of worry from COVID-19 was still higher among the study respondents compared to the level of worry from Mpox (66% vs. 34%). In line with this result, the overall level of anxiety as measured through the GAD-7 score revealed a mean score of 3.6 out of 21 maximum points.
Regarding the level of Mpox knowledge, variable defects were observed as follows: first, the most severe gaps in Mpox knowledge were observed for the items assessing prevention through vaccination. Specifically, correct knowledge of the recommended vaccine for SOT patients (JYNNEOS) was only found among less than a quarter of the respondents. Additionally, correct knowledge of the safety of the MVA vaccine among SOT patient was found among merely 10% of the study sample. Furthermore, 79% of the participants incorrectly thought that chickenpox vaccination can be protective against Mpox. Previous studies reflected that inadequate Mpox vaccine knowledge is commonplace in various studies worldwide. For example, an early survey among Saudi physicians found that the awareness of availability of vaccines to prevent Mpox was reported at a rate of 70% [
24]. Much lower rate of Mpox vaccine availability was observed among HCWs in Jordan, where less than a third of the participants had such knowledge [
25]. Improving the level of vaccine knowledge is of particular importance among SOT HCWs considering the previous evidence that better knowledge can be linked with a favorable attitude towards vaccination and, in turn, a higher likelihood of recommending vaccination to the SOT patients who are considered at a higher risk of severe disease [
26,
27].
Second, the level of Mpox knowledge regarding the possible transmission route was slightly better. However, defects in knowledge were observed for lack of transmission through respiratory droplets, with only 47% correct responses, and regarding sexual transmission of MPXV, with only 57% correct responses. Similarly, inadequate knowledge of Mpox transmission was observed among Italian and Indonesian physicians, as well as HCWs in Kuwait, Jordan, and the Czech Republic [
25,
27,
28,
29,
30]. Moreover, in a recent review of 16 studies that were conducted in non-endemic countries, there were unsatisfactory levels of knowledge and awareness among both HCWs and the general adult population [
31].
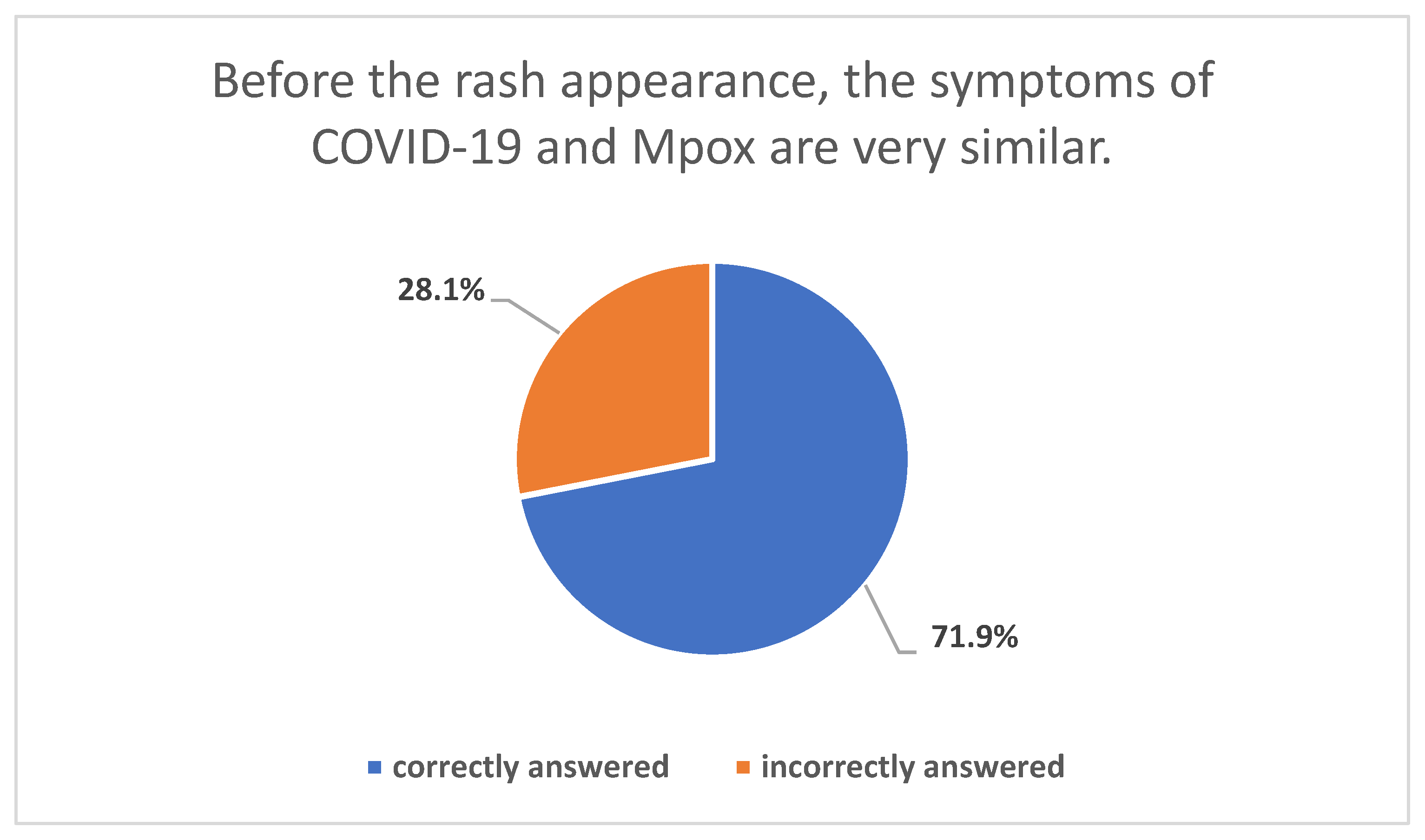
Third, variable knowledge was observed for the items assessing the initial clinical presentation of Mpox as follows: knowledge of fever and skin rash was found in the vast majority of the participants (>90%). Nevertheless, inadequate knowledge of the following signs/symptoms was found among the participants: lymphadenopathy (53%); exhaustion (37%). Finally, several areas need improvement regarding the precautionary measures needed to halt Mpox spread, where 22% and 27% of the participants were not aware of the importance of contact and airborne precautions, respectively.
From a broader perspective, the overall Mpox knowledge was evaluated at a rate of 20.4 out of 32 points as a maximum score. This highlights the need for educational efforts to address these gaps in SOT HCWs’ knowledge. The importance of educational efforts needed to increase the confidence of HCWs to diagnose and manage Mpox case and subsequently mitigate the spread of the virus was underlined in a recent review by Di Gennaro et al. [
32]. The previous and recent studies showing inadequate Mpox knowledge highlights the importance of educational intervention measures that can improve the attitude towards the patients as well, which was advocated by the WHO to limit Mpox spread [
24,
25,
27,
29,
33,
34,
35,
36,
37].
In this study, a special aspect of Mpox knowledge evaluation was related to the finding of lower Mpox vaccination knowledge among nurses and nurse coordinators in multivariate analysis. This recurring pattern was also found in recent studies among HCWs in Jordan and Kuwait [
25,
28], highlighting the need for educational programs tailored to meet the needs of different occupational categories of health professionals.
Treatment of Mpox in immune-compromised patients could be optimized if initiated early and in accordance with the best available evidence. At the time of our research, there were no approved specific antivirals for Mpox therapy and the mainstay relied on supportive treatment. In the Saudi ministry of health guidelines, the two suggested medications were Brincidofovir (once available) and Vaccinia immune globulin (SPIG) (for severe cases) [
38]. In a meta-analysis of 71 individuals, the most commonly used antiviral was tecovirimat, and cidofovir was used in seven patients and brincidofovir was used for three patients [
39].
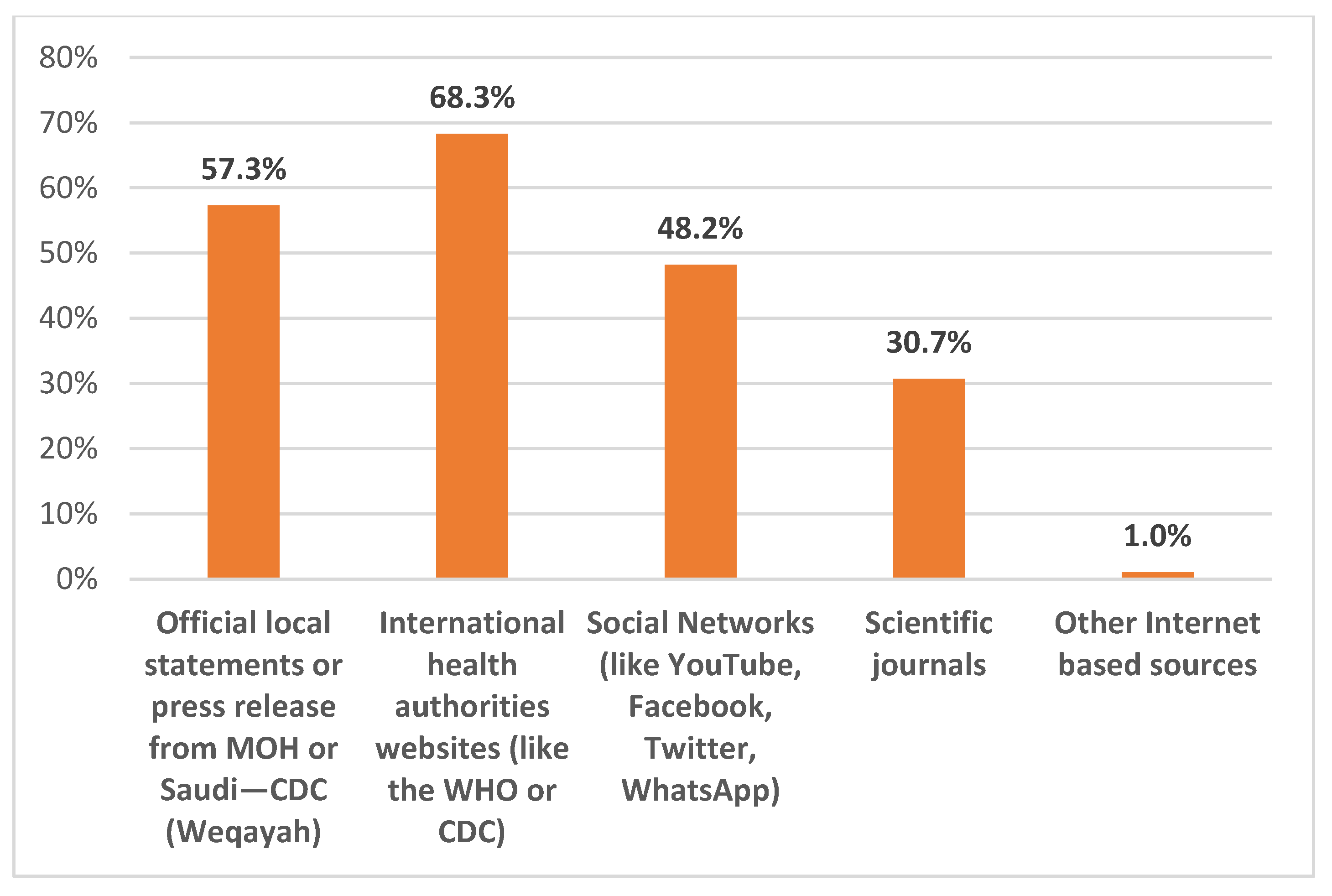
An important area to be considered in the awareness and educational programs is the source of Mpox information. In this study, the majority of respondents reported the reliance on trusted sources of information (e.g., the WHO and CDC websites, the MOH website). However, it was noteworthy to find that almost half of the participants used social networks as a source of updates regarding Mpox. This should be considered carefully, considering the previous evidence of the easy spread of misinformation regarding infectious diseases through social media outlets, which was noticeable during the COVID-19 pandemic [
40,
41]. In line with this concept, conspiracy beliefs regarding Mpox among emerging infections were noticeable from the early days of the Mpox outbreak declaration [
25,
28,
36,
42]. The importance of the source of Mpox information was revealed in our results; we found better Mpox knowledge in the multivariate analysis if the source of information was based on scientific journals or the international health authorities’ websites (the WHO, CDC).
Strengths and Limitations
Our study is the first study to explore the solid organ transplant HCWs’ Mpox perceptions and vaccine advocacy. In the face of the emerging alert of an infectious disease that is novel to the local healthcare system, we were able to identify areas of improvement in Mpox awareness and vaccine advocacy among the HCWs for this vulnerable patient population. Limitations of our research may relate to our inability to explore the HCW’s previous travel experience to countries with endemic Mpox. Other limitations relate to cross-sectional survey limitations in relation to the sampling technique and recall bias.

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





