
Empanelment of the Population to the Primary Medical Care Institution of Sri Lanka: A Mixed-Methods Study on Outcomes and Challenges
 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
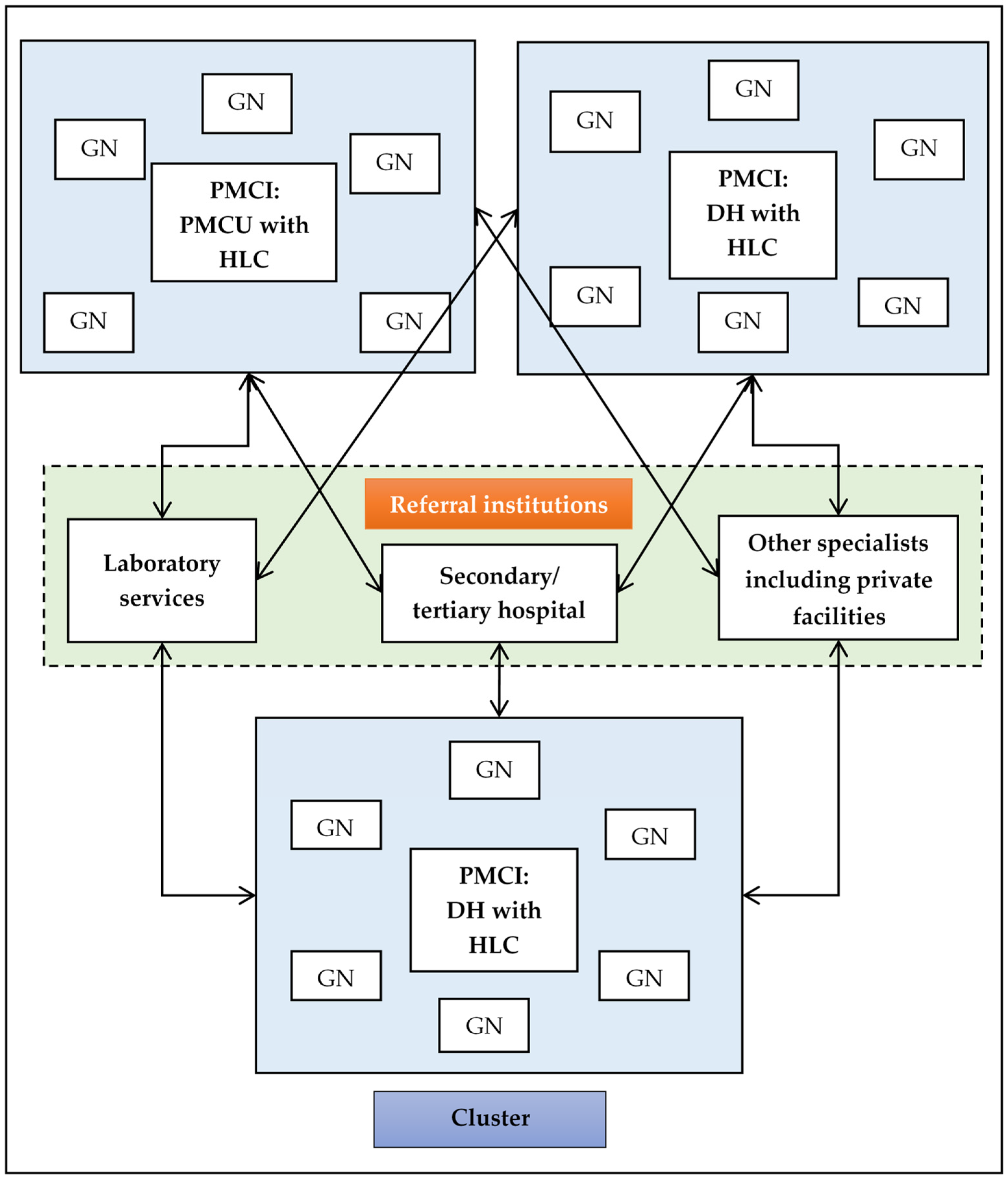
2.2.1. General Setting
2.2.2. Specific Setting
Identification of the Panel for PMCI
Registration of Identified Population with Personal Health Number
Review and Updating the Panel with Personal Health Record
2.3. Study Population
2.3.1. Quantitative Component
2.3.2. Qualitative Component
2.4. Data Collection, Study Variables, Data Source and Study Tools
2.4.1. Quantitative Component
2.4.2. Qualitative Component
2.5. Data Analysis
2.5.1. Quantitative Component
- The percentage of the total population registered in the PMCI: the numerator is all individuals registered until censor date and the denominator is total population in the PMCI area as per the 2012 census of Sri Lanka;
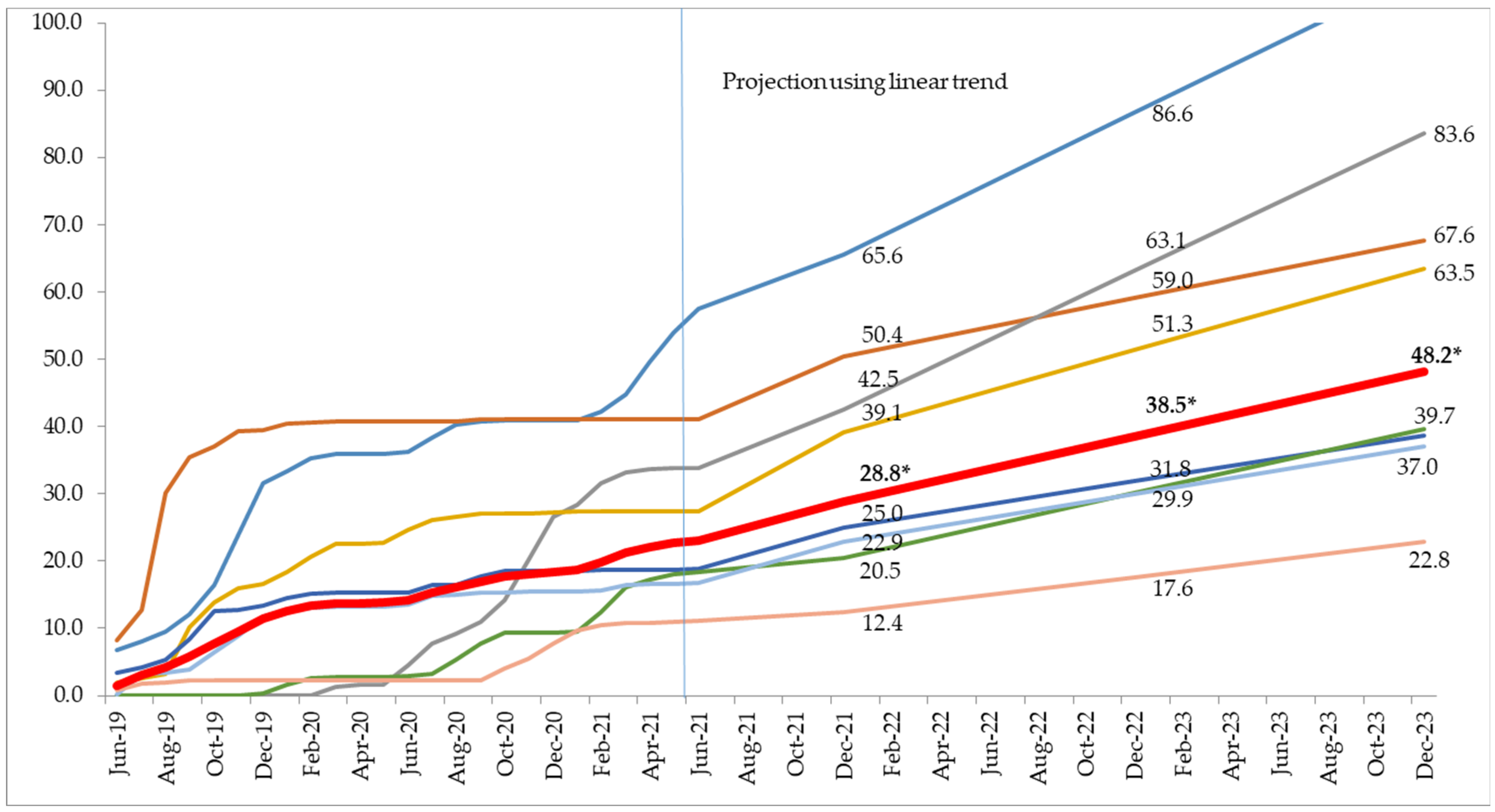
- The monthly trend in percentage of the total registered per PMCI from June 2019 to June 2021: The total percentage registered at the end of each month is calculated with the total number of individuals registered until the end of each month as the numerator and the total population in the PMCI area as per the 2012 census of Sri Lanka as the denominator. Assuming a similar trend (linear) we projected the percentage of the total that would be registered by December 2021, December 2022, and December 2023 (end of project). For this analysis only eight PMCIs which initiated registration since June 2019 were included;
- The percentage of the individuals aged ≥35 years registered in the PMCI: The numerator is individuals aged ≥35 years registered until censor date and the denominator is the total number of individuals aged ≥35 years in the PMCI area as per the 2012 census of Sri Lanka. The age cut off of 35 years was chosen as the PSSP had a mandate for screening individuals aged ≥35 years for NCD risk factors;
- The percentage of males among all the individuals registered in the PMCI: the percentage was calculated with the total number of males registered in the PMCI as the numerator and the total number of individuals registered in the PMCI as the denominator;
- The median (IQR) percentage of the total population registered in the GN divisions of the selected PMCIs: The percentage was calculated with individuals registered from each GN division as numerator and the total population in the respective GN division as per the 2012 census of Sri Lanka as denominator. The median (IQR) of the percentages calculated for each GN division was deduced.
2.5.2. Qualitative Component
3. Results
3.1. Quantitative Component
3.1.1. Identification of Panel for PMCI
3.1.2. Registration at the PMCI
Awareness Generation and Registration Process
Coverage of Registration and Estimated Coverage by December 2023
Coverage of Registration among Individuals Aged ≥35 Years
Gender Distribution of Registered Individuals
Coverage of Registration across the GN Division
3.1.3. Updating of Panel with Personal Health Records
Issuance and Completeness of Paper-Based PHR
Availability of HMIS for Updating Electronic PHR
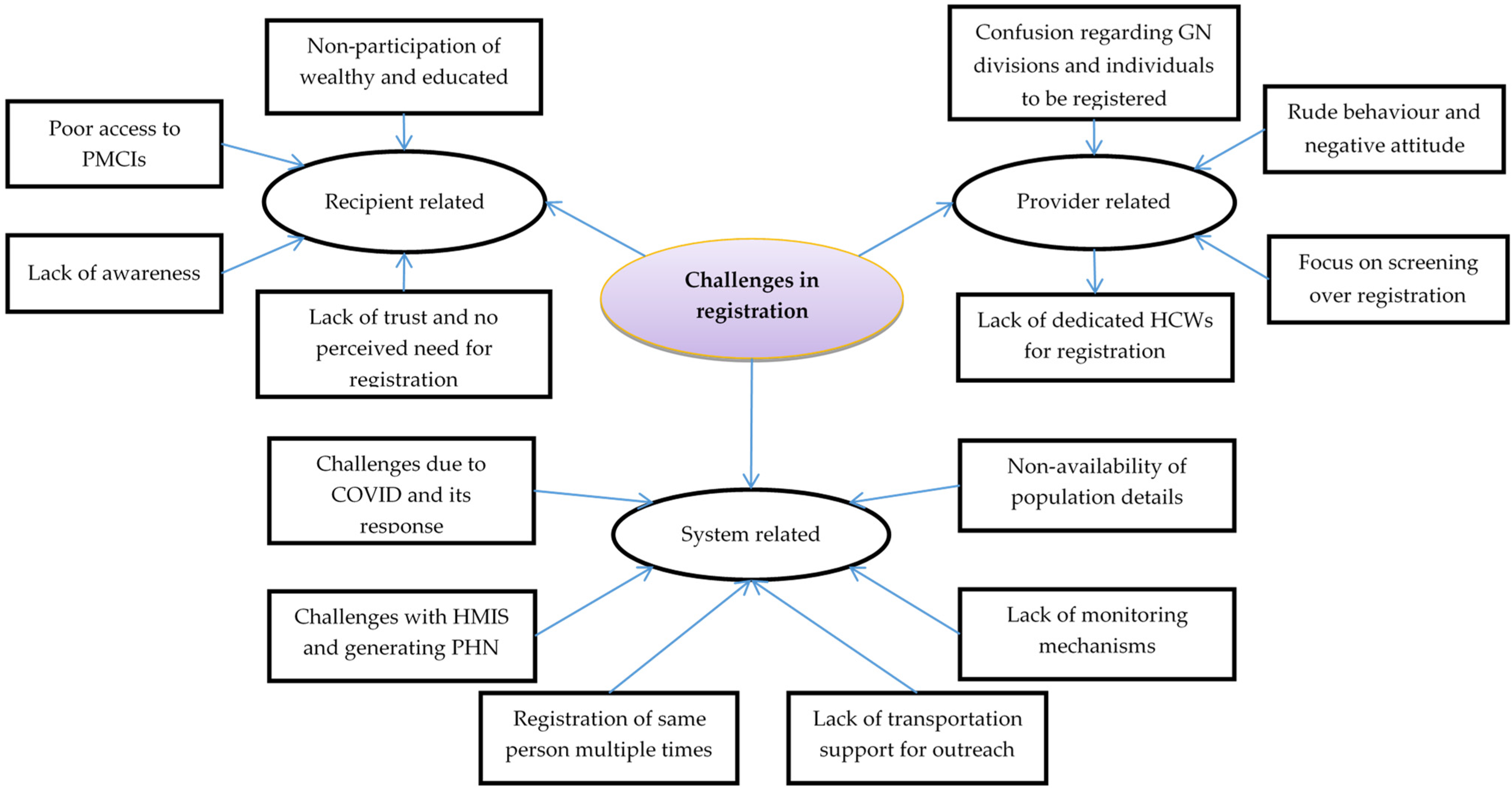
3.2. Qualitative Component
3.2.1. Recipient Related
Lack of Awareness
“No, I have never heard of that. I think such a system is not there in XXX. This is because XXX is a divisional hospital. I think the hospital is not developed to that level. Actually, they don’t use any computers. All registrations are done manually.”
Lack of Perceived Need for Registration
“Sometimes we deliver the message to the community. But if we make 100 people aware, only 25 come. It’s very difficult to gather people. When we give a date for registration, they don’t come on that date…”.
“But one thing I noticed is the rich and educated people do not participate in this but the other poor villagers came and engaged in this… Because the rich go to private clinics.”
Lack of Trust on Identified PMCI
“Almost all the people are going to XXX hospital (secondary hospital) for treatment. Because, here in YYY (PMCI) they have few facilities and there are also no specialist doctors. For every illness they are visiting XXX. But only for OPD some are visiting YYY. That is because of lack of facilities here. Even when someone visits for an emergency at night they are sending that person to YYY, because they don’t have enough facilities.”
Poor Access to PMCI
“Though individuals are empaneled to this PMCI, they do not utilize services from the hospital. When we consider XXX (GN division), people living along the main road (highway connecting two cities) tend to go to YYY (secondary hospital). They never come to (the assigned) PMCI as it is not convenient for them to travel to this PMCI, which is located far away from highways and there are no proper transport facilities.”
“They (individuals in his village) went. They informed me too. But I was at work on that day. A very big crowd went on that day for the camp (registration).”
3.2.2. System Related
Non-Availability of Population Details
“We don’t have details. We didn’t even receive voter’s registries. I requested that from Divisional Secretary, XXX. But he said that he is not authorized to give that and needs to ask from the YYY (District Secretary office). Finally, he said that he can’t give it.”
Challenges with HMIS and Generating PHN
“The huge challenge we have is HMIS due to internet connection. Even in hospital, we are working with our personal hot spot. We are not able to readily generate PHN for registration. So, we need to generate PHN before camp or register the individual after camp. Sometimes because of this, we failed to give the PHN numbers to those registered.”
Registration of Same Person Multiple Times
“Actually, there are instances where we register a single patient 10–12 times. This is a waste of resources. We waste paper, money, and time.”
Lack of Transportation Support for Outreach Camps
“The problem is that when we want to have mobile clinics, the staff are lacking and transport is not available. Also, we can’t use the ambulance as well. Sometimes staff paid their own money for traveling to camp sites.”
Lack of Monitoring Mechanisms
“She (nursing officer) stated that data were entered (registration). But when we checked only 7 (people) were entered. So, we had to start from the beginning… There were no data. So, we started from the beginning…”
Challenges due to COVID and Its Response
“The registration numbers collapsed with the onset of COVID-19. That count drastically dropped down as individuals were registered only when they came to OPD. Even OPD numbers went down with COVID-19 as our facility was functioning as a dedicated COVID hospital…”
3.2.3. Provider Related
Lack of Dedicated Staff for Registration
“After the project started we registered patients daily from the outpatient department (OPD). But we didn’t have enough resources and time. The main problem was lack of staff. We had problems with assigning a dedicated nurse or other staff for this task.”
“No, we didn’t have any opportunity (outreach activity). Basically, we didn’t have a dedicated health worker to organize this. We really need someone dedicated.”
Focus on Screening Targets over Registration
“The population assigned to us was around 64,200, the eligible population (≥35 years) for registration was about 34,000. We had screened about 23,000 from 2017 itself. Thus, we were well ahead of the target for registration.”
“In PSSP, we were given targets such as 25% registration per year. Assume, 40% of the total population were above 35 years in a particular catchment area, 25% had to be registered in year 1 and 50% by year 2.”
Confusion Regarding GN Divisions and Individuals to Be Registered
“Hmmm (looks confused), I can’t remember exactly. As I remember it is around 20.”
“I can’t remember exactly. As I remember it is 48 GN divisions (same as the MOH area).”
“I didn’t go for registration. Last year when they were doing it (registration), it was definitely for older people. I’m not quite sure whether it was 35 or 40 (age). Not for us… I think even the banners said so (we verified by looking at the photographs, both the notice and the letter sent to households mentioned that the programme of registration was intended for people above 35 years).”
“RDHS informed us to register all those aged 35 years and above in the given empanelment area.”
Negative Attitude and Rude Behaviour
“Some of the medical officers in charge of the PMCIs were very negative towards it. They didn’t want to take it over and increase their burden of work. In my opinion, I feel if you see any deficiencies in other institutions that would be the main reason. For example, the two experienced doctors at XXX and YYY got themselves transferred just because their PMCI was selected for implementing PSSP, and they didn’t want to exert themselves with this project.”
3.2.4. Positive Aspect of Empanelment
“As you say if I get sick at a relative’s residence and they too are unaware of health conditions and when I am taken to hospital all my details will be available in the computer or book. That will be easy for everyone.”
“As one can access the data base (electronic PHR) via this number (PHN) it is good. I don’t know how far Sri Lanka uses this technology yet. But if the health system has this kind of thing it is valuable for quality care provision at hospitals.”
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Declaration of Astana. Global Conference on Primary Health Care; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Universal Health Coverage-Primary Health Care towards Universal Health Coverage. Report by the Director-General; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Bodenheimer, T.; Ghorob, A.; Willard-Grace, R.; Grumbach, K. The 10 Building Blocks of High-Performing Primary Care. Ann. Fam. Med. 2014, 12, 166–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bearden, T.; Ratcliffe, H.L.; Sugarman, J.R.; Bitton, A.; Anaman, L.A.; Buckle, G.; Cham, M.; Quan, D.C.W.; Ismail, F.; Jargalsaikhan, B.; et al. Empanelment: A Foundational Component of Primary Health Care. Gates Open Res. 2019, 3, 1654. [Google Scholar] [CrossRef] [PubMed]
- Pesec, M.; Ratcliffe, H.L.; Karlage, A.; Hirschhorn, L.R.; Gawande, A.; Bitton, A. Primary Health Care That Works: The Costa Rican Experience. Health Aff. Proj. Hope 2017, 36, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Özçelik, E.A.; Massuda, A.; Castro, M.C.; Barış, E. A Comparative Case Study: Does the Organization of Primary Health Care in Brazil and Turkey Contribute to Reducing Disparities in Access to Care? Health Syst. Reform 2021, 7, e1939931. [Google Scholar] [CrossRef] [PubMed]
- The World Bank; Health Nutrition and Population Global Practice. Project Appraisal Document: Primary Health Care System Strengthening Project; The World Bank: Washington, DC, USA, 2018. [Google Scholar]
- Ministry of Health Nutrition and Indigenous Medicine. Road Map for the Primary Healthcare System Strengthening Project (PSSP); Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2019.
- Ministry of Health Nutrition and Indigenous Medicine. Guidelines for Operationalizing Primary Medical Care Services in Sri Lanka; Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2019.
- Bitton, A.; Fifield, J.; Ratcliffe, H.; Karlage, A.; Wang, H.; Veillard, J.H.; Schwarz, D.; Hirschhorn, L.R. Primary Healthcare System Performance in Low-Income and Middle-Income Countries: A Scoping Review of the Evidence from 2010 to 2017. BMJ Glob. Health 2019, 4, e001551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creswell, J.; Clark, V.P. Designing and Conducting Mixed Methods Research, 2nd ed.; Sage Publications Ltd.: London, UK, 2010. [Google Scholar]
- DeJonckheere, M.; Vaughn, L.M. Semistructured Interviewing in Primary Care Research: A Balance of Relationship and Rigour. Fam. Med. Community Health 2019, 7, e000057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The World Bank. Sri Lanka|Data. Available online: https://data.worldbank.org/country/sri-lanka?view=chart (accessed on 6 January 2021).
- Department of Census and Statistics; Ministry of Finance and Planning; United Nations Population Fund. Census of Population and Housing 2012 Key Findings Department of Census and Statistics Ministry of Finance and Planning Supported by UNFPA, United Nations Population Fund Sri Lanka; Ministry of Finance and Planning: Colombo, Sri Lanka, 2012.
- Government of Sri Lanka. List of Codes for the Administrative Divisions of Sri Lanka 2001. Available online: https://web.archive.org/web/20110519151751/http://www.statistics.gov.lk/GNcode/introduction.pdf (accessed on 6 January 2021).
- Ministry of Health. Summary of Government Hospitals. Available online: http://www.health.gov.lk/moh_final/english/others.php?pid=92 (accessed on 7 January 2021).
- Govindaraj, R.; Navaratne, K.; Cavagnero, E.; Seshadri, S.R. Health Care in Sri Lanka: What Can the Private Health Sector Offer? The World Bank: Washington, DC, USA, 2014. [Google Scholar]
- Ministry of Health Nutrition and Indigenous Medicine. Reorganising Primary Health Care in Sri Lanka—Preserving Our Progress, Preparing Our Future; Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2017.
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Authority; Ministry of Health and Family Welfare; Government of India. Ayushman Bharat Digital Mission. Available online: https://abdm.gov.in/abdm-components (accessed on 6 January 2023).
- Farooq, M.; Arshad, M.I.; Usman, M. Towards Universal Health Coverage in Pakistan: Challenges Ahead. Lancet Reg. Health Southeast Asia 2022, 1, 100003. [Google Scholar] [CrossRef]
- Elrod, J.K.; Fortenberry, J.L. Advertising in Health and Medicine: Using Mass Media to Communicate with Patients. BMC Health Serv. Res. 2020, 20, 818. [Google Scholar] [CrossRef] [PubMed]
- Macinko, J.; Harris, M.J. Brazil’s Family Health Strategy—Delivering Community-Based Primary Care in a Universal Health System. N. Engl. J. Med. 2015, 372, 2177–2181. [Google Scholar] [CrossRef] [PubMed]
- VanderZanden, A.; Pesec, M.; Abrams, M.K.; Bitton, A.; Kennedy, A.; Ratcliffe, H.; Zephyrin, L.; Schwarz, D. Community-Oriented Primary Health Care Lessons from Costa Rica|Commonwealth Fund. Available online: https://www.commonwealthfund.org/publications/case-study/2021/mar/community-oriented-primary-care-lessons-costa-rica (accessed on 6 January 2023).
- Moosa, S. Community-Oriented Primary Care for National Health Insurance in South Africa. Afr. J. Prim. Health Care Fam. Med. 2022, 14, 3243. [Google Scholar] [CrossRef] [PubMed]
- Thekkur, P.; Fernando, M.; Nair, D.; Kumar, A.M.V.; Satyanarayana, S.; Chandraratne, N.; Chandrasiri, A.; Attygalle, D.E.; Higashi, H.; Bandara, J.; et al. Primary Health Care System Strengthening Project in Sri Lanka: Status and Challenges with Human Resources, Information Systems, Drugs and Laboratory Services. Healthcare 2022, 10, 2251. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.; Madiba, S. Barriers to the Implementation of the Ward-Based Outreach Team Program in Mpumalanga Province: Results from Process Evaluation. J. Prim. Care Community Health 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Huang, W.; Zheng, P.; Li, J.; Tao, S.; Tang, S.; Abdullah, A.S. Barriers and Facilitators of Engaging Community Health Workers in Non-Communicable Disease (NCD) Prevention and Control in China: A Systematic Review (2006–2016). Int. J. Environ. Res. Public Health 2018, 15, 2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rural Health Information Hub. Implementation Challenges for Community Health Worker Programs. Available online: https://www.ruralhealthinfo.org/toolkits/community-health-workers/4/implementation-challenges (accessed on 6 January 2023).
- Lim, J.; Broughan, J.; Crowley, D.; O’Kelly, B.; Fawsitt, R.; Burke, M.C.; McCombe, G.; Lambert, J.S.; Cullen, W. COVID-19’s Impact on Primary Care and Related Mitigation Strategies: A Scoping Review. Eur. J. Gen. Pract. 2021, 27, 175. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.C.; Pati, S.; Negi, S.; Patel, K.; Mishra, B.K.; Palo, S.K. Challenges in Maternal and Child Health Services Delivery and Access during Pandemics or Public Health Disasters in Low-and Middle-Income Countries: A Systematic Review. Healthcare 2021, 9, 828. [Google Scholar] [CrossRef] [PubMed]
- Nair, D.; Thekkur, P.; Fernando, M.; Kumar, A.M.V.; Satyanarayana, S.; Chandraratne, N.; Chandrasiri, A.; Attygalle, D.E.; Higashi, H.; Bandara, J.; et al. Outcomes and Challenges in Noncommunicable Disease Care Provision in Health Facilities Supported by Primary Health Care System Strengthening Project in Sri Lanka: A Mixed-Methods Study. Healthcare 2023, 11, 202. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thekkur, P.; Nair, D.; Fernando, M.; Kumar, A.M.V.; Satyanarayana, S.; Chandraratne, N.; Chandrasiri, A.; Attygalle, D.E.; Higashi, H.; Bandara, J.; et al. Empanelment of the Population to the Primary Medical Care Institution of Sri Lanka: A Mixed-Methods Study on Outcomes and Challenges. Healthcare 2023, 11, 575. https://doi.org/10.3390/healthcare11040575
Thekkur P, Nair D, Fernando M, Kumar AMV, Satyanarayana S, Chandraratne N, Chandrasiri A, Attygalle DE, Higashi H, Bandara J, et al. Empanelment of the Population to the Primary Medical Care Institution of Sri Lanka: A Mixed-Methods Study on Outcomes and Challenges. Healthcare. 2023; 11(4):575. https://doi.org/10.3390/healthcare11040575
Chicago/Turabian StyleThekkur, Pruthu, Divya Nair, Manoj Fernando, Ajay M. V. Kumar, Srinath Satyanarayana, Nadeeka Chandraratne, Amila Chandrasiri, Deepika Eranjanie Attygalle, Hideki Higashi, Jayasundara Bandara, and et al. 2023. "Empanelment of the Population to the Primary Medical Care Institution of Sri Lanka: A Mixed-Methods Study on Outcomes and Challenges" Healthcare 11, no. 4: 575. https://doi.org/10.3390/healthcare11040575