
Effect of an Integrated Physiotherapy Protocol on Knee Osteoarthritis Patients: A Preliminary Study

Abstract
:1. Introduction
2. Materials and Methods
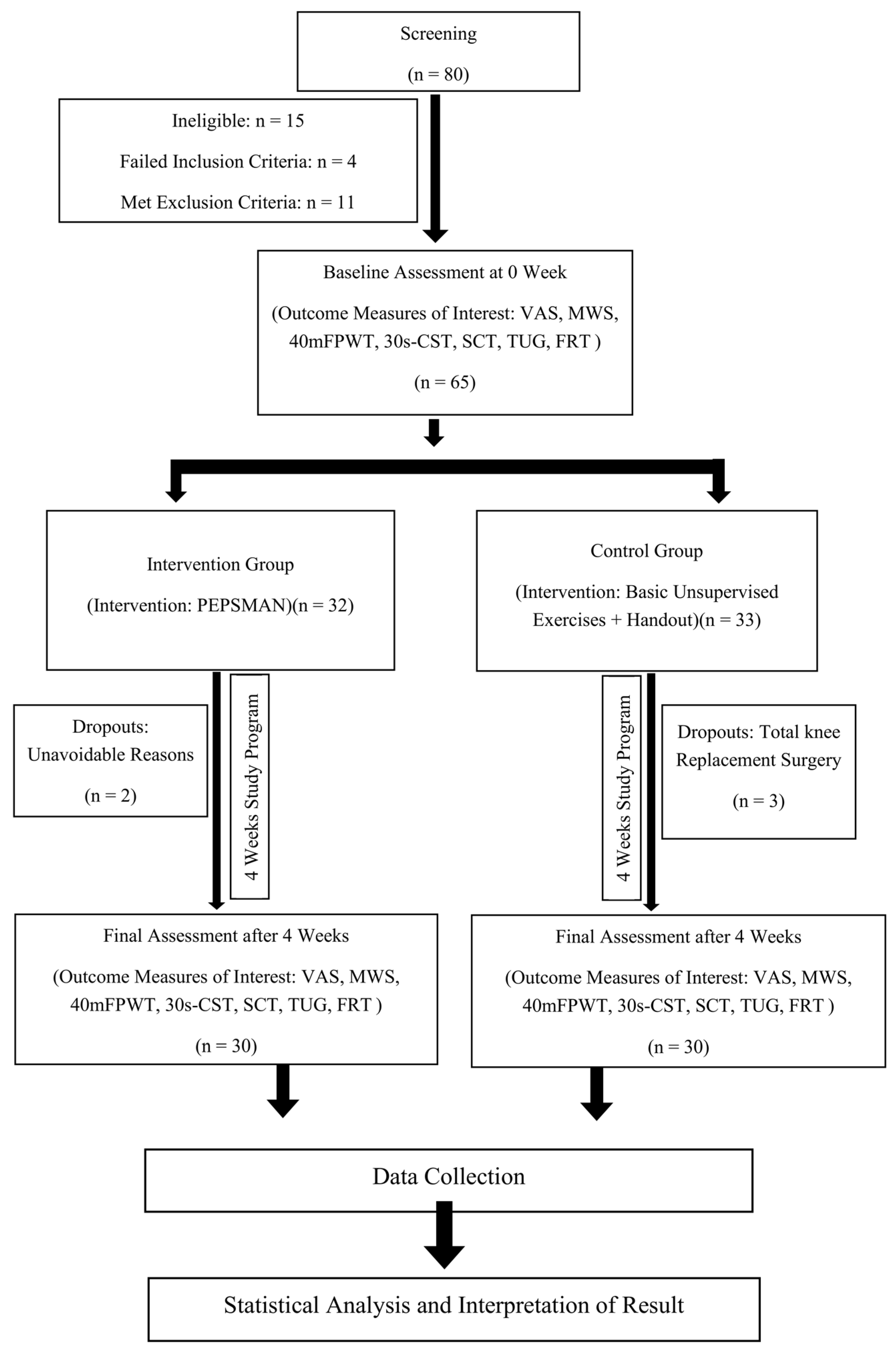
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Outcome Measure
2.5. Statistical Analyses
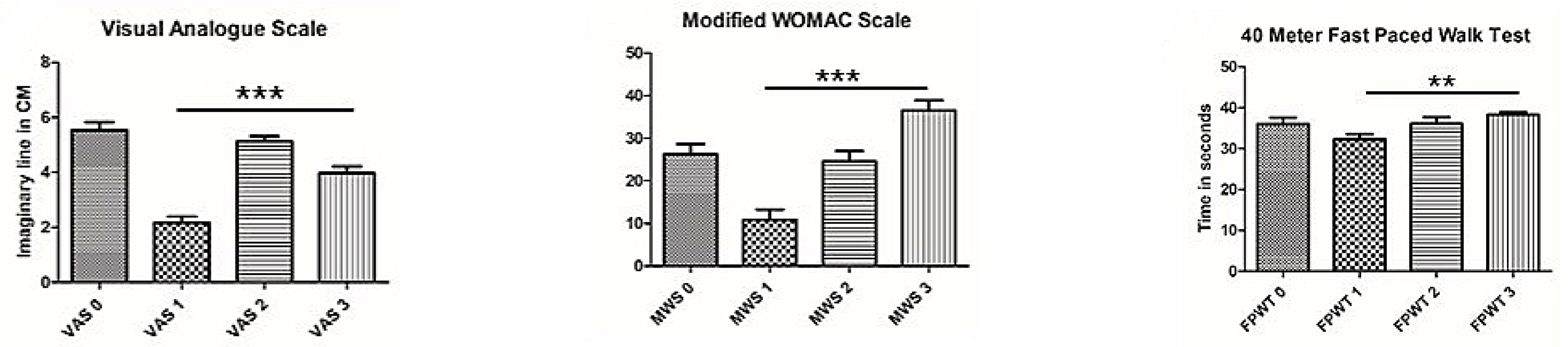
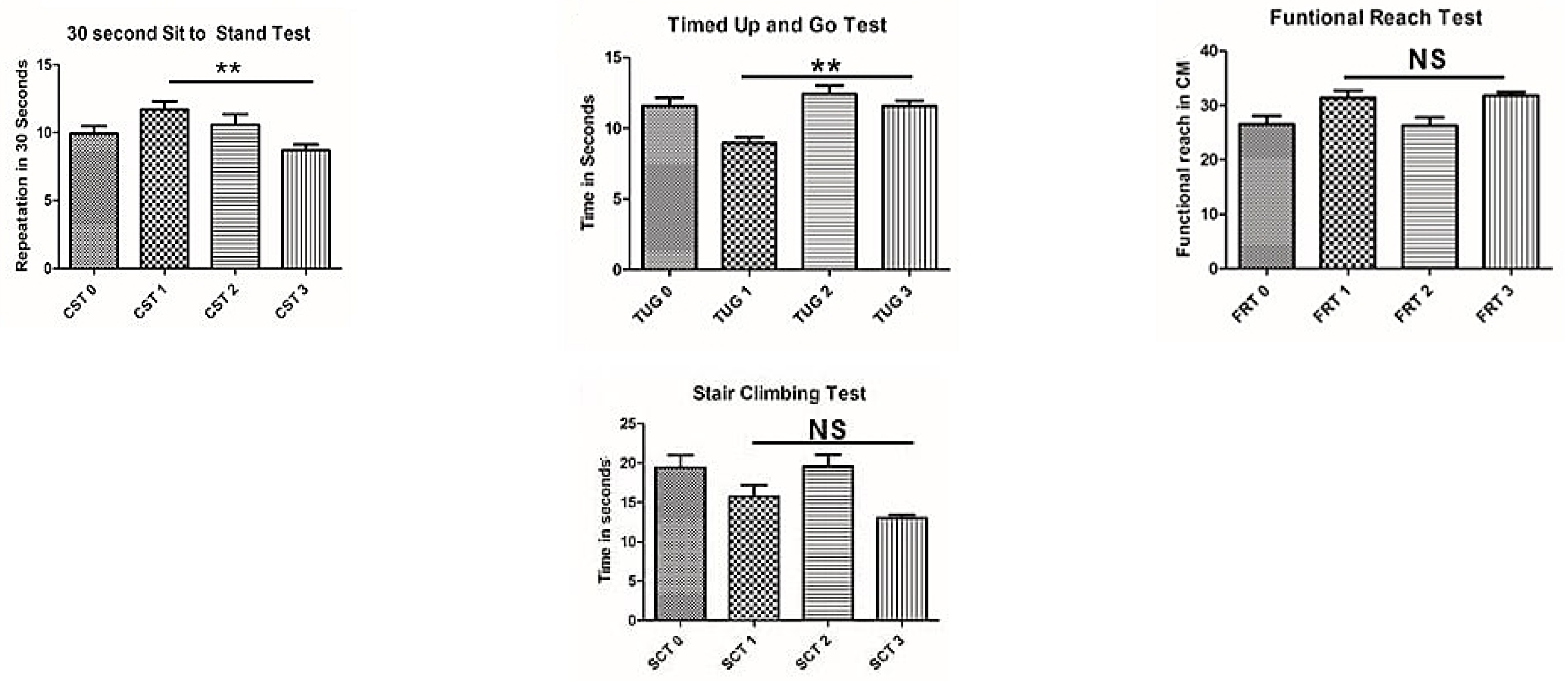
3. Results
4. Discussion
4.1. Strength of the Study
4.2. Limitations of the Study
4.3. Recommendations for Future Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, C.J.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sanchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal health conditions represent a global threat to healthy aging: A report for the 2015 World Health Organization world report on ageing and health. Gerontologist 2016, 56 (Suppl. 2), S243–S255. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29, 100587. [Google Scholar] [CrossRef]
- Kaur, R.; Sharma, V.L.; Singh, A. Prevalence of knee osteoarthritis and its correlation in women of rural and urban parts of Hoshiarpur (Punjab). J. Postgrad. Med. Educ. Res. 2015, 49, 32. [Google Scholar] [CrossRef]
- Odole, A.C.; Ogunlana, M.O.; Adegoke, B.O.; Ojonima, F.; Useh, U. Depression, pain and physical function in patients with osteoarthritis of the knee: Implications for interprofessional care. Niger. J. Med. Rehabil. 2015, 18. [Google Scholar] [CrossRef]
- Knoop, J.; Steultjens, M.P.; Van der Leeden, M.; Van der Esch, M.; Thorstensson, C.A.; Roorda, L.D.; Lems, W.F.; Dekker, J. Proprioception in knee osteoarthritis: A narrative review. Osteoarthr. Cartil. 2011, 19, 381–388. [Google Scholar] [CrossRef]
- Bascuas, I.; Tejero, M.; Monleón, S.; Boza, R.; Muniesa, J.M.; Belmonte, R. Balance 1 year after TKA: Correlation with clinical variables. Orthopedics 2013, 36, e6–e12. [Google Scholar] [CrossRef]
- Sharma, L.; Pai, Y.C.; Holtkamp, K.; Rymer, W.Z. Is knee joint proprioception worse in the arthritic knee versus the unaffected knee in unilateral knee osteoarthritis? Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1997, 40, 1518–1525. [Google Scholar] [CrossRef]
- Khalaj, N.; Abu Osman, N.A.; Mokhtar, A.H.; Mehdikhani, M.; Wan Abas, W.A. Balance and risk of fall in individuals with bilateral mild and moderate knee osteoarthritis. PLoS ONE 2014, 9, e92270. [Google Scholar] [CrossRef] [Green Version]
- Susanne, G.; Dominique, M. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9, F1000 Faculty Rev-325. [Google Scholar] [CrossRef]
- Felson, D.T. Priorities for osteoarthritis research: Much to be done. Nat. Rev. Rheumatol. 2014, 10, 447–448. [Google Scholar] [CrossRef] [PubMed]
- Dantas, L.O.; de Fátima Salvini, T.; McAlindon, T.E. Knee osteoarthritis: Key treatments and implications for physical therapy. Braz. J. Phys. Ther. 2021, 25, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; McConnell, S.; Harmer, A.R.; Van der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2015, 1, CD004376. [Google Scholar] [CrossRef] [PubMed]
- National Clinical Guideline Centre (UK). Osteoarthritis: Care and Management in Adults; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Brosseau, L.; Taki, J.; Desjardins, B.; Thevenot, O.; Fransen, M.; Wells, G.A.; Imoto, A.M.; Toupin-April, K.; Westby, M.; Gallardo, I.C.; et al. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Part one: Introduction, and mind-body exercise programs. Clin. Rehabil. 2017, 31, 582–595. [Google Scholar] [CrossRef]
- Brosseau, L.; Taki, J.; Desjardins, B.; Thevenot, O.; Fransen, M.; Wells, G.A.; Mizusaki Imoto, A.; Toupin-April, K.; Westby, M.; Alvarez Gallardo, I.C.; et al. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Part two: Strengthening exercise programs. Clin. Rehabil. 2017, 31, 596–611. [Google Scholar] [CrossRef]
- Brosseau, L.; Taki, J.; Desjardins, B.; Thevenot, O.; Fransen, M.; Wells, G.A.; Mizusaki Imoto, A.; Toupin-April, K.; Westby, M.; Alvarez Gallardo, I.C.; et al. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Part three: Aerobic exercise programs. Clin. Rehabil. 2017, 31, 612–624. [Google Scholar] [CrossRef]
- Fernandes, L.; Hagen, K.B.; Bijlsma, J.W.; Andreassen, O.; Christensen, P.; Conaghan, P.G.; Doherty, M.; Geenen, R.; Hammond, A.; Kjeken, I.; et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann. Rheum. Dis. 2013, 72, 1125–1135. [Google Scholar] [CrossRef] [Green Version]
- Hayami, T.A. Osteoarthritis of the knee joint as a cause of musculoskeletal ambulation disability symptom complex (MADS). Clin. Calcium 2008, 18, 1574–1580. [Google Scholar] [PubMed]
- Piyakhachornrot, N.; Aree-Ue, S.; Putwatana, P.; Kawinwonggowit, V. Impact of an integrated health education and exercise program in middle-aged Thai adults with osteoarthritis of the knee. Orthop. Nurs. 2011, 30, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Goff, A.J.; Silva, D.D.; Merolli, M.; Bell, E.C.; Crossley, K.M.; Barton, C.J. Patient education improves pain and function in people with knee osteoarthritis with better effects when combined with exercise therapy: A systematic review. J. Physiother. 2021, 67, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Rizvi, J. The effects of muscle energy technique and static stretching of gastrocnemius on pain and disability in knee osteoarthritis. Pak. J. Rehabil. 2018, 7, 32–37. [Google Scholar] [CrossRef]
- Abbott, J.H.; Chapple, C.M.; Fitzgerald, G.K.; Fritz, J.M.; Childs, J.D.; Harcombe, H.; Stout, K. The incremental effects of manual therapy or booster sessions in addition to exercise therapy for knee osteoarthritis: A randomized clinical trial. J. Orthop. Sport. Phys. Ther. 2015, 45, 975–983. [Google Scholar] [CrossRef]
- Anwer, S.; Alghadir, A.; Zafar, H.; Brismee, J.M. Effects of orthopaedic manual therapy in knee osteoarthritis: A systematic review and meta-analysis. Physiotherapy 2018, 104, 264–276. [Google Scholar] [CrossRef]
- Jorge, R.T.; Souza, M.C.; Chiari, A.; Jones, A.; Fernandes, A.D.; Júnior, I.L.; Natour, J. Progressive resistance exercise in women with osteoarthritis of the knee: A randomized controlled trial. Clin. Rehabil. 2015, 29, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Sartoyo, S.; Pradita, A.; Halimah, N. Perbandingan Frekuensi Kunjungan pada Pemberian Post Isometric Relaxation Muscle Energy Technique terhadap Peningkatan Kekuatan Otot Kondisi Knee Osteoarthritis di Rs. Dr. Soepraeon Kota Malang. J. Penelit. Kesehat. “SUARA FORIKES” (J. Health Res. “Voice”) 2022, 13, 136–139. [Google Scholar]
- Rangey, P.S.; Sheth, M.S.; Vyas, N.J. Comparison of Immediate Effect of Two Different Maitland Mobilization Protocols on Pain and Range Of Motion in Subjects with Osteoarthritis of Knee. Pain 2015, 6, 8. [Google Scholar]
- Luan, L.; Bousie, J.; Pranata, A.; Adams, R.; Han, J. Stationary cycling exercise for knee osteoarthritis: A systematic review and meta-analysis. Clin. Rehabil. 2021, 35, 522–533. [Google Scholar] [CrossRef]
- Rodica Trăistaru, M.; Kamal, D.; Constantin Kamal, K.; Ovidiu Alexandru, D.; Radu, M. Complex rehabilitation in patients with knee arthroplasty. Palestrica Third Millenn. Civiliz. Sport 2020, 21, 140–149. [Google Scholar] [CrossRef]
- Glossary. Spine 2000, 25, 3200–3202. Available online: https://journals.lww.com/spinejournal/fulltext/2000/12150/glossary.16.aspx (accessed on 27 November 2022). [CrossRef]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15, S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Price, D.D.; Harkins, S.W.; Baker, C. Sensory-affective relationships among different types of clinical and experimental pain. Pain 1987, 28, 297–307. [Google Scholar] [CrossRef]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Samuel, A.J.; Kanimozhi, D. Outcome measures used in patient with knee osteoarthritis: With special importance on functional outcome measures. Int. J. Health Sci. 2019, 13, 52. [Google Scholar]
- Bergquist, R.; Weber, M.; Schwenk, M.; Ulseth, S.; Helbostad, J.L.; Vereijken, B.; Taraldsen, K. Performance-based clinical tests of balance and muscle strength used in young seniors: A systematic literature review. BMC Geriatr. 2019, 19, 9. [Google Scholar] [CrossRef]
- Dobson, F.; Hinman, R.S.; Roos, E.M.; Abbott, J.H.; Stratford, P.; Davis, A.M.; Buchbinder, R.; Snyder-Mackler, L.; Henrotin, Y.; Thumboo, J.; et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1042–1052. [Google Scholar] [CrossRef]
- Maly, M.R.; Krupa, T. Personal experience of living with knee osteoarthritis among older adults. Disabil. Rehabil. 2007, 29, 1423–1433. [Google Scholar] [CrossRef]
- Nyvang, J.; Hedström, M.; Gleissman, S.A. It’s not just a knee, but a whole life: A qualitative descriptive study on patients’ experiences of living with knee osteoarthritis and their expectations for knee arthroplasty. Int. J. Qual. Stud. Health Well-Being 2016, 11, 30193. [Google Scholar] [CrossRef]
- Pouli, N.; Das Nair, R.; Lincoln, N.B.; Walsh, D. The experience of living with knee osteoarthritis: Exploring illness and treatment beliefs through thematic analysis. Disabil. Rehabil. 2014, 36, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Deyle, G.D.; Henderson, N.E.; Matekel, R.L.; Ryder, M.G.; Garber, M.B.; Allison, S.C. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee: A randomized, controlled trial. Ann. Intern. Med. 2000, 132, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Ko, T.; Lee, S.; Lee, D. Manual therapy and exercise for OA knee: Effects on muscle strength, proprioception, and functional performance. J. Phys. Ther. Sci. 2009, 21, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Abbott, J.H.; Robertson, M.C.; Chapple, C.; Pinto, D.; Wright, A.A.; De la Barra, S.L.; Baxter, G.D.; Theis, J.C.; Campbell, A.J.; MOA Trial Team. Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee: A randomized controlled trial. 1: Clinical effectiveness. Osteoarthr. Cartil. 2013, 21, 525–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| S. No. | Exercise | Description | Sets/Repetitions/Hold Time | Inter-Repetition/Inter-Set Rest Time | Duration | Supporting Evidence |
|---|---|---|---|---|---|---|
| 1. | Patient Education | Four Sessions | - | - | 4 weeks | Piyakhachornrot, N. et al., 2011 [23]; Goff, A.J. et al., 2021 [24] |
| 2. | Progressive Resistance Exercise (PRE) | With patient specific resistance, for:
| 3 sets of 10 repetitions with 10 s hold | 2 s between repetitions and 30 s between sets | 4 weeks | Khan, A.A. et al., 2018 [25]; Abbott, J.H. et al., 2015 [26] |
| 3. | Stretching Exercise | Therapist performed passive stretching of:
| Single set of 3 repetitions with 30 s hold | 30 s between repetitions | 4 weeks | Anwer et al., 2018 [27]; Abbott et al., 2015 [26] |
| Soft Tissue Manipulation (STM) |
| 3 to 5 min | - | 4 weeks | Abbott, J.H. et al., 2015 [26]; Jorge, R.T. et al., 2015 [28] | |
| 4. | Muscle Energy Technique (MET) | Post isometric relaxation technique was administered after application of 15 min of superficial moist heat to:
| Single set of 5 repetitions, isometric contraction for 5 s and passive stretch for 10 s. | 30 s between repetitions | 4 weeks | Sartoyo, S. et al., 2022 [29]; Khan, A.A. et al., 2018 [25] |
| Maitland Mobilization |
| Specific to patient’s needs | - | 4 weeks | Abbott, J.H. et al., 2015 [26]; Rangey, P.S. et al., 2015 [30] | |
| 5. | Aerobic Exercise | Pedo-Cycling: At patient specific self-selected speed and seat height | 3 sets of 50 repetitions | 30 s between sets | 4 weeks | Luan, L. et al., 2021 [31]; Abbott, J.H. et al., 2015 [26] |
| 6. | Neuromuscular Training: | Frenkel Exercise | 3 sets of 15 repetitions | 2 s between repetitions and 30 s between sets | 4 weeks | Rodica Trăistaru et al., 2020 [32]; Abbott et al., 2015 [26] |
| Standing balance on unstable surface | 3 sets of 3 repetitions with 60 s hold | 120 s between repetitions as well as between sets |
| Variables | Control Group (n = 30) | Intervention Group (n = 30) | ||
|---|---|---|---|---|
| Mean/Frequency | SD | Mean/frequency | SD | |
| Gender: | ||||
| Male (n) | 20 | 14 | ||
| Female (n) | 10 | 16 | ||
| Age (years) | 51.5 | (5.5) | 51.5 | (5.2) |
| Height (cm) | 160.6 | (9.2) | 159.1 | (9.0) |
| Weight (kg) | 70.4 | (13.5) | 71.1 | (13.1) |
| Body Mass Index | 27.8 | (7.3) | 28.02 | (4.0) |
| Grade of Osteoarthritis | 1.8 | (0.8) | 1.9 | (0.5) |
| Diabetes (n) | 5 | 7 | ||
| Inflammatory arthritis (n) | 1 | 2 | ||
| Thyroid (n) | 4 | 7 | ||
| Outcome Measures | PEPSMAN | Mean | SD | N |
|---|---|---|---|---|
| Visual Analogue Scale | Inter_P | 5.53 | 1.613 | 30 |
| Inter_Po | 2.17 | 1.234 | 30 | |
| Non_P | 5.13 | 1.008 | 30 | |
| Non_Po | 3.97 | 1.351 | 30 | |
| Total | 4.20 | 1.850 | 120 | |
| Modified WOMAC Scale | Inter_P | 25.80 | 13.664 | 30 |
| Inter_Po | 10.43 | 9.662 | 30 | |
| Non_P | 25.10 | 13.737 | 30 | |
| Non_Po | 37.00 | 7.497 | 30 | |
| Total | 24.58 | 14.755 | 120 | |
| 40 m Fast Paced Walk Test | Inter_P | 36.03 | 8.704 | 30 |
| Inter_Po | 32.30 | 6.993 | 30 | |
| Non_P | 36.07 | 8.952 | 30 | |
| Non_Po | 38.33 | 3.198 | 30 | |
| Total | 35.68 | 7.558 | 120 | |
| 30 s Chair Stand Test | Inter_P | 9.93 | 2.947 | 30 |
| Inter_Po | 11.70 | 3.292 | 30 | |
| Non_P | 10.57 | 4.329 | 30 | |
| Non_Po | 8.70 | 2.307 | 30 | |
| Total | 10.23 | 3.436 | 120 | |
| Stair Climb Test | Inter_P | 19.41 | 8.699 | 30 |
| Inter_Po | 15.77 | 7.811 | 30 | |
| Non_P | 19.53 | 8.545 | 30 | |
| Non_Po | 13.00 | 2.181 | 30 | |
| Total | 16.93 | 7.731 | 120 | |
| Timed Up and Go Test | Inter_P | 11.58 | 3.276 | 30 |
| Inter_Po | 8.97 | 2.266 | 30 | |
| Non_P | 12.43 | 3.191 | 30 | |
| Non_Po | 11.57 | 2.144 | 30 | |
| Total | 11.14 | 3.029 | 120 | |
| Functional Reach Test | Inter_P | 26.50 | 8.444 | 30 |
| Inter_Po | 31.43 | 7.295 | 30 | |
| Non_P | 26.30 | 8.197 | 30 | |
| Non_Po | 31.80 | 3.727 | 30 | |
| Total | 29.01 | 7.549 | 120 |
| Source | Dependent Variable | Type III Sum of Squares | df | Mean Square | F | Sig. | Partial Eta Squared | Noncent. Parameter | Observed Power h |
|---|---|---|---|---|---|---|---|---|---|
| Corrected Model | VAS | 207.423 a | 6 | 34.570 | 19.554 | 0.000 | 0.509 | 117.325 | 1.000 |
| MWS | 11,329.510 b | 6 | 1888.252 | 14.635 | 0.000 | 0.437 | 87.810 | 1.000 | |
| FPWT | 683.526 c | 6 | 113.921 | 2.105 | 0.058 | 0.101 | 12.632 | 0.736 | |
| CST | 157.733 d | 6 | 26.289 | 2.382 | 0.033 | 0.112 | 14.291 | 0.797 | |
| SCT | 1811.865 e | 6 | 301.978 | 6.439 | 0.000 | 0.255 | 38.632 | 0.999 | |
| TUG | 225.334 f | 6 | 37.556 | 4.896 | 0.000 | 0.206 | 29.378 | 0.989 | |
| FRT | 1148.139 g | 6 | 191.357 | 3.839 | 0.002 | 0.169 | 23.033 | 0.959 | |
| Intercept | VAS | 17.504 | 1 | 17.504 | 9.901 | 0.002 | 0.081 | 9.901 | 0.877 |
| MWS | 223.236 | 1 | 223.236 | 1.730 | 0.191 | 0.015 | 1.730 | 0.257 | |
| FPWT | 709.776 | 1 | 709.776 | 13.117 | 0.000 | 0.104 | 13.117 | 0.949 | |
| CST | 58.305 | 1 | 58.305 | 5.283 | 0.023 | 0.045 | 5.283 | 0.625 | |
| SCT | 180.330 | 1 | 180.330 | 3.845 | 0.052 | 0.033 | 3.845 | 0.494 | |
| TUG | 51.358 | 1 | 51.358 | 6.696 | 0.011 | 0.056 | 6.696 | 0.728 | |
| FRT | 1306.551 | 1 | 1306.551 | 26.211 | 0.000 | 0.188 | 26.211 | 0.999 | |
| Gender | VAS | 1.058 | 1 | 1.058 | 0.598 | 0.441 | 0.005 | 0.598 | 0.120 |
| MWS | 614.148 | 1 | 614.148 | 4.760 | 0.031 | 0.040 | 4.760 | 0.581 | |
| FPWT | 44.959 | 1 | 44.959 | 0.831 | 0.364 | 0.007 | 0.831 | 0.148 | |
| CST | 2.996 | 1 | 2.996 | 0.271 | 0.603 | 0.002 | 0.271 | 0.081 | |
| SCT | 10.367 | 1 | 10.367 | 0.221 | 0.639 | 0.002 | 0.221 | 0.075 | |
| TUG | 9.515 | 1 | 9.515 | 1.240 | 0.268 | 0.011 | 1.240 | 0.197 | |
| FRT | 171.653 | 1 | 171.653 | 3.444 | 0.066 | 0.030 | 3.444 | 0.452 | |
| age_yrs | VAS | 0.239 | 1 | 0.239 | 0.135 | 0.714 | 0.001 | 0.135 | 0.065 |
| MWS | 35.305 | 1 | 35.305 | 0.274 | 0.602 | 0.002 | 0.274 | 0.081 | |
| FPWT | 27.623 | 1 | 27.623 | 0.511 | 0.476 | 0.004 | 0.511 | 0.109 | |
| CST | 11.767 | 1 | 11.767 | 1.066 | 0.304 | 0.009 | 1.066 | 0.176 | |
| SCT | 702.350 | 1 | 702.350 | 14.975 | 0.000 | 0.117 | 14.975 | 0.970 | |
| TUG | 7.076 | 1 | 7.076 | 0.922 | 0.339 | 0.008 | 0.922 | 0.159 | |
| FRT | 20.015 | 1 | 20.015 | 0.402 | 0.528 | 0.004 | 0.402 | 0.096 | |
| BMI | VAS | 0.359 | 1 | 0.359 | 0.203 | 0.653 | 0.002 | 0.203 | 0.073 |
| MWS | 180.450 | 1 | 180.450 | 1.399 | 0.239 | 0.012 | 1.399 | 0.216 | |
| FPWT | 92.138 | 1 | 92.138 | 1.703 | 0.195 | 0.015 | 1.703 | 0.253 | |
| CST | 0.839 | 1 | 0.839 | 0.076 | 0.783 | 0.001 | 0.076 | 0.059 | |
| SCT | 255.285 | 1 | 255.285 | 5.443 | 0.021 | 0.046 | 5.443 | 0.638 | |
| TUG | 14.093 | 1 | 14.093 | 1.837 | 0.178 | 0.016 | 1.837 | 0.269 | |
| FRT | 33.370 | 1 | 33.370 | 0.669 | 0.415 | 0.006 | 0.669 | 0.128 | |
| PEPSMAN | VAS | 206.275 | 3 | 68.758 | 38.892 | 0.000 | 0.508 | 116.675 | 1.000 |
| MWS | 9779.811 | 3 | 3259.937 | 25.266 | 0.000 | 0.401 | 75.799 | 1.000 | |
| FPWT | 510.427 | 3 | 170.142 | 3.144 | 0.028 | 0.077 | 9.433 | 0.717 | |
| CST | 144.201 | 3 | 48.067 | 4.355 | 0.006 | 0.104 | 13.065 | 0.860 | |
| SCT | 894.736 | 3 | 298.245 | 6.359 | 0.001 | 0.144 | 19.077 | 0.963 | |
| TUG | 188.461 | 3 | 62.820 | 8.190 | 0.000 | 0.179 | 24.570 | 0.991 | |
| FRT | 825.118 | 3 | 275.039 | 5.518 | 0.001 | 0.128 | 16.553 | 0.934 |
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| Dependent Variable | PEPSMAN | Mean | Standard Error | Lower Bound | Upper Bound |
| Visual Analogue Scale | Inter_P | 5.512 a | 0.244 | 5.028 | 5.995 |
| Inter_Po | 2.145 a | 0.244 | 1.661 | 2.629 | |
| Non_P | 5.155 a | 0.244 | 4.671 | 5.639 | |
| Non_Po | 3.988 a | 0.244 | 3.505 | 4.472 | |
| Modified WOMAC Scale | Inter_P | 26.277 a | 2.086 | 22.145 | 30.410 |
| Inter_Po | 10.911 a | 2.086 | 6.778 | 15.043 | |
| Non_P | 24.623 a | 2.086 | 20.490 | 28.755 | |
| Non_Po | 36.523 a | 2.086 | 32.390 | 40.655 | |
| 40 m Fast Paced Walk Test | Inter_P | 36.151 a | 1.351 | 33.475 | 38.828 |
| Inter_Po | 32.418 a | 1.351 | 29.742 | 35.094 | |
| Non_P | 35.949 a | 1.351 | 33.272 | 38.625 | |
| Non_Po | 38.215 a | 1.351 | 35.539 | 40.891 | |
| 30 s Chair Stand Test | Inter_P | 9.969 a | 0.610 | 8.760 | 11.178 |
| Inter_Po | 11.736 a | 0.610 | 10.527 | 12.944 | |
| Non_P | 10.531 a | 0.610 | 9.322 | 11.740 | |
| Non_Po | 8.664 a | 0.610 | 7.456 | 9.873 | |
| Stair Climb Test | Inter_P | 19.444 a | 1.258 | 16.953 | 21.936 |
| Inter_Po | 15.798 a | 1.258 | 13.306 | 18.289 | |
| Non_P | 19.502 a | 1.258 | 17.011 | 21.994 | |
| Non_Po | 12.969 a | 1.258 | 10.478 | 15.461 | |
| Timed Up and Go Test | Inter_P | 11.632 a | 0.509 | 10.624 | 12.640 |
| Inter_Po | 9.022 a | 0.509 | 8.014 | 10.030 | |
| Non_P | 12.378 a | 0.509 | 11.370 | 13.386 | |
| Non_Po | 11.511 a | 0.509 | 10.504 | 12.519 | |
| Functional Reach Test | Inter_P | 26.776 a | 1.296 | 24.207 | 29.345 |
| Inter_Po | 31.709 a | 1.296 | 29.141 | 34.278 | |
| Non_P | 26.024 a | 1.296 | 23.455 | 28.593 | |
| Non_Po | 31.524 a | 1.296 | 28.955 | 34.093 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, S.A.; Parasher, P.; Ansari, M.A.; Parvez, S.; Fatima, N.; Alam, I. Effect of an Integrated Physiotherapy Protocol on Knee Osteoarthritis Patients: A Preliminary Study. Healthcare 2023, 11, 564. https://doi.org/10.3390/healthcare11040564
Khan SA, Parasher P, Ansari MA, Parvez S, Fatima N, Alam I. Effect of an Integrated Physiotherapy Protocol on Knee Osteoarthritis Patients: A Preliminary Study. Healthcare. 2023; 11(4):564. https://doi.org/10.3390/healthcare11040564
Chicago/Turabian StyleKhan, Sohrab Ahmad, Prithvi Parasher, Mairaj Ahmed Ansari, Suhel Parvez, Noor Fatima, and Iqbal Alam. 2023. "Effect of an Integrated Physiotherapy Protocol on Knee Osteoarthritis Patients: A Preliminary Study" Healthcare 11, no. 4: 564. https://doi.org/10.3390/healthcare11040564