
Digital Patient-Reported Outcome Measures Assessing Health-Related Quality of Life in Skull Base Diseases—Analysis of Feasibility and Pitfalls Two Years after Implementation
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Implementation of PROMs
2.3. Disease-Specific Selection of Questionnaires
- -
- Subgroup AMSB (anterior and middle skull base):patients with (mainly benign) tumors located in the region of the anterior or middle skull base (mostly meningiomas), excluding tumors of the sella.
- -
- Subgroup CPA (cerebellopontine angle):patients with (mainly benign) tumors located in the cerebellopontine angle or petroclival region (e.g., meningiomas, (vestibular) schwannomas, epidermoid cysts, etc.).
- -
- Subgroup NVC (neurovascular conflict):patients with neurovascular compression syndromes (mostly trigeminal neuralgia).
2.4. Statistical Analysis
3. Results
3.1. Availability of PROMs and Participation Rate
3.2. Conduction of PROMs in Relation to the COVID-19 Pandemic
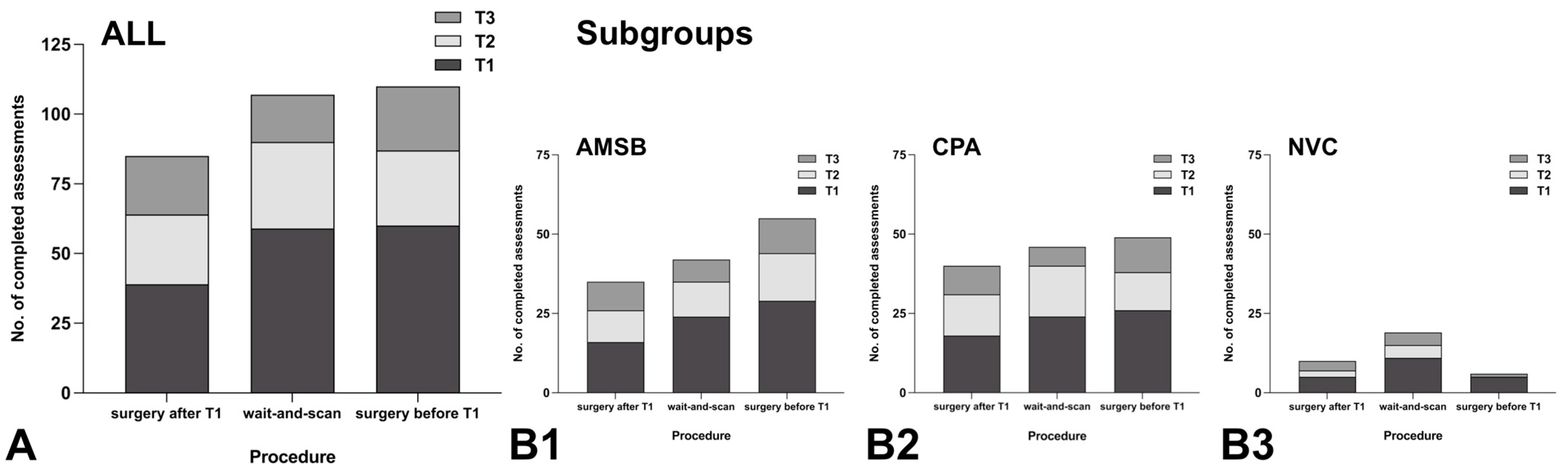
3.3. Response Rate to PROMs Depending on Subgroup and Neurosurgical Procedure
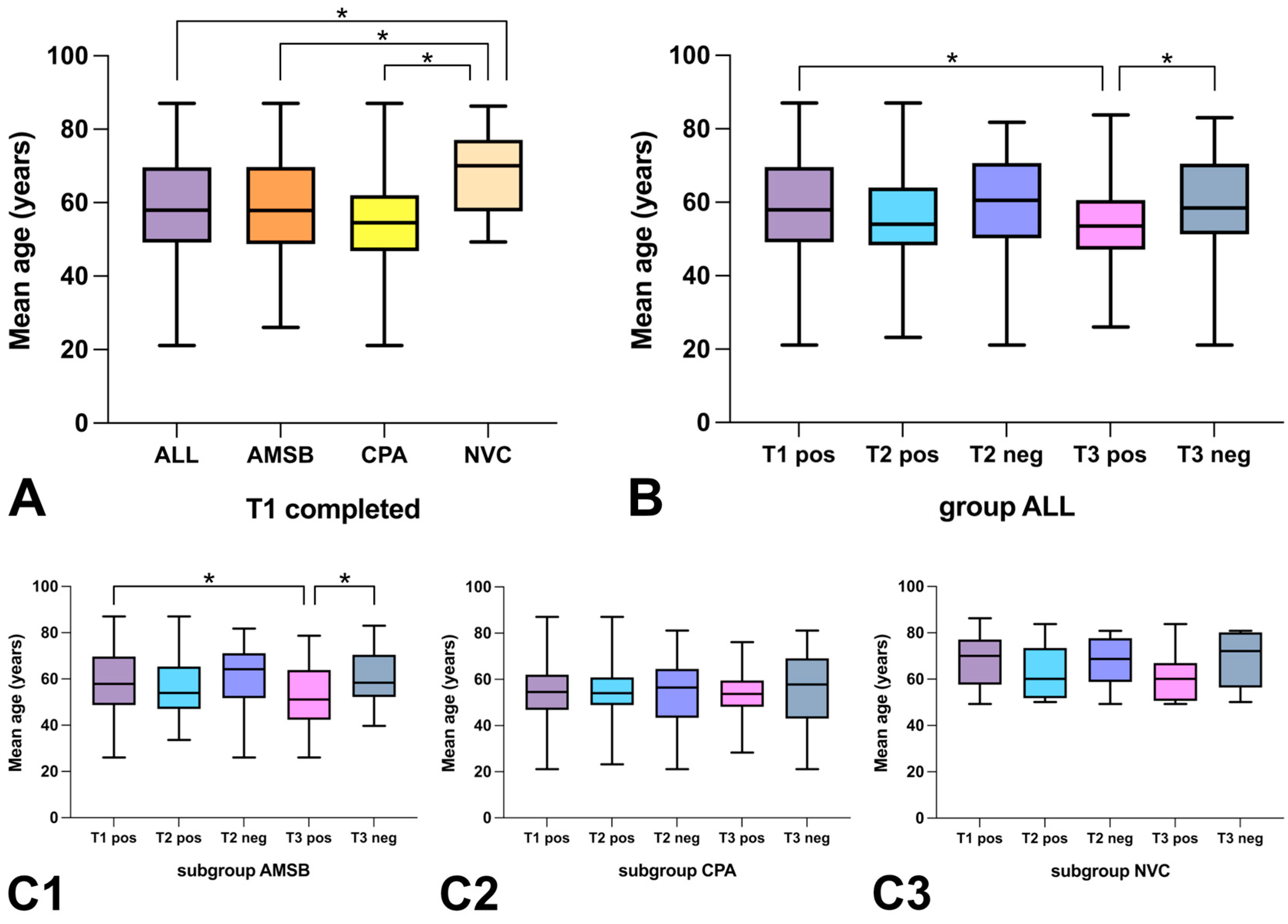
3.4. Response Rate to PROMs Depending on Age
3.5. Response Rate to PROMs Depending on Gender
4. Discussion
4.1. Availability of PROMs and Participation Rate
4.2. Conduction of PROMs in Relation to the COVID-19 Pandemic
4.3. Response Rate to PROMs Depending on Subgroup and Neurosurgical Procedure
4.4. Response Rate to PROMs Depending on Age
4.5. Response Rate to PROMs Depending on Gender
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Epstein, R.M.; Street, R.L. The Values and Value of Patient-Centered Care. Ann. Fam. Med. 2011, 9, 100–103. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Naik, A.D.; Dodson, J.A. Moving from Disease-Centered to Patient Goals-Directed Care for Patients with Multiple Chronic Conditions: Patient Value-Based Care. JAMA Cardiol. 2016, 1, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Ting, H.H.; Brito, J.P.; Montori, V.M. Shared Decision Making: Science and Action. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Briffa, N. The Employment of Patient-Reported Outcome Measures to Communicate the Likely Benefits of Surgery. Patient Relat. Outcome Meas. 2018, 9, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Légaré, F.; Stacey, D.; Turcotte, S.; Cossi, M.-J.; Kryworuchko, J.; Graham, I.D.; Lyddiatt, A.; Politi, M.C.; Thomson, R.; Elwyn, G.; et al. Interventions for Improving the Adoption of Shared Decision Making by Healthcare Professionals. Cochrane Database Syst. Rev. 2014, 9, CD006732. [Google Scholar] [CrossRef] [PubMed]
- Bender, M.; Tatagiba, M.; Gharabaghi, A. Quality of Life After Vestibular Schwannoma Surgery: A Question of Perspective. Front. Oncol. 2021, 11, 770789. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.; Taphoorn, M.J.B.; Drummond, K.J.; Walbert, T. Health-Related Quality of Life in Meningioma. Neurooncol. Adv. 2021, 3, vdab089. [Google Scholar] [CrossRef]
- Dammann, P.; Herten, A.; Santos, A.N.; Rauschenbach, L.; Chen, B.; Darkwah Oppong, M.; Schmidt, B.; Forsting, M.; Kleinschnitz, C.; Sure, U. Multimodal Outcome Assessment after Surgery for Brainstem Cavernous Malformations. J. Neurosurg. 2020, 135, 401–409. [Google Scholar] [CrossRef]
- De Witt Hamer, P.C.; De Witt Hamer, P.C.; Klein, M.; Hervey-Jumper, S.L.; Wefel, J.S.; Berger, M.S. Functional Outcomes and Health-Related Quality of Life Following Glioma Surgery. Neurosurgery 2021, 88, 720–732. [Google Scholar] [CrossRef] [PubMed]
- Dirven, L.; Vos, M.E.; Walbert, T.; Armstrong, T.S.; Arons, D.; van den Bent, M.J.; Blakeley, J.; Brown, P.D.; Bulbeck, H.; Chang, S.M.; et al. Systematic Review on the Use of Patient-Reported Outcome Measures in Brain Tumor Studies: Part of the Response Assessment in Neuro-Oncology Patient-Reported Outcome (RANO-PRO) Initiative. Neurooncol. Pract. 2021, 8, 417–425. [Google Scholar] [CrossRef]
- Passias, P.G.; Alas, H.; Bess, S.; Line, B.G.; Lafage, V.; Lafage, R.; Ames, C.P.; Burton, D.C.; Brown, A.; Bortz, C.; et al. Patient-Related and Radiographic Predictors of Inferior Health-Related Quality-of-Life Measures in Adult Patients with Nonoperative Spinal Deformity. J. Neurosurg. Spine 2021, 34, 907–913. [Google Scholar] [CrossRef]
- Pauwels, R.W.J.; Oterdoom, D.L.M.; Drost, G.; van Laar, T.; van Dijk, J.M.C. Long-Term Patient-Reported Outcome of Radiofrequency Thalamotomy for Tremor. Stereotact. Funct. Neurosurg. 2020, 98, 187–192. [Google Scholar] [CrossRef]
- Savchuk, S.; Jin, M.C.; Choi, S.; Kim, L.H.; Quon, J.L.; Bet, A.; Prolo, L.M.; Hong, D.S.; Mahaney, K.B.; Grant, G.A. Incorporating Patient-Centered Quality-of-Life Measures for Outcome Assessment after Chiari Malformation Type I Decompression in a Pediatric Population: A Pilot Study. J. Neurosurg. Pediatr. 2021, 29, 200–207. [Google Scholar] [CrossRef]
- Baba, A.; Saha, A.; McCradden, M.D.; Boparai, K.; Zhang, S.; Pirouzmand, F.; Edelstein, K.; Zadeh, G.; Cusimano, M.D. Development and Validation of a Patient-Centered, Meningioma-Specific Quality-of-Life Questionnaire. J. Neurosurg. 2021, 135, 1685–1694. [Google Scholar] [CrossRef]
- Ghimire, P.; Hasegawa, H.; Kalyal, N.; Hurwitz, V.; Ashkan, K. Patient-Reported Outcome Measures in Neurosurgery: A Review of the Current Literature. Neurosurgery 2018, 83, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Fuentealba-Bassaletti, C.; Neve, O.M.; van Esch, B.F.; Jansen, J.C.; Koot, R.W.; van Benthem, P.P.G.; Hensen, E.F. Vestibular Complaints Impact on the Long-Term Quality of Life of Vestibular Schwannoma Patients. Otol. Neurotol. 2023, 44, 161. [Google Scholar] [CrossRef] [PubMed]
- Soulier, G.; van Leeuwen, B.M.; Putter, H.; Jansen, J.C.; Malessy, M.J.A.; van Benthem, P.P.G.; van der Mey, A.G.L.; Stiggelbout, A.M. Quality of Life in 807 Patients with Vestibular Schwannoma: Comparing Treatment Modalities. Otolaryngol. Head Neck Surg. 2017, 157, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Robinett, Z.N.; Walz, P.C.; Miles-Markley, B.; Moberly, A.C.; Welling, D.B. Comparison of Long-Term Quality-of-Life Outcomes in Vestibular Schwannoma Patients. Otolaryngol. Head Neck Surg. 2014, 150, 1024–1032. [Google Scholar] [CrossRef]
- Pronk, Y.; Pilot, P.; Brinkman, J.M.; van Heerwaarden, R.J.; van der Weegen, W. Response Rate and Costs for Automated Patient-Reported Outcomes Collection Alone Compared to Combined Automated and Manual Collection. J. Patient Rep. Outcomes 2019, 3, 31. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.S.; Toonstra, J.L.; Meade, A.R.; Whale Conley, C.E.; Mattacola, C.G. Feasibility of Conducting a Web-Based Survey of Patient-Reported Outcomes and Rehabilitation Progress. Digit. Health 2016, 2, 2055207616644844. [Google Scholar] [CrossRef] [Green Version]
- Basch, E. Patient-Reported Outcomes: An Essential Component of Oncology Drug Development and Regulatory Review. Lancet Oncol. 2018, 19, 595–597. [Google Scholar] [CrossRef]
- Dirven, L.; Armstrong, T.S.; Taphoorn, M.J.B. Health-Related Quality of Life and Other Clinical Outcome Assessments in Brain Tumor Patients: Challenges in the Design, Conduct and Interpretation of Clinical Trials. Neurooncol. Pract. 2015, 2, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Kluetz, P.G.; Slagle, A.; Papadopoulos, E.J.; Johnson, L.L.; Donoghue, M.; Kwitkowski, V.E.; Chen, W.-H.; Sridhara, R.; Farrell, A.T.; Keegan, P.; et al. Focusing on Core Patient-Reported Outcomes in Cancer Clinical Trials: Symptomatic Adverse Events, Physical Function, and Disease-Related Symptoms. Clin. Cancer Res. 2016, 22, 1553–1558. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.C.; Eftimovska, E.; Lind, C.; Hager, A.; Wasson, J.H.; Lindblad, S. Patient Reported Outcome Measures in Practice. BMJ 2015, 350, g7818. [Google Scholar] [CrossRef]
- Fisher, F.L.; Zamanipoor Najafabadi, A.H.; van der Meer, P.B.; Boele, F.W.; Peerdeman, S.M.; Peul, W.C.; Taphoorn, M.J.B.; Dirven, L.; van Furth, W.R. Long-Term Health-Related Quality of Life and Neurocognitive Functioning after Treatment in Skull Base Meningioma Patients. J. Neurosurg. 2022, 136, 1077–1089. [Google Scholar] [CrossRef]
- Martinez-Perez, R.; Kortz, M.W.; Florez-Perdomo, W.; Ung, T.H.; Youssef, A.S. Endocrinological Outcomes after Transcranial Resection of Tuberculum Sellae Meningiomas: A Systematic Review and Meta-Analysis. Neurosurg. Rev. 2022, 45, 1965–1975. [Google Scholar] [CrossRef]
- Adegboyega, G.; Jordan, C.; Kawka, M.; Chisvo, N.; Toescu, S.M.; Hill, C. Quality of Life Reporting in the Management of Posterior Fossa Tumours: A Systematic Review. Front. Surg. 2022, 9, 970889. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Gandek, B.; Guyer, R.; Deng, N. Standardizing Disease-Specific Quality of Life Measures across Multiple Chronic Conditions: Development and Initial Evaluation of the QOL Disease Impact Scale (QDIS®). Health Qual. Life Outcomes 2016, 14, 84. [Google Scholar] [CrossRef]
- Nielsen, A.S.; Kidholm, K.; Kayser, L. Patients’ Reasons for Non-Use of Digital Patient-Reported Outcome Concepts: A Scoping Review. Health Inform. J. 2020, 26, 2811–2833. [Google Scholar] [CrossRef] [PubMed]
- Brochmann, N.; Zwisler, A.-D.; Kjerholt, M.; Flachs, E.M.; Hasselbalch, H.C.; Andersen, C.L. A New Internet-Based Tool for Reporting and Analysing Patient-Reported Outcomes and the Feasibility of Repeated Data Collection from Patients with Myeloproliferative Neoplasms. Qual. Life Res. 2016, 25, 835–846. [Google Scholar] [CrossRef]
- Kjær, A.S.H.K.; Rasmussen, T.A.; Hjollund, N.H.; Rodkjaer, L.O.; Storgaard, M. Patient-Reported Outcomes in Daily Clinical Practise in HIV Outpatient Care. Int. J. Infect. Dis. 2018, 69, 108–114. [Google Scholar] [CrossRef]
- Basch, E.; Dueck, A.C.; Rogak, L.J.; Minasian, L.M.; Kelly, W.K.; O’Mara, A.M.; Denicoff, A.M.; Seisler, D.; Atherton, P.J.; Paskett, E.; et al. Feasibility Assessment of Patient Reporting of Symptomatic Adverse Events in Multicenter Cancer Clinical Trials. JAMA Oncol. 2017, 3, 1043–1050. [Google Scholar] [CrossRef]
- Chen, J.; Ou, L.; Hollis, S.J. A Systematic Review of the Impact of Routine Collection of Patient Reported Outcome Measures on Patients, Providers and Health Organisations in an Oncologic Setting. BMC Health Serv. Res. 2013, 13, 211. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.H.; Lee, J.W.; Shin, Y.-W.; Jo, M.-W.; Sohn, G.; Lee, J.-H.; Lee, G.; Jung, K.H.; Sung, J.; Ko, B.S.; et al. Daily Collection of Self-Reporting Sleep Disturbance Data via a Smartphone App in Breast Cancer Patients Receiving Chemotherapy: A Feasibility Study. J. Med. Internet Res. 2014, 16, e135. [Google Scholar] [CrossRef]
- Melissant, H.C.; Verdonck-de Leeuw, I.M.; Lissenberg-Witte, B.I.; Konings, I.R.; Cuijpers, P.; Van Uden-Kraan, C.F. “Oncokompas”, a Web-Based Self-Management Application to Support Patient Activation and Optimal Supportive Care: A Feasibility Study among Breast Cancer Survivors. Acta Oncol. 2018, 57, 924–934. [Google Scholar] [CrossRef]
- Wintner, L.M.; Giesinger, J.M.; Zabernigg, A.; Rumpold, G.; Sztankay, M.; Oberguggenberger, A.S.; Gamper, E.M.; Holzner, B. Evaluation of Electronic Patient-Reported Outcome Assessment with Cancer Patients in the Hospital and at Home. BMC Med. Inform. Decis. Mak. 2015, 15, 110. [Google Scholar] [CrossRef]
- Bauer, A.M.; Iles-Shih, M.; Ghomi, R.H.; Rue, T.; Grover, T.; Kincler, N.; Miller, M.; Katon, W.J. Acceptability of MHealth Augmentation of Collaborative Care: A Mixed Methods Pilot Study. Gen. Hosp. Psychiatry 2018, 51, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Benze, G.; Nauck, F.; Alt-Epping, B.; Gianni, G.; Bauknecht, T.; Ettl, J.; Munte, A.; Kretzschmar, L.; Gaertner, J. PROutine: A Feasibility Study Assessing Surveillance of Electronic Patient Reported Outcomes and Adherence via Smartphone App in Advanced Cancer. Ann. Palliat. Med. 2019, 8, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Blocker, O.; Bullock, A.; Morgan-Jones, R.; Ghandour, A.; Richardson, J. Using Text Messaging in Long-Term Arthroplasty Follow-Up: A Pilot Study. JMIR Res. Protoc. 2017, 6, e88. [Google Scholar] [CrossRef]
- Gossec, L.; Cantagrel, A.; Soubrier, M.; Berthelot, J.-M.; Joubert, J.-M.; Combe, B.; Czarlewski, W.; Wendling, D.; Dernis, E.; Grange, L.; et al. An E-Health Interactive Self-Assessment Website (Sanoia®) in Rheumatoid Arthritis. A 12-Month Randomized Controlled Trial in 320 Patients. Jt. Bone Spine 2018, 85, 709–714. [Google Scholar] [CrossRef]
- Jiang, Y.; Sereika, S.M.; Dabbs, A.D.; Handler, S.M.; Schlenk, E.A. Acceptance and Use of Mobile Technology for Health Self-Monitoring in Lung Transplant Recipients during the First Year Post-Transplantation. Appl. Clin. Inform. 2016, 7, 430–445. [Google Scholar] [CrossRef] [PubMed]
- Pahlevan Sharif, S.; She, L.; Liu, L.; Naghavi, N.; Lola, G.K.; Sharif Nia, H.; Froelicher, E.S. Retaining Nurses via Organizational Support and Pay during COVID-19 Pandemic: The Moderating Effect between Intrinsic and Extrinsic Incentives. Nurs. Open 2022, 10, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Schug, C.; Geiser, F.; Hiebel, N.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Morawa, E.; Erim, Y. Sick Leave and Intention to Quit the Job among Nursing Staff in German Hospitals during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1947. [Google Scholar] [CrossRef] [PubMed]
- Khalafallah, A.M.; Rakovec, M.; Burapachaisri, K.; Fung, S.; Kozachik, S.L.; Valappil, B.; Abou-Al-Shaar, H.; Wang, E.W.; Snyderman, C.H.; Zenonos, G.A.; et al. The Suprasellar Meningioma Patient-Reported Outcome Survey: A Disease-Specific Patient-Reported Outcome Measure for Resection of Suprasellar Meningioma. J. Neurosurg. 2021, 136, 1551–1559. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| In Total | Subgroups | ||||
|---|---|---|---|---|---|
| ALL | AMSB | CPA | NVC | ||
| Total no. of Patients with Completed T1 (n) | 158 | 69 | 68 | 21 | |
| no. of patients with completed T1 per procedure (n, % in relation to no. of T1 of the corresponding group) | surgery between T1 and T2 | 39 (24.7%) | 16 (23.2%) | 18 (26.5%) | 5 (23.8%) |
| wait-and-scan strategy | 59 (37.3%) | 24 (34.8%) | 24 (35.3%) | 11 (52.4%) | |
| previous surgery before T1 § | 60 (38.0%) | 29 (42.0%) | 26 (38.2%) | 5 (23.8%) | |
| total no. of patients with completed T2 (n) | 83 | 36 | 41 & | 6 && | |
| no. of patients with completed T2 per procedure (n, % in relation to no. of T2 of the corresponding group) | surgery between T1 and T2 | 25 (30.1%) | 10 (27.8%) | 13 (31.7%) | 2 (33.3%) |
| wait-and-scan strategy | 31 (37.4%) | 11 (30.5%) | 16 (39.0%) | 4 (66.7%) | |
| previous surgery before T1 | 27 (32.5%) | 15 (41.7%) | 12 (29.3%) | 0 (0.0%) | |
| total no. of patients with completed T3 (n) | 61 | 27 # | 26 ## | 8 ### | |
| no. of patients with completed T3 per procedure (n, % in relation to no. of T3 of the corresponding group) | surgery between T1 and T2 | 21 (34.4%) | 9 (33.3%) | 9 (34.6%) | 3 (37.5%) |
| wait-and-scan strategy | 17 (27.9%) | 7 (25.9%) | 6 (23.1%) | 4 (50.0%) | |
| previous surgery before T1 | 23 (37.7%) | 11 (40.8%) | 11 (42.3%) | 1 (12.5%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steiert, C.; Lambeck, J.; Grauvogel, T.D.; Beck, J.; Grauvogel, J. Digital Patient-Reported Outcome Measures Assessing Health-Related Quality of Life in Skull Base Diseases—Analysis of Feasibility and Pitfalls Two Years after Implementation. Healthcare 2023, 11, 472. https://doi.org/10.3390/healthcare11040472
Steiert C, Lambeck J, Grauvogel TD, Beck J, Grauvogel J. Digital Patient-Reported Outcome Measures Assessing Health-Related Quality of Life in Skull Base Diseases—Analysis of Feasibility and Pitfalls Two Years after Implementation. Healthcare. 2023; 11(4):472. https://doi.org/10.3390/healthcare11040472
Chicago/Turabian StyleSteiert, Christine, Johann Lambeck, Tanja Daniela Grauvogel, Juergen Beck, and Juergen Grauvogel. 2023. "Digital Patient-Reported Outcome Measures Assessing Health-Related Quality of Life in Skull Base Diseases—Analysis of Feasibility and Pitfalls Two Years after Implementation" Healthcare 11, no. 4: 472. https://doi.org/10.3390/healthcare11040472