


Vaccine Hesitancy among Medical Students at a Tertiary Hospital—Affiliated Medical School
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Data Collection
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
3.1. Participant Characteristics
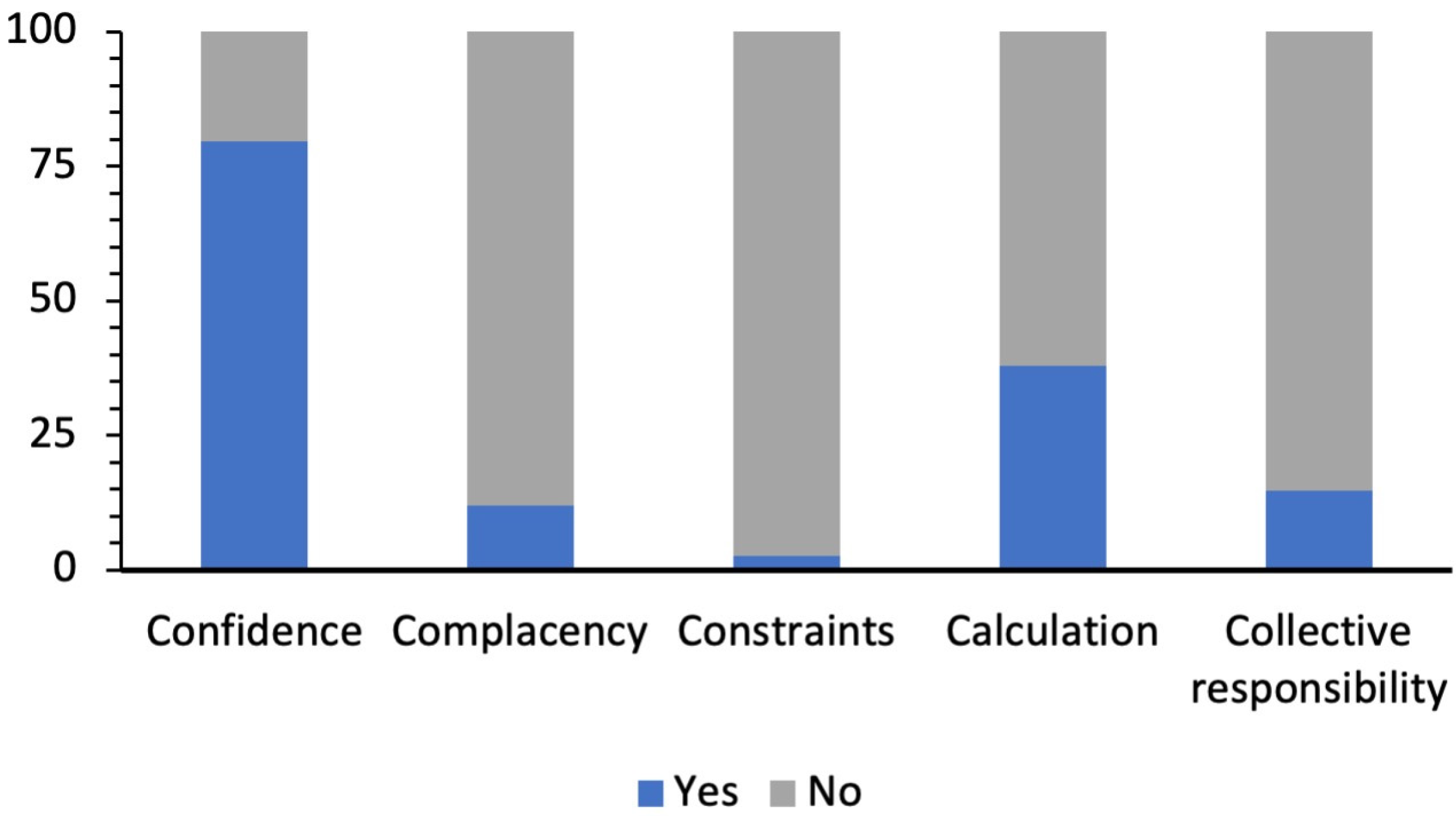
3.2. COVID-19 Psychological Antecedents
3.3. Bivariate Analyses
3.4. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19). 2021. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 10 December 2021).
- DeSalvo, K.; Hughes, B.; Bassett, M.; Benjamin, G.; Fraser, M.; Galea, S.; Gracia, J.N.; Howard, J. Public Health COVID-19 impact assessment: Lessons learned and compelling needs. NAM Perspect. 2021, 2021. [Google Scholar] [CrossRef]
- International Myeloma Foundation. Policy Responses to COVID19. 2021. Available online: https://www.imf.org/en/Topics/imf-andcovid19/Policy-Responses-to-COVID-19 (accessed on 15 December 2021).
- United States Department of the Treasury. Covid-19 Economic Relief. 2021. Available online: https://home.treasury.gov/policy-issues/coronavirus (accessed on 15 December 2021).
- France 24. Lebanon announces two-week lockdown over coronavirus. 2020. Available online: https://www.france24.com/en/20200315-lebanon-announces-two-week-lockdown-over-coronavirus (accessed on 15 December 2021).
- English Al Arabiya. Coronavirus: Kuwait to Impose Full Lockdown, Curfew for 20 Days Starting May 10. 2021. Available online: https://english.alarabiya.net/coronavirus/2020/05/08/Coronavirus-Kuwait-to-impose-20-day-totalcurfew-from-May-10 (accessed on 9 December 2021).
- India Today. Coronavirus in India: 277 Indians from Iran Reach Jodhpur. 2020. Available online: https://www.indiatoday.in/india/story/novel-coronavirus-covid19-latest-news-update-indialockdown-confirmed-positive-cases-deaths-uk-usa-italy-iran-china-1658922-2020-03-24 (accessed on 8 December 2021).
- Reuters. Factbox: Countries Making COVID-19 Vaccines Mandatory. 2021. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/countries-making-covid-19-vaccines-mandatory-2021-08-16/ (accessed on 19 December 2021).
- Council on Foreign Relations. A Guide to Global Covid-19 Vaccine Efforts. 2022. Available online: https://www.cfr.org/backgrounder/guide-global-covid-19-vaccine-efforts (accessed on 10 August 2022).
- Centers for Disease Control and Prevention. SARS-CoV-2 Variant Classifications and Definitions. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html (accessed on 4 December 2021).
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.W. Omicron (B.1.1.529): Infectivity, vaccine breakthrough, and antibody resistance. arXiv 2021, arXiv:2112.01318v1. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Macdonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Butler, R.; MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Diagnosing the determinants of vaccine hesitancy in specific subgroups: The Guide to Tailoring Immunization Programmes (TIP). Vaccine 2015, 33, 4176–4179. [Google Scholar] [CrossRef]
- World Health Organization. Ten Health Issues Who Will Tackle this Year. 2021. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 10 December 2021).
- Gangarosa, E.; Galazka, A.; Wolfe, C.; Phillips, L.; Miller, E.; Chen, R. Impact of anti-vaccine movements on pertussis control: The untold story. Lancet 1998, 351, 356–361. [Google Scholar] [CrossRef]
- Dube, E.; Vivion, M.; MacDonald, N.E. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2015, 14, 99–117. [Google Scholar] [CrossRef]
- Ainslie, D.; Ogwuru, C.; Sinclair, R. Great Britain: Office for National Statistics. Coronavirus and Vaccine Hesitancy, Great Britain: 9 August 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandvaccinehesitancygreatbritain/9august2021 (accessed on 10 August 2022).
- Kelekar, A.K.; Lucia, V.C.; Afonso, N.M.; Mascarenhas, A.K. COVID-19 vaccine acceptance and hesitancy among dental and medical students. J. Am. Dent. Assoc. 2021, 152, 596–603. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2020, 43, 445–449. [Google Scholar] [CrossRef]
- Jain, J.; Saurabh, S.; Kumar, P.; Verma, M.K.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect. 2021, 149, e132. [Google Scholar] [CrossRef]
- Riyadh Urban Observatory. Riyadh City. 2022. Available online: http://www.ruo.gov.sa/RiyadhCity (accessed on 5 January 2022).
- ElHafeez, S.A.; Elbarazi, I.; Shaaban, R.; ElMakhzangy, R.; Aly, M.O.; Alnagar, A.; Yacoub, M.; El Saeh, H.M.; Eltaweel, N.; Alqutub, S.T.; et al. Arabic validation and cross-cultural adaptation of the 5C scale for assessment of COVID-19 vaccines psychological antecedents. PLoS ONE 2021, 16, e0254595. [Google Scholar] [CrossRef]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5C validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Ghazy, R.M.; ElHafeez, S.A.; Shaaban, R.; Elbarazi, I.; Abdou, M.S.; Ramadan, A.; Kheirallah, K.A. Determining the cutoff points of the 5C scale for assessment of COVID-19 vaccines psychological antecedents among the Arab population: A multinational study. J. Prim. Care Community Health 2021, 12, 21501327211018568. [Google Scholar] [CrossRef]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Rabin, K.; Ratzan, S.C.; Leigh, J.P.; Hu, J.; El-Mohandes, A. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat. Commun. 2022, 13, 3801. [Google Scholar] [CrossRef]
- Dai, D. Three in Four Adults Globally Say They’d Get a Vaccine for COVID-19–but is this Enough. In World Econ. Forum. 2020. Available online: https://www.weforum.org/press/2020/08/three-in-four-adults-globally-say-they-d-get-a-vaccine-for-covid-19-but-is-this-enough/ (accessed on 22 December 2021).
- Anyiam-Osigwe, T. COVID-19 Vaccines Are Now Approved in Some Countries. What Will It Take to Approve Them for the Rest of the World? Retrieved from the GAVI Website. 2021. Available online: https://www.gavi.org/vaccineswork/covid-19-vaccines-are-now-approved-some-countries-what-will-it-take-approve-them (accessed on 24 December 2022).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID19 vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The nature and extent of COVID-19 vaccination hesitancy in healthcare workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef]
- Hamel, L.; Kirzinger, A.; Munana, C.; Brodie, M. KFF COVID-19 Vaccine Monitor. 2020. Available online: https://www.kf.org/coronaviruscovid-19/report/kf-covid-19-vaccine-monitor-december-2020/ (accessed on 15 December 2020).
- Elharake, J.A.; Galal, B.; Alqahtani, S.A.; Kattan, R.F.; Barry, M.A.; Temsah, M.-H.; Malik, A.A.; McFadden, S.M.; Yildirim, I.; Khoshnood, K.; et al. COVID-19 vaccine acceptance among health care workers in the Kingdom of Saudi Arabia. Int. J. Infect. Dis. 2021, 109, 286–293. [Google Scholar] [CrossRef]
- Qunaibi, E.A.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy among Arabs: Results of a large-scale survey. eLife 2021, 10, e68038. [Google Scholar] [CrossRef]


{kind=link}
| Term | Definition |
|---|---|
| Confidence | “Trust in (i) the effectiveness and safety of vaccines, (ii) the system that delivers them, including the reliability and competence of the health services and health professionals, and (iii) the motivations of policy-makers who decide on the need of vaccines.” [25] |
| Complacency | “Complacency exists where perceived risks of vaccine-preventable diseases are low and vaccination is not deemed a necessary preventive action.” [25] |
| Constraints | “Constraints can manifest in limited physical availability, affordability and willingness-to-pay, geographical accessibility, ability to understand (language and health literacy) and appeal of immunization service.” [25] |
| Calculation | “Individuals’ engagement in extensive information searching.” [26] |
| Collective responsibility | “Willingness to protect others by one’s own vaccination by means of herd immunity.” [26] |
| Variable | n | % | |
|---|---|---|---|
| (n = 266) | |||
| Sex | Female | 120 | 45.1 |
| Male | 146 | 54.9 | |
| Academic year | 1st | 82 | 30.8 |
| 2nd | 33 | 12.4 | |
| 3rd | 95 | 35.7 | |
| 4th | 27 | 10.2 | |
| 5th | 29 | 10.9 | |
| Age (mean ± SD) | 21.3 ± 1.7 | ||
| Social status | Single | 263 | 98.9 |
| Married | 3 | 1.1 | |
| Chronic illness(es) | 25 | 9.4 | |
| Annual receipt of the influenza vaccine | 97 | 36.5 | |
| Previous infection with SARS-CoV-2 1 | 89 | 33.5 | |
| Family member with previous SARS-CoV-2 infection | 200 | 75.2 | |
| Family member or friend passed away due to COVID-19 2 | 76 | 28.6 | |
| Aware of the availability of multiple COVID-19 vaccines | 264 | 99.3 | |
| Vaccinated against COVID-19 | 266 | 100 | |
| Perceived best vaccine | |||
| Pfizer-BioNTech Oxford-AstraZeneca Moderna Sinopharm | 232 | 87.2 | |
| 23 | 8.7 | ||
| 7 | 2.6 | ||
| 4 | 1.5 | ||
| Knew of a family member or friend who had been infected with COVID-19 after receiving vaccination | 224 | 84.2 | |
| Read precautions provided by the local authorities related to COVID-19 vaccination | 106 | 39.9 | |
| Searched for information related to COVID-19 vaccination online | 172 | 64.7 | |
| Free COVID-19 vaccine as an influential factor in receiving it | 168 | 63.2 | |
| Variable | Confidence | ||
|---|---|---|---|
| n (%) | p-Value | ||
| Yes | No | ||
| Sex | |||
| Female | 92 (76.7) | 28 (23.3) | 0.265 |
| Male | 120 (82.2) | 26 (17.8) | |
| Academic Year | |||
| 2nd year | 54 (65.9) | 28 (34.2) | <0.001 1 |
| 3rd year | 31 (93.9) | 2 (6.1) | |
| 4th year | 84 (88.4) | 11 (11.6) | |
| 5th year | 22 (81.5) | 5 (18.5) | |
| 6th year | 21 (72.4) | 8 (27.6) | |
| Chronic illness(es) | 20 (80.0) | 5 (20.0) | 0.969 |
| Annual receipt of influenza vaccine | 79 (81.4) | 18 (18.6) | 0.592 |
| Previous infection with SARS-CoV-2 * | 65 (73.0) | 24 (27.0) | 0.021 1 |
| Family member with previous SARS-CoV-2 infection | 154 (77.0) | 46 (23.0) | 0.161 |
| Family member or friend passed away due to COVID-19 ** | 58 (76.3) | 18 (23.7) | 0.057 |
| Perceived Best COVID-19 Vaccine | |||
| Pfizer-BioNTech | 187 (80.6) | 45 (19.4) | 0.202 2 |
| Oxford-AstraZeneca | 19 (82.6) | 4 (17.4) | |
| Moderna | 4 (57.1) | 3 (42.9) | |
| Sinopharm | 2 (50.0) | 2 (50.0) | |
| Knew a family member or friend who had been infected with SARS-CoV-2 after receiving vaccination | 174 (77.7) | 50 (22.3) | 0.059 2 |
| Read precautions provided by the local authorities for COVID-19 vaccination | 88 (83.0) | 18 (17.0) | 0.273 |
| Searched for information related to COVID-19 vaccination online | 140 (81.4) | 32 (18.6) | 0.352 |
| Free COVID-19 vaccine as an influential factor in receiving it | 141 (83.9) | 27 (16.1) | 0.025 1 |
| Variable | Complacency | ||
|---|---|---|---|
| n (%) | p-Value | ||
| Yes | No | ||
| Sex | |||
| Female | 16 (13.3) | 104 (86.7) | 0.554 |
| Male | 16 (11) | 130 (89) | |
| Academic Year | |||
| 2nd year | 11 (13.4) | 71 (86.6) | 0.919 2 |
| 3rd year | 5 (15.2) | 28 (84.8) | |
| 4th year | 11 (11.6) | 84 (88.4) | |
| 5th year | 2 (7.41) | 25 (92.6) | |
| 6th year | 3 (10.4) | 26 (89.7) | |
| Chronic illness(es) | 4 (16.0) | 21 (84.0) | 0.518 2 |
| Annual receipt of influenza vaccine | 9 (9.3) | 88 (90.7) | 0.296 |
| Previous infection with SARS-CoV-2 * | 14 (15.7) | 75 (84.3) | 0.404 |
| Family member with previous SARS-CoV-2 * infection | 22 (11.0) | 178 (89.0) | 0.001 1 |
| Family member or friend passed away due to COVID-19 ** | 11 (14.5) | 65 (85.5) | 0.047 1 |
| Perceived Best COVID-19 Vaccine | |||
| Pfizer-BioNTech | 25 (10.8) | 207 (89.2) | 0.052 2 |
| Oxford-AstraZeneca | 3 (13.0) | 20 (87.0) | |
| Moderna | 3 (42.9) | 4 (57.1) | |
| Sinopharm | 1 (25.0) | 3 (75.0) | |
| Knew a family member or friend who had been infected with SARS-CoV-2 * after receiving vaccination | 30 (13.4) | 194 (86.6) | 0.192 2 |
| Read precautions provided by the local authorities for COVID-19 ** vaccination | 14 (13.2) | 92 (86.8) | 0.631 |
| Searched for information related to COVID-19 ** vaccination online | 21 (12.2) | 151 (87.8) | 0.903 |
| Free COVID-19 ** vaccine as an influential factor in receiving it | 19 (11.3) | 149 (88.7) | 0.636 |
| Variable | Constraints | ||
|---|---|---|---|
| n (%) | p-Value | ||
| Yes | No | ||
| Sex | |||
| Female | 7 (5.8) | 113 (94.2) | 0.003 1,2 |
| Male | 0 (0) | 146 (100.0) | |
| Academic Year | |||
| 2nd year | 2 (2.4) | 80 (97.6) | 0.821 2 |
| 3rd year | 1 (3.0) | 32 (97.0) | |
| 4th year | 4 (4.2) | 91 (95.8) | |
| 5th year | 0 (0.0) | 27 (100.0) | |
| 6th year | 0 (0.0) | 29 (100.0) | |
| Chronic illness(es) | 1 (4.0) | 24 (96.0) | 0.503 2 |
| Annual receipt of influenza vaccine | 3 (3.1) | 94 (96.9) | 0.708 2 |
| Previous infection with SARS-CoV-2 * | 7 (7.9) | 82 (92.1) | 0.001 1,2 |
| Family member with previous SARS-CoV-2 * infection | 7 (3.5) | 193 (96.5) | 0.467 2 |
| Family member or friend passed away due to COVID-19 ** | 6 (7.9) | 70 (92.1) | 0.007 1,2 |
| Perceived Best COVID-19 Vaccine | |||
| Pfizer-BioNTech | 6 (2.6) | 226 (97.4) | 0.621 2 |
| Oxford-AstraZeneca | 1 (4.4) | 22 (95.6) | |
| Moderna | 0 (0.0) | 7 (100.0) | |
| Sinopharm | 0 (0.0) | 4 (100.0) | |
| Knew a family member or friend who had been infected with SARS-CoV-2 *after receiving vaccination | 7 (3.1) | 217 (96.9) | 0.601 2 |
| Read precautions provided by the local authorities for COVID-19 ** vaccination | 6 (5.7) | 100 (94.3) | 0.017 1,2 |
| Searched for information related to COVID-19 ** vaccination online | 7 (4.1) | 165 (95.9) | 0.053 2 |
| Free COVID-19 ** vaccine as an influential factor in receiving it | 5 (3.0) | 163 (97.0) | 1.00 2 |
| Variable | Calculation | ||
|---|---|---|---|
| n (%) | p-Value | ||
| Yes | No | ||
| Sex | |||
| Female | 43 (35.8) | 77 (64.2) | 0.515 |
| Male | 58 (39.7) | 88 (60.3) | |
| Academic Year | |||
| 2nd year | 29 (35.4) | 53 (64.6) | 0.280 |
| 3rd year | 8 (24.2) | 25 (75.8) | |
| 4th year | 43 (45.3) | 52 (54.7) | |
| 5th year | 10 (37.0) | 17 (63.0) | |
| 6th year | 11 (37.9) | 18 (62.1) | |
| Chronic illness(es) | 8 (32.0) | 17 (68.0) | 0.518 |
| Annual receipt of influenza vaccine | 35 (36.1) | 62 (63.9) | 0.631 |
| Previous infection with SARS-CoV-2 * | 25 (28.1) | 64 (71.9) | 0.022 1 |
| Family member with previous SARS-CoV-2 * infection | 67 (33.5) | 133 (66.5) | 0.024 1,2 |
| Family member or friend passed away due to COVID-19 ** | 34 (44.7) | 42 (55.3) | 0.294 2 |
| Perceived Best COVID-19 Vaccine | |||
| Pfizer-BioNTech | 82 (35.3) | 150 (64.7) | 0.003 1,2 |
| Oxford-AstraZeneca | 13 (56.5) | 10 (43.5) | |
| Moderna | 6 (85.7) | 1 (14.3) | |
| Sinopharm | 0 (0.0) | 4 (100.0) | |
| Knew a family member or friend who had been infected with SARS-CoV-2 *after receiving vaccination | 82 (36.6) | 142 (63.4) | 0.290 |
| Read precautions provided by the local authorities for COVID-19 ** vaccination | 54 (50.9) | 52 (49.1) | <0.001 1 |
| Searched for information related to COVID-19 ** vaccination online | 80 (46.5) | 92 (53.5) | <0.001 1 |
| Free COVID-19 ** vaccine as an influential factor in receiving it | 58 (34.5) | 110 (65.5) | 0.129 |
| Variable | Collective Responsibility | ||
|---|---|---|---|
| n (%) | p-Value | ||
| Yes | No | ||
| Sex | |||
| Female | 12 (10) | 108 (90) | 0.051 |
| Male | 27 (18.5) | 119 (81.5) | |
| Academic Year | |||
| 2nd year | 15 (18.3) | 67 (81.7) | 0.683 2 |
| 3rd year | 5 (15.2) | 28 (84.8) | |
| 4th year | 14 (14.7) | 81 (85.3) | |
| 5th year | 3 (11.1) | 24 (88.9) | |
| 6th year | 2 (6.9) | 27 (93.1) | |
| Chronic illness(es) | 3 (12.0) | 22 (88.0) | 0.693 |
| Annual receipt of influenza vaccine | 10 (10.3) | 87 (89.7) | 0.128 |
| Previous infection with SARS-CoV-2 * | 14 (15.7) | 75 (84.3) | 0.199 |
| Family member with previous SARS-CoV-2 infection | 30 (15.0) | 170 (85.0) | 0.480 |
| Family member or friend passed away due to COVID-19 ** | 16 (21.1) | 60 (78.9) | 0.108 |
| Perceived Best COVID-19 Vaccine | |||
| Pfizer-BioNTech | 34 (14.7) | 198 (85.3) | 0.601 2 |
| Oxford-AstraZeneca | 3 (13.0) | 20 (87.0) | |
| Moderna | 2 (28.6) | 5 (71.4) | |
| Sinopharm | 0 (0.0) | 4 (100.0) | |
| Knew a family member or friend who had been infected with SARS-CoV-2 after receiving vaccination | 32 (14.3) | 192 (85.7) | 0.689 |
| Read precautions provided by the local authorities for COVID-19 vaccination | 16 (15.1) | 90 (84.9) | 0.871 |
| Searched for information related to COVID-19 vaccination online | 25 (14.5) | 147 (85.5) | 0.937 |
| Free COVID-19 vaccine as an influential factor in receiving it | 31 (18.5) | 137 (81.5) | 0.022 1 |
| Independent Variable | Odds Ratio | p-Value | 95% CI for Odds Ratio | Goodness-of-Fit | |
|---|---|---|---|---|---|
| Confidence | R2 = 0.108 Entropy R2 = 0.108 Generalized R2 = 0.162 | ||||
| Academic year | 2nd year (a) | 7.042 | 0.012 1 | (1.548, 32.044) | |
| 3rd year (a) | 3.349 | 0.003 1 | (1.507, 7.445) | ||
| 4th year (a) | 1.803 | 0.295 | (0.598, 5.433) | ||
| 5th year (a) | 1.222 | 0.683 | (0.465, 3.201) | ||
| Previous infection with SARS-CoV-2 * | No (b) | 4.368 | 0.028 1 | (1.169, 16.314) | |
| Yes (b) | 2.487 | 0.180 | (0.655, 9.444) | ||
| Free COVID-19 ** vaccine as an influential factor in receiving it | Yes (c) | 2.002 | 0.038 1 | (1.038, 3.860) | |
| Complacency | |||||
| Age | 0.689 | 0.017 1 | (0.509, 0.934) | R2 = 0.108 Entropy R2 = 0.108 Generalized R2 = 0.147 | |
| Family member previously infected with SARS-CoV-2 | No (b) | 0.080 | 0.007 1 | (0.012, 0.496) | |
| Yes (b) | 0.066 | 0.002 1 | (0.012, 0.357) | ||
| Perceived best COVID-19 vaccine | Sinopharm (d) | 0.195 | 0.269 | (0.195, 42.853) | |
| Pfizer-BioNTech (d) | 0.057 | 0.002 1 | (0.009, 0.342) | ||
| Oxford-AstraZeneca (d) | 0.346 | 0.441 | (0.023, 5.134) | ||
| Calculation | R2 = 0.084 Entropy R2 = 0.084 Generalized R2 = 0.143 | ||||
| Previous infection with SARS-CoV-2 | No (b) | 0.486 | 0.245 | (0.144, 1.641) | |
| Yes (b) | 0.232 | 0.024 1 | (0.065, 0.826) | ||
| Read precautions provided by the local authorities for COVID-19 vaccination | Yes (c) | 1.798 | 0.039 1 | (1.028, 3.148) | |
| Searched for information related to COVID-19 vaccination online | Yes (c) | 2.651 | 0.002 1 | (1.418, 4.953) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omer, I.; Alhuzali, A.; Aletani, T.; Althagafi, Z.; Ghulam, E.; Awadh, A. Vaccine Hesitancy among Medical Students at a Tertiary Hospital—Affiliated Medical School. Healthcare 2023, 11, 461. https://doi.org/10.3390/healthcare11040461
Omer I, Alhuzali A, Aletani T, Althagafi Z, Ghulam E, Awadh A. Vaccine Hesitancy among Medical Students at a Tertiary Hospital—Affiliated Medical School. Healthcare. 2023; 11(4):461. https://doi.org/10.3390/healthcare11040461
Chicago/Turabian StyleOmer, Ibrahim, Abdullah Alhuzali, Tala Aletani, Zaher Althagafi, Enas Ghulam, and Abdullah Awadh. 2023. "Vaccine Hesitancy among Medical Students at a Tertiary Hospital—Affiliated Medical School" Healthcare 11, no. 4: 461. https://doi.org/10.3390/healthcare11040461