The main challenges can be grouped around the demand for NGS tests (which is influenced by the level at which NGS testing is organized, governance and strategy, awareness and education, etc.) and the supply of tests (influenced predominantly by the number of NGS tests conducted for research or diagnosis activities, reimbursement, infrastructure for conducting and validating tests, etc.). The surveys showed significant variability in the uptake of NGS technology in different global regions, but also some similarities.
4.1. Demand-Side Issues
4.1.1. Use of NGS in Routine Practise and Level of Organisation
According to data from three centres in Italy, NGS is used in routine practise for both clinical care and research. The same applies in France, Germany, Poland, China, India, Brazil, Colombia, Egypt, and the United States. In centres in Brunei and India, NGS is used only for clinical care, whereas in one centre from Belgium, it is used for public health research and guideline-making. Angola is in the process of implementing NGS/genomic medicine. At two centres in Italy, NGS testing is organized and operationalized at the regional level, whereas at the third institution, it is at department level. In France, this happens both at the hospital and departmental levels, and in Poland, China, Colombia, and Egypt, it happens at the hospital level. In India, it ranges from the department level to the national level or being outsourced to a national-level private lab. In one Brazilian and one United States centre, NGS testing is organized and operationalized at the national level. In the Middle East, the demand for NGS-based testing currently exceeds local capacity, and several countries rely on reference laboratories, mainly in Europe and the United States, to meet the demand. Only 16 laboratories in the Middle East are currently accredited by the College of American Pathologists to perform molecular genetic testing [
23].
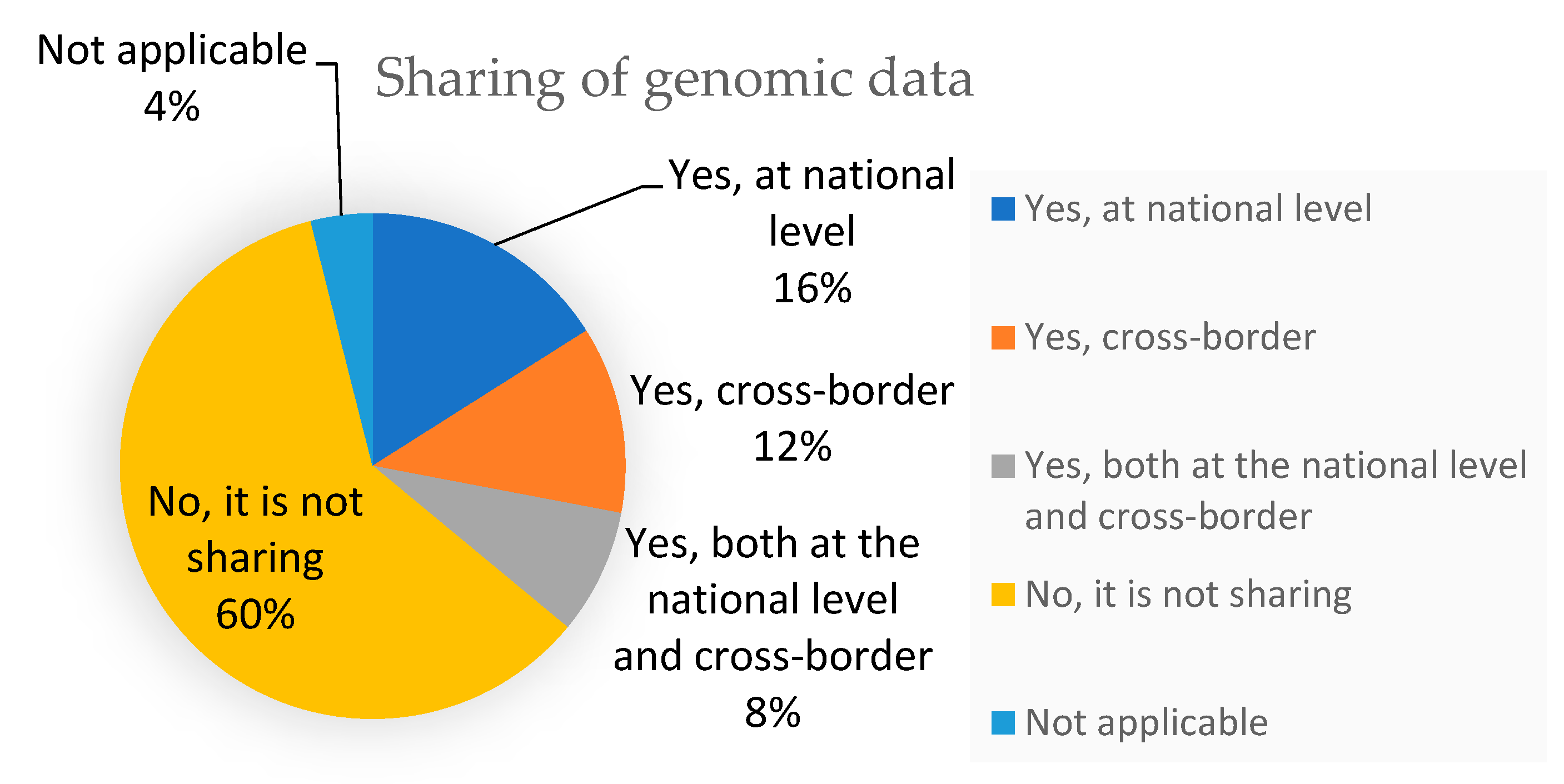
4.1.2. Sharing Genomic Data and Linking Data from Sequenced Genomes to Clinical Data
In Italy, two institutions do not share genomic data with other institutions. The third centre shares data cross-border. One of the centres in Germany shares genomic data with other institutions at national level, and another shares data both at the national level and cross-border. Centres in Poland, China, India, Brazil, Colombia, Brazil, and Egypt reported that they do not share genomic data with other institutions. The institution from the United States shares genomic data with other institutions at the national level. In Italy, two centres do not link data from sequenced genomes to clinical data such as Electronic Health Records (EHR). The third centre regularly links data from sequenced genomes to clinical data, and this linking regularly takes place with clinical data (EHR) or other types of data in Germany and China. Linking data to EHR or other types of data is done on request in Poland. One centre in India routinely links data from sequenced genomes to clinical or other types of data, but another does so only on request, and in the third, data is not linked. A centre from Brazil reported that they link data from sequenced genomes to clinical data on a regular basis, whereas in one Colombian centre, they do so on request. In one centre from Egypt, as well as one from the United States, data is not linked from sequenced genomes to clinical data.
4.1.3. Turnaround Times for NGS Tests That Are Used for Patient Care
The turnaround times for NGS tests that are used for patient care differs: at one centre in France, the average turnaround time is ≥21 days, whereas in Germany, the average is <21 days; in a Polish centre, it is ≥21 days, whereas it is just <14 days in China and Egypt, and it is less than 21 days in India and Brazil.
4.1.4. Governance and Strategy
In Italy, local-level NGS sequence generation for clinical use is aligned with ISO lab accreditation/protocols. Guidelines for NGS data analysis are available at the local/organizational level, and guidelines for clinical interpretation of NGS results are defined locally. Guidelines to protect and ensure the lawful, fair, and transparent processing of personal data are implemented and consistently enforced. There is no guideline to ensure that appropriate consent is obtained or that counselling is provided in relation to NGS testing. In France, the governance body for bringing NGS into healthcare is institutionalised, recognised as the lead for genomics in healthcare, and is open to novel developments and supportive of international cooperation. NGS is implemented in health and other relevant plans, and it is periodically evaluated for optimization. There is a national and/or regional investment plan for NGS in healthcare that incorporates innovation according to opportunities and international developments. In Germany, Poland, Canada, and Angola the scope of governance for NGS is defined, but elements are still under development. In the Republic of Korea, a governance body for bringing NGS into healthcare is fully operational and led centrally, and activities are monitored based on a work plan. In China, elements of governance for bringing NGS into healthcare exist but are not fully functional, whereas the inclusion of NGS in healthcare in relevant national/regional health plans is under discussion. In Japan, the governance body for bringing NGS into healthcare is institutionalised, recognised as the lead for genomics in healthcare, and is open to novel developments and supportive of international cooperation. NGS is implemented in health and other relevant plans, and it is periodically evaluated for optimization. On the other hand, in India, there is no dedicated governance for bringing NGS into healthcare, and the uptake of NGS in healthcare is not included in national/regional health plans. There is no dedicated governance for bringing NGS into healthcare in Philippines, Venezuela, Brazil, Lebanon, South Africa, or Mexico. In Qatar, the governance body for bringing NGS into healthcare is institutionalised, recognised as the lead for genomics in healthcare, and is open to novel developments and supportive of international cooperation. In Israel, there is a governance body that is fully operational and led centrally, and activities are monitored based on a work plan, whereas in the United States, elements of governance for bringing NGS into healthcare exist, but they are not fully functional. In Kenya and Tunisia, elements of governance for bringing NGS into healthcare exist, but they are not fully functional. The genomics services in the Middle East are fragmented and often generated by individual interests with a lack of a centralized or population-based national strategy.
4.1.5. Clinical Standardization
Laboratories in Italy face challenges in adapting to constantly evolving technologies. In Italy, Mexico, and the Philippines, teams for NGS/genomic medicine are assembled in some hospitals as a bottom-up initiative, but not all areas are covered, nor are all necessary tools available. Novel technologies and tools are selected and implemented locally (e.g., in the hospital or lab), and processes for integrating clinics with research outcomes are implemented at the local level. In France, multidisciplinary teams are the norm for the implementation of national genomics in medicine strategy. There is clinical and economic evidence for NGS in lung cancer, and there is limited evidence for NGS in melanoma in France. According to literature data, more than 60,000 cancer patients have taken molecular predictive tests. Moreover, since 2013, the French National Cancer Institute (INCa) supported the implementation of targeted NGS as part of routine clinical practise [
24]. Genomic centres for the uptake of NGS are implemented and operate under common guidelines and policies. Guidelines for clinical interpretation of NGS results from internationally recognised bodies are implemented nationally, and there are interactions with these international bodies for guideline definitions for specific diseases. In Germany, guidelines for assembling multidisciplinary teams and referral networks are implemented at the regional/national level, aligned with a strategy for genomics in healthcare and with dedicated funding. Guidelines for clinical interpretations of NGS results are defined regionally/nationally. Processes for the integration of clinics with research outcomes are implemented at local and regional levels according to a local strategy.
Among Asian countries, the adoption and implementation of genomic medicine and NGS is growing, but it is still heterogenous. In four southeast Asian countries (Indonesia, Malaysia, Singapore, and Thailand), progress in this area still leaves significant variability in clinical implementations [
25]. China has plans to adopt novel technologies and tools to support clinical decision making. These plans are centralised at the regional/national levels and aligned with a national strategy for NGS in healthcare. Novel technologies and software tools to support clinical decisions have not been adopted in the Philippines. In Egypt, Qatar, the Kingdom of Saudi Arabia, and the United Arab Emirates, some well-organised initiatives have emerged, aiming to enhance the integration of genomics into healthcare [
26]. In Qatar, ICT tools supporting clinical interpretations of NGS results, clinical decision-making, and communication with the patients are under wider implementation in healthcare systems following a strategy for genomic medicine. In Israel, pathology laboratories that have received approval from the Ministry of Health Laboratories Division are able to perform molecular profiling for all patients with non-small cell lung cancer (NSCLC) in medical centres throughout the country, and it is completely covered by insurance. Six laboratories are already approved to perform broad molecular profiling using the Oncomine Dx Target Test, an NGS-based test that evaluates patient tumour samples for up to 23 biomarkers associated with NSCLC [
27]. ICT tools supporting clinical interpretations of NGS results are under wider implementation in healthcare systems following a strategy for genomic medicine. In Lebanon, with the introduction of NGS technologies, clinical diagnoses were significantly improved, and the identification of the origin of various disorders was accelerated. There is a lack of expertise, and the cost of genetic tests are associated with this. There is a lack of clinical geneticists and genetic counselling services in Lebanon, which is an issue in view of the high number of genetic disorders in their population [
28,
29,
30]. ICT tools are available in selected hospitals in Lebanon, and teams for NGS are assembled in some hospitals as a bottom-up initiative, but not all areas are covered, nor are the necessary tools available. African countries are facing numerous challenges in increasing and adopting their NGS capabilities [
31]. In South Africa, there is a huge difference between public and private sectors regarding the availability of novel technologies and software tools to support clinical decisions. In Angola, there are plans and processes for adoption of novel technologies and tools to support clinical decision making, but they are not widely implemented at the regional/national levels.
4.1.6. Awareness and Education
Literacy programmes or campaigns are available locally, as a bottom-up initiative, on particular topics in Italy, France, Poland, the Republic of Korea, Mexico, Venezuela, Israel, Lebanon, and the United States. In Italy, the integration of NGS into general university curricula for medical doctors must be assessed as gaps are identified and training options are under development. Bioinformatics expertise for data analysis, as well as specific predictive biomarkers required to identify patients most likely to respond to treatment, are under development [
4,
5]. In France, guidelines to protect and ensure the lawful, fair, and transparent processing of personal data are implemented, enforced, and fit-for-purpose. In Germany, gaps were identified with, and training options are under development regarding, the integration of NGS into general university curricula for medical doctors. In Poland, there is a National Cancer Strategy wherein the promotion of health research and innovation is addressed. The processing of health and genetic data for research has not yet been implemented. In Republic of Korea, training for NGS is available but under implementation. In China, a strategy for literacy programmes or campaigns targeting specific audiences is defined and widely implemented with dedicated funds. There are no systematic courses about NGS integrated into general university curricula for medical doctors. They are only mentioned in a few textbooks for undergraduates, but some colleges and universities have established optional courses for graduate students. In Japan, the integration of NGS into general university curricula must be assessed as gaps are identified and training options are under development. The Japan Agency for Medical Research and Development supports some research programs to promote the education of medical professionals regarding clinical cancer sequencing. These programs consist of lectures, tutorial sessions, and e-learning. Literacy programmes or campaigns on NGS do not exist in India, and there is no communication strategy for NGS. In the Philippines, Colombia, South Africa, and Angola there are no literacy programmes or campaigns on NGS, and synergies with patient associations are not well established. NGS is not integrated into their general university curricula for medical doctors. In Colombia, NGS is not integrated into general university curricula for medical doctors, and there are no programmes for policy makers and healthcare managers to use to raise awareness on NGS. What is crucially needed is to create national genetic data registries, which would establish the true significance of country-specific cancer-related variants, and a collaborative environment that promotes NGS research on outcomes, impacts, and cost-effectiveness in Colombia [
20].
In terms of education and awareness, medical associations and patient organisations should develop activities to better inform patients and healthcare professionals about the uses, applications, and limitations of NGS. Collaboration is needed between academic institutions and medical associations to develop continuing medical education for oncology-related health-care professionals on the use of NGS. In Mexico, synergies with patient associations are not well established. The integration of NGS into general university curricula for medical doctors must be assessed as gaps are identified and training options are under development. In Venezuela, synergies with patient associations are available locally as bottom-up initiatives with specific associations. NGS is not integrated into their general university curricula for medical doctors. In Qatar, literacy programmes or campaigns on NGS are minimal through the Qatar Genome Project and Qatar BioBank so far. In Lebanon, there is no communication strategy for NGS. In the United States, literacy programmes or campaigns on NGS are available locally as bottom-up initiatives on particular topics. In the United States, the communication strategy for NGS is available locally for bottom-up initiatives with specific target audiences. In South Africa and in Angola, synergies with patient associations are not well-established, and programmes for policy makers and healthcare managers to raise awareness of NGS have gaps. In Angola, there are no programmes for policy makers and healthcare managers to raise awareness of NGS and its implications for healthcare. In Tunisia, a strategy for literacy programmes or campaigns targeting specific audiences was defined based on genomic literacy surveys, and it is under implementation (see
Appendix A,
Table A4,
Table A5,
Table A6 and
Table A7).
4.2. Supply-Side Issues
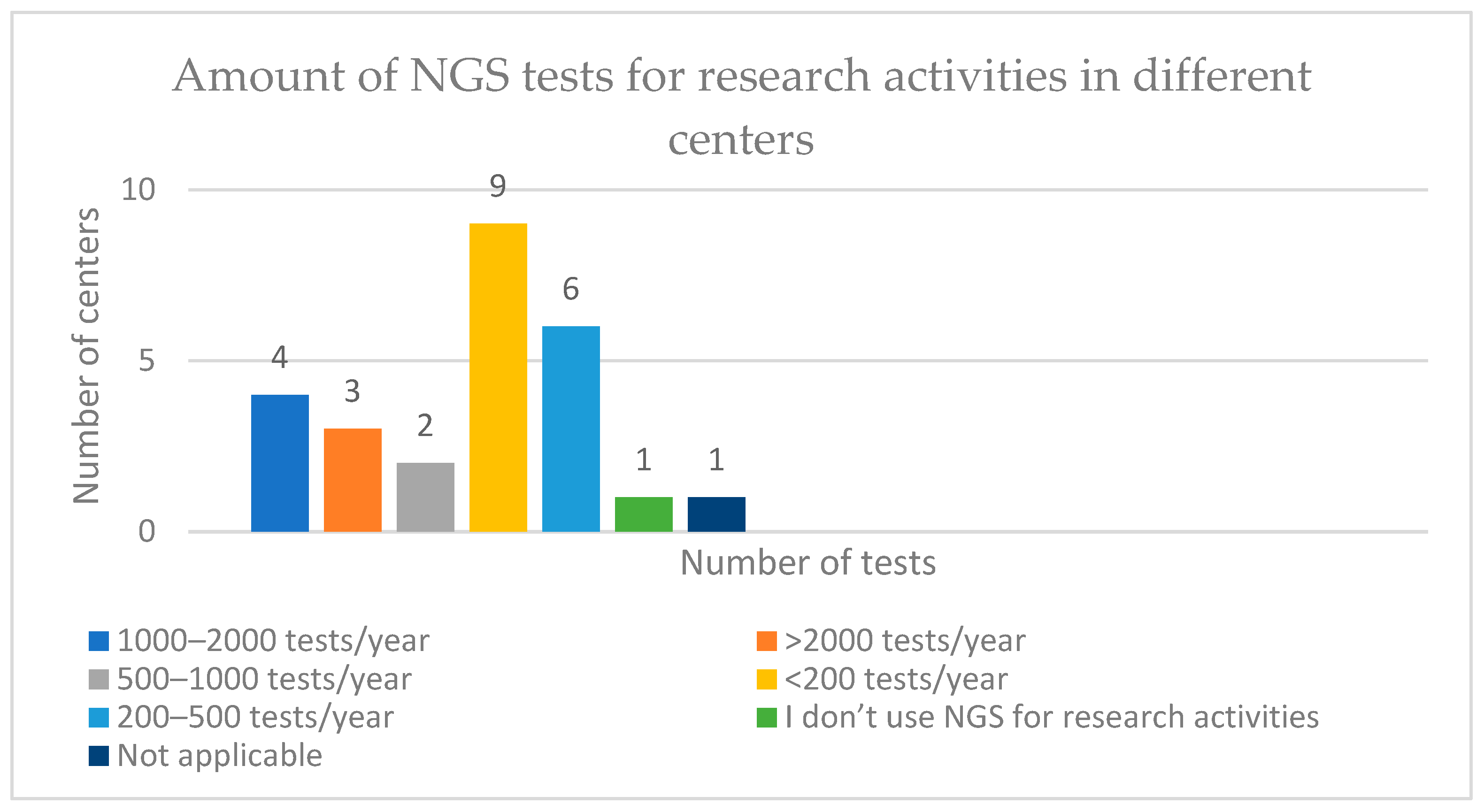
4.2.1. Numbers of NGS Tests Conducted or Ordered for Research or Diagnostic Activities
In Italy, 1000–2000 NGS tests are conducted or ordered from an external lab for research activities in a year at one of their centres, whereas for diagnostic activities, the number is 500–1000 tests/year. At a second centre, >2000 tests/year are conducted or ordered for research activities, whereas for diagnostic activities, there are <200 tests/year. At their third institution, the number of tests conducted or ordered for research activities is 200–500 tests/year, whereas for diagnostic activities, it is <200 tests/year. In France, in one of their centres, <200 tests/year are conducted or ordered from an external lab for research activities in a year, and 500–1000 tests/year are conducted for diagnostic activities. In their second centre, these numbers are 1000–2000 tests/year for research activities and 200–500 tests/year for diagnostic activities. More than 2000 NGS tests are conducted or ordered from an external lab for diagnostic activities in a year, according to data from two centres in Germany. In Poland, the number of tests conducted or ordered from an external lab for research activities in a year is 500–1000 tests/year, and for diagnostic activities, it is 200–500 tests/year. One Chinese centre reported that >2000 tests are conducted or ordered from an external lab for both research and diagnostic activities in a year. In two centres from India, 200–500 tests/year are conducted or ordered for research activities, whereas in their third, less than 200 tests are conducted in a year. For diagnostic activities, two centres reported conducting 500–1000 tests per year, but a third centre only conducts <200 tests per year. In one centre from Brazil, less than 200 tests are ordered or conducted from an external lab for research activities in a year, whereas for diagnostic activities, there are 1000–2000 tests/year. One Colombian centre reported <200 tests/year for both research and diagnostic activities. For research activities, one centre from Egypt conducts <200 tests/year, whereas for diagnostic activities, the figure is 200–500 tests/year. In one centre from the United States, 200–500 tests/year are conducted for research activities, whereas for diagnostic activities, there are 500–1000 tests/year.
4.2.2. Professionals Involved in Molecular Tumour Boards (MTBs)
In Italy, a molecular tumour board (MTB) is present at all three institutions, involving oncologists (medical, surgical, or radiation), pathologists, molecular biologists, geneticists, and bioinformaticians. In France, oncologists (medical, surgical, or radiation) and molecular biologists are routinely involved in the MTB. Oncologists (medical, surgical, or radiation), pathologists, molecular biologists, and geneticists are part of the MTB in Germany, whereas in Poland, oncologists (medical, surgical, or radiation) and molecular biologists are involved. An MTB in China routinely involves oncologists (medical, surgical, or radiation), pathologists, geneticists, and bioinformaticians, and in Brazil, oncologists (medical, surgical, or radiation), pathologists, and geneticists are involved. One centre from Colombia reported that oncologists (medical, surgical, or radiation), pathologists, and nurses are involved, whereas in one centre from Egypt, oncologists (medical, surgical, or radiation), pathologists, molecular biologists, geneticists, and pharmacologists are involved. In Japan, multidisciplinary teams are the norm for implementations of national genomics in medicine strategy. Since 2013, several institutions, including the National Cancer Center (NCC) and university hospitals, have initiated research-based NGS clinical sequencing to guide patients to relevant clinical trials [
32]. In Venezuela, teams for NGS are assembled in some hospitals as a bottom-up initiative, but not all areas are covered, and not all of the necessary tools are available. Teams for NGS, in Qatar, are assembled in some hospitals as bottom-up initiatives, but without all areas or necessary tools covered. In South Africa, teams for NGS are assembled in some hospitals as bottom-up initiatives, but not all areas are covered, nor are all of the necessary tools available. In Kenya, teams for NGS are assembled in some hospitals as bottom-up initiatives but with the same deficiencies as in South Africa. In Tunisia, multidisciplinary teams are the norm for the implementation of national genomics in medicine strategy.
4.2.3. Types of Diagnoses for Which NGS Tests Were Ordered >5× in the Last Year
At centres in Italy, the most common diagnosis types for which NGS tests were ordered >5× in the last year are breast cancer, lung cancer, and colon cancer. In France, breast cancer, colon cancer, and lung cancer were the most common, whereas breast cancer, colon cancer, and pancreatic cancer top the list in Germany. One centre from Poland lists breast cancer, colon cancer, lung cancer, pancreatic cancer, prostate cancer, and rare cancers. In China, at one centre, an NGS test for <50 genes was ordered >5× in the last year for breast and colon cancer, and tests were ordered >5× for >50 genes for leukaemia, lung cancer, pancreatic cancer, prostate cancer, and rare cancers. The picture varies across India, with one centre ordering tests frequently for breast cancer, colon cancer, leukaemia, lung cancer, and pancreatic cancer, whereas in another only, breast cancer and colon cancer featured on their list of >5×. In one centre from Brazil, breast cancer, colon cancer, leukaemia, lung cancer, prostate cancer, and rare cancers featured on the list, and in one United States centre, breast cancer, colon cancer, lung cancer, and pancreatic cancer dominated. In Colombia, lung cancer, breast cancer, and cancers of unknown primary sites were the most common categories [
33,
34].
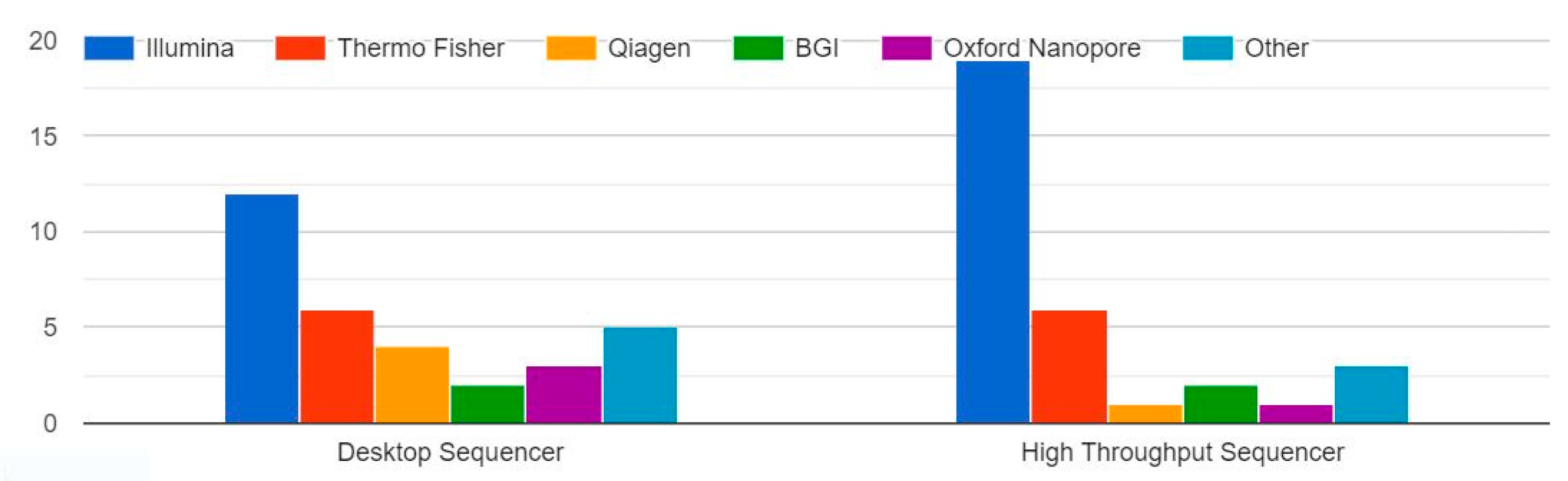
4.2.4. Types of Sequencers Used for the Greatest Number of Tests in Workplace
In Italy, the sequencers used for the greatest number of NGS tests are Thermo Fisher and Illumina, whereas Illumina is the most used at one institution in France. In Germany, Oxford Nanopore, Oxford, UK and Illumina dominate, and in Poland, Illumina and Thermo Fisher are the most frequently used. In China, BGI, Beijing, China is mostly used, and each centre in India favours one of Oxford Nanopore, Thermo Fisher, or Illumina. In Brazil and Colombia, Illumina is the most frequently used, and a centre in Egypt uses Illumina, Thermo Fisher, Qiagen, Hilden, Germany, and BGI. Qiagen is the sequencer used for the greatest number of NGS tests in one centre in the United States.
4.2.5. Equitable Reimbursement, Investment Plans, and Funding
In Italy, the inclusion of NGS in healthcare in relevant national/regional health plans is under discussion, and there is no framework to bring NGS into the healthcare strategy with a costed implementation plan. An investment plan for bringing NGS into healthcare at the national and/or regional levels is under development. A health technology assessment (HTA)-based approach for NGS is needed in Italy to show the medical and cost effectiveness of NGS, and this is still under development. In France, a reimbursement framework or no-cost access plan for specific NGS tests is fully implemented, periodically evaluated, and optimised, with a plan for adoption of novel tools and technologies. In Germany, integration of NGS into healthcare is dictated by law, and there is no HTA framework for NGS. In Poland, an investment plan for bringing NGS into healthcare at the national and/or regional levels is under development, and an HTA framework to assess genomic tests is urgently needed. In Republic of Korea, a national and/or regional investment plan for NGS in healthcare is mostly dedicated to setting up infrastructure. A framework for cost-effectiveness assessment of NGS tests is under development. In China, there is no established investment plan at the national or regional level for bringing NGS into healthcare systems. One of the major challenges is still the cost of NGS tests, and most genetic tests are not covered by governmental health insurance; thus, most patients end up paying out-of-pocket [
35,
36,
37,
38,
39,
40]. Reimbursement frameworks or no-cost access plans for specific NGS tests are developed, approved, and operationalised with disease- or patient-specific models. There is no HTA framework for NGS. Regarding investment, Japan’s national and/or regional investment plans for NGS in healthcare incorporate innovation according to opportunities and international developments, but there is no framework for cost-effectiveness assessment of NGS tests. In India, investment plans at the national or regional level are not in place, and there is no framework for reimbursement or no-cost access plans for NGS tests. Philippines has no established investment plan, and there is no HTA framework for NGS. NGS-based oncology panels are not seen as cost-effective solutions for many governments in Latin America countries, and they are not being implemented in health and insurance systems despite local sequencing capabilities [
41]. In Colombia, there are substantial inequities in available therapies between the public and private healthcare systems. There is no established investment plan at the national or regional level for bringing NGS into healthcare systems, and there is no HTA framework for NGS. Although the price of NGS has decreased in Colombia, the cost remains four to five times higher than in other countries because of taxes, analysis costs, shipping costs, and required infrastructure. In Brazil, the cost of sequencing tests can still be four to five times higher than in high-income countries because of taxes and the high cost of analysis, shipment, and infrastructure [
42]. The uptake of NGS in healthcare is not included in national/regional health plans, and no investment plan at the national or regional level for bringing NGS into healthcare systems is established. There is no HTA framework and no framework for the cost-effectiveness assessment of NGS tests.
There is no established investment plan in Mexico, and there is no HTA framework for NGS. In Venezuela, there is no established plan, and societal benefits are not considered in economic modelling for NGS. In Lebanon, NGS tests are not covered by insurance; thus, patients often withdraw from recommended genetic testing [
28,
29]. The costs of establishing and running sequencing facilities obstruct the implementation and wide adoption of NGS. The uptake of NGS in healthcare is not included in national/regional health plans, and there is no framework to bring NGS into the healthcare strategy with a costed implementation plan. In the United States, there is no established investment plan for bringing NGS into healthcare system, but an HTA framework for NGS was developed and approved. In Canada, patients in some cases are offered testing via private insurance or self-pay, but this approach may bring inequity [
25]. There is no established investment plan at the national or regional level for bringing NGS into healthcare systems, and an HTA framework for NGS is still under development. In South Africa, the uptake of NGS in healthcare is not included in national/regional health plans, and no investment plan at the national or regional level for bringing NGS into healthcare systems is established. Angola has no established investment plan for bringing NGS into healthcare systems and no HTA framework for NGS, and societal benefits are not considered in economic models for NGS. In Angola, there is no established investment plan at the national or regional level for bringing NGS into healthcare systems. In Tunisia, NGS is included in relevant national/regional health plans, and a strategy for integrating NGS in healthcare with a costed implementation plan is under discussion. An investment plan for bringing NGS into healthcare at the national and/or regional levels is under development as well as an HTA framework for NGS. In Italian centres and in Germany and Egypt, most NGS tests for clinical care are funded through national or regional healthcare systems, whereas in Poland, Brazil, and the United States, most tests are industry-funded.
4.2.6. Infrastructure for Conducting and Validating Tests
In Italy and Poland, ICT tools supporting clinical interpretation of NGS results, clinical decision-making, and communication with patients are implemented in select hospitals, whereas in France, they are fully implemented and periodically evaluated. In Germany, on the other hand, they are under wider implementation. Genomic centre infrastructure networks are implemented at the regional/national levels. Data sharing policies and data flows are not established, whereas computational and data infrastructures for medical reuse and secondary data analysis are available to support local analyses of data. Processes for the integration of clinics with research outcomes are implemented at the national and international level with well-established partnerships. In Germany, genomic centre infrastructure networks for the uptake of NGS are under development, and guidelines for NGS data generation are available locally (e.g., in the hospital, laboratory, or project). Security policies and the infrastructure within NGS are established under national regulations and fully enforced. Computational and data infrastructures for medical reuse and secondary data analysis are available to support local analyses of data. In Poland, novel technologies and software tools to support clinical decisions are not adopted. The security policies and the infrastructure within NGS are defined at the organisation level. Data access granting is fully manual and computational, and data infrastructure for medical reuse and secondary data analysis is available to support local analyses of data.
In the Republic of Korea, novel technologies and software tools are centralised at the regional/national levels and aligned with a national strategy for NGS in healthcare and with international standards. Genomic centres for the uptake of NGS are implemented at the regional/national levels. Guidelines for NGS data analysis are available at the regional/national levels. Security policies and infrastructure within NGS are nationally defined but not sufficiently enforced, whereas electronic systems to support data sharing policies are implemented and adopted nationally. In China, security policies and infrastructure within NGS are established under national regulation and fully enforced. Computational and data infrastructure for medical reuse and secondary data analysis is available to support local analysis of data. In Japan, genomic centres for the uptake of NGS are implemented, and they operate under common guidelines and policies. Guidelines for NGS data analysis are available at the regional/national level, whereas guidelines for the clinical interpretation of NGS results are defined regionally/nationally. The security policies within NGS follow international best practises for data security and are regularly reviewed based on changes in technological, regulatory, and ethical considerations. Electronic systems are implemented to support data sharing policies and are adopted nationally.
Indian research based on NGS has brought significant progress both in benign and malignant haematology [
43]. NGS facilities are available in 24 states and 3 union territories with 63 operational sites that mostly use sequencers from Oxford Nanopore, Thermo Fisher, and Illumina—which is in line with literature data that show Illumina, Ion Torrent, and Oxford Nanopore are the most used NGS platforms [
44,
45]. Novel technologies and software tools to support clinical decisions are not adopted. Genomic centres for the uptake of NGS are not established, and guidelines for NGS are not defined. Security policies and infrastructure within NGS are defined at the organisational level, whereas computational and data infrastructures for medical reuse and secondary data analysis are not available.
In Philippines, genomic centres for the uptake of NGS are not established, and the guidelines for NGS are not defined, nor are guidelines for genomic data analysis, the clinical interpretation of NGS results, structuring of metadata for datasets, or for data sharing policies and data flows. In Colombia, only a few public or private laboratories offer standardized NGS in-house tests, partly because of the complex technology involved (i.e., technical expertise, bioinformatics and computing infrastructure, and data interpretation). Most institutions in Colombia do not have the robust infrastructure of human, technological, financial, and bioinformatic resources that NGS requires. In Brazil, inequalities in NGS access result from challenges such as limited laboratory infrastructure, refunding and logistics issues, limited medical and patient education and empowerment, and lack of availability [
46,
47,
48,
49]. Novel technologies and tools are selected and implemented locally (e.g., in the hospital or lab). Infrastructure and policies for data security within NGS are not established. In Mexico, novel technologies and tools are selected and implemented locally (e.g., in the hospital or lab). Genomic centres for the uptake of NGS are local (e.g., in the hospital or laboratory) as well as in Venezuela, Lebanon, and Angola, whereas guidelines for NGS are not defined in Mexico. The security policies and infrastructure within NGS are defined at the organisational level. Data sharing policies and data flows are not established, and computational and data infrastructures for medical reuse and secondary data analysis are not available. In Venezuela, effective partnerships with stakeholders from the industry sector are implemented at the local level.
Population genetic screening, in the form of limited or expanded gene panels, is still lacking in the Middle East. There is a shortage of well-trained personnel, such as clinical molecular geneticists, bioinformaticians, genomic analysts, etc. due to the regional brain drain of talent. Certain countries such as the United Arab Emirates, Qatar, the Kingdom of Saudi Arabia (KSA), and Lebanon have taken substantial steps towards establishing clinical genomic sequencing facilities and local expertise [
26,
50,
51,
52,
53]. In Qatar, genomic centres for the uptake of NGS are implemented and operate under common guidelines and policies. Computational and data infrastructures for medical reuse and secondary data analysis are in place to support national analyses of data. In Israel, genomic centres for the uptake of NGS are implemented and operate under common guidelines and policies. In Lebanon, novel technologies and tools are selected and implemented locally (e.g., in the hospital or lab). In the United States, novel technologies and tools are selected and implemented locally (e.g., in the hospital or lab). Genomic centres for the uptake of NGS are implemented and operate under common guidelines and policies. In Canada, one of the key obstacles with expanding the use of whole-exome sequencing/whole-genome sequencing (WES/WGS) further is the lack of infrastructure to deliver clinical exomes on time; thus, most WES testing is sent out of the country. Extensive paperwork is also required to request testing. In South Africa, genomic centres for the uptake of NGS are not established, and guidelines for NGS and for genomic data analysis are not defined. The security policies and infrastructure within NGS are defined at the organisational level. In Angola, there are plans and processes for the adoption of novel technologies and tools to support clinical decision making, but they are not widely implemented. In Tunisia, genomic centres for the uptake of NGS are implemented.
4.2.7. Testing Access Driven by Evidence Generation
In Europe, access to molecular diagnostics varies among countries. The United Kingdom, Denmark, Sweden, and Germany show the highest uptakes of NGS according to literature data, which is possibly linked to more centralised systems with substantial infrastructure investment. A shortage of pathologists in eastern and central Europe results partly from the brain drain to western countries [
7,
54]. In Italy, effective partnerships with stakeholders from the industry sector are implemented at the local level. In Poland, guidelines for the clinical reporting of genomic results are developed at the organisational level. In Republic of Korea, guidelines to protect and ensure the lawful, fair, and transparent processing of personal data are implemented, enforced, and fit-for-purpose, as are guidelines to ensure appropriate consent is obtained and counselling is provided in relation to NGS testing. In China, guidelines to protect and ensure the lawful, fair, and transparent processing of personal data are implemented and consistently enforced, but guidelines to ensure appropriate consent is obtained are implemented but insufficient in scope. In Japan, effective partnerships with stakeholders from the industry sector are implemented at the national level with well-established partnerships. In the Philippines, guidelines protecting the confidentiality of patient genetic/genomic test results are implemented only in a few hospitals, whereas guidelines that limit genetic/genomic testing to legitimate purposes and prevent misuse do not exist. In Mexico, guidelines to protect and ensure the lawful, fair, and transparent processing of personal data do not exist, whereas guidelines protecting the confidentiality of patient genetic/genomic test results are implemented but insufficient in scope. Guidelines to ensure appropriate consent is obtained and counselling is provided in relation to NGS testing are implemented but insufficient in scope. In Venezuela, guidelines for the transparent processing of personal data are implemented but insufficient in scope. Guidelines protecting the confidentiality of patient genetic/genomic test results do not exist, whereas guidelines to ensure appropriate consent is obtained and counselling is provided in relation to NGS testing are implemented but insufficient in scope. In the United States, guidelines to protect and ensure the lawful, fair, and transparent processing of personal data are implemented but not yet consistently enforced. In Tunisia, many guidelines, such as those protecting the confidentiality of patient genetic/genomic test results, are implemented and consistently enforced (see
Appendix A,
Table A4,
Table A5,
Table A6 and
Table A7).
4.3. Summary
- A.
Using the Delphi method, study objectives were almost completely accomplished.
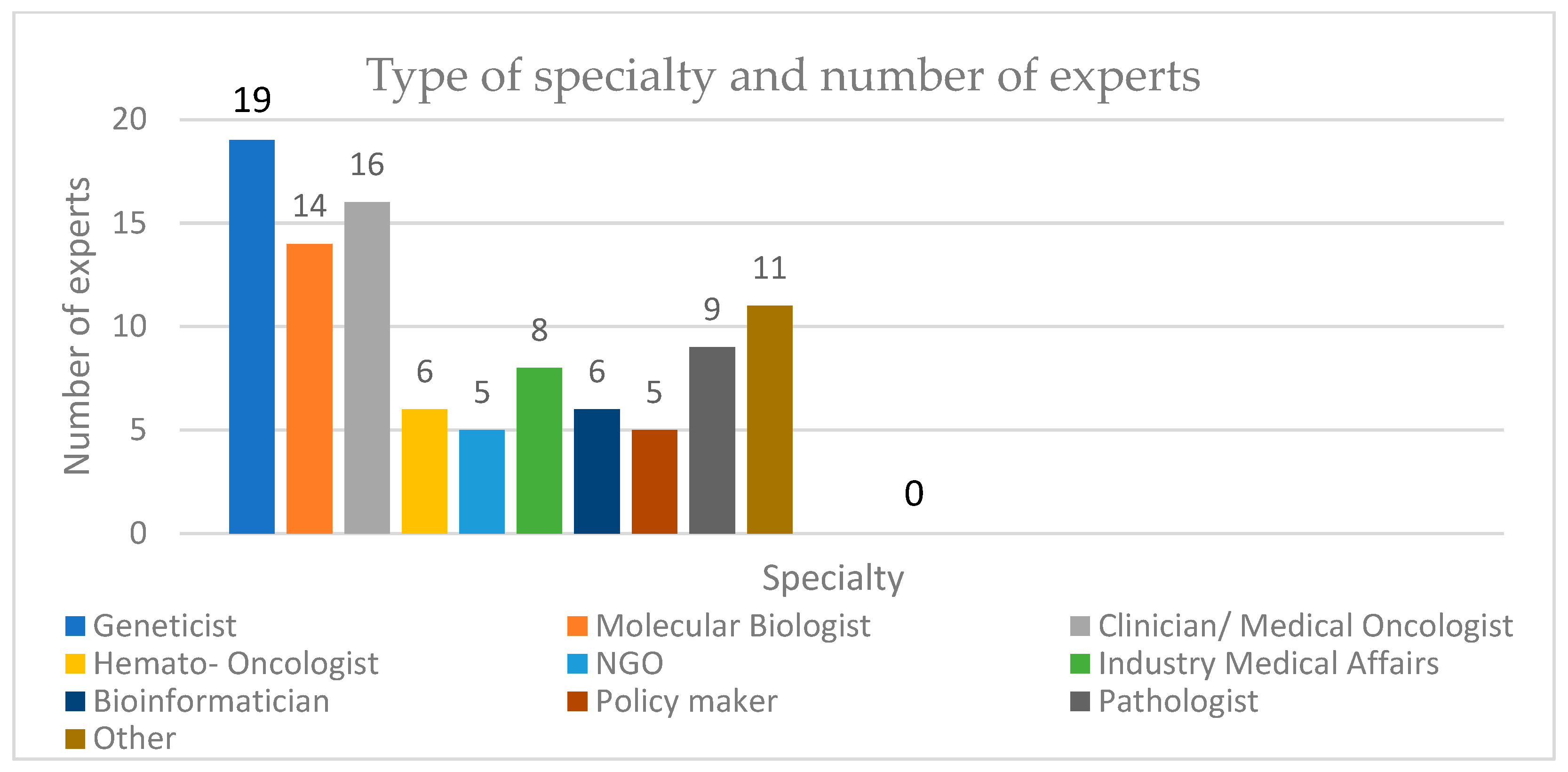
A two-round Delphi [
55] was used because there was a clear literature base from which to establish the survey instrument. The aim was to reach a group consensus; thus, a high representative agreement rate was particularly important [
56]. The first round of expert panels yielded agreement on a cut-off rate for criterion validation of 85%, whereas for the second round, it was around 90%, which was the threshold. Sixty-two experts participated on the first round table, whereas for the second round table, there were 64 participants. Panels between 10 and 50 participants are recommended according to the literature [
57]; thus, the quantitative figure of professionals involved was addressed. The ratio of each group of professionals was intended to be as equal as possible, which was achieved for the first round but not the second.
- B.
Main and novel findings for the demand side and key recommendations
Demand-side issues can be grouped around the use of NGS in routine practise and levels of organisation, sharing genomic data and linking data from sequenced genomes to clinical data, turnaround time for NGS tests that are used for patient care, governance and strategy, clinical standardization, and awareness and education. NGS is used in routine practise for both clinical care and research in most of the centres globally, according to the survey. Centres in Poland, China, India, Brazil, Colombia, and Egypt reported that they are not sharing genomic data, whereas the situation in other centres in Europe, Latin America, Asia, and Africa varies. The turnaround time for NGS tests that are used for patient care also varies from >21 days to <21 and even <14 days. There is no dedicated governance for bringing NGS into healthcare in the Philippines, Venezuela, Brazil, Lebanon, South Africa, or Mexico. In Israel, there is a governance body that is fully operational, whereas in Kenya and Tunisia, elements of governance for bringing NGS into healthcare exist, but they are not fully functional. In Italy, local-level NGS sequence generation for clinical use is aligned with ISO lab accreditation/protocols, whereas in France, the governance body for bringing NGS into healthcare is institutionalised, recognised as the lead for genomics in healthcare, and is open to novel developments and supportive of international cooperation. In Italy, Mexico, and the Philippines, teams for NGS/genomic medicine are assembled in some hospitals as a bottom-up initiative, but not all areas are covered, nor are all of the necessary tools available. Among Asian countries, the adoption and implementation of genomic medicine and NGS is growing, but it is still quite heterogenous. In Egypt, Qatar, the Kingdom of Saudi Arabia, and the United Arab Emirates, some well-organised initiatives have emerged, aiming to enhance the integration of genomics into healthcare. Literacy programmes or campaigns are available locally as bottom-up initiatives on specific topics in Italy, France, Poland, the Republic of Korea, Mexico, Venezuela, Israel, Lebanon, and the United States. In terms of education and awareness, medical associations and patient organisations should develop activities to better inform patients and health care professionals about the uses, applications, and limitations of NGS.
- C.
Main and novel findings for the supply side and key recommendations
Supply-side issues can be grouped around the number of NGS tests conducted or ordered for research or diagnostic activities, professionals involved in MTBs, types of diagnosis for which NGS tests were ordered >5× in the last year, types of sequencers most used, equitable reimbursement, investment plans and funding, infrastructure for conducting and validating tests, and testing access driven by evidence generation. In centres in Italy and France, 1000–2000 NGS tests are conducted or ordered from an external lab for research activities in a year. Centres from Colombia, Egypt, and Brazil reported that they conduct <200 tests/year for research activities. Performances of 200–500 tests/year for diagnostic activities were reported in centres from Egypt, the United States, and France. In most of the centres, MTBs are present and most often consist of oncologists (medical, surgical, or radiation). In many centres, multidisciplinary teams are the norm for the implementation of national genomics in medicine strategy. The most common diagnosis types for which NGS tests were ordered >5× in the last year are breast cancer, colon cancer, and lung cancer. Different sequencers are used, ranging from Thermo Fisher and Illumina as the most frequent to Oxford Nanopore, BGI, and Qiagen. HTA-based approaches for NGS are needed to show the medical efficacy and cost effectiveness of NGS, and these are still under development in Italy. In France, a reimbursement framework or no-cost access plans for specific NGS tests are fully implemented. In Republic of Korea, a national and/or regional investment plan for NGS in healthcare is put in place, which is mostly dedicated to setting up infrastructure, whereas in China, there is no established investment plan at the national or regional level for bringing NGS into healthcare systems. The price of NGS testing in Colombia and Brazil remains higher than in other countries. In Italy and Poland, ICT tools supporting the clinical interpretation of NGS results, clinical decision-making, and communication with patients are implemented in selected hospitals, whereas in Germany, they are under wider implementation. In the Republic of Korea, novel technologies and software tools are centralized at the regional/national levels, and in China, security policies and infrastructure within NGS are established under national regulation and fully enforced. In Mexico, guidelines for NGS are not defined, and genomic centres for the uptake of NGS are local (e.g., in the hospital or laboratory), which is also the case in Venezuela, Lebanon, and Angola. In the Middle East, population genetic screening in the form of limited or expanded gene panels is still lacking, and there is a shortage of well-trained personnel. In Europe, access to molecular diagnostics varies: the United Kingdom, Denmark, Sweden, and Germany show the highest uptakes of NGS. In China, guidelines to protect and ensure the lawful, fair, and transparent processing of personal data are implemented and consistently enforced, whereas in Mexico, they do not exist. In Venezuela, guidelines to protect and ensure the lawful, fair, and transparent processing of personal data are implemented but insufficient in scope.

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








