

Factors Affecting Preventive Behaviors for Safety and Health at Work during the COVID-19 Pandemic among Thai Construction Workers


Abstract
:1. Introduction
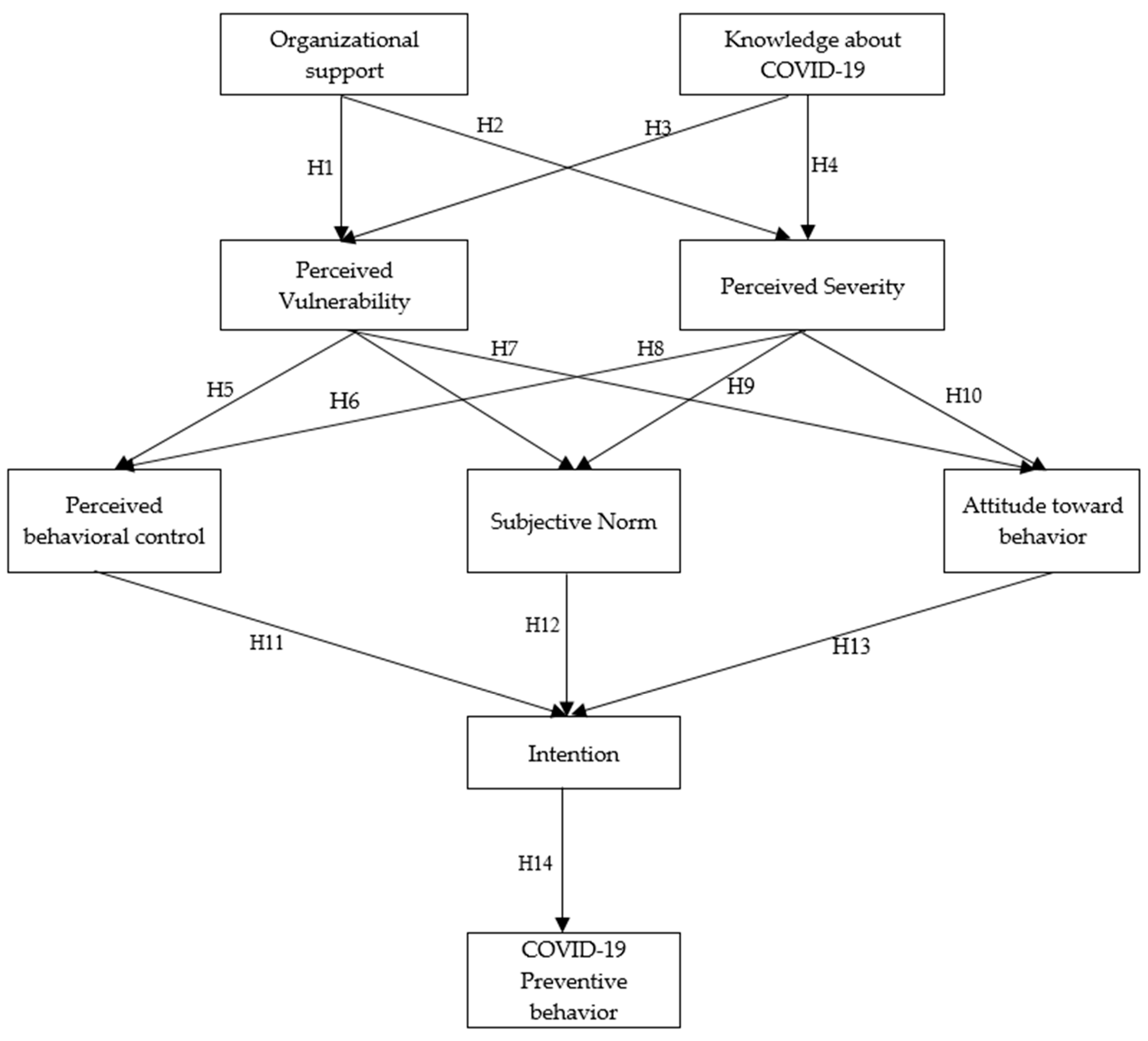
2. Theoretical Research Framework
3. Methodology
3.1. Participation and Sampling Design
3.2. Questionnaire

{kind=link}
{kind=link}
{kind=link}
| Constructs | Items | Measures | References |
|---|---|---|---|
| Organizational support | OS1 | I receive organizational support during COVID-19 pandemic. | [59,64,65] |
| OS2 | My company provides sufficient personal protective equipment for the workers (i.e., gloves, facemasks, alcohol, face shields, and hand washing). | ||
| OS3 | When the COVID-19 pandemic broke out, the company urgently established a pandemic prevention committee. | ||
| OS4 | Management promotes internal communication on COVID-19 prevention via newsletter, e-mail, Facebook, etc. | ||
| OS5 | My managers always try to enforce safety rules and procedures for COVID-19 prevention at the workplace. | ||
| Knowledge about COVID-19 | KN1 | I do understand the transmission of COVID-19. | [66,67,68,69] |
| KN2 | I do understand the incubation period of COVID-19. | ||
| KN3 | I do understand the symptoms of COVID-19. | ||
| KN4 | I do understand the protocol if I have symptoms that might lead to COVID-19. | ||
| KN5 | I do understand which hospital in local can treat COVID-19 patients. | ||
| Perceived vulnerability | PV1 | I live in an environment where I can be exposed to COVID-19 infection. | [70,71,72] |
| PV2 | I think I will be infected with COVID-19 easier than others. | ||
| PV3 | I think my friends/colleagues are vulnerable to COVID-19. | ||
| PV4 | I think Thailand is more vulnerable than other ASEAN countries. | ||
| PV5 | I think that I could become infected with COVID-19 through vaccination. | ||
| Perceived severity | PS1 | I believe that COVID-19 is highly dangerous. | [73,74] |
| PS2 | I find COVID-19 may lead to sudden death. | ||
| PS3 | I find COVID-19 may affect my mental health. | ||
| PS4 | I think COVID-19 in Thailand is more severe than in other ASEAN countries. | ||
| PS5 | If my family member were infected with COVID-19, I would keep it a secret. | ||
| Perceived behavioral control | PBC1 | The preventive protocols are completely up to me. | [33,56] |
| PBC2 | I think preventive protocols are easy to be implemented. | ||
| PBC3 | I think although I am healthy, I still have a chance to spread COVID-19 to others. | ||
| PBC4 | I think the risk of death caused by COVID-19 infection is great. | ||
| PBC5 | I think COVID-19 is highly dangerous. | ||
| Subjective Norm | SN1 | Most people I know are following the preventive protocols given by the government. | [33,56,75,76] |
| SN2 | Most people I know are staying at home and work from home. | ||
| SN3 | Most people I know are using hand sanitizer. | ||
| SN4 | Most people I know, are keeping physical distancing. | ||
| Attitude toward behavior | AB1 | I feel insecure if someone stand too close to me during the COVID-19 outbreak. | [77,78,79,80] |
| AB2 | I am worried about myself, my family members, and colleagues who may be affected by COVID-19. | ||
| AB3 | I am scared of individuals coming from the affected areas. | ||
| AB4 | I worry about the number of people infected by COVID-19. | ||
| AB5 | I feel stressed during the COVID-19 outbreak. | ||
| Intention to follow | IF1 | I intend to follow the recommended precautions until the end of the COVID-19 outbreak. | [2,81] |
| IF2 | I intend to follow every rule by the government during the COVID-19 pandemic. | ||
| IF3 | I intend to continue to use standard control measures. | ||
| IF4 | I intend to follow my company’s protocol during the spreading of COVID-19. | ||
| COVID-19 preventive behavior | PB1 | I usually wear a facial mask when I leave home. | [29,30,82,83] |
| PB2 | I embrace personal hygiene practices and washed my hands more often and longer. | ||
| PB3 | I wash my hands or clean them with alcohol often. | ||
| PB4 | I usually wear gloves when interacting with shelf materials/products. | ||
| PB5 | I practice 1-meter social distancing to reduce unnecessary infection. |
3.3. Reliability and Validity Assessments
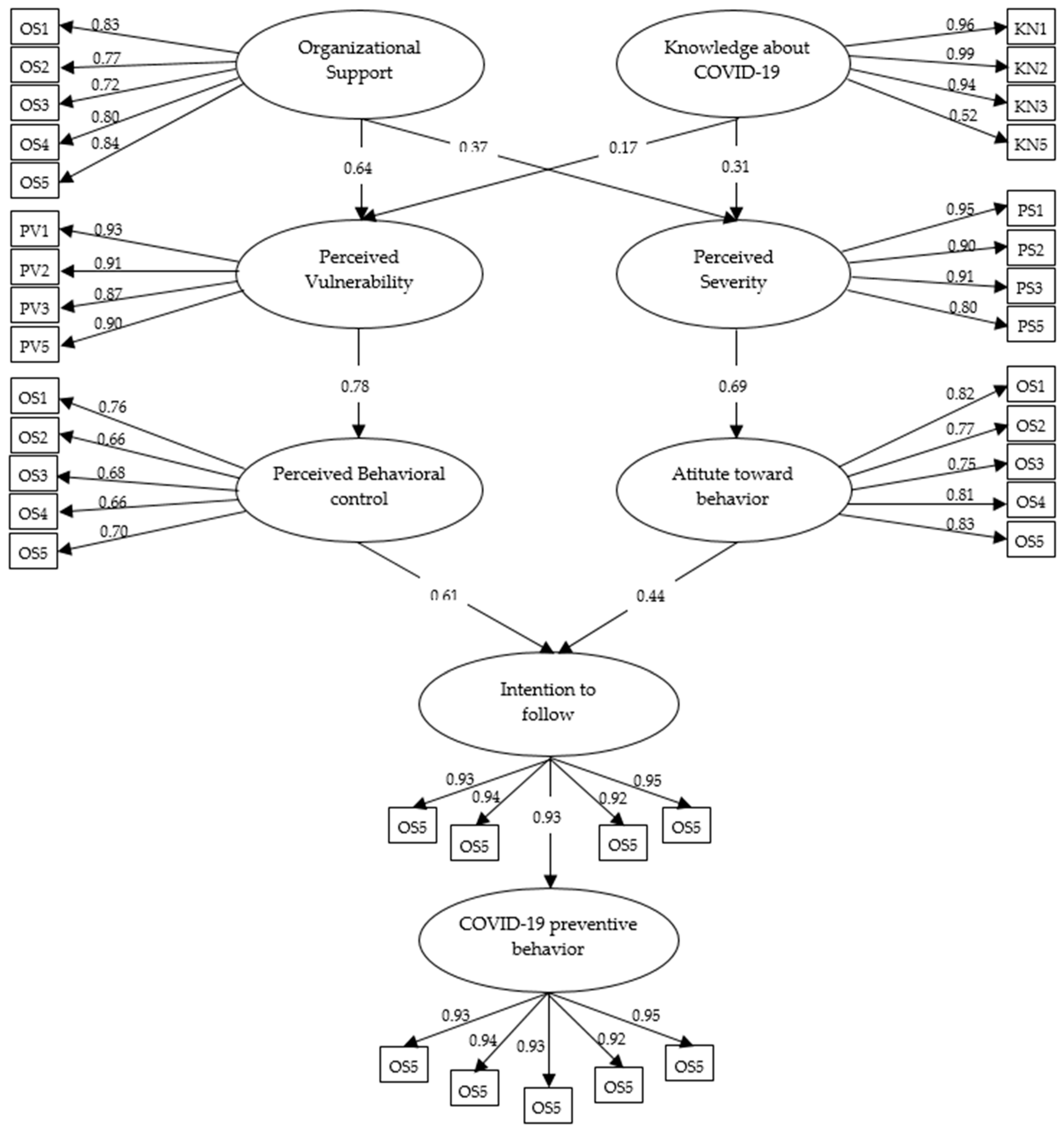
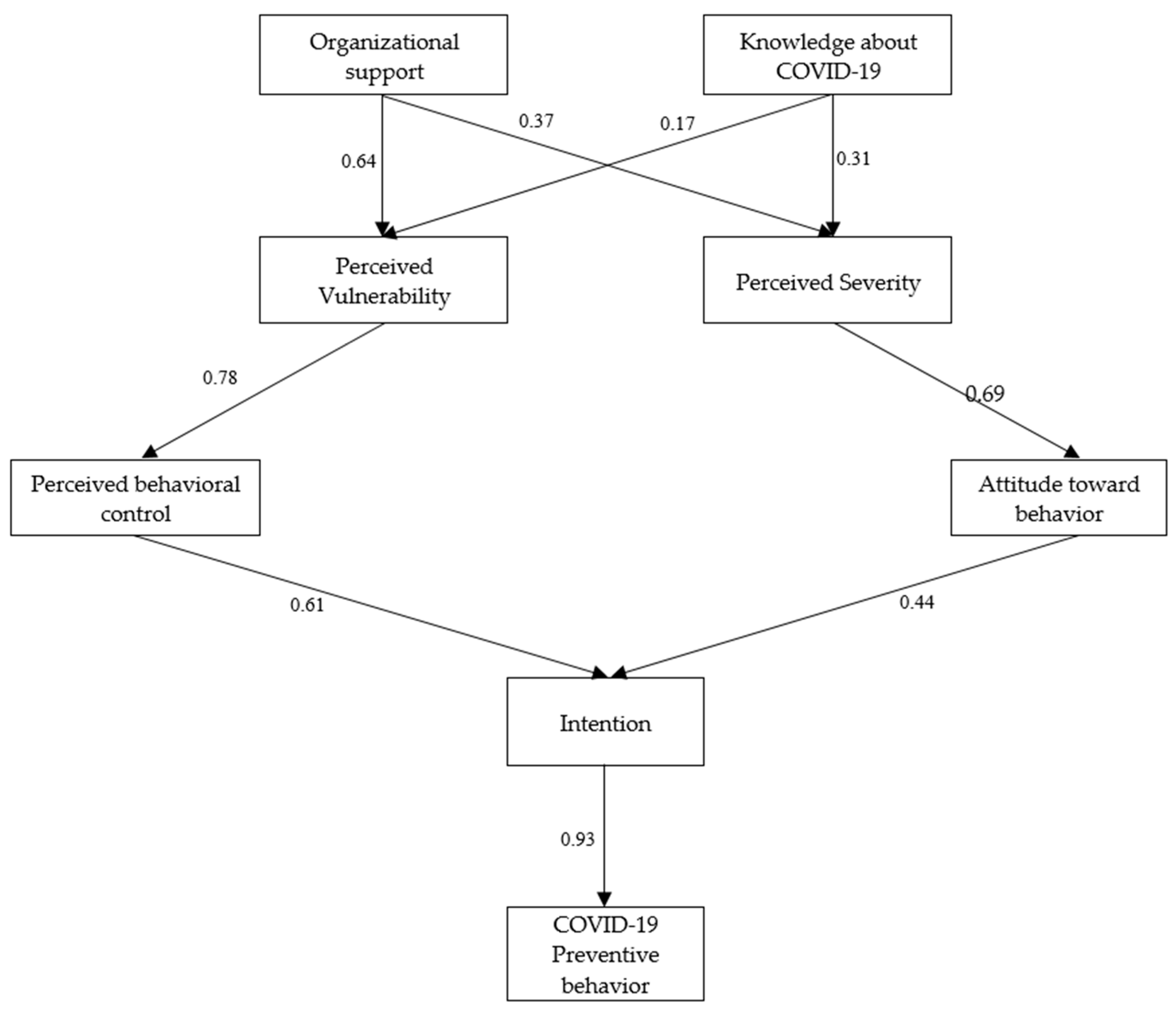
3.4. Structural Equation Modeling
4. Result
5. Discussion
5.1. Theoretical Implications
5.2. Theoretical Contribution
5.3. Practical Implications
5.4. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ashraf, G.; Aziz, A.; Qaisrani, R.N.; Chen, W.; Asif, M. Detecting and inactivating severe cute respiratory syndrome coronavirus-2 under the auspices of electrochemistry. Curr. Opin. Chem. Biol. 2021, 1, 100001. [Google Scholar]
- Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/healthywater/hygiene/etiquette/coughing_sneezing.html (accessed on 15 June 2022).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Jamal, A.J.; Mozafarihashjin, M.; Coomes, E.; Powis, J.; Li, A.X.; Paterson, A.; Anceva-Sami, S.; Barati, S.; Crowl, G.; Mubareka, S.; et al. Sensitivity of nasopharyngeal swabs and saliva for the detection of severe acute respiratory syndrome coronavirus 2. Arch. Clin. Infect. Dis. 2021, 72, 1064–1066. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Mikacenic, C.; et al. COVID-19 in critically ill patients in the Seattle region—Case series. N. Engl. J. Med 2020, 382, 2012–2022. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Zoia, E.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Elhadi, M.; Alsoufi, A.; Alhadi, A.; Hmeida, A.; Alshareea, E.; Dokali, M.; Abodabos, S.; Alsadiq, O.; Abdelkabir, M.; Ashini, A.; et al. Knowledge, attitude, and acceptance of healthcare workers and the public regarding the COVID-19 vaccine: A cross-sectional study. BMC Public Health 2021, 21, 955. [Google Scholar] [CrossRef]
- Limbu, D.K.; Piryani, R.M.; Sunny, A.K. Healthcare workers’ knowledge, attitude and practices during the COVID-19 pandemic response in a tertiary care hospital of Nepal. PLoS ONE 2020, 15, e0242126. [Google Scholar] [CrossRef]
- World Health Organization. Considerations in Adjusting Public Health and Social Measures in the Context of COVID-19. Interim Guidance. 16 April 2020. Available online: https://www.who.int/publications-detail/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-COVID-19-interim-guidance (accessed on 12 May 2020).
- Bish, A.; Michie, S. Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef]
- Rubin, G.J.; Amlôt, R.; Page, L.; Wessely, S. Public perceptions, anxiety and behavioural change in relation to the swine flu outbreak: A cross-sectional telephone survey. Br. Med. J 2009, 339, b2651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, C.S.K.; Wong, C.Y. An outbreak of the severe acute respiratory syndrome: Predictors of health behaviours and effect of community prevention measures in Hong Kong, China. Am. J. Public Health 2003, 93, 1887–1888. [Google Scholar] [CrossRef]
- Puterman, E.; Delongis, A.; Lee-Baggley, D.; Greenglass, E. Coping and health behaviours in times of global health crises: Lessons from SARS and West Nile. Glob. Public Health 2009, 4, 69–81. [Google Scholar] [CrossRef]
- Vartti, A.-M.; Oenema, A.; Schreck, M.; Uutela, A.; de Zwart, O.; Brug, J.; Aro, A.R. SARS Knowledge, Perceptions, and Behaviors: A Comparison between Finns and the Dutch during the SARS Outbreak in 2003. Int. J. Behav. Med. 2009, 16, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Pfattheicher, S.; Nockur, L.; Böhm, R.; Sassenrath, C.; Petersen, M.B. The Emotional Path to Action: Empathy Promotes Physical Distancing and Wearing of Face Masks During the COVID-19 Pandemic. Psychol. Sci. 2020, 31, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2021, 51, 1763–1769. [Google Scholar] [CrossRef]
- Simpeh, F.; Amoah, C. Assessment of measures instituted to curb the spread of COVID-19 on construction site. Int. J. Constr. Manag. 2021, 1–19. [Google Scholar] [CrossRef]
- Koh, D. Migrant workers and COVID-19. Occup. Environ. Med. 2020, 77, 634–636. [Google Scholar] [CrossRef] [PubMed]
- Onubi, H.O.; Yusof, N.; Hassan, A.S. Perceived COVID-19 Safety Risk and Safety Behavior on Construction Sites: Role of Safety Climate and Firm Size. J. Constr. Eng. Manag. 2021, 147, 04021153. [Google Scholar] [CrossRef]
- Pasco, R.F.; Fox, S.J.; Johnston, S.C.; Pignone, M.; Meyers, L.A. Estimated Association of Construction Work With Risks of COVID-19 Infection and Hospitalization in Texas. JAMA Netw. Open 2020, 3, e2026373. [Google Scholar] [CrossRef] [PubMed]
- Jamaludin, S.; Azmir, N.A.; Ayob, A.F.M.; Zainal, N. COVID-19 exit strategy: Transitioning towards a new normal. Ann. Med. Surg. 2020, 59, 165–170. [Google Scholar] [CrossRef]
- Nnaji, C.; Jin, Z.; Karakhan, A. Safety and health management response to COVID-19 in the construction industry: A perspective of fieldworkers. Process. Saf. Environ. Prot. 2022, 159, 477–488. [Google Scholar] [CrossRef]
- Carvalhais, C.; Querido, M.; Pereira, C.C.; Santos, J. Biological risk assessment: A challenge for occupational safety and health practitioners during the COVID-19 (SARS-CoV-2) pandemic. Work 2021, 69, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Rossi, M.F.; Borrelli, I.; Santoro, P.E.; Amantea, C.; Daniele, A.; Tumminello, A.; Moscato, U. Returning to work and the impact of post COVID-19 condition: A systematic review. Work 2022, 73, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Huo, J.; Li, J.; Jiang, Y. Research on the influence of the COVID-19 epidemic on work stress of returning workers in China: A study based on empirical analyses of industrial enterprises. Work 2020, 67, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Çelikkalp, Ü.; Irmak, A.Y.; Ekuklu, G. Working conditions and anxiety levels of employees who have to work during the COVID-19 pandemic. Work 2021, 70, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Lüdecke, D.; von dem Knesebeck, O. Protective Behavior in Course of the COVID-19 Outbreak—Survey Results From Germany. Front. Public Health 2020, 8, 567. [Google Scholar] [CrossRef] [PubMed]
- Dai, B.; Fu, D.; Meng, G.; Liu, B.; Li, Q.; Liu, X. The Effects of Governmental and Individual Predictors on COVID-19 Protective Behaviors in China: A Path Analysis Model. Public Adm. Rev. 2020, 80, 797–804. [Google Scholar] [CrossRef]
- Rogers, R.W.; Prentice-Dunn, S. Protection motivation theory. In Handbook of Health Behavior Research 1: Personal and Social Determinants; Gochman, D.S., Ed.; Plenum Press: New York, NY, USA, 1997; pp. 113–132. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Prasetyo, Y.T.; Castillo, A.M.; Salonga, L.J.; Sia, J.A.; Seneta, J.A. Factors affecting perceived effectiveness of COVID-19 prevention measures among Filipinos during Enhanced Community Quarantine in Luzon, Philippines: Integrating Protection Motivation Theory and extended Theory of Planned Behavior. Int. J. Infect. Dis. 2020, 99, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Ong, A.K.S.; Prasetyo, Y.T.; Salazar, J.M.L.D.; Erfe, J.J.C.; Abella, A.A.; Young, M.N.; Chuenyindee, T.; Nadlifatin, R.; Redi, A.A.N.P. Investigating the acceptance of the reopening Bataan nuclear power plant: Integrating protection motivation theory and extended theory of planned behavior. Nucl. Eng. Technol. 2022, 54, 1115–1125. [Google Scholar] [CrossRef]
- Westcott, R.; Ronan, K.; Bambrick, H.; Taylor, M. Expanding protection motivation theory: Investigating an application to animal owners and emergency responders in bushfire emergencies. BMC Psychol. 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.-S.; Feng, J.-Y. Residents’ Disaster Preparedness after the Meinong Taiwan Earthquake: A Test of Protection Motivation Theory. Int. J. Environ. Res. Public Health 2018, 15, 1434. [Google Scholar] [CrossRef]
- Kurata, Y.B.; Prasetyo, Y.T.; Ong, A.K.S.; Nadlifatin, R.; Chuenyindee, T. Factors affecting perceived effectiveness of Typhoon Vamco (Ulysses) flood disaster response among Filipinos in Luzon, Philippines: An integration of protection motivation theory and extended theory of planned behavior. Int. J. Disaster Risk Reduct. 2022, 67, 102670. [Google Scholar] [CrossRef]
- Gong, J.; Stanton, B.; Lunn, S.; Deveaux, L.; Li, X.; Marshall, S.; Brathwaite, N.V.; Cottrell, L.; Harris, C.; Chen, X. Effects Through 24 Months of an HIV/AIDS Prevention Intervention Program Based on Protection Motivation Theory Among Preadolescents in the Bahamas. Pediatrics 2009, 123, e917–e928. [Google Scholar] [CrossRef] [PubMed]
- Al-Rasheed, M. Protective Behavior against COVID-19 among the Public in Kuwait: An Examination of the Protection Motivation Theory, Trust in Government, and Sociodemographic Factors. Soc. Work. Public Health 2020, 35, 546–556. [Google Scholar] [CrossRef]
- Hung, W.-S.; Hu, S.C.; Hsu, Y.-C.; Chen, K.-L.; Chen, K.-H.; Yu, M.-C.; Chen, K.-T. Factors affecting the use of anti-malaria preventive measures among Taiwan immigrants returning to malaria-endemic regions. Travel Med. Infect. Dis. 2014, 12, 370–377. [Google Scholar] [CrossRef]
- Chen, M.-F.; Tung, P.-J. Developing an extended Theory of Planned Behavior model to predict consumers’ intention to visit green hotels. Int. J. Hosp. Manag. 2014, 36, 221–230. [Google Scholar] [CrossRef]
- Bamidis, P.D.; Gabarron, E.; Hors-Fraile, S.; Konstantinidis, E.; Konstantinidis, S.; Rivera, O. Gamification and behavioral change: Techniques for health social media. In Participatory Health through Social Media; Academic Press: Cambridge, MA, USA, 2016; pp. 112–135. [Google Scholar]
- Leslie, R.A.; Zhou, S.S.; Macinga, D.R. Inactivation of SARS-CoV-2 by commercially available alcohol-based hand sanitizers. Am. J. Infect. Control 2021, 49, 401–402. [Google Scholar] [CrossRef]
- Gardona, R.G.B.; da Silva, J.V.; Arruda, G.; Damin, S.; Abdala, E.; Lima, C.A.S.; Vasconcellos, L.D.S.; Queiroz, W.; Zandonái, A.C.; Danielsk, A.M.; et al. Brazilians’ level of knowledge, attitudes and practices towards COVID-19: A cross-sectional study. Sao Paulo Med. J. 2022, 140, 331–340. [Google Scholar] [CrossRef]
- Bashirian, S.; Jenabi, E.; Khazaei, S.; Barati, M.; Karimi-Shahanjarini, A.; Zareian, S.; Rezapur-Shahkolai, F.; Moeini, B. Factors associated with preventive behaviours of COVID-19 among hospital staff in Iran in 2020: An application of the Protection Motivation Theory. J. Hosp. Infect. 2020, 105, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Rad, R.E.; Mohseni, S.; Takhti, H.K.; Azad, M.H.; Shahabi, N.; Aghamolaei, T.; Norozian, F. Application of the protection motivation theory for predicting COVID-19 preventive behaviors in Hormozgan, Iran: A cross-sectional study. BMC Public Health 2021, 21, 466. [Google Scholar] [CrossRef]
- Mortada, E.; Abdel-Azeem, A.; Al Showair, A.; Zalat, M.M. Preventive behaviors towards COVID-19 pandemic among healthcare providers in Saudi Arabia using the protection motivation theory. Risk Manag. Healthc. Policy 2021, 14, 685. [Google Scholar]
- Nguyen, D.T.; Tran, V.D.; Ghafoor, A. The Impact of COVID-19 lockdown on Intention to Follow Preventive Measures in Vietnam: Integrated Protection Motivation Theory and Theory Planed Behavior. Cogent Bus. Manag. 2022, 9, 2054502. [Google Scholar] [CrossRef]
- Trifiletti, E.; Shamloo, S.E.; Faccini, M.; Zaka, A. Psychological predictors of protective behaviours during the COVID-19 pandemic: Theory of planned behaviour and risk perception. J. Community Appl. Soc. Psychol. 2022, 32, 382–397. [Google Scholar] [CrossRef]
- Shanka, M.S.; Kotecho, M.G. Combining rationality with morality—Integrating theory of planned behavior with norm activation theory to explain compliance with COVID-19 prevention guidelines. Psychol. Health Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Ajzen, I.; Madden, T.J. Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. J. Exp. Soc. Psychol. 1986, 22, 453–474. [Google Scholar] [CrossRef]
- Aschwanden, D.; Strickhouser, J.E.; Sesker, A.A.; Lee, J.H.; Luchetti, M.; Terracciano, A.; Sutin, A.R. Preventive Behaviors During the COVID-19 Pandemic: Associations With Perceived Behavioral Control, Attitudes, and Subjective Norm. Front. Public Health 2021, 9, 662835. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Psychology Press: New York, NY, USA, 2010. [Google Scholar]
- Manstead, A.S.R. The benefits of a critical stance: A reflection on past papers on the theories of reasoned action and planned behaviour. Br. J. Soc. Psychol. 2011, 50, 366–373. [Google Scholar] [CrossRef]
- Jandawapee, S.; Siripipatthanakul, S.; Phayaphrom, B.; Limna, P. Factors Influencing Intention to Follow the Preventive COVID-19 Protocols Among Thai People. Int. J. Behav. Sci. 2022, 2, 1–15. [Google Scholar]
- Han, H.; Hsu, L.-T.; Sheu, C. Application of the Theory of Planned Behavior to green hotel choice: Testing the effect of environmental friendly activities. Tour. Manag. 2010, 31, 325–334. [Google Scholar] [CrossRef]
- Taylor, S.; Todd, P. Understanding Household Garbage Reduction Behavior: A Test of an Integrated Model. J. Public Policy Mark. 1995, 14, 192–204. [Google Scholar] [CrossRef]
- Tonglet, M.; Phillips, P.S.; Read, A.D. Using the Theory of Planned Behaviour to investigate the determinants of recycling behaviour: A case study from Brixworth, UK. Resour. Conserv. Recycl. 2004, 41, 191–214. [Google Scholar] [CrossRef]
- Husain, F.; Shahnawaz, G.; Khan, N.H.; Parveen, H.; Savani, K. Intention to get COVID-19 vaccines: Exploring the role of attitudes, subjective norms, perceived behavioral control, belief in COVID-19 misinformation, and vaccine confidence in Northern India. Hum. Vaccines Immunother. 2021, 17, 3941–3953. [Google Scholar] [CrossRef]
- Gualano, M.R.; Santoro, P.E.; Borrelli, I.; Rossi, M.F.; Amantea, C.; Tumminello, A.; Daniele, A.; Beccia, F.; Moscato, U. Employee Participation in Workplace Vaccination Campaigns: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1898. [Google Scholar] [CrossRef]
- Mamman, M.; Ogunbado, A.F.; Abu-Bakr, A.S. Factors influencing customer’s behavioral intention to adopt Islamic banking in Northern Nigeria: A proposed framework. J. Econ. Financ. 2016, 7, 51–55. [Google Scholar]
- Norman, P.; Wilding, S.; Conner, M. Reasoned action approach and compliance with recommended behaviours to prevent the transmission of the SARS-CoV-2 virus in the UK. Br. J. Health Psychol. 2020, 25, 1006–1019. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef]
- Chi, H.; Vu, T.-V.; Vo-Thanh, T.; Nguyen, N.P.; Van Nguyen, D. Workplace health and safety training, employees’ risk perceptions, behavioral safety compliance, and perceived job insecurity during COVID-19: Data of Vietnam. Data Brief 2020, 33, 106346. [Google Scholar] [CrossRef]
- Vinodkumar, M.; Bhasi, M. Safety management practices and safety behaviour: Assessing the mediating role of safety knowledge and motivation. Accid. Anal. Prev. 2010, 42, 2082–2093. [Google Scholar] [CrossRef]
- Liu, L. Emerging study on the transmission of the Novel Coronavirus (COVID-19) from urban perspective: Evidence from China. Cities 2020, 103, 102759. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M. Factors determining the diffusion of COVID-19 and suggested strategy to prevent future accelerated viral infectivity similar to COVID. Sci. Total Environ. 2020, 729, 138474. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef]
- Nicola, M.; O’Neill, N.; Sohrabi, C.; Khan, M.; Agha, M.; Agha, R. Evidence based management guideline for the COVID-19 pandemic—Review article. Int. J. Surg. 2020, 77, 206–216. [Google Scholar] [CrossRef]
- Guidry, J.P.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control 2021, 49, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Oh, S. Factors associated with preventive behaviors for COVID-19 among adolescents in South Korea. J. Pediatr. Nurs. 2022, 62, e69–e76. [Google Scholar] [CrossRef]
- Chuenyindee, T.; Ong, A.K.S.; Prasetyo, Y.T.; Persada, S.F.; Nadlifatin, R.; Sittiwatethanasiri, T. Factors Affecting the Perceived Usability of the COVID-19 Contact-Tracing Application “Thai Chana” during the Early COVID-19 Omicron Period. Int. J. Environ. Res. Public Health 2022, 19, 4383. [Google Scholar] [CrossRef] [PubMed]
- de Zwart, O.; Veldhuijzen, I.K.; Elam, G.; Aro, A.R.; Abraham, T.; Bishop, G.D.; Voeten, H.A.C.M.; Richardus, J.H.; Brug, J. Perceived Threat, Risk Perception, and Efficacy Beliefs Related to SARS and Other (Emerging) Infectious Diseases: Results of an International Survey. Int. J. Behav. Med. 2009, 16, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Walrave, M.; Waeterloos, C.; Ponnet, K. Adoption of a Contact Tracing App for Containing COVID-19: A Health Belief Model Approach. JMIR Public Health Surveill. 2020, 6, e20572. [Google Scholar] [CrossRef]
- Conner, K. Face Masks in Cars, Stores, Outside: Places You’re Expected to Wear a Covering. 2020. Available online: https://www.cnet.com/health/face-masks-in-cars-stores-outside-places-youre-expected-to-wear-a-covering/ (accessed on 5 June 2020).
- Yancey-Bragg, N.; Bravo, N.; Bravo, V. Can I Still Go For A Walk, Run Under Stay at Home Orders? Should I Wear A Mask? 2020. Available online: https://www.usatoday.com/in-depth/news/health/2020/04/15/coronavirus-masks-how-safely-go-outside-during-stay-home-order/2970072001/ (accessed on 20 April 2020).
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatry 2020, 51, 102083. [Google Scholar] [CrossRef]
- Shader, R.I. COVID-19 and depression. Clin. Ther. 2020, 42, 962–963. [Google Scholar] [CrossRef] [PubMed]
- Sarkodie, S.A.; Owusu, P.A. Investigating the cases of novel coronavirus disease (COVID-19) in China using dynamic statistical techniques. Heliyon 2020, 6, e03747. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef]
- Oyeniran, O.; Chia, T. Novel coronavirus disease 2019 (COVID-19) outbreak in Nigeria: How effective are government interventions? Ethics Med. Public Health 2020, 14, 100515. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, M. Personality Traits, Risk Perception, and Protective Behaviors of Arab Residents of Qatar During the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 20, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Yang, W.; Liu, T.; Xia, F. Demographic Influences on Perceived Stressors of Construction Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4192. [Google Scholar] [CrossRef]
- Ab Hamid, M.R.; Sami, W.; Sidek, M.M. Discriminant validity assessment: Use of Fornell & Larker criterion versus HTMT criterion. Int. J. Phys. Conf. Ser. 2017, 890, 012163. [Google Scholar]
- Fornell, C.; Larker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Bagozzi, R.P.; Yi, Y. On the evaluation of structural equation models. J. Acad. Mark. Sci. 1988, 16, 74–94. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sinkovics, R.R. The use of partial least squares path modeling in international marketing. In New Challenges to International Marketing; Emerald Group Publishing Ltd.: Bradford, UK, 2009; Volume 20, pp. 277–319. [Google Scholar]
- Hair, J.F.; Hult, G.T.M., Jr.; Ringle, C.; Sarstedt, M. A primer on partial least squares structural equation modeling (PLS-SEM). Sage Open 2016, 32, 220–221. [Google Scholar]
- Hair, J.F. Multivariate Data Analysis: A Global Perspective. Upper Saddle River Pearson: Hoboken, NJ, USA, 2010. [Google Scholar]
- Martinez, J.E.F.; Prasetyo, Y.T.; Robielos, R.A.C.; Panopio, M.M.; Urlanda, A.A.C.; Topacio-Manalaysay, K.A.C. The usability of metropolitan manila development authority (MMDA) mobile traffic navigator as perceived by users in Quezon City and Mandaluyong City, Philippines. In Proceedings of the 5th International Conference on Industrial and Business Engineering, Hong Kong, China, 27–29 September 2019; pp. 207–211. [Google Scholar]
- Torres, M.E.S.; Prasetyo, Y.T.; Robielos, R.A.C.; Domingo, C.V.Y.; Morada, M.C. The effect of nutrition labelling on purchasing decisions. In Proceedings of the 2019 5th International Conference on Industrial and Business Engineering—ICIBE 2019 USAID, Climate Change Risk Profile: Philippines, 8 February 2017; Available online: https://www.climatelinks.org/resources/climate-change-risk-profile-philippines (accessed on 8 February 2017).
- Hu, L.T.; Benler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Steiger, J.H. Understanding the limitations of global fit assessment in structural equation modeling. Pers. Individ. Differ. 2007, 42, 893–898. [Google Scholar] [CrossRef]
- Labour Protection Act. 1998. Available online: http://www.klongrua.go.th (accessed on 20 January 2023).
- Eisenberger, R.; Stinglhamber, F. Perceived Organizational Support: Fostering Enthusiastic and Productive Employees; American Psychological Association: Washington, DC, USA, 2011. [Google Scholar]
- Nguyen, H.N.; Tran, M.D. The effect of perceived organizational support on employee engagement during the COVID-19 pandemic: An empirical study in Vietnam. J. Asian Finance Econ. Bus. 2021, 8, 415–426. [Google Scholar]
- Duncan, L.A.; Schaller, M. Prejudicial Attitudes Toward Older Adults May Be Exaggerated When People Feel Vulnerable to Infectious Disease: Evidence and Implications. Anal. Soc. Issues Public Policy 2009, 9, 97–115. [Google Scholar] [CrossRef]
- Miller, S.L.; Maner, J.K. Overperceiving disease cues: The basic cognition of the behavioral immune system. J. Pers. Soc. Psychol. 2012, 102, 1198–1213. [Google Scholar] [CrossRef]
- Mortensen, C.R.; Becker, D.V.; Ackerman, J.M.; Neuberg, S.L.; Kenrick, D.T. Infection breeds reticence: The effects of disease salience on self-perceptions of personality and behavioral avoidance tendencies. Psychol. Sci. 2010, 21, 40–447. [Google Scholar] [CrossRef] [PubMed]
- Neuberg, S.L.; Kenrick, D.T.; Schaller, M. Human threat management systems: Self-protection and disease avoidance. Neurosci. Biobehav. Rev. 2011, 35, 1042–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, Y.; Cheng, Y.; Sui, M. The Moderating Effects of Perceived Severity on the Generational Gap in Preventive Behaviors during the COVID-19 Pandemic in the U.S. Int. J. Environ. Res. Public Health 2021, 18, 2011. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Prentice Hall: Hoboken, NJ, USA, 2009. [Google Scholar]



| Characteristics | Category | N | % |
|---|---|---|---|
| Gender | Male Female | 381 229 | 62.5 37.5 |
| Age group | Below 15 years old 15–24 years old 25–34 years old 35–44 years old 45–54 years old | 17 55 232 185 94 | 2.8 9.0 38.0 30.0 15.4 |
| 55–64 years old Above 64 years old | 27 - | 4.4 - | |
| Educational level | No formal education Primary school Middle school High school Post-secondary | 53 141 199 106 111 | 8.7 23.1 32.6 17.4 18.2 |
| Vaccinated COVID-19 protection | Yes No | 456 154 | 74.8 25.2 |
| Detected COVID-19 disease | Yes No | 404 206 | 66.2 33.8 |
| Goodness of Fit Measures | Parameter Estimates | Minimum Cutoff |
|---|---|---|
| Incremental Fitness Index (IFI) | 0.99 | >0.90 a |
| Tucker Lewis Index (TLI) | 0.99 | >0.90 b |
| Comparative Fit Index (CFI) | 0.98 | >0.90 a |
| Root Mean Square Error of Approximation (RMSEA) | 0.04 | <0.08 a |
| Factors | Items | Mean | STD | Factor Loading | |
|---|---|---|---|---|---|
| Initial | Final | ||||
| Organizational support | OS1 | 4.09 | 0.75 | 0.81 | 0.83 |
| OS2 | 4.07 | 0.79 | 0.80 | 0.77 | |
| OS3 | 4.04 | 0.81 | 0.75 | 0.72 | |
| OS4 | 4.11 | 0.74 | 0.80 | 0.80 | |
| OS5 | 4.16 | 0.66 | 0.80 | 0.84 | |
| Knowledge about COVID-19 | KN1 | 4.27 | 0.63 | 0.89 | 0.96 |
| KN2 | 4.29 | 0.64 | 0.91 | 0.99 | |
| KN3 | 4.22 | 0.68 | 0.89 | 0.94 | |
| KN5 | 3.95 | 1.06 | 0.62 | 0.52 | |
| Perceived Vulnerability | PV1 | 4.12 | 0.66 | 0.85 | 0.93 |
| PV2 | 4.05 | 0.73 | 0.85 | 0.91 | |
| PV3 | 4.01 | 0.74 | 0.84 | 0.87 | |
| PV4 | 4.07 | 0.72 | 0.83 | 0.90 | |
| Perceived Severity | PS1 | 4.22 | 0.65 | 0.81 | 0.95 |
| PS2 | 4.25 | 0.65 | 0.83 | 0.90 | |
| PS3 | 4.28 | 0.66 | 0.83 | 0.91 | |
| PS4 | 4.24 | 0.65 | 0.82 | 0.80 | |
| Perceived behavioral control | PBC1 | 4.14 | 0.69 | 0.75 | 0.76 |
| PBC2 | 4.10 | 0.73 | 0.69 | 0.66 | |
| PBC3 | 4.09 | 0.71 | 0.69 | 0.68 | |
| PBC4 | 4.04 | 0.72 | 0.66 | 0.66 | |
| PBC5 | 4.08 | 0.70 | 0.76 | 0.70 | |
| Attitude toward behavior | AB1 | 4.04 | 0.81 | 0.74 | 0.83 |
| AB2 | 3.89 | 0.81 | 0.75 | 0.81 | |
| AB3 | 3.91 | 0.81 | 0.75 | 0.75 | |
| AB4 | 3.95 | 0.81 | 0.76 | 0.77 | |
| AB5 | 4.04 | 0.76 | 0.71 | 0.82 | |
| Intention to follow | IF1 | 4.40 | 0.60 | 0.88 | 0.93 |
| IF2 | 4.46 | 0.60 | 0.89 | 0.94 | |
| IF3 | 4.51 | 0.57 | 0.90 | 0.92 | |
| IF4 | 4.42 | 0.59 | 0.89 | 0.95 | |
| COVID-19 Preventive behavior | PB1 | 4.35 | 0.59 | 0.70 | 0.80 |
| PB2 | 4.34 | 0.63 | 0.87 | 0.95 | |
| PB3 | 4.36 | 0.58 | 0.87 | 0.94 | |
| PB4 | 4.32 | 0.62 | 0.87 | 0.99 | |
| PB5 | 4.34 | 0.63 | 0.87 | 0.97 | |
| Goodness of Fit Measures | Parameter Estimates | Minimum Cutoff |
|---|---|---|
| Incremental Fit Index (IFI) | 0.91 | >0.90 a |
| Tucker Lewis Index (TLI) | 0.90 | >0.90 b |
| Comparative Fit Index (CFI) | 0.91 | >0.90 a |
| Root Mean Square Error of Approximation (RMSEA) | 0.70 | <0.08 a |
| Factors | Cronbach’s Alpha | Composite Reliability | AVE |
|---|---|---|---|
| Organizational support | 0.89 | 0.79 | 0.63 |
| Knowledge about COVID-19 | 0.87 | 0.87 | 0.76 |
| Perceived Vulnerability | 0.95 | 0.89 | 0.80 |
| Perceived Severity | 0.69 | 0.71 | 0.52 |
| Perceived behavioral control | 0.94 | 0.80 | 0.63 |
| Attitude toward behavior | 0.90 | 0.94 | 0.87 |
| Intention to follow | 0.97 | 0.86 | 0.74 |
| COVID-19 Preventive behavior | 0.97 | 0.93 | 0.87 |
| Variables | OS | KN | PV | PS | PBC | AT | IF | PB |
|---|---|---|---|---|---|---|---|---|
| OS | 0.79 | |||||||
| KN | 0.22 ** | 0.87 | ||||||
| PV | 0.31 ** | 0.33 ** | 0.89 | |||||
| PS | 0.28 ** | 0.29 ** | 0.40 ** | 0.71 | ||||
| PBC | 0.20 ** | 0.19 ** | 0.30 ** | 0.32 ** | 0.80 | |||
| AT | 0.26 ** | 0.20 ** | 0.29 ** | 0.40 ** | 0.2 ** | 0.94 | ||
| IF | 0.15 ** | 0.20 ** | 0.18 ** | 0.32 ** | 0.17 ** | 0.31 ** | 0.86 | |
| PB | 0.21 ** | 0.28 ** | 0.32 ** | 0.36 ** | 0.29 ** | 0.47 ** | 0.50 ** | 0.93 |
| Variable | Direct Effect | p-Value | Indirect Effect | p-Value | Total Effect | p-Value |
|---|---|---|---|---|---|---|
| OS→PV | 0.404 | <0.0001 | - | - | 0.404 | <0.0001 |
| OS→PS | 0.349 | <0.0001 | - | - | 0.349 | <0.0001 |
| OS→AB | - | - | 0.330 | <0.0001 | 0.330 | <0.0001 |
| OS→PBC | - | - | 0.342 | <0.0001 | 0.342 | <0.0001 |
| OS→IF | - | - | 0.137 | 0.001 | 0.137 | 0.001 |
| OS→PB | - | - | 0.295 | <0.0001 | 0.295 | <0.0001 |
| KN→PV | 0.378 | <0.0001 | - | - | 0.378 | <0.0001 |
| KN→PS | 0.319 | <0.0001 | - | - | 0.319 | <0.0001 |
| KN→AB | - | - | 0.164 | <0.0001 | 0.164 | <0.0001 |
| KN→PBC | - | - | 0.151 | <0.0001 | 0.151 | <0.0001 |
| KN→IF | - | - | 0.114 | 0.002 | 0.114 | 0.002 |
| KN→PB | - | - | 0.195 | <0.0001 | 0.195 | <0.0001 |
| PV→PBC | 0.426 | <0.0001 | - | - | 0.426 | <0.0001 |
| PV→IF | - | - | 0.127 | 0.003 | 0.127 | 0.003 |
| PV→PB | - | - | 0.246 | <0.0001 | 0.246 | <0.0001 |
| PS→AB | 0.430 | <0.0001 | - | - | 0.430 | <0.0001 |
| PS→IF | - | - | 0.263 | <0.0001 | 0.263 | <0.0001 |
| PS→PB | - | - | 0.438 | <0.0001 | 0.438 | <0.0001 |
| PBC→IF | 0.183 | <0.0001 | - | - | 0.183 | <0.0001 |
| PBC→PB | - | - | 0.481 | <0.0001 | 0.481 | <0.0001 |
| AB→IF | 0.348 | <0.0001 | - | - | 0.348 | <0.0001 |
| AB→PB | - | - | 0.370 | <0.0001 | 0.370 | <0.0001 |
| IF→PB | 0.538 | <0.0001 | - | - | 0.538 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khaday, S.; Li, K.-W.; Dorloh, H. Factors Affecting Preventive Behaviors for Safety and Health at Work during the COVID-19 Pandemic among Thai Construction Workers. Healthcare 2023, 11, 426. https://doi.org/10.3390/healthcare11030426
Khaday S, Li K-W, Dorloh H. Factors Affecting Preventive Behaviors for Safety and Health at Work during the COVID-19 Pandemic among Thai Construction Workers. Healthcare. 2023; 11(3):426. https://doi.org/10.3390/healthcare11030426
Chicago/Turabian StyleKhaday, Samsiya, Kai-Way Li, and Halimoh Dorloh. 2023. "Factors Affecting Preventive Behaviors for Safety and Health at Work during the COVID-19 Pandemic among Thai Construction Workers" Healthcare 11, no. 3: 426. https://doi.org/10.3390/healthcare11030426