

Prevalence of Potentially Inappropriate Prescriptions According to the New STOPP/START Criteria in Nursing Homes: A Systematic Review
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
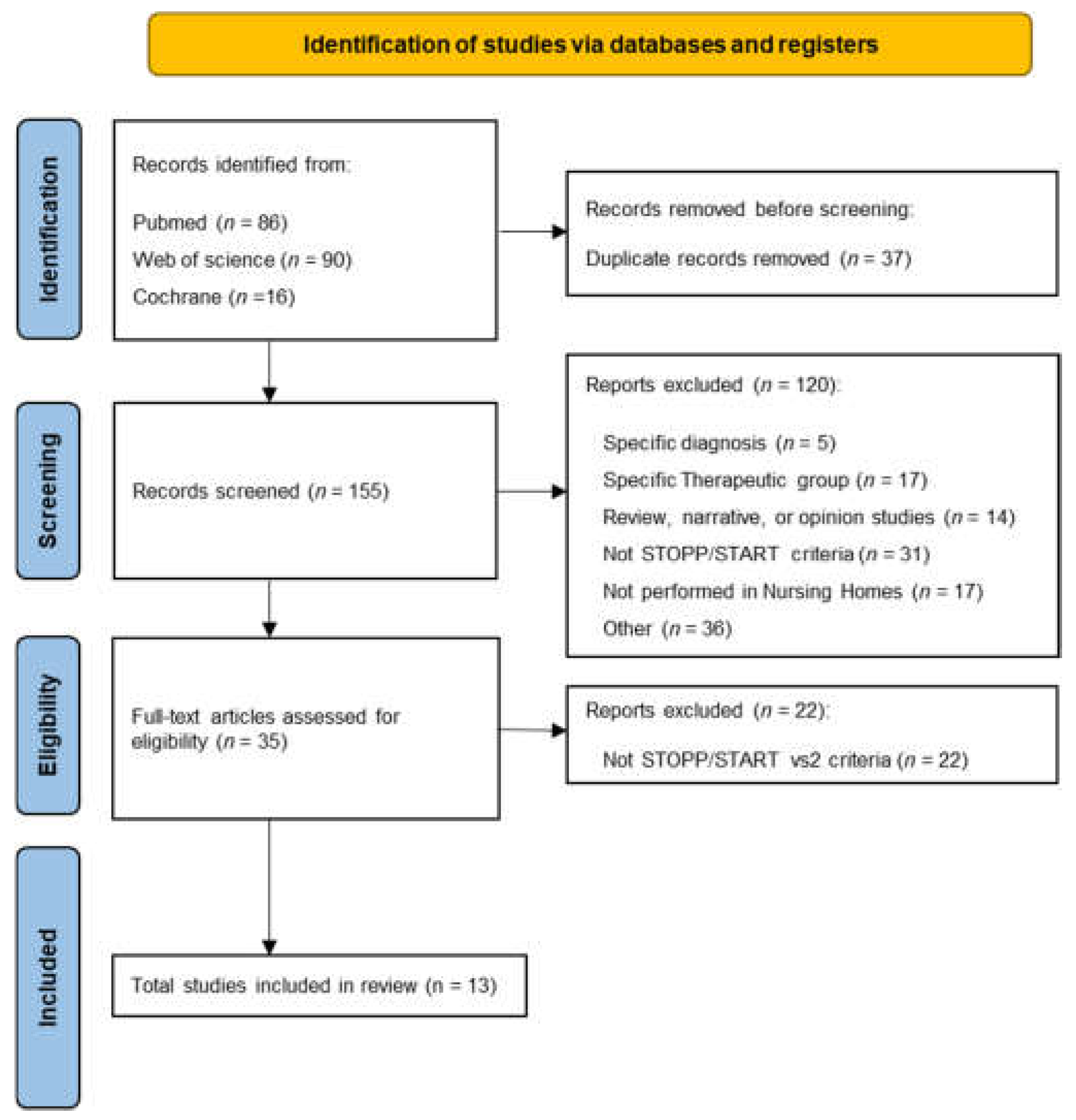
2.1. Search Strategy
2.2. Selection Criteria and Data Extraction
2.3. Quality Assessment of Studies
3. Results
3.1. Characteristics of the Studies and Residents in NH
3.2. Prevalence of PIPs According to New STOPP/START Criteria
3.3. Factors Associated with the Appearance of PIPs
3.4. Study Quality Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADRs | Adverse drug reactions |
| CVS | Cardiovascular system |
| GRADE | Grading of Recommendations, Assessment, Development and Evaluation |
| NH | Nursing homes |
| NSAIDs | Nonsteroidal anti-inflammatory drugs |
| PIPs | Potentially inadequate prescriptions |
| PRISMA | Preferred reporting items for systematic reviews and meta-analysis |
| START | Screening Tool to Alert to Right Treatment |
| STOPP | Screening Tool of Older Persons’ Prescriptions |
Appendix A

{kind=link}
| ((((“inappropriate”[All Fields] OR “inappropriately”[All Fields] OR “inappropriateness”[All Fields]) AND “prescri*”[All Fields] AND (“potentially inappropriate medication list”[MeSH Terms] OR (“potentially”[All Fields] AND “inappropriate”[All Fields] AND “medication”[All Fields] AND “list”[All Fields]) OR “potentially inappropriate medication list”[All Fields] OR “stopp”[All Fields])) AND “nursing homes”[Title/Abstract]) OR (((“inappropriate”[All Fields] OR “inappropriately”[All Fields] OR “inappropriateness”[All Fields]) AND “prescri*”[All Fields] AND (“start”[All Fields] OR “started”[All Fields] OR “starting”[All Fields] OR “starts”[All Fields])) AND “nursing homes”[Title/Abstract])) |
| Translations Inappropriate: “inappropriate”[All Fields] OR “inappropriately”[All Fields] OR “inappropriateness”[All Fields] STOPP: “potentially inappropriate medication list”[MeSH Terms] OR (“potentially”[All Fields] AND “inappropriate”[All Fields] AND “medication”[All Fields] AND “list”[All Fields]) OR “potentially inappropriate medication list”[All Fields] OR “stopp”[All Fields] INAPPROPRIATE: “inappropriate”[All Fields] OR “inappropriately”[All Fields] OR “inappropriateness”[All Fields] START: “start”[All Fields] OR “started”[All Fields] OR “starting”[All Fields] OR “starts”[All Fields] |
| Item No | Recommendation | |
|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | ||
| Introduction | ||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses |
| Methods | ||
| Study design | 4 | Present key elements of study design early in the paper |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection |
| Participants | 6 | (a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the rationale for the choice of cases and controls Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants |
| (b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed Case-control study—For matched studies, give matching criteria and the number of controls per case | ||
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable |
| Data sources/ measurement | 8 | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group |
| Bias | 9 | Describe any efforts to address potential sources of bias |
| Study size | 10 | Explain how the study size was arrived at |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding |
| (b) Describe any methods used to examine subgroups and interactions | ||
| (c) Explain how missing data were addressed | ||
| (d) Cohort study—If applicable, explain how loss to follow-up was addressed Case-control study—If applicable, explain how matching of cases and controls was addressed Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy | ||
| (e) Describe any sensitivity analyses | ||
| Results | ||
| Participants | 13 | (a) Report numbers of individuals at each stage of study—e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed |
| (b) Give reasons for non-participation at each stage | ||
| (c) Consider use of a flow diagram | ||
| Descriptive data | 14 | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders |
| (b) Indicate number of participants with missing data for each variable of interest | ||
| (c) Cohort study—Summarise follow-up time (e.g., average and total amount) | ||
| Outcome data | 15 | Cohort study—Report numbers of outcome events or summary measures over time |
| Case-control study—Report numbers in each exposure category, or summary measures of exposure | ||
| Cross-sectional study—Report numbers of outcome events or summary measures | ||
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included |
| (b) Report category boundaries when continuous variables were categorized | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | ||
| Other analyses | 17 | Report other analyses done—e.g., analyses of subgroups and interactions, and sensitivity analyses |
| Discussion | ||
| Key results | 18 | Summarise key results with reference to study objectives |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results |
| Other information | ||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based |
| STROBE Item Number | COR/ Quality | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | ||
| Aneys et al. (2018) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 18/22 (82%) High | ||||
| Carvalho et al. (2019) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 17/22 (81%) High | |||||
| Díaz et al. (2021) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 17/22 (77%) High | |||||
| Eshetie et al. (2020) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 16/22 (73%) Moderate | ||||||
| García-Caballero el al (2018) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 15/22 (68%) Moderate | ||||||
| Gaubert et al. (2019) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 18/22 (82%) High | ||||
| Gutiérrez- Valencia et al. (2018) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 15/22 (68%) Moderate | ||||||
| Liew et al. (2019) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 17/22 (77%) High | |||||
| Monteiro et al. (2020) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 15/22 (68%) Moderate | |||||||
| Nieves-Pérez et al. (2018) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 15/22 (68%) Moderate | |||||||
| Perulero et al. (2016) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 15/22 (68%) Moderate | |||||||
| Stojanovic et al. (2020) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 18/22 (82%) High | ||||
| Quality Assessment | Nº of Patients | Effect | Quality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Nº of Studies | Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Intervention | Control | Relative (95%CI) | Absolute | |
| Strauven (2019). Interdisciplinary case conferences for nursing home staff vs. usual care | ||||||||||
| 1 | CRCT | Serious risk of bias NHs that applied freely were included and high number of missing data) | No Serious inconsistency | No Serious indirectness | Serious imprecision (very wide range of results) | 847 | 957 | Effect in favor of the intervention: (odds ratio 1.479 [95% CI 1.062–2.059, P = 0.021]). | Moderate +++/++++ | |
References
- Organización Mundial de la Salud. Informe Mundial Sobre El Envejecimiento y La Salud; OMS: Geneva, Switzerland, 2015. [Google Scholar]
- Salech, F.; Daniel Palma, Q.F.; Pablo Garrido, Q.F. Epidemiología del uso de medicamentos en el adulto mayor. Rev. Médica Clínica Las Condes 2016, 27, 660–670. [Google Scholar] [CrossRef]
- Pérez Díaz, J.; Abellán García, A.; Aceituno Nieto, P.; Ramiro Fariñas, D. Un Perfil de Las Personas Mayores En España, 2020. Indicadores Estadísticos Básicos; Informes Envejecimiento en red: Madrid, Spain, 2020; Volume 25, 38p. [Google Scholar]
- Bo, M.; Gibello, M.; Brunetti, E.; Boietti, E.; Sappa, M.; Falcone, Y.; Aurucci, M.L.; Iacovino, M.; Fonte, G.; Cappa, G. Prevalence and Predictors of Inappropriate Prescribing According to the Screening Tool of Older People’s Prescriptions and Screening Tool to Alert to Right Treatment Version 2 Criteria in Older Patients Discharged from Geriatric and Internal Medicine Ward. Geriatr. Gerontol. Int. 2019, 19, 5–11. [Google Scholar] [CrossRef] [PubMed]
- De, G.; Lozano Montoya, D.I. Buena Práctica Clínica En GERIATRÍA Presidente de La Sociedad Española de Geriatría y Gerontología (SEGG); Sociedad Española de Geriatría y Gerontología: Madrid, Spain, 2015. [Google Scholar]
- Parodi López, N.; Villán Villán, Y.F.; Granados Menéndez, M.I.; Royuela, A. Prescripción Potencialmente Inapropiada En Mayores de 65 Años En Un Centro de Salud de Atención Primaria. Atención Primaria 2014, 46, 290–297. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, D.P.; O’Mahony, D.; Parsons, C.; Hughes, C.; Murphy, K.; Patterson, S.; Byrne, S. A Prevalence Study of Potentially Inappropriate Prescribing in Irish Long-Term Care Residents. Drugs Aging 2013, 30, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Riordan, D.O.; Aubert, C.E.; Walsh, K.A.; Van Dorland, A.; Rodondi, N.; Du Puy, R.S.; Poortvliet, R.K.E.; Gussekloo, J.; Sinnott, C.; Byrne, S.; et al. Prevalence of Potentially Inappropriate Prescribing in a Subpopulation of Older European Clinical Trial Participants: A Cross-Sectional Study. BMJ Open 2018, 8, e019003. [Google Scholar] [CrossRef]
- Hill-Taylor, B.; Sketris, I.; Hayden, J.; Byrne, S.; O’Sullivan, D.; Christie, R. Application of the STOPP/START Criteria: A Systematic Review of the Prevalence of Potentially Inappropriate Prescribing in Older Adults, and Evidence of Clinical, Humanistic and Economic Impact. J. Clin. Pharm. Ther. 2013, 38, 360–372. [Google Scholar] [CrossRef]
- Delgado Silveira, E.; Muñoz García, M.; Montero Errasquin, B.; Sánchez Castellano, C.; Gallagher, P.F.; Cruz-Jentoft, A.J. Prescripción Inapropiada de Medicamentos En Los Pacientes Mayores: Los Criterios STOPP/START. Rev. Esp. Geriatr. Gerontol. 2009, 44, 273–279. [Google Scholar] [CrossRef]
- Gallo, C.; Vilosio, J.; Saimovici, J. Actualización de Los Criterios STOPP-START: Una Herramienta Para La Detección de Medicación Potencialmente Inadecuada En Ancianos New Version of STOPP-START Criteria: Tools for the Detection of Potentially Inappropriate Medications in the Elderly. Evidencia. Actual. En La Práctica Ambulatoria 2015, 18, 124–129. [Google Scholar]
- Tommelein, E.; Mehuys, E.; Petrovic, M.; Somers, A.; Colin, P.; Boussery, K. Potentially Inappropriate Prescribing in Community-Dwelling Older People across Europe: A Systematic Literature Review. Eur. J. Clin. Pharmacol. 2015, 71, 1415–1427. [Google Scholar] [CrossRef]
- Storms, H.; Marquet, K.; Aertgeerts, B.; Claes, N. Prevalence of Inappropriate Medication Use in Residential Long-Term Care Facilities for the Elderly: A Systematic Review. Eur. J. Gen. Pract. 2017, 23, 69–77. [Google Scholar] [CrossRef]
- Morin, L.; Laroche, M.L.; Texier, G.; Johnell, K. Prevalence of Potentially Inappropriate Medication Use in Older Adults Living in Nursing Homes: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 862.e1–862.e9. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, H.; Darvishi, N.; Salari, N.; Hosseinian-Far, A.; Akbari, H.; Mohammadi, M. Global Prevalence of Polypharmacy among the COVID-19 Patients: A Comprehensive Systematic Review and Meta-Analysis of Observational Studies. Trop. Med. Health 2022, 50, 60. [Google Scholar] [CrossRef]
- Liew, T.M.; Lee, C.S.; Shawn, K.L.G.; Chang, Z.Y. Potentially Inappropriate Prescribing Among Older Persons: A Meta-Analysis of Observational Studies. Ann. Fam. Med. 2019, 17, 257–266. [Google Scholar] [CrossRef]
- Puche Cañas, E.; Luna del Castillo, J.D. Reacciones adversas a medicamentos en pacientes que acudieron a un hospital general: Un meta-análisis de resultados. Ann. Med. Interna 2007, 24, 574–578. [Google Scholar] [CrossRef]
- Cahir, C.; Fahey, T.; Teeling, M.; Teljeur, C.; Feely, J.; Bennett, K. Potentially Inappropriate Prescribing and Cost Outcomes for Older People: A National Population Study. Br. J. Clin. Pharmacol. 2010, 69, 543–552. [Google Scholar] [CrossRef]
- Moriarty, F.; Hardy, C.; Bennett, K.; Smith, S.M.; Fahey, T. Trends and Interaction of Polypharmacy and Potentially Inappropriate Prescribing in Primary Care over 15 Years in Ireland: A Repeated Cross-Sectional Study. BMJ Open 2015, 5, e008656. [Google Scholar] [CrossRef]
- Beers, M.H.; Ouslander, J.G.; Rollingher, I.; Reuben, D.B.; Brooks, J.; Beck, J.C. Explicit Criteria for Determining Inappropriate Medication Use in Nursing Home Residents. Arch. Intern. Med. 1991, 151, 1825. [Google Scholar] [CrossRef]
- Gallagher, P.; Ryan, C.; Byrne, S.; Kennedy, J.; O Mahony, D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert Doctors to Right Treatment). Consensus Validation. Int. J. Clin. Pharmacol. Ther. 2008, 46, 72–83. [Google Scholar] [CrossRef]
- Bahat, G.; Bay, I.; Tufan, A.; Tufan, F.; Kilic, C.; Karan, M.A. Prevalence of Potentially Inappropriate Prescribing among Older Adults: A Comparison of the Beers 2012 and Screening Tool of Older Person’s Prescriptions Criteria Version 2. Geriatr. Gerontol. Int. 2017, 17, 1245–1251. [Google Scholar] [CrossRef]
- Ubeda, A.; Ferrándiz, L.; Maicas, N.; Gomez, C.; Bonet, M.; Peris, J.E. Potentially Inappropriate Prescribing in Institutionalised Older Patients in Spain: The STOPP-START Criteria Compared with the Beers Criteria. Pharm. Pract. 2012, 10, 83–91. [Google Scholar] [CrossRef]
- Reeve, E.; Shakib, S.; Hendrix, I.; Roberts, M.S.; Wiese, M.D. The Benefits and Harms of Deprescribing. Med. J. Aust. 2014, 201, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Frankenthal, D.; Lerman, Y.; Kalendaryev, E.; Lerman, Y. Intervention with the Screening Tool of Older Persons Potentially Inappropriate Prescriptions/Screening Tool to Alert Doctors to Right Treatment Criteria in Elderly Residents of a Chronic Geriatric Facility: A Randomized Clinical Trial. J. Am. Geriatr. Soc. 2014, 62, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Khodyakov, D.; Ochoa, A.; Olivieri-Mui, B.L.; Bouwmeester, C.; Zarowitz, B.J.; Patel, M.; Ching, D.; Briesacher, B. STOPP/START Medication Criteria Modified for US Nursing Home Setting. J. Am. Geriatr. Soc. 2017, 65, 586. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START Criteria for Potentially Inappropriate Prescribing in Older People: Version 2. Age Ageing 2014, 44, 213–218. [Google Scholar] [CrossRef]
- Delgado Silveira, E.; Montero Errasquín, B.; Muñoz García, M.; Vélez-Díaz-Pallarés, M.; Lozano Montoya, I.; Sánchez-Castellano, C.; Cruz-Jentoft, A.J. Mejorando La Prescripción de Medicamentos En Las Personas Mayores: Una Nueva Edición de Los Criterios STOPP-START. Rev. Esp. Geriatr. Gerontol. 2015, 50, 89–96. [Google Scholar] [CrossRef]
- Moriarty, F.; Bennett, K.; Cahir, C.; Kenny, R.A.; Fahey, T. Potentially Inappropriate Prescribing According to STOPP and START and Adverse Outcomes in Community-Dwelling Older People: A Prospective Cohort Study. Br. J. Clin. Pharmacol. 2016, 82, 849–857. [Google Scholar] [CrossRef]
- Sevilla-Sánchez, D.; Espaulella-Panicot, J.; de Andrés-Lazaro, A.M.; Torres-Allezpuz, R.; Soldevila-Llagostera, M.; Codina-Jane, C. Medicación Potencialmente Inapropiada Al Ingreso En Una Unidad de Media Estancia Según Los Criterios STOPP & START. Rev. Esp. Geriatr. Gerontol. 2012, 47, 155–157. [Google Scholar] [CrossRef]
- Cruz-Esteve, I.; Marsal-Mora, J.R.; Galindo-Ortego, G.; Galván-Santiago, L.; Serrano-Godoy, M.; Ribes-Murillo, E.; Real-Gatius, J. Análisis Poblacional de La Prescripción Potencialmente Inadecuada En Ancianos Según Criterios STOPP/START (Estudio STARTREC). Atención Primaria 2016, 49, 166–176. [Google Scholar] [CrossRef]
- San-José, A.; Agustí, A.; Vidal, X.; Formiga, F.; Gómez-Hernández, M.; García, J.; López-Soto, A.; Ramírez-Duque, N.; Torres, O.H.; Barbé, J. Inappropriate Prescribing to the Oldest Old Patients Admitted to Hospital: Prevalence, Most Frequently Used Medicines, and Associated Factors. BMC Geriatr. 2015, 15, 42. [Google Scholar] [CrossRef]
- Tosato, M.; Landi, F.; Martone, A.M.; Cherubini, A.; Corsonello, A.; Volpato, S.; Bernabei, R.; Onder, G. Potentially Inappropriate Drug Use among Hospitalised Older Adults: Results from the CRIME Study. Age Ageing 2014, 43, 767–773. [Google Scholar] [CrossRef]
- Fialová, D.; Laffon, B.; Marinković, V.; Tasić, L.; Doro, P.; Sόos, G.; Mota, J.; Dogan, S.; Brkić, J.; Teixeira, J.P.; et al. Medication Use in Older Patients and Age-Blind Approach: Narrative Literature Review (Insufficient Evidence on the Efficacy and Safety of Drugs in Older Age, Frequent Use of PIMs and Polypharmacy, and Underuse of Highly Beneficial Nonpharmacological Strategies). Eur. J. Clin. Pharmacol. 2019, 75, 451–466. [Google Scholar] [CrossRef] [Green Version]
- Hill-Taylor, B.; Walsh, K.A.; Stewart, S.; Hayden, J.; Byrne, S.; Sketris, I.S. Effectiveness of the STOPP/START (Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions/Screening Tool to Alert Doctors to the Right Treatment) Criteria: Systematic Review and Meta-Analysis of Randomized Controlled Studies. J. Clin. Pharm. Ther. 2016, 41, 158–169. [Google Scholar] [CrossRef]
- Tian, F.; Chen, Z.; Zhou, D.; Mo, L. Prevalence of Polypharmacy and Potentially Inappropriate Medication Use in Older Lung Cancer Patients: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2022, 13, 1044885. [Google Scholar] [CrossRef]
- Atmaja, D.S.; Yulistiani; Suharjono; Zairina, E. Detection Tools for Prediction and Identification of Adverse Drug Reactions in Older Patients: A Systematic Review and Meta-Analysis. Sci. Rep. 2022, 12, 13189. [Google Scholar] [CrossRef]
- Lee, J.W.; Li, M.; Boyd, C.M.; Green, A.R.; Szanton, S.L. Preoperative Deprescribing for Medical Optimization of Older Adults Undergoing Surgery: A Systematic Review. J. Am. Med. Dir. Assoc. 2022, 23, 528–536.e2. [Google Scholar] [CrossRef]
- Alshammari, H.; Al-Saeed, E.; Ahmed, Z.; Aslanpour, Z. Reviewing Potentially Inappropriate Medication in Hospitalized Patients Over 65 Using Explicit Criteria: A Systematic Literature Review. Drug. Healthc. Patient Saf. 2021, 13, 183–210. [Google Scholar] [CrossRef]
- Mekonnen, A.B.; Redley, B.; de Courten, B.; Manias, E. Potentially Inappropriate Prescribing and Its Associations with Health-Related and System-Related Outcomes in Hospitalised Older Adults: A Systematic Review and Meta-Analysis. Br. J. Clin. Pharmacol. 2021, 87, 4150–4172. [Google Scholar] [CrossRef]
- Farhat, A.; Al-Hajje, A.; Csajka, C.; Panchaud, A. Clinical and Economic Impacts of Explicit Tools Detecting Prescribing Errors: A Systematic Review. J. Clin. Pharm. Ther. 2021, 46, 877–886. [Google Scholar] [CrossRef]
- Thomas, R.E.; Thomas, B.C. A Systematic Review of Studies of the STOPP/START 2015 and American Geriatric Society Beers 2015 Criteria in Patients ≥ 65 Years. Curr. Aging Sci. 2019, 12, 121–154. [Google Scholar] [CrossRef]
- Cooper, J.A.; Cadogan, C.A.; Patterson, S.M.; Kerse, N.; Bradley, M.C.; Ryan, C.; Hughes, C.M. Interventions to Improve the Appropriate Use of Polypharmacy in Older People: A Cochrane Systematic Review. BMJ Open 2015, 5, e009235. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, W-65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Suvarna, B.; Suvarna, A.; Phillips, R.; Juster, R.-P.; McDermott, B.; Sarnyai, Z. Health Risk Behaviours and Allostatic Load: A Systematic Review. Neurosci. Biobehav. Rev. 2020, 108, 694–711. [Google Scholar] [CrossRef] [PubMed]
- Osei, F.; Block, A.; Wippert, P.-M.; Qorbani, M.; Djalalinia, S.; Tabatabaei-Malazy, O. Association of Primary Allostatic Load Mediators and Metabolic Syndrome (MetS): A Systematic Review. Front. Endocrinol. 2022, 13, 946740. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H.; et al. GRADE Guidelines: 1. Introduction-GRADE Evidence Profiles and Summary of Findings Tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Díaz Planelles, I.; Saurí Ferrer, I.; Trillo-Mata, J.L.; Navarro-Pérez, J. Analysis of Potentially Inappropriate Prescriptions According to the START Criteria in Nursing Homes. Rev. Esp. Geriatr. Gerontol. 2021, 56, 195–202. [Google Scholar] [CrossRef]
- Gutiérrez-Valencia, M.; Izquierdo, M.; Lacalle-Fabo, E.; Marín-Epelde, I.; Ramón-Espinoza, M.F.; Domene-Domene, T.; Casas-Herrero, Á.; Galbete, A.; Martínez-Velilla, N. Relationship between Frailty, Polypharmacy, and Underprescription in Older Adults Living in Nursing Homes. Eur. J. Clin. Pharmacol. 2018, 74, 961–970. [Google Scholar] [CrossRef]
- García-Caballero, T.M.; Lojo, J.; Menéndez, C.; Fernández-Álvarez, R.; Mateos, R.; Garcia-Caballero, A. Polimedication: Applicability of a Computer Tool to Reduce Polypharmacy in Nursing Homes. Int. Psychogeriatr. 2018, 30, 1001–1008. [Google Scholar] [CrossRef]
- Perulero, M.L.M. Impacto de un programa de prescripción prudente en residentes de centros sociosanitarios. Pharm. Care Esp. 2016, 18, 154–167. [Google Scholar]
- Carvalho, R.; Lavrador, M.; Cabral, A.C.; Veríssimo, M.T.; Figueiredo, I.V.; Fernandez-Llimos, F.; Margarida Castel-Branco, M. Patients’ Clinical Information Requirements to Apply the STOPP/START Criteria. Int. J. Clin. Pharm. 2019, 41, 1562–1569. [Google Scholar] [CrossRef]
- Monteiro, C.; Canário, C.; Ribeiro, M.Â.; Duarte, A.P.; Alves, G. Medication Evaluation in Portuguese Elderly Patients According to Beers, STOPP/START Criteria and EU(7)-PIM List—An Exploratory Study. Patient Prefer. Adherence 2020, 14, 795. [Google Scholar] [CrossRef]
- Anrys, P.M.S.; Strauven, G.C.; Foulon, V.; Degryse, J.M.; Henrard, S.; Spinewine, A. Potentially Inappropriate Prescribing in Belgian Nursing Homes: Prevalence and Associated Factors. J. Am. Med. Dir. Assoc. 2018, 19, 884–890. [Google Scholar] [CrossRef]
- Strauven, G.; Anrys, P.; Vandael, E.; Henrard, S.; De Lepeleire, J.; Spinewine, A.; Foulon, V. Cluster-Controlled Trial of an Intervention to Improve Prescribing in Nursing Homes Study. J. Am. Med. Dir. Assoc. 2019, 20, 1404–1411. [Google Scholar] [CrossRef]
- Stojanović, M.; Vuković, M.; Jovanović, M.; Dimitrijević, S.; Radenković, M. GheOP3S Tool and START/STOPP Criteria Version 2 for Screening of Potentially Inappropriate Medications and Omissions in Nursing Home Residents. J. Eval. Clin. Pract. 2019, 26, 158–164. [Google Scholar] [CrossRef]
- Gaubert-Dahan, M.-L.; Sebouai, A.; Tourid, W.; Fauvelle, F.; Aikpa, R.; Bonnet-Zamponi, D. The Impact of Medication Review with Version 2 STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert Doctors to Right Treatment) Criteria in a French Nursing Home: A 3-Month Follow-up Study. Ther. Adv. Drug Saf. 2019, 10, 2042098619855535. [Google Scholar] [CrossRef]
- Nieves-Pérez, B.F.; Hostos, S.G.-D.; Frontera-Hernández, M.I.; González, I.C.; Muñoz, J.J.H. Potentially Inappropriate Medication Use Among Institutionalized Older Adults at Nursing Homes in Puerto Rico. Consult. Pharm. 2018, 33, 619–636. [Google Scholar] [CrossRef]
- Eshetie, T.C.; Roberts, G.; Nguyen, T.A.; Gillam, M.H.; Maher, D.; Ellett, L.M.K. Potentially Inappropriate Medication Use and Related Hospital Admissions in Aged Care Residents: The Impact of Dementia. Br. J. Clin. Pharmacol. 2020, 86, 2414–2423. [Google Scholar] [CrossRef]
- Liew, N.Y.; Chong, Y.Y.; Yeow, S.H.; Kua, K.P.; Saw, P.S.; Lee, S.W.H. Prevalence of Potentially Inappropriate Medications among Geriatric Residents in Nursing Care Homes in Malaysia: A Cross-Sectional Study. Int. J. Clin. Pharm. 2019, 41, 895–902. [Google Scholar] [CrossRef]
- Anrys, P.; Strauven, G.; Boland, B.; Dalleur, O.; Declercq, A.; Degryse, J.-M.; De Lepeleire, J.; Henrard, S.; Lacour, V.; Simoens, S.; et al. Collaborative Approach to Optimise MEdication Use for Older People in Nursing Homes (COME-ON): Study Protocol of a Cluster Controlled Trial. Implement. Sci. 2016, 11, 35. [Google Scholar] [CrossRef]
- O’Mahony, D. STOPP/START Criteria for Potentially Inappropriate Medications/Potential Prescribing Omissions in Older People: Origin and Progress. Expert Rev. Clin. Pharmacol. 2020, 13, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Hernandez Martin, J.; Merino-Sanjuán, V.; Peris-Martí, J.; Correa-Ballester, M.; Vial-Escolano, R.; Merino-Sanjuán, M. Applicability of the STOPP/START Criteria to Older Polypathological Patients in a Long-Term Care Hospital. Eur. J. Hosp. Pharm. 2018, 25, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Díez, R.; Cadenas, R.; Susperregui, J.; Sahagún, A.M.; Fernández, N.; García, J.J.; Sierra, M.; López, C. Drug-Related Problems and Polypharmacy in Nursing Home Residents: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 4313. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The Global Epidemiology of Hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Inzitari, M.; Merino Méndez, R.; Santaeugenia, S.; Pascual Arce, B.; Montero Leno, A.; Sunyer, B.; López, S.A.C. Prescripción Potencialmente Inadecuadas En Dos Centros Sociosanitarios Según Los Criterios START-STOPP. Available online: https://aquas.gencat.cat/web/.content/minisite/aquas/publicacions/2017/prescripcion_sociosanitarios_START-STOPP_Red_aquas2017.pdf (accessed on 21 July 2020).
- Primejdie, D.P.; Bojita, M.T.; Popa, A. Potentially Inappropriate Medications in Elderly Ambulatory and Institutionalized Patients: An Observational Study. BMC Pharmacol. Toxicol. 2016, 17, 38. [Google Scholar] [CrossRef]
- Awad, A.; Hanna, O. Potentially Inappropriate Medication Use among Geriatric Patients in Primary Care Setting: A Cross-Sectional Study Using the Beers, STOPP, FORTA and MAI Criteria. PLoS ONE 2019, 14, e0218174. [Google Scholar] [CrossRef]
- Rivas-Cobas, P.C.; Ramírez-Duque, N.; Gómez Hernández, M.; García, J.; Agustí, A.; Vidal, X.; Formiga, F.; López-Soto, A.; Torres, O.H.; San-José, A. Características Del Uso Inadecuado de Medicamentos En Pacientes Pluripatológicos de Edad Avanzada. Gac. Sanit. 2017, 31, 327–331. [Google Scholar] [CrossRef]
- Blanco-Reina, E.; Ariza-Zafra, G.; Ocaña-Riola, R.; León-Ortiz, M. 2012 American Geriatrics Society Beers Criteria: Enhanced Applicability for Detecting Potentially Inappropriate Medications in European Older Adults? A Comparison with the Screening Tool of Older Person’s Potentially Inappropriate Prescriptions. J. Am. Geriatr. Soc. 2014, 62, 1217–1223. [Google Scholar] [CrossRef]
- Ruiz-Millo, O.; Climente-Martí, M.; Navarro-Sanz, J.R. Improvement on Prescribing Appropriateness after Implementing an Interdisciplinary Pharmacotherapy Quality Programme in a Long-Term Care Hospital. Eur. J. Hosp. Pharm. 2018, 25, 267–273. [Google Scholar] [CrossRef]
- Renom-Guiteras, A.; Thürmann, P.A.; Miralles, R.; Klaaßen-Mielke, R.; Thiem, U.; Stephan, A.; Bleijlevens, M.H.C.; Jolley, D.; Leino-Kilpi, H.; Hallberg, I.R.; et al. Potentially Inappropriate Medication among People with Dementia in Eight European Countries. Age Ageing 2018, 47, 68–74. [Google Scholar] [CrossRef]
- Lind, K.E.; Raban, M.Z.; Georgiou, A.; Westbrook, J.I. NSAID Use among Residents in 68 Residential Aged Care Facilities 2014 to 2017: An Analysis of Duration, Concomitant Medication Use, and High-Risk Conditions. Pharmacoepidemiol. Drug Saf. 2019, 28, 1480–1488. [Google Scholar] [CrossRef]
- Wright, D.J.; Maskrey, V.; Blyth, A.; Norris, N.; Alldred, D.P.; Bond, C.M.; Desborough, J.; Hughes, C.M.; Holland, R.C. Systematic Review and Narrative Synthesis of Pharmacist Provided Medicines Optimisation Services in Care Homes for Older People to Inform the Development of a Generic Training or Accreditation Process. Int. J. Pharm. Pract. 2020, 28, 207–219. [Google Scholar] [CrossRef] [Green Version]

| Characteristics of the Studies | Results Related to PIPs |
|---|---|
| Author (year; country) | Prevalence of PIPs according to STOPP/START criteria |
| Residents (% of women) | Number of STOPP criteria calculated |
| Number of NH | Number of PIPs detected according to STOPP criteria |
| Data collection method | Prevalence of PIPs according to STOPP criteria |
| Study design | Average PIPs detected according to STOPP |
| Inclusion criteria | Number of START criteria calculated |
| Patient age | Number of PIPs detected according START criteria |
| Number of drugs prescribed | Average PIPs detected according to START |
| Most prevalent diagnoses | Prevalence of PIPs according to START criteria |
| Risk factors associated with PIPs |
| Author (Year)/ Country | Residents n (% Women) | NH (n) | Data Collection Method (Period of Study) | Study Design | Inclusion Criteria | Age Average (SD/Range) | Average No. of Drugs | Diagnosis n (%) | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| Carvalho et al. (2019)/ Portugal [54] | 208 (68.75%) | 4 | Electronic records (NS) | Descriptive study cross-sectional | >65 y | 87 (10) | 8 (5) | NS | High |
| Stojanovic et al. (2020)/ Serbia [58] | 400 (69%) | 1 | Review of medical records at the patient’s first visit (January-June 2018) | Retrospective observational study | >65 y At least 1 chronic prescription drug | 83 (11) | 8 (5) | Arterial hypertension: 358 (89.5) Angina pectoris: 181 (45.2) Dementia: 151 (37.7) Depression: 135 (33.7) Psychosis: 133 (33.2) Sleep disorders: 124 (31) Heart failure: 105 (26.2) COPD: 68 (17) Infarction: 631 (15.7) Anxiety: 57 (14.2) Osteoporosis: 45 (11.2) | High |
| Anrys et al. (2018)/ Belgium [56] | 1410 (72%) | 54 | Data extracted from the COME-ON multicenter study (April 2015-June 2016) | Cross-sectional descriptive study | ≥65 y Patients not in palliative care | 87 (82–91) | 9 (6–12) | NS | High |
| Liew et al. (2019)/ Malaysia [62] | 155 (44.5%) | 4 | Data collected manually by patient interview (November–December 2016) | Cross-sectional multicenter study | ≥60 y At least 1 prescribed drug Exclusion: residents unable to sign informed consent form | 75 (8.49) | Total drugs: 3.52 (3.07) Chronic drugs: 2.69 (2.49) | Cardiovascular disease: 102 (65.8) Endocrine disease: 56 (36.1) Respiratory disease: 17 (11) Gastrointestinal disease: 15 (9.7) | High |
| Gaubert et al. (2019)/ France [59] | 52 (83%) | 1 | Electronic records (January–March 2015) | Prospective observational study | All residents of the socio-health center | 84 (9) | 8.5 (3.5) | Depression: 37 (71) Dementia: 33 (63) Chronic constipation: 33 (63) Hypertension: 29 (56) Osteoporosis: 18 (35) Osteoarthritis: 12 (23) | High |
| Díaz et al. (2021)/ Spain [50] | 2251 (69%) | 13 | Electronic records (2016–2018) | Retrospective observational descriptive study | All residents of the socio-health center | 79.5 (78.3–80.4) | Total drugs: 6.30 (6.0–6.4) Chronic drugs: 4.5 (4.4–4.7) | Alzheimer’s disease: NS Gastroesophageal reflux: NS Severe anxiety: NS Cerebral vascular disease: NS COPD: NS Chronic atrial fibrillation: NS | High |
| Nieves-Pérez et al. (2018)/ Puerto Rico [60] | 104 (72%) | 3 | Electronic records (NS) | Cross-sectional descriptive study | ≥65 y At least 1 prescribed drug 1 or more chronic diseases and data in the electronic medical record | 84 (7.67) | 8.6 (3.41) | NS | Moderate |
| Monteiro et al. (2020)/ Portugal [55] | 90 (78.9%) | 1 | Electronic records (NS) | Cross-sectional descriptive study | ≥65 y | 84 (65–103) | 7.6 (NS) <5 drugs: 26 rs 5–9 drugs: 30 rs ≥10 drugs: 33 rs | Diseases of the cardiovascular system: 72 (80) Endocrine and metabolic system diseases: 46 (51) Mental disease: 43 (47.8) Diseases of the musculoskeletal system: 32 (35.5) | Moderate |
| Gutiérrez-Valencia et al. (2018)/ Spain [51] | 110 (71.8%) | 2 | Data obtained from electronic records, subsequently anonymized, encoded and stored for further analysis (NS) | Cross-sectional cohort study | ≥65 y | 86.3 (7.3) | NS 5–9 drugs: 81 rs <5 drugs: 29 rs | NS | Moderate |
| García-Caballero et al. (2018)/ Spain [52] | 115 (61.74%) | 1 | Data collected manually and subsequently entered into an Excel created to detect PIP (NS) | Feasibility study | All residents of the socio-health center | 79 (11.44; 46–102) | 6.77 (2.92) | NS | Moderate |
| Perulero et al. (2016)/ Spain [53] | 332 (NS) | 2 | Individualized information was collected for each patient (March–May 2015) | Prospective observational study | ≥65 y | 83.9 (7.6) | 8.7 (4) ≥10 drugs: 39.5% rs | NS | Moderate |
| Strauven et al. (2019)/Belgium [57] | 1507 Intervention group: 791 (69.9%) Control group: 716 (73.4%) | 54 | Data from a web site created for data collection and filled in by the study investigators (Intervention period: May 2015 to June 2016) | Randomized blinded study (multicenter). | ≥65 y Patients without palliative care | Intervention group: 87 (82–91) Control group: 87 (83–91) | Intervention group: 9 (6–12) Control group: 9 (6–11) | Intervention group: Hypertension (56) Dementia (59.2) Osteoarthritis (63.3) Control group: Hypertension (56.1) Dementia (54.2) Osteoarthritis (66.2) | Moderate |
| Eshetie et al. (2020)/ Australia [61] | 181 (54.7%) | NS | Manually collected data (June–July 2017) | Prospective multicenter observational study | ≥ 75 y ≥5 drugs prescribed prior to admission to the hospital | With dementia: 88.4 (83–92) Without dementia: 87 (82–91) | ADMISSION: With dementia Total drugs: 9.5 (3.5) Chronic drugs: 8.8 (3.2) Without Dementia Total drugs: 11 (3.4) Chronic Drugs: 10 (3.2) | ADMISSION: Pneumonia/lower respiratory tract infection: 45 (24.9) Falls: 25 (13.8) Cardiovascular problems: 21 (11.6) | Moderate |
| Author (Year)/ Country | Prevalence of PIPs According to STOPP/ START Criteria | No. of Criteria Calculated STOPP | PIPs Detected According to STOPP Criteria | Average PIPs Detected According to STOPP | Prevalence of PIPs (STOPP Criteria) | No. of Criteria Calculated START | PIPs Detected According to START Criteria | Average PIPs Detected According to START | Prevalence of PIPs (START Criteria) | Risk Factors Associated with PIPs |
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | (n) | n (%) | Mean (SD; Range) | n (%) | (n) | n (%) | Mean (SD; Range) | n (%) | ||
| Carvalho et al. (2019)/ Portugal [54] | NS | 29 | 529 (32.5) Most prevalent criteria: STOPP K1: 134 STOPP K2: 99 | NS | NS | 1 | NS | NS | NS | NS |
| Stojanovic et al. (2020)/ Serbia [58] | NS | All | 841 (NS) Most prevalent section: STOPP K: 448 (53.1) STOPP D: 357 (42.3) | NS | 344 (86) Most prevalent criteria: STOPP K1: 253 (NS) STOPP D5: 207 (NS) Neuroleptics: 152 (NS) STOPP D6: 100 (NS) | All | 1067 (NS) Most prevalent section: START I: 627 (52.4) START A: 318 (26.5) | NS | 399 (99.7) Most prevalent criteria: START I1: 399 (NS) START I2: 228 (NS) START A3: 99 (NS) | STOPP Age (ρ = 0.17; p = 0.02) Prescribed drugs (ρ = 0.17; p = 0.003) START Age (ρ = 0.10; p = 0.02) Prescribed drugs (ρ = 0.17; p = 0.0005) Number of diagnoses (ρ = 0.40; p < 0.0001) CCI (ρ = 0.31; p ≤ 0.0001) MCI (ρ = 0.35; p < 0.0001) |
| Anrys et al. (2018)/ Belgium [56] | NS | 76 | NS Most prevalent criteria: STOPP K1:659 (46.7) STOPP D5: 644 (45.7) STOPP K2: 417 (29.6) STOPP I1: 190 (13.5) STOPP D9: 184 (13.0) | 2 (NS) | NS | 31 | NS Most prevalent criteria: START E5: 726 (51.5) START A3: 303 (21.5) START E4: 295 (20.9) START G3: 221 (15.7) START A6:196 (13.9) START E3: 191 (13.5) | 2 (NS) | 1199 (85) | STOPP Number of drugs: 5–9 (RR = 2.29; CI: 1.23–2.75); p < 0.01 ≥10 (RR = 4.27; CI: 3.60–5.11); p < 0.01 Comorbidities START Age: >85 (RR = 1.21; CI: 1.02–1.44); p = 0.029 Comorbidity: CIRS g ≥ 17 (RR = 1.81; CI: 1.58–2.06); p < 0.01 Dependence: Katz Index ≥ 20 (RR = 1.34; CI: 1.16–1.54); p < 0.01 |
| Liew et al. (2019)/ Malaysia [62] | NS | NS | NS Most prevalent criteria: STOPP D: 8 (40) STOPP J: 4 (20) STOPP F: 4 (20) | 1.23 (0.44) | 16 (9.7) | NS | NS | NS | NS | Polypharmacy (OR: 4.81; CI 95%: 2.31–10) p < 0.001 |
| Gaubert et al. (2019)/ France [59] | NS | NS | NS | 2 (1.4; 0–6) | 45 (86.5) Most prevalent criteria: STOPP A2: 33 (63) STOPP A1: 26 (50) STOPP A3: 18 (35) | NS | NS | 0.7 (0.6; 0–2) | 30 (57.7) Most prevalent criteria: START E5: 28 (54) START A4: 3 (6) | NS |
| Díaz et al. (2021)/ Spain [50] | NS | NS | NS | NS | NS | 18 | 2647 (NS) | NS | 1765 (39.54) Most prevalent criteria: START E2: NS (94.4) START E7: NS (87.5) START H2: NS(88.6) START A5: NS(84.0) START A6: NS(89.6) | NS |
| Nieves-Pérez et al. (2018)/ Puerto Rico [60] | NS | NS | 417 (NS) | NS | 91 (87.5) Most prevalent criteria: STOPP A1: 82 (NS) STOPP K1: 42 (NS) STOPP D5: 41 (NS) STOPP D9: 27 (NS) STOPP K2: 26 (NS) STOPP A3: 17 (NS) | NS | 162 (NS) | NS | 89 (85.58) Most prevalent criteria: START A3: 53 (NS) START E5: 49 (NS) START A5: 14 (NS) | NS |
| Monteiro et al. (2020)/ Portugal [55] | NS | NS | 250 (NS) | NS | 77 (85.5) Most prevalent criteria: STOPP A2: 58 (NS) STOPP D5: 54 (NS) STOPP K1: 54 (NS) STOPP K2: 28 (NS) STOPP A3: 12 (NS) | NS | 68 (NS) | NS | 52 (57.7) Most prevalent criteria: START I1: 36 (NS) START E4 and A3: 8 (NS) | NS |
| Gutiérrez-Valencia et al. (2018)/ Spain [51] | NS | NS | NS | NS | NS | NS | NS | Frail participants: 1.9 (NS) Non-frail participants: 1 (NS) | Frail participants: NS (87.5) Non-frail participants: NS (50) OR: 7.00 (CI 95%: 1.3–36.6) Most prevalent criteria: START E4: 26 (23.6) START E3: 21 (19.1) START A6: 10 (9.1) START A8: 10 (9.1) | NS |
| García-Caballero et al. (2018)/ Spain [52] | NS | NS | 1155 (NS) | 10 (NS) | NS (67.83) | NS | NS | NS | NS | Drugs associated with a greater number of PIP: Neuroleptics: 41.48% Benzodiazepines: 16.48% diuretics: 10.80% anticholinergics: 7.95% antihistamines: 5.68 |
| Perulero et al. (2016)/ Spain [53] | 233 (70.18) | NS | NS | NS | NS Most prevalent criteria: STOPP A1: 111 (29.2) STOPP D5: 110 (28.9) STOPP A2: 46 (21.1) STOPP C1: 35 (9.2) | NS | 10 (NS) | NS | NS | NS |
| Strauven et al. (2019)/ Belgium [57] | NS | NS | NS | NS | NS Most prevalent criteria in intervention group: STOPP K1: NS (54.3) STOPP D5: NS (53.9) STOPP K2: NS (37.2) STOPP I1: NS (14.5) STOPP D9: NS (12.9) Most prevalent criteria in control group: STOPP K1: NS (55.9) STOPP D5: NS (53.6) STOPP K2: NS (33.5) STOPP I1: NS (12.9) STOPP D9: NS (16.6) | NS | NS | Intervention group: 2 (1–3) Control group: 2 (1–3) | NS Most prevalent criteria in intervention group: START E5: NS (48.9) START A3: NS (14.1) START G3: NS (20.7) START E4: NS (27.2) START E3: NS (18.5) Most prevalent criteria in control group: START E5: NS (52.9) START A3: NS (21.9) START G3: NS (20.9) START E4: NS (19.8) START E3: NS (12.8) | NS |
| Eshetie et al. (2020)/ Australia [61] | NS | 62 | NS | Dementia: 2 (1–4) Non-dementia: 2 (1–4) | Dementia: 71 (78) Most prevalent criteria in dementia group: Use of drugs with anticholinergic properties: 32 (35.2) STOPP F2: 29 (31.9) STOPP K1: 16 (17.6) STOPP A3: 14 (15.4) STOPP B7: 13 (14.3) STOPP K2: 13 (14.3) Non-dementia 79 (87.8) Most prevalent criteria in non-dementia group: Use of drugs with anticholinergic properties: 22 (24.4) STOPP F2: 43 (47.8) STOPP B7: 23 (25.6) STOPP D5: 22 (24.4) STOPP L3: 16 (17.8) | NS | NS | NS | NS | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz Planelles, I.; Navarro-Tapia, E.; García-Algar, Ó.; Andreu-Fernández, V. Prevalence of Potentially Inappropriate Prescriptions According to the New STOPP/START Criteria in Nursing Homes: A Systematic Review. Healthcare 2023, 11, 422. https://doi.org/10.3390/healthcare11030422
Díaz Planelles I, Navarro-Tapia E, García-Algar Ó, Andreu-Fernández V. Prevalence of Potentially Inappropriate Prescriptions According to the New STOPP/START Criteria in Nursing Homes: A Systematic Review. Healthcare. 2023; 11(3):422. https://doi.org/10.3390/healthcare11030422
Chicago/Turabian StyleDíaz Planelles, Isabel, Elisabet Navarro-Tapia, Óscar García-Algar, and Vicente Andreu-Fernández. 2023. "Prevalence of Potentially Inappropriate Prescriptions According to the New STOPP/START Criteria in Nursing Homes: A Systematic Review" Healthcare 11, no. 3: 422. https://doi.org/10.3390/healthcare11030422