
Use of Ultrasound and Ki–67 Proliferation Index to Predict Breast Cancer Tumor Response to Neoadjuvant Endocrine Therapy
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
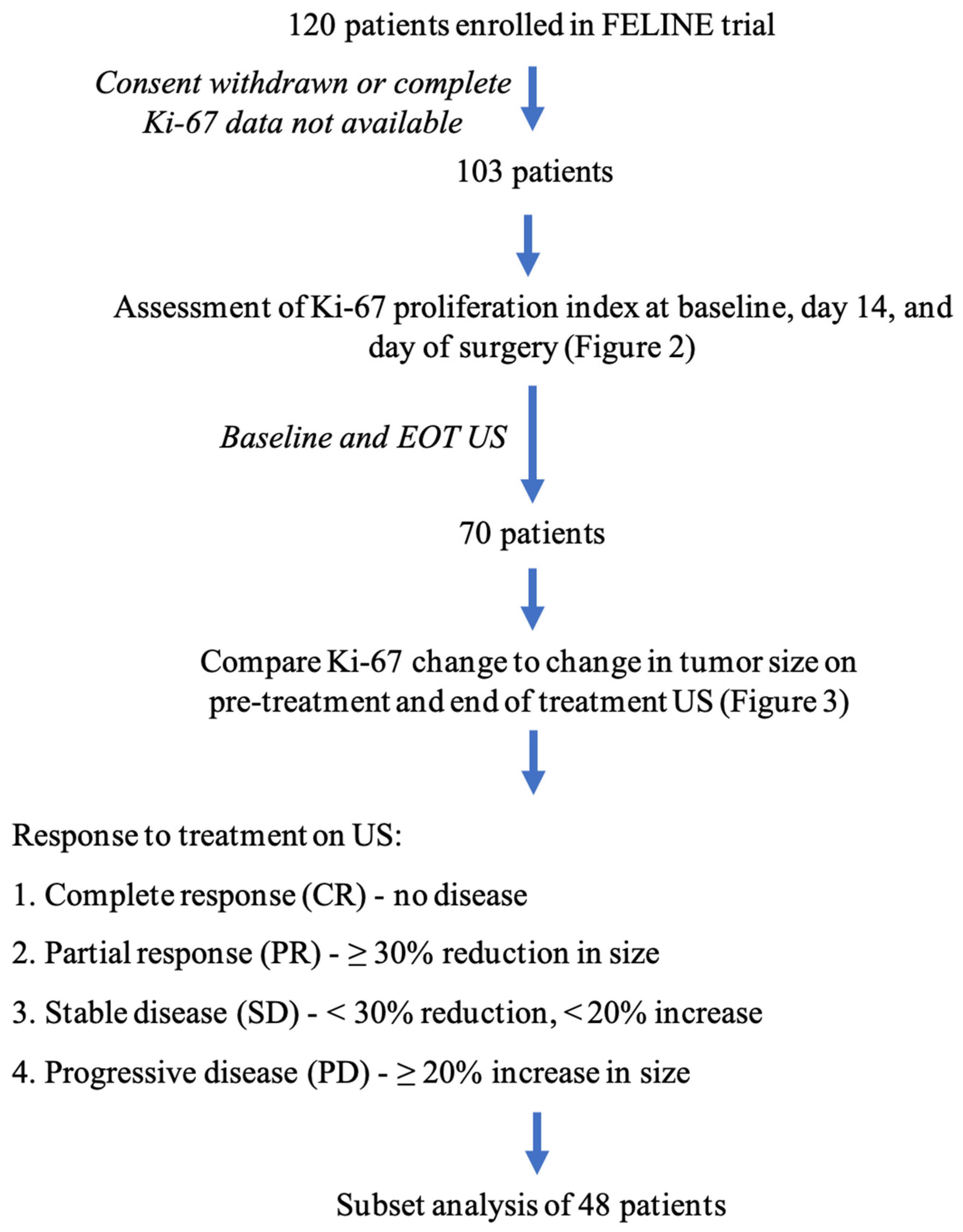
2. Methods
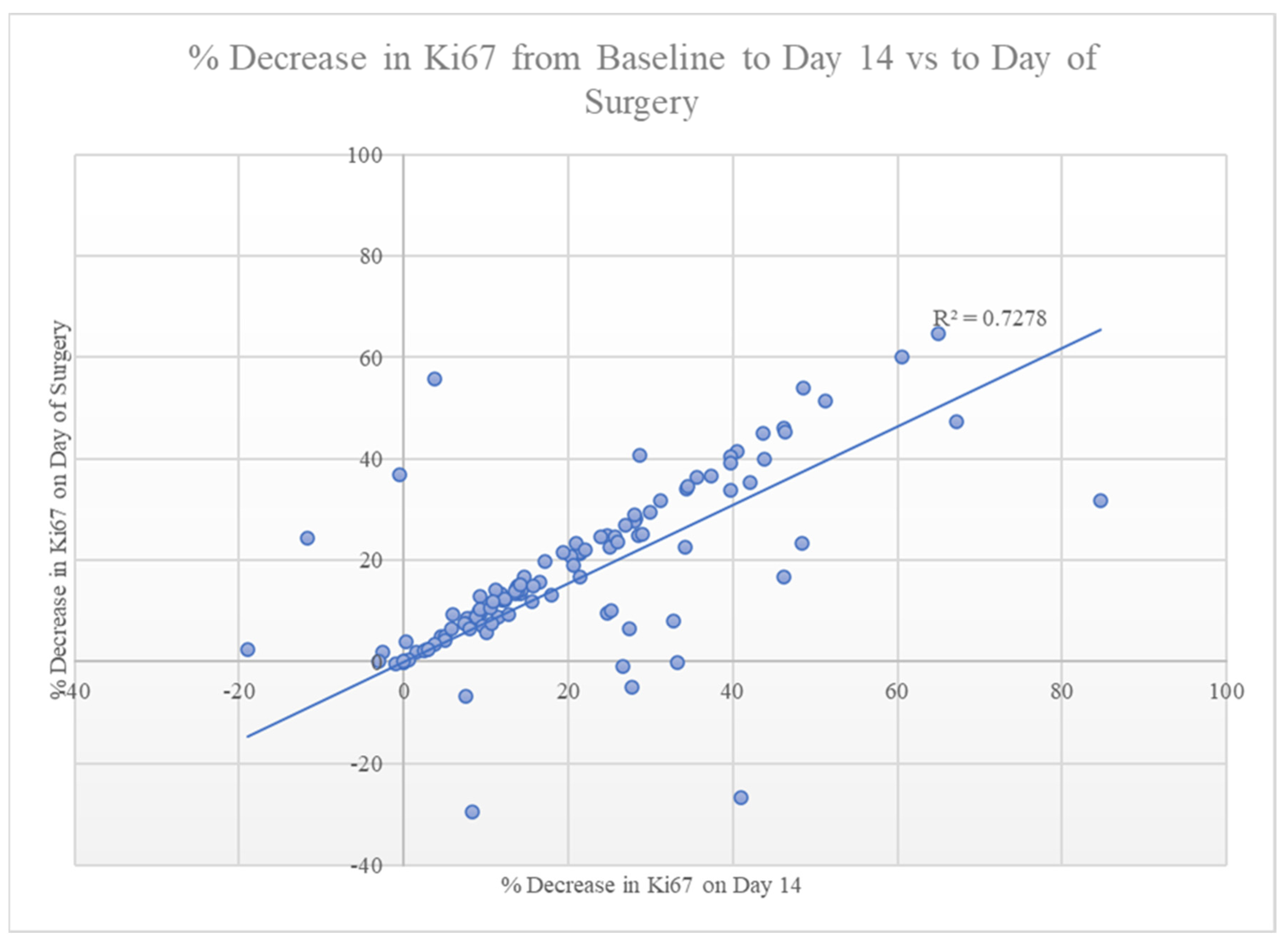
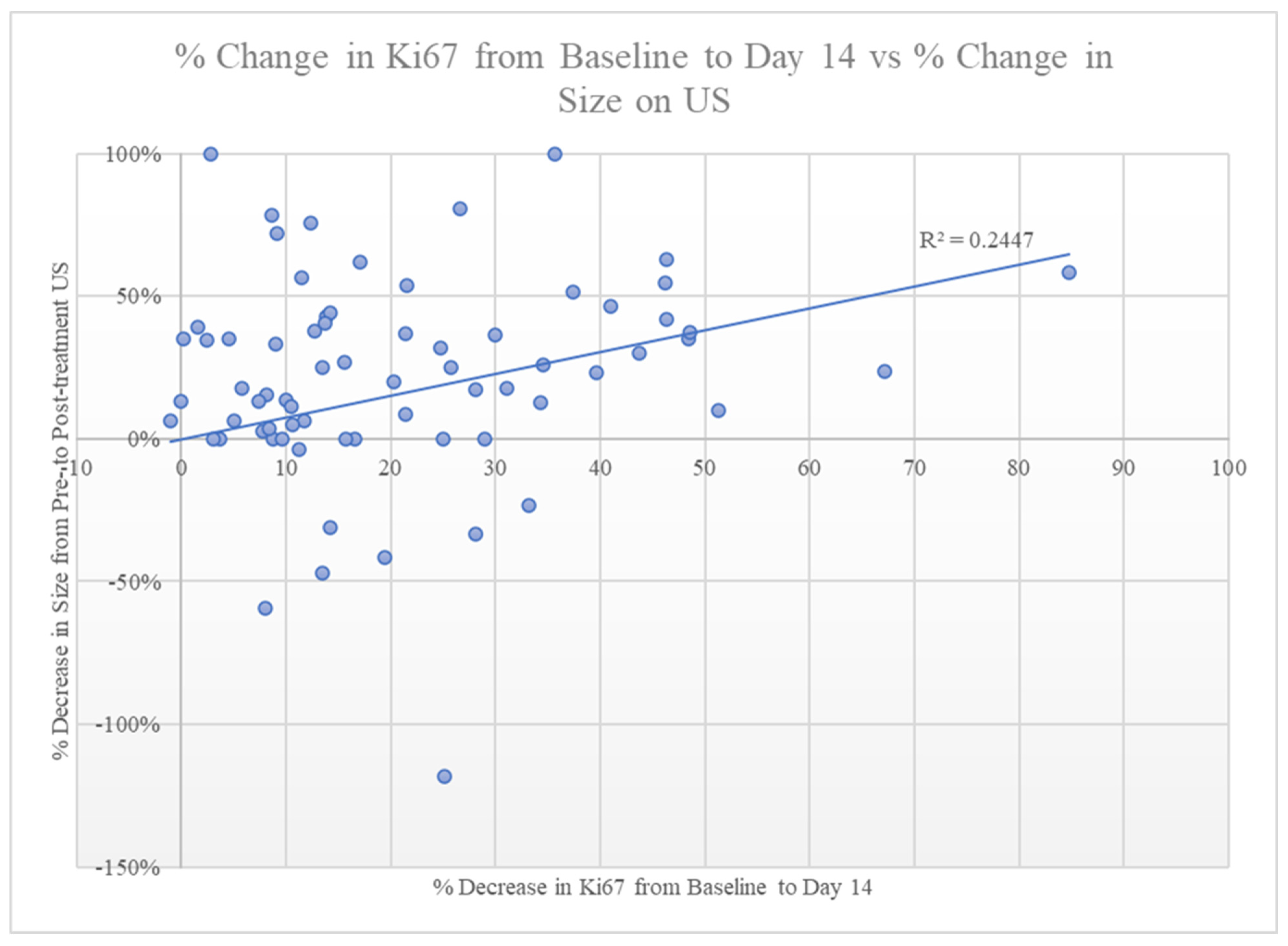
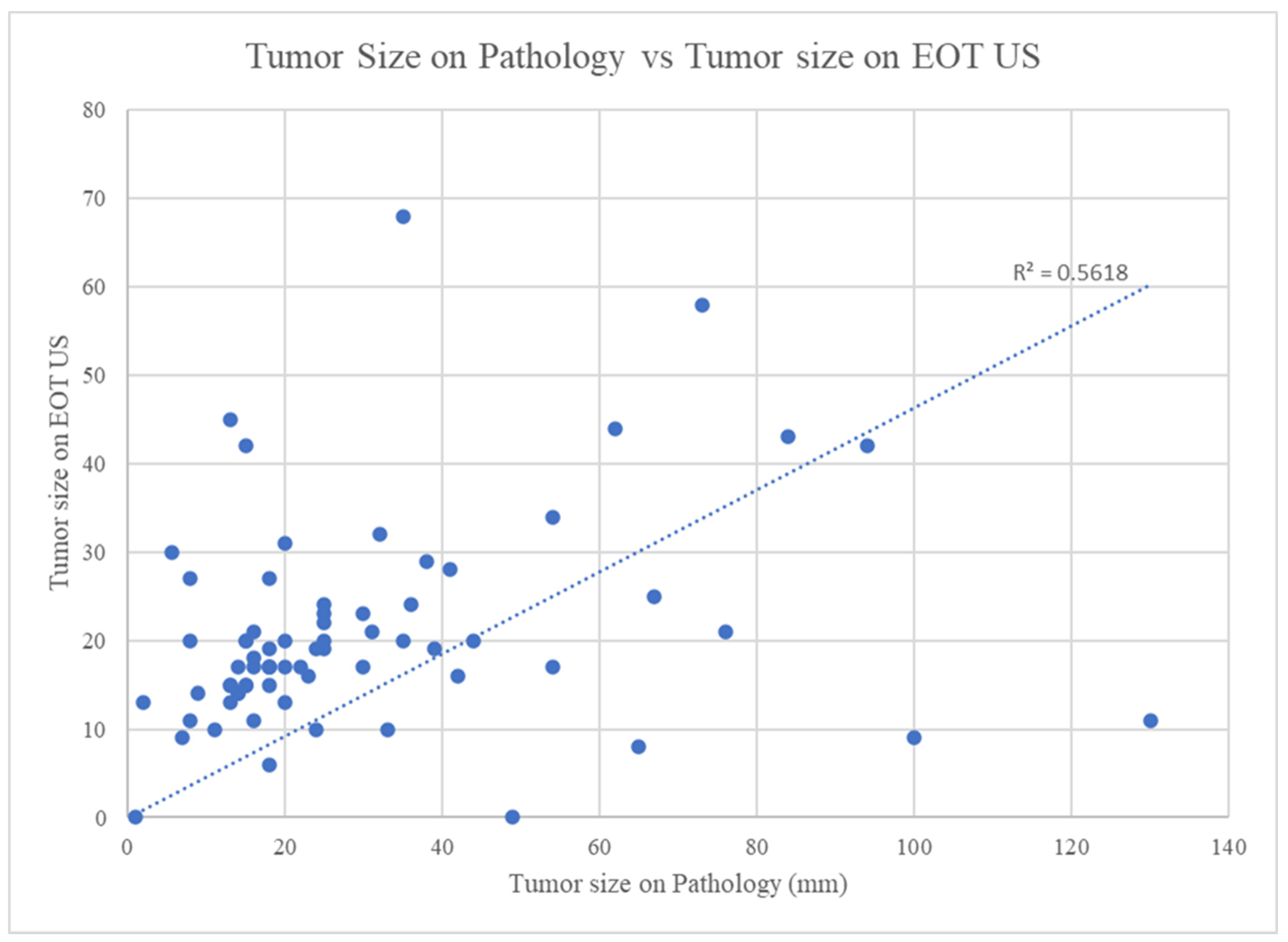
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Breast Cancer Facts and Figures 2022–2024; American Cancer Society, Inc.: Atlanta, GA, USA, 2022. [Google Scholar]
- Nabholtz, J.M.; Buzdar, A.; Pollak, M.; Harwin, W.; Burton, G.; Manalik, A.; Steinberg, M.; Webster, A.; von Euler, M. Anastrozole Is Superior to Tamoxifen as First-Line Therapy for Advanced Breast Cancer in Postmenopausal Women: Results of a North American Multicenter Randomized Trial. J. Clin. Oncol. 2000, 18, 3758–3767. [Google Scholar] [CrossRef]
- Mouridsen, H.; Gershanovich, M.; Sun, Y.; Pérez-Carrión, R.; Boni, C.; Monnier, A.; Apffelstaedt, J.; Smith, R.; Sleeboom, H.P.; Jänicke, F.; et al. Superior efficacy of letrozole versus tamoxifen as first-line therapy for postmenopausal women with advanced breast cancer: Results of a phase III study of the International Letrozole Breast Cancer Group. J. Clin. Oncol. 2001, 19, 2596–2606. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.J.; Suman, V.J.; Hoog, J.; Lin, L.; Snider, J.; Prat Aparicio, A.; Parker, J.S.; Luo, J.; DeSchryver, K.; Allred, D.C.; et al. Randomized Phase II Neoadjuvant Comparison Between Letrozole, Anastrozole, and Exemestane for Postmenopausal Women With Estrogen Receptor–Rich Stage 2 to 3 Breast Cancer: Clinical and Biomarker Outcomes and Predictive Value of the Baseline PAM50-Based Int. J. Clin. Oncol. 2011, 29, 2342–2349. [Google Scholar] [CrossRef]
- Chiba, A.; Hoskin, T.L.; Heins, C.N.; Hunt, K.K.; Habermann, E.B.; Boughey, J.C. Trends in Neoadjuvant Endocrine Therapy Use and Impact on Rates of Breast Conservation in Hormone Receptor-Positive Breast Cancer: A National Cancer Data Base Study. Ann. Surg. Oncol. 2017, 24, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Dubsky, P.C.; Singer, C.F.; Egle, D.; Wette, V.; Petru, E.; Balic, M.; Pichler, A.; Greil, R.; Petzer, A.L.; Bago-Horvath, Z.; et al. The EndoPredict score predicts response to neoadjuvant chemotherapy and neoendocrine therapy in hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer patients from the ABCSG-34 trial. Eur. J. Cancer 2020, 134, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, C.; Cleator, S.; Kilburn, L.S.; Kim, S.B.; Ahn, S.H.; Beresford, M.; Gong, G.; Mansi, J.; Mallon, E.; Reed, S.; et al. NEOCENT: A randomised feasibility and translational study comparing neoadjuvant endocrine therapy with chemotherapy in ER-rich postmenopausal primary breast cancer. Breast Cancer Res. Treat. 2014, 148, 581–590. [Google Scholar] [CrossRef]
- Prat, A.; Saura, C.; Pascual, T.; Hernando, C.; Muñoz, M.; Paré, L.; Farré, B.G.; Fernández, P.L.; Galván, P.; Chic, N.; et al. Ribociclib plus letrozole versus chemotherapy for postmenopausal women with hormone receptor-positive, HER2-negative, luminal B breast cancer (CORALLEEN): An open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 33–43. [Google Scholar] [CrossRef]
- Grossman, J.; Ma, C.; Aft, R. Neoadjuvant Endocrine Therapy. Surg. Oncol. Clin. N. Am. 2018, 27, 121–140. [Google Scholar] [CrossRef]
- Kim, H.J.; Noh, W.C.; Lee, E.S.; Jung, Y.S.; Kim, L.S.; Han, W.; Nam, S.J.; Gong, G.Y.; Kim, H.J.; Ahn, S.H. Efficacy of neoadjuvant endocrine therapy compared with neoadjuvant chemotherapy in pre-menopausal patients with oestrogen receptor-positive and HER2-negative, lymph node-positive breast cancer. Breast Cancer Res. 2020, 22, 54. [Google Scholar] [CrossRef]
- Leal, F.; Liutti, V.T.; dos Santos, V.C.; de Figueiredo, M.A.; Macedo, L.T.; Junior, J.A.; Sasse, A.D. Neoadjuvant endocrine therapy for resectable breast cancer: A systematic review and meta-analysis. Breast 2015, 24, 406–412. [Google Scholar] [CrossRef]
- Mayer, E.L.; Burstein, H.J. Adjuvant endocrine therapy for postmenopausal women: Type and duration. Breast 2015, 24, S126–S128. [Google Scholar] [CrossRef] [PubMed]
- Barchiesi, G.; Mazzotta, M.; Krasniqi, E.; Pizzuti, L.; Marinelli, D.; Capomolla, E.; Sergi, D.; Amodio, A.; Natoli, C.; Gamucci, T.; et al. Neoadjuvant Endocrine Therapy in Breast Cancer: Current Knowledge and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 3528. [Google Scholar] [CrossRef] [PubMed]
- Spring, L.M.; Gupta, A.; Reynolds, K.L.; Gadd, M.A.; Ellisen, L.W.; Isakoff, S.J.; Moy, B.; Bardia, A. Neoadjuvant Endocrine Therapy for Estrogen Receptor–Positive Breast Cancer. JAMA Oncol. 2016, 2, 1477. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.M.; Love, C.D.B.; Tucker, S.; Bellamy, C.; Leonard, R.C.F.; Miller, W.R. Letrozole as primary medical therapy for locally advanced and large operable breast cancer. Eur. J. Cancer 1998, 34, S13. [Google Scholar] [CrossRef]
- Dixon, J.M.; Renshaw, L.; Bellamy, C.; Stuart, M.; Hoctin-Boes, G.; Miller, W.R. The effects of neoadjuvant anastrozole (Arimidex) on tumor volume in postmenopausal women with breast cancer: A randomized, double-blind, single-center study. Clin. Cancer Res. 2000, 6, 2229. [Google Scholar] [PubMed]
- Ellis, M.J.; Tao, Y.; Luo, J.; A’hern, R.; Evans, D.B.; Bhatnagar, A.S.; Chaudri Ross, H.A.; Von Kameke, A.; Miller, W.R.; Smith, I.; et al. Outcome Prediction for Estrogen Receptor-Positive Breast Cancer Based on Postneoadjuvant Endocrine Therapy Tumor Characteristics. JNCI J. Natl. Cancer Inst. 2008, 100, 1380–1388. [Google Scholar] [CrossRef]
- Ellis, M.J.; Suman, V.J.; Hoog, J.; Goncalves, R.; Sanati, S.; Creighton, C.J.; DeSchryver, K.; Crouch, E.; Brink, A.; Watson, M.; et al. Ki67 Proliferation Index as a Tool for Chemotherapy Decisions During and After Neoadjuvant Aromatase Inhibitor Treatment of Breast Cancer: Results From the American College of Surgeons Oncology Group Z1031 Trial (Alliance). J. Clin. Oncol. 2017, 35, 1061–1069. [Google Scholar] [CrossRef]
- Yeo, B.; Dowsett, M. Neoadjuvant endocrine therapy: Patient selection, treatment duration and surrogate endpoints. Breast 2015, 24, S78–S83. [Google Scholar] [CrossRef]
- Fukada, I.; Araki, K.; Kobayashi, K.; Shibayama, T.; Takahashi, S.; Gomi, N.; Kokubu, Y.; Oikado, K.; Horii, R.; Akiyama, F.; et al. Pattern of Tumor Shrinkage during Neoadjuvant Chemotherapy Is Associated with Prognosis in Low-Grade Luminal Early Breast Cancer. Radiology 2018, 286, 49–57. [Google Scholar] [CrossRef]
- Spronk, P.E.R.; Volders, J.H.; van den Tol, P.; Smorenburg, C.H.; Vrancken Peeters, M.-J.T.F.D. Breast conserving therapy after neoadjuvant chemotherapy; data from the Dutch Breast Cancer Audit. Eur. J. Surg. Oncol. 2019, 45, 110–117. [Google Scholar] [CrossRef]
- Letrozole Plus Ribociclib or Placebo as Neo-adjuvant Therapy in ER-positive, HER2-negative Early Breast Cancer. Clinicaltrials.Gov. Published 2016. Available online: https://clinicaltrials.gov/show/NCT02712723 (accessed on 9 September 2022).
- Ogston, K.N.; Miller, I.D.; Payne, S.; Hutcheon, A.W.; Sarkar, T.K.; Smith, I.; Schofield, A.; Heys, S.D. A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival. Breast 2003, 12, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Ye, Y.; Yang, C.; Peng, Y.; Zong, B.; Qu, F.; Tang, Z.; Wang, Y.; Su, X.; Li, H.; et al. Assessment of the predictive role of pretreatment Ki–67 and Ki–67 changes in breast cancer patients receiving neoadjuvant chemotherapy according to the molecular classification: A retrospective study of 1010 patients. Breast Cancer Res. Treat. 2018, 170, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Vriens, B.E.; de Vries, B.; Lobbes, M.B.; van Gastel, S.M.; van den Berkmortel, F.W.; Smilde, T.J.; van Warmerdam, L.J.; de Boer, M.; van Spronsen, D.J.; Smidt, M.L.; et al. Ultrasound is at least as good as magnetic resonance imaging in predicting tumour size post-neoadjuvant chemotherapy in breast cancer. Eur. J. Cancer 2016, 52, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Song, I.H.; Seo, A.N.; Lim, B.; Kim, J.Y.; Lee, J.J.; Park, I.A.; Shin, J.; Yu, J.H.; Ahn, J.H.; et al. Correlations Between Molecular Subtypes and Pathologic Response Patterns of Breast Cancers After Neoadjuvant Chemotherapy. Ann. Surg. Oncol. 2015, 22, 392–400. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liebscher, S.C.; Kilgore, L.J.; Winblad, O.; Gloyeske, N.; Larson, K.; Balanoff, C.; Nye, L.; O’Dea, A.; Sharma, P.; Kimler, B.; et al. Use of Ultrasound and Ki–67 Proliferation Index to Predict Breast Cancer Tumor Response to Neoadjuvant Endocrine Therapy. Healthcare 2023, 11, 417. https://doi.org/10.3390/healthcare11030417
Liebscher SC, Kilgore LJ, Winblad O, Gloyeske N, Larson K, Balanoff C, Nye L, O’Dea A, Sharma P, Kimler B, et al. Use of Ultrasound and Ki–67 Proliferation Index to Predict Breast Cancer Tumor Response to Neoadjuvant Endocrine Therapy. Healthcare. 2023; 11(3):417. https://doi.org/10.3390/healthcare11030417
Chicago/Turabian StyleLiebscher, Sean C., Lyndsey J. Kilgore, Onalisa Winblad, Nika Gloyeske, Kelsey Larson, Christa Balanoff, Lauren Nye, Anne O’Dea, Priyanka Sharma, Bruce Kimler, and et al. 2023. "Use of Ultrasound and Ki–67 Proliferation Index to Predict Breast Cancer Tumor Response to Neoadjuvant Endocrine Therapy" Healthcare 11, no. 3: 417. https://doi.org/10.3390/healthcare11030417