
Impact of Endodontic Irrigant Activation on Smear Layer Removal and Surface Disintegration of Root Canal Dentine In Vitro

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
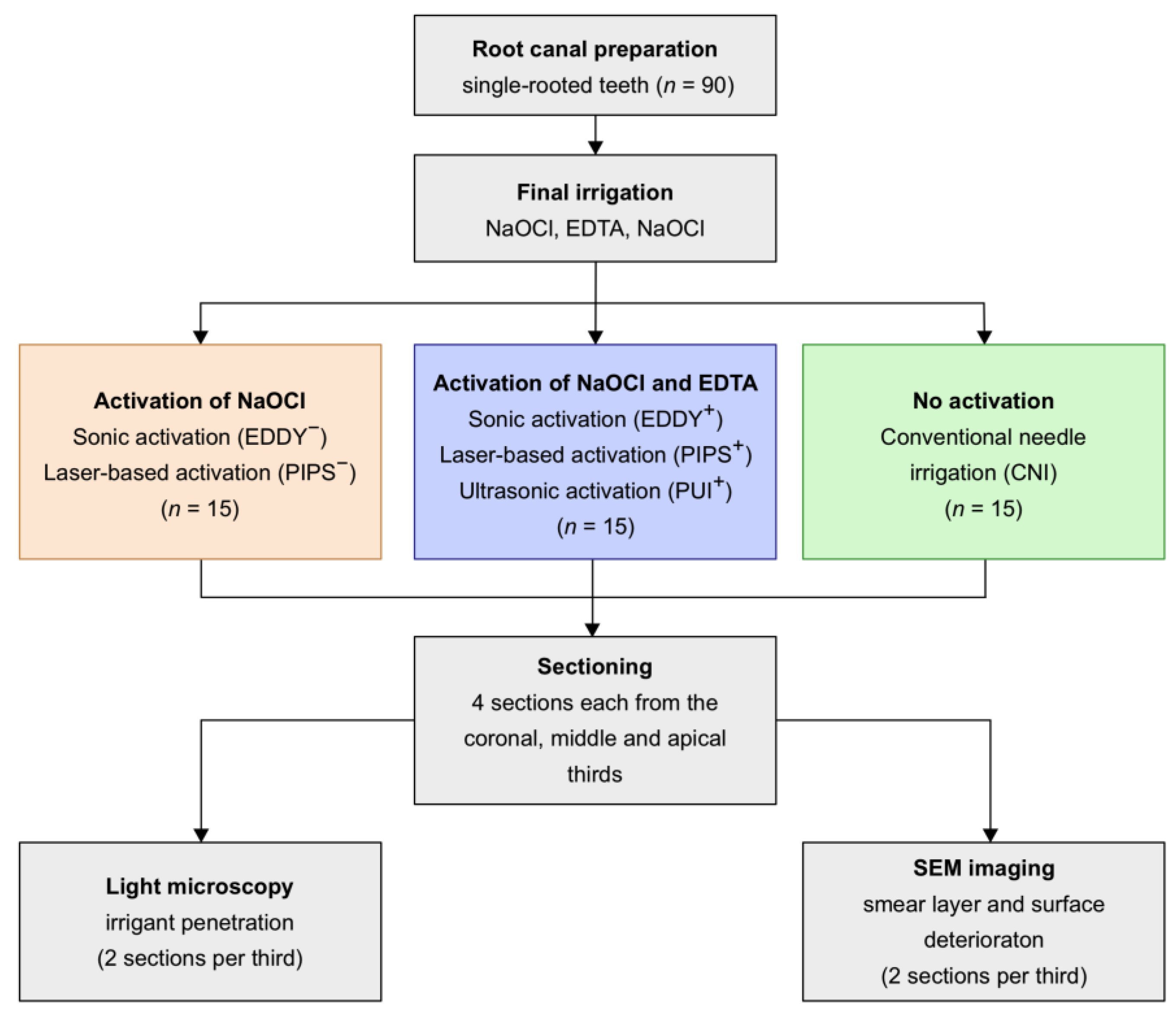
2.1. Preparation of Teeth
2.2. Final Irrigation and Activation
- NaOCl (5 mL, 1 min);
- Distilled water (5 mL, 1 min);
- EDTA (5 mL, 1 min), with or without activation for 30 s (according to groups);
- Distilled water (5 mL, 1 min);
- NaOCl (5 mL, 1 min), with or without activation for 30 s, resting phase for 30 s, activation for 30 s (according to groups);
- Distilled water (5 mL, 1 min);
- Methylene blue, activation for 30 s.
2.3. Sectioning and Imaging
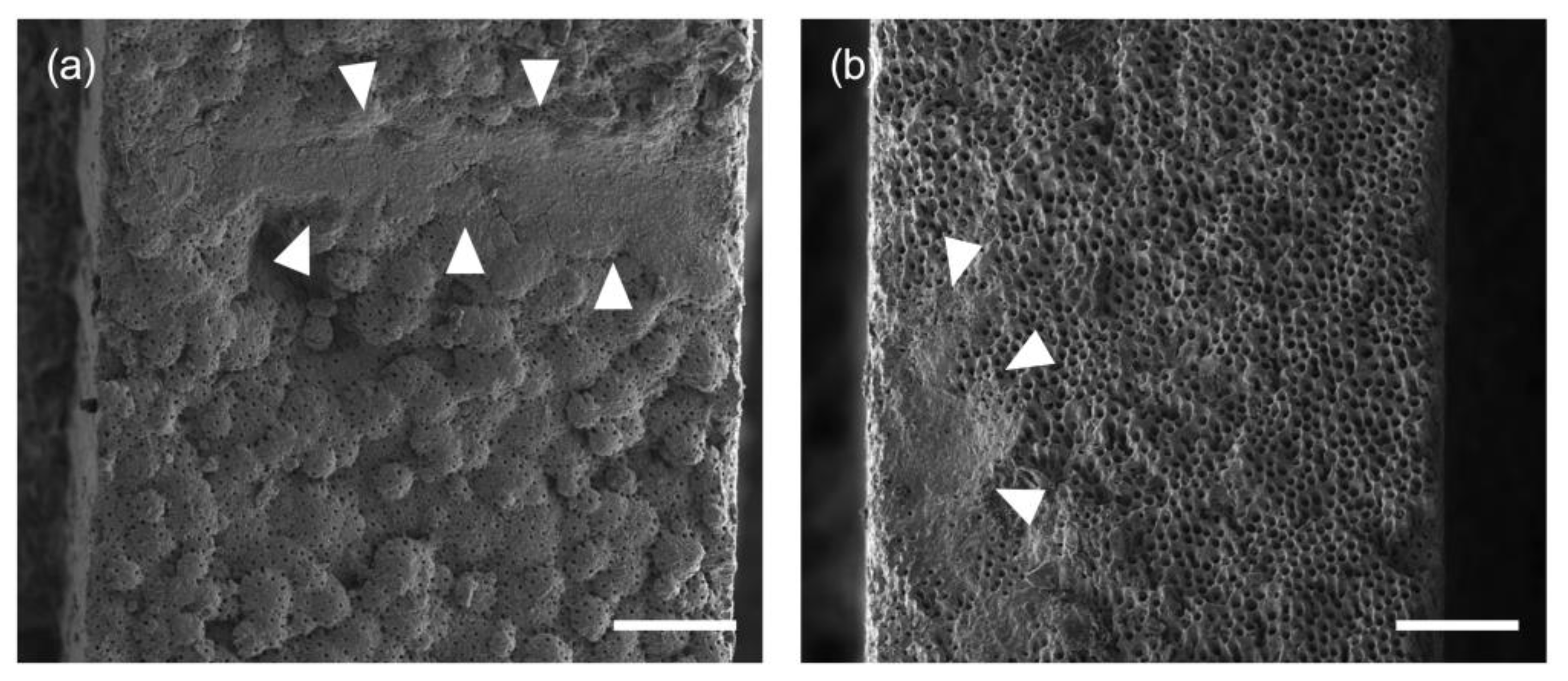
- Score 0: not present;
- Score 1: detectable on ≤ 25% of the surface area;
- Score 2: detectable on 25–50% of the surface area;
- Score 3: detectable on 50–75% of the surface area;
- Score 4: detectable on > 75% of the surface area.
2.4. Data Analysis
3. Results
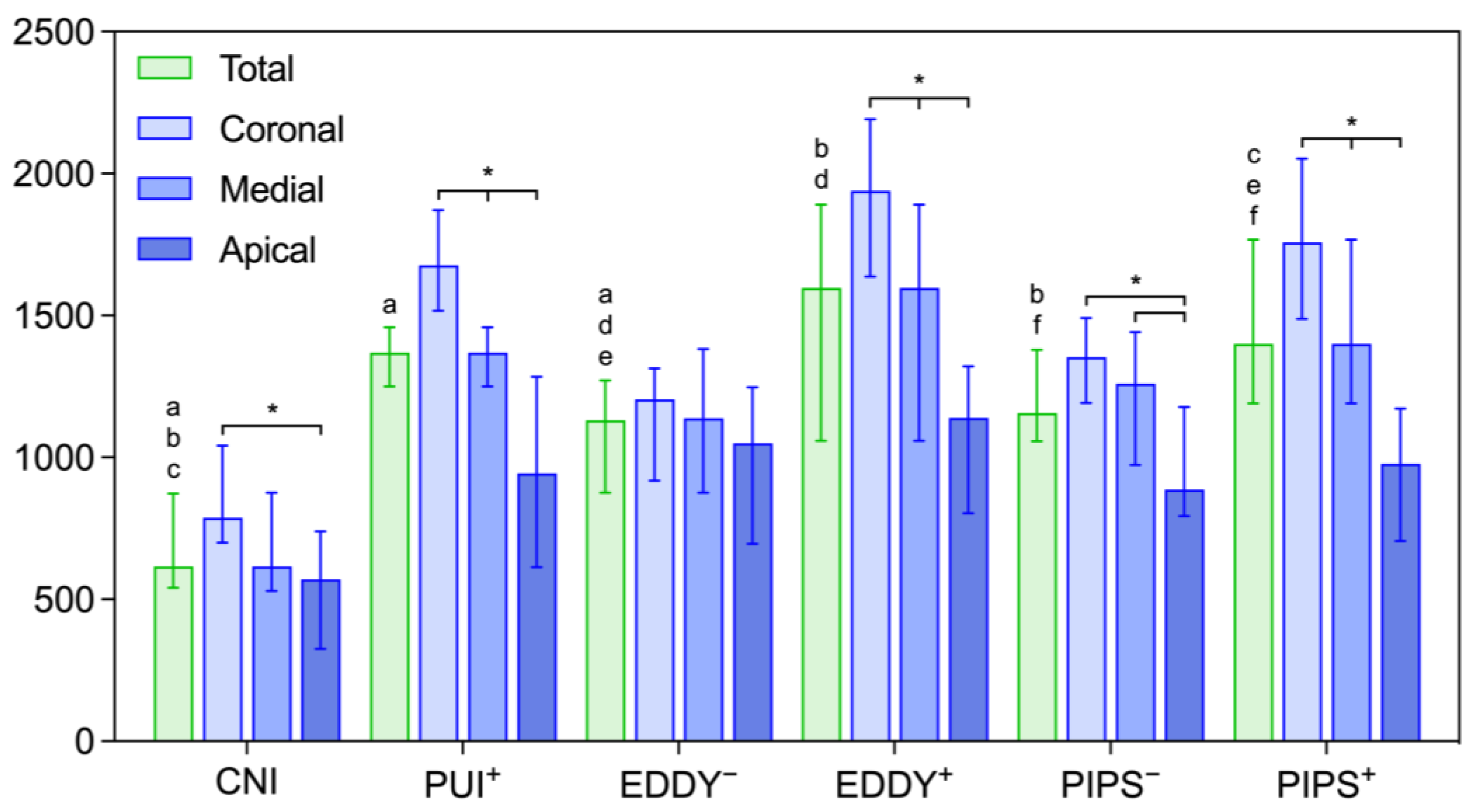
3.1. Penetration Depth of an Irrigant with and without Activation of EDTA
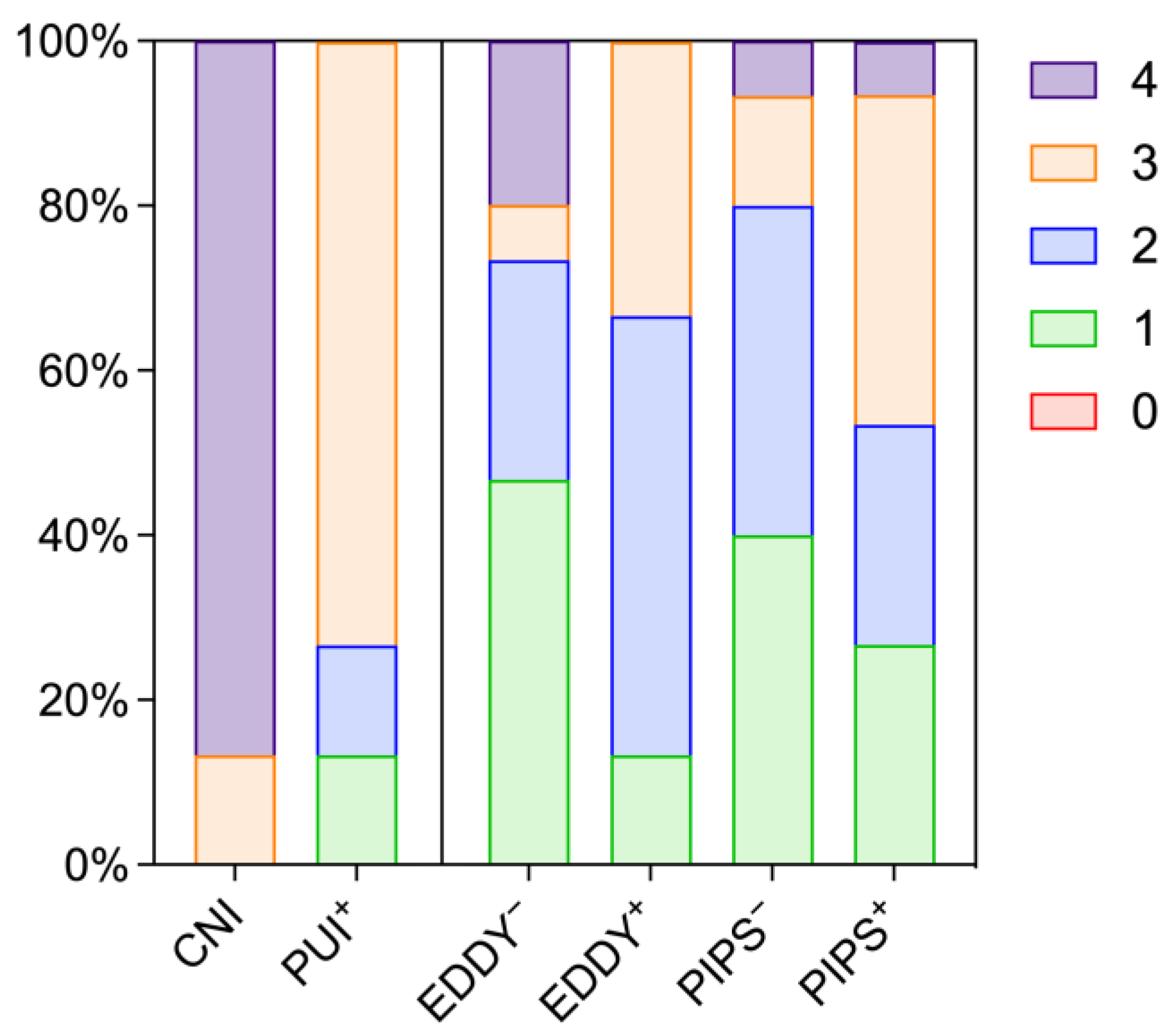
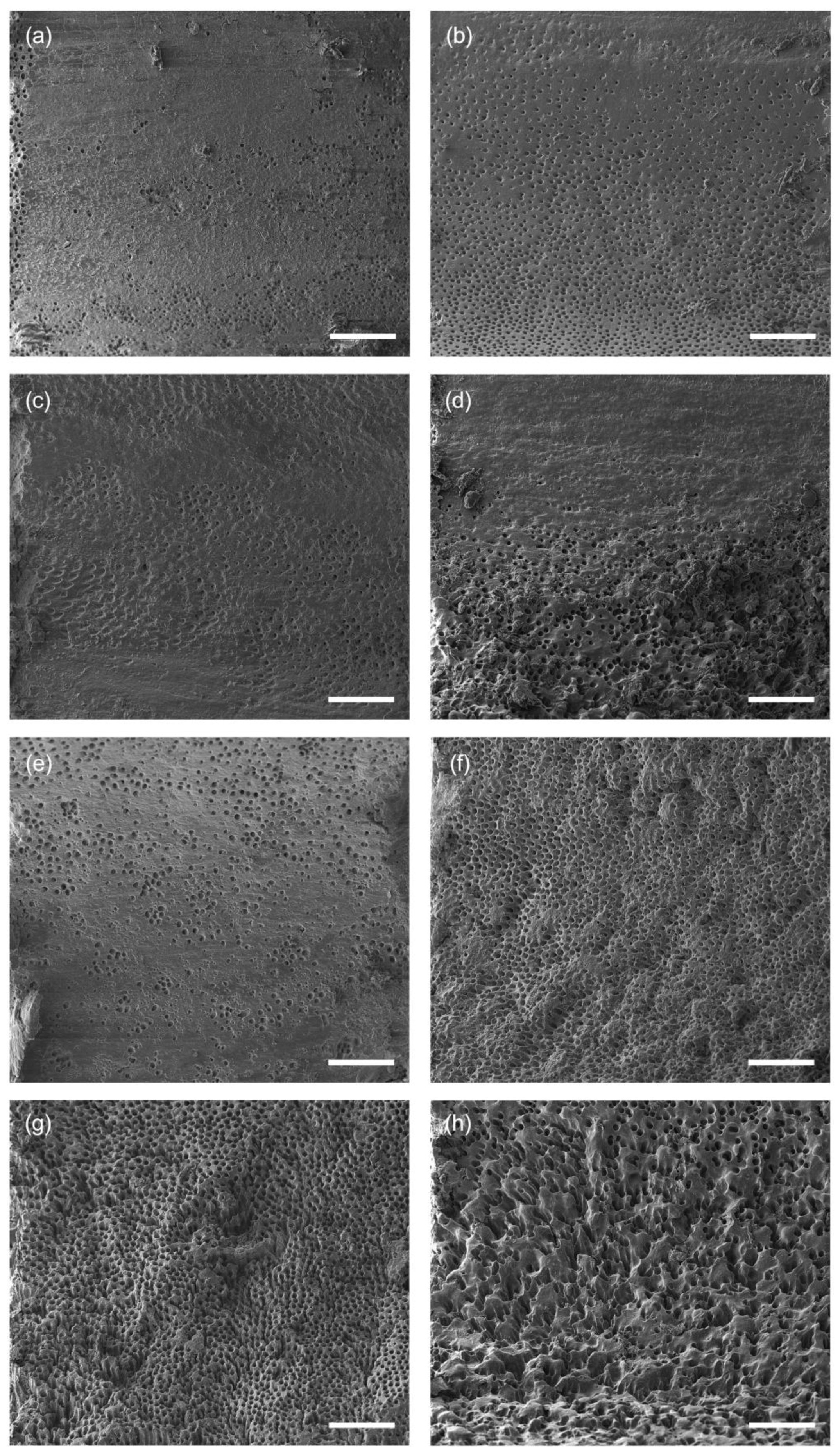
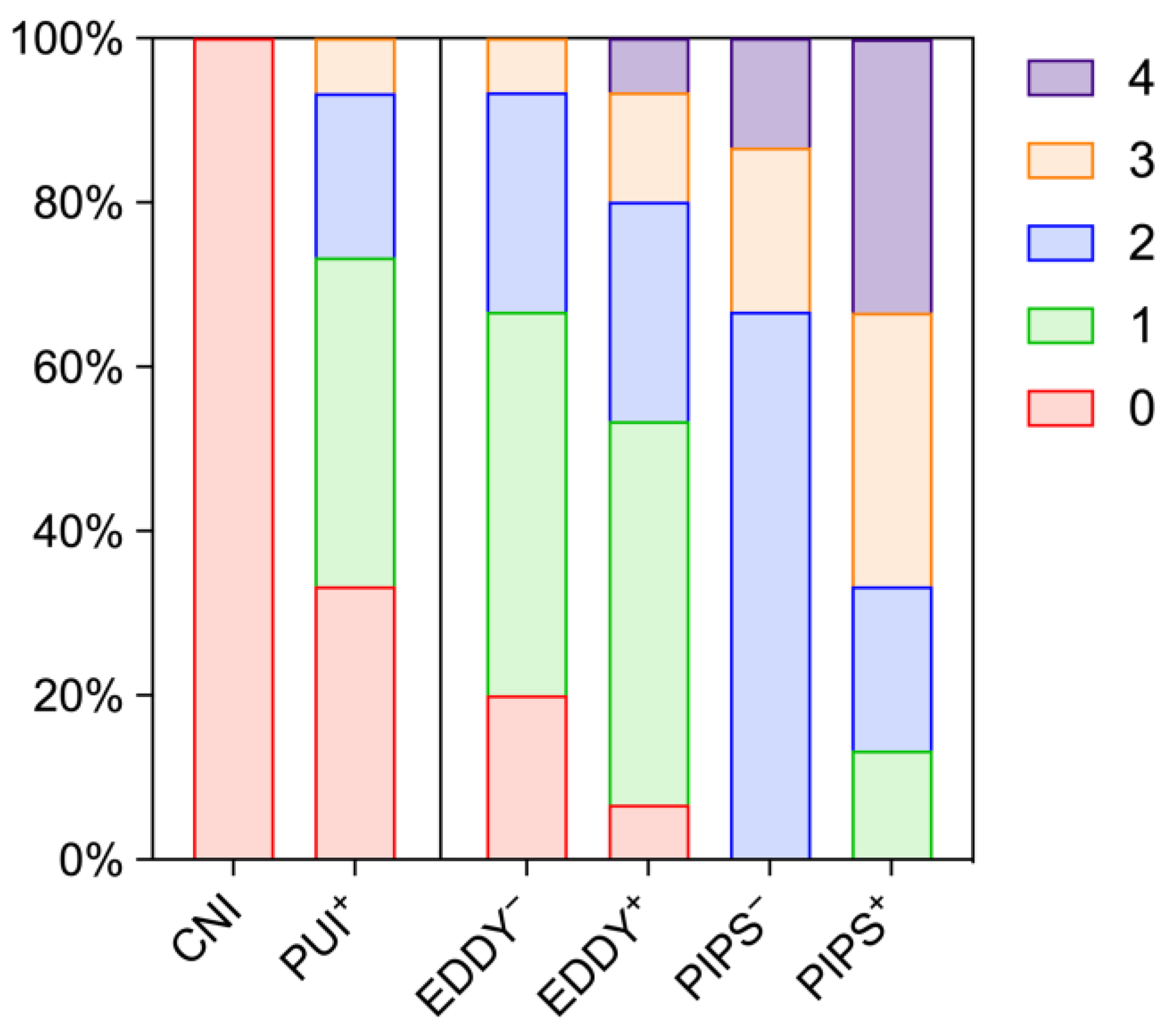
3.2. Removal of the Smear Layer
3.3. Deterioration of Dentine Surfaces
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gulabivala, K.; Patel, B.; Evans, G.; Ng, Y. Effects of mechanical and chemical procedures on root canal surfaces. Endod. Top. 2005, 10, 103–122. [Google Scholar] [CrossRef]
- Căpută, P.E.; Retsas, A.; Kuijk, L.; de Paz, L.E.C.; Boutsioukis, C. Ultrasonic irrigant activation during root canal treatment: A systematic review. J. Endod. 2019, 45, 31–44.e13. [Google Scholar] [CrossRef] [PubMed]
- Sluis, L.W.M.V.D.; Versluis, M.; Wu, M.K.; Wesselink, P.R. Passive ultrasonic irrigation of the root canal: A review of the literature. Int. Endod. J. 2007, 40, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Yadav, R.-K.; Tikku, A.-P.; Chandra, A.; Verma, P.; Bharti, R.; Shakya, V.-K. A Randomized controlled trial of endodontic treatment using ultrasonic irrigation and laser activated irrigation to evaluate healing in chronic apical periodontitis. J. Clin. Exp. Dent. 2020, 12, e821–e829. [Google Scholar] [CrossRef] [PubMed]
- Urban, K.; Donnermeyer, D.; Schäfer, E.; Bürklein, S. Canal cleanliness using different irrigation activation systems: A SEM evaluation. Clin. Oral Investig. 2017, 21, 2681–2687. [Google Scholar] [CrossRef] [PubMed]
- DiVito, E.; Peters, O.A.; Olivi, G. Effectiveness of the Erbium: YAG laser and new design radial and stripped tips in removing the smear layer after root canal instrumentation. Laser Med. Sci. 2012, 27, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Olivi, G.; DiVito, E.; Peters, O.; Kaitsas, V.; Angiero, F.; Signore, A.; Benedicenti, S. Disinfection efficacy of photon-induced photoacoustic streaming on root canals infected with Enterococcus Faecalis. J. Am. Dent. Assoc. 2014, 145, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Galler, K.M.; Grubmüller, V.; Schlichting, R.; Widbiller, M.; Eidt, A.; Schuller, C.; Wölflick, M.; Hiller, K.-A.; Buchalla, W. Penetration depth of irrigants into root dentine after sonic, ultrasonic and photoacoustic activation. Int. Endod. J. 2019, 52, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Swimberghe, R.C.D.; Buyse, R.; Meire, M.A.; Moor, R.J.G.D. Efficacy of different irrigation technique in simulated curved root canals. Laser Med. Sci. 2021, 36, 1317–1322. [Google Scholar] [CrossRef]
- Widbiller, M.; Keim, L.; Schlichting, R.; Striegl, B.; Hiller, K.-A.; Jungbauer, R.; Buchalla, W.; Galler, K.M. Debris removal by activation of endodontic irrigants in complex root canal systems: A standardized in-vitro-study. Appl. Sci. 2021, 11, 7331. [Google Scholar] [CrossRef]
- Wolf, T.G.; Paqué, F.; Woop, A.-C.; Willershausen, B.; Briseño-Marroquín, B. Root canal morphology and configuration of 123 maxillary second molars by means of micro-CT. Int. J. Oral Sci. 2017, 9, 33–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomaszewska, I.M.; Skinningsrud, B.; Jarzębska, A.; Pękala, J.R.; Tarasiuk, J.; Iwanaga, J. Internal and external morphology of mandibular molars: An original micro-CT study and meta-analysis with review of implications for endodontic therapy. Clin. Anat. 2018, 31, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Ordinola-Zapata, R.; Martins, J.N.R.; Niemczyk, S.; Bramante, C.M. Apical root canal anatomy in the mesiobuccal root of maxillary first molars: Influence of root apical shape and prevalence of apical foramina—A micro-ct study. Int. Endod. J. 2019, 52, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Nagendrababu, V.; Murray, P.E.; Ordinola-Zapata, R.; Peters, O.A.; Rôças, I.N.; Siqueira, J.F.; Priya, E.; Jayaraman, J.; Pulikkotil, S.; Camilleri, J.; et al. PRILE 2021 guidelines for reporting laboratory studies in endodontology: A consensus-based development. Int. Endod. J. 2021, 54, 1482–1490. [Google Scholar] [CrossRef] [PubMed]
- Widbiller, M.; Eidt, A.; Hiller, K.-A.; Buchalla, W.; Schmalz, G.; Galler, K.M. Ultrasonic activation of irrigants increases growth factor release from human dentine. Clin. Oral Investig. 2017, 21, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Do, Q.L.; Gaudin, A. The efficiency of the Er: YAG laser and photoninduced photoacoustic streaming (PIPS) as an activation method in endodontic irrigation: A literature review. J. Lasers Med. Sci. 2020, 11, 316–334. [Google Scholar] [CrossRef]
- Susila, A.; Minu, J. Activated irrigation vs. conventional non-activated irrigation in endodontics—A systematic review. Eur. Endod. J. 2019, 4, 96–110. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Jayaraman, J.; Suresh, A.; Kalyanasundaram, S.; Neelakantan, P. Effectiveness of ultrasonically activated irrigation on root canal disinfection: A systematic review of in vitro studies. Clin. Oral Investig. 2018, 22, 655–670. [Google Scholar] [CrossRef]
- Kakoli, P.; Nandakumar, R.; Romberg, E.; Arola, D.; Fouad, A.F. The effect of age on bacterial penetration of radicular dentin. J. Endod. 2009, 35, 78–81. [Google Scholar] [CrossRef]
- Virdee, S.S.; Farnell, D.J.J.; Silva, M.A.; Camilleri, J.; Cooper, P.R.; Tomson, P.L. The influence of irrigant activation, concentration and contact time on sodium hypochlorite penetration into root dentine: An ex vivo experiment. Int. Endod. J. 2020, 53, 986–997. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, K.V.; da Silva, B.M.; Leonardi, D.P.; Crozeta, B.M.; de Sousa-Neto, M.D.; Baratto-Filho, F.; Gabardo, M.C.L. Effectiveness of different final irrigation techniques and placement of endodontic sealer into dentinal tubules. Braz. Oral Res. 2017, 31, e114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haapasalo, M.; Shen, Y.; Qian, W.; Gao, Y. Irrigation in endodontics. Dent. Clin. N. Am. 2010, 54, 291–312. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shen, Y.; Haapasalo, M. Effect of smear layer against disinfection protocols on Enterococcus Faecalis–infected dentin. J. Endod. 2013, 39, 1395–1400. [Google Scholar] [CrossRef]
- Wang, Z.; Maezono, H.; Shen, Y.; Haapasalo, M. Evaluation of root canal dentin erosion after different irrigation methods using energy-dispersive X-ray spectroscopy. J. Endod. 2016, 42, 1834–1839. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | CNI | PUI+ | EDDY− | EDDY+ | PIPS− | PIPS+ | |
|---|---|---|---|---|---|---|---|
| Total | 0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 1 | 0.0 | 13.3 | 46.7 | 13.3 | 40.0 | 26.7 | |
| 2 | 0.0 | 13.3 | 26.7 | 53.3 | 40.0 | 26.7 | |
| 3 | 13.3 | 73.3 | 6.7 | 33.3 | 13.3 | 40.0 | |
| 4 | 86.7 | 0.0 | 20.0 | 0.0 | 6.7 | 6.7 | |
| Coronal | 0 | 6.7 | 0.0 | 0.0 | 0.0 | 0.0 | 6.7 |
| 1 | 0.0 | 6.7 | 40.0 | 33.3 | 40.0 | 46.7 | |
| 2 | 26.7 | 46.7 | 33.3 | 40.0 | 33.3 | 20.0 | |
| 3 | 0.0 | 40.0 | 13.3 | 20.0 | 20.0 | 20.0 | |
| 4 | 66.7 | 6.7 | 13.3 | 6.7 | 6.7 | 6.7 | |
| Medial | 0 | 0.0 | 0.0 | 0.0 | 0.0 | 6.7 | 6.7 |
| 1 | 0.0 | 13.3 | 60.0 | 33.3 | 33.3 | 26.7 | |
| 2 | 13.3 | 26.7 | 20.0 | 40.0 | 40.0 | 20.0 | |
| 3 | 0.0 | 60.0 | 6.7 | 20.0 | 13.3 | 40.0 | |
| 4 | 86.7 | 0.0 | 13.3 | 6.7 | 6.7 | 6.7 | |
| Apical | 0 | 0.0 | 0.0 | 0.0 | 0.0 | 13.3 | 0.0 |
| 1 | 0.0 | 13.3 | 13.3 | 0.0 | 26.7 | 13.3 | |
| 2 | 0.0 | 6.7 | 26.7 | 20.0 | 33.3 | 13.3 | |
| 3 | 13.3 | 46.7 | 33.3 | 60.0 | 0.0 | 40.0 | |
| 4 | 86.7 | 33.3 | 26.7 | 20.0 | 26.7 | 33.3 |
| Score | CNI | PUI+ | EDDY− | EDDY+ | PIPS− | PIPS+ | |
|---|---|---|---|---|---|---|---|
| Total | 0 | 100.0 | 33.3 | 20.0 | 6.7 | 0.0 | 0.0 |
| 1 | 0.0 | 40.0 | 46.7 | 46.7 | 0.0 | 13.3 | |
| 2 | 0.0 | 20.0 | 26.7 | 26.7 | 66.7 | 20.0 | |
| 3 | 0.0 | 6.7 | 6.7 | 13.3 | 20.0 | 33.3 | |
| 4 | 0.0 | 0.0 | 0.0 | 6.7 | 13.3 | 33.3 | |
| Coronal | 0 | 100.0 | 46.7 | 46.7 | 20.0 | 13.3 | 6.7 |
| 1 | 0.0 | 40.0 | 33.3 | 66.7 | 13.3 | 13.3 | |
| 2 | 0.0 | 13.3 | 20.0 | 6.7 | 53.3 | 33.3 | |
| 3 | 0.0 | 0.0 | 0.0 | 6.7 | 13.3 | 20.0 | |
| 4 | 0.0 | 0.0 | 0.0 | 0.0 | 6.7 | 26.7 | |
| Medial | 0 | 100.0 | 40.0 | 26.7 | 13.3 | 20.0 | 13.3 |
| 1 | 0.0 | 46.7 | 53.3 | 53.3 | 46.7 | 26.7 | |
| 2 | 0.0 | 13.3 | 13.3 | 13.3 | 26.7 | 6.7 | |
| 3 | 0.0 | 0.0 | 6.7 | 20.0 | 6.7 | 33.3 | |
| 4 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 20.0 | |
| Apical | 0 | 100.0 | 46.7 | 53.3 | 33.3 | 13.3 | 13.3 |
| 1 | 0.0 | 33.3 | 33.3 | 46.7 | 40.0 | 33.3 | |
| 2 | 0.0 | 13.3 | 6.7 | 13.3 | 26.7 | 20.0 | |
| 3 | 0.0 | 6.7 | 6.7 | 0.0 | 13.3 | 26.7 | |
| 4 | 0.0 | 0.0 | 0.0 | 6.7 | 6.7 | 6.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Widbiller, M.; Rosendahl, A.; Schlichting, R.; Schuller, C.; Lingl, B.; Hiller, K.-A.; Buchalla, W.; Galler, K.M. Impact of Endodontic Irrigant Activation on Smear Layer Removal and Surface Disintegration of Root Canal Dentine In Vitro. Healthcare 2023, 11, 376. https://doi.org/10.3390/healthcare11030376
Widbiller M, Rosendahl A, Schlichting R, Schuller C, Lingl B, Hiller K-A, Buchalla W, Galler KM. Impact of Endodontic Irrigant Activation on Smear Layer Removal and Surface Disintegration of Root Canal Dentine In Vitro. Healthcare. 2023; 11(3):376. https://doi.org/10.3390/healthcare11030376
Chicago/Turabian StyleWidbiller, Matthias, Andreas Rosendahl, Ralf Schlichting, Christine Schuller, Benedikt Lingl, Karl-Anton Hiller, Wolfgang Buchalla, and Kerstin M. Galler. 2023. "Impact of Endodontic Irrigant Activation on Smear Layer Removal and Surface Disintegration of Root Canal Dentine In Vitro" Healthcare 11, no. 3: 376. https://doi.org/10.3390/healthcare11030376