
The Effect of Service Quality on Patient Citizenship Behaviors: Evidence from the Health Sector

Abstract
:1. Introduction
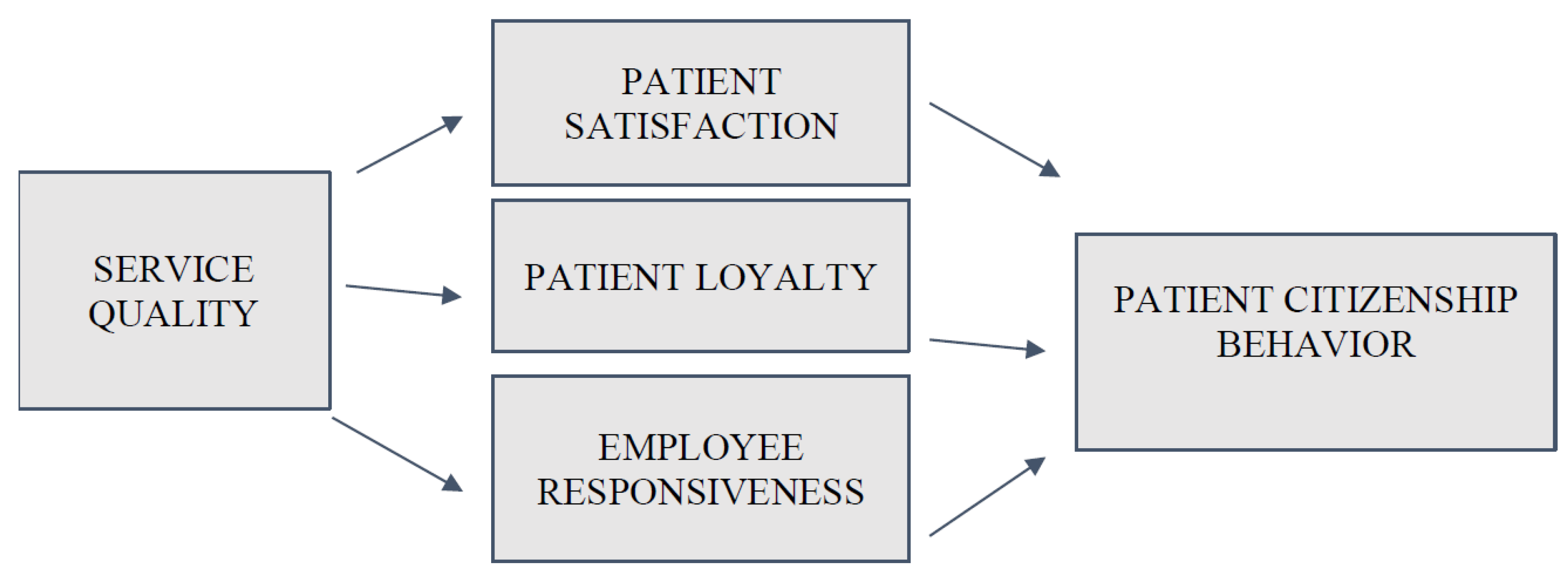
1.1. Theoretical Framework
1.1.1. The Mediating Role of Patient Satisfaction
1.1.2. The Mediating Role of Patient Loyalty
1.1.3. The Mediating Role of Employee Responsiveness
2. Materials and Methods
2.1. Sample and Data Collection
2.2. Instruments
2.3. Ethics
2.4. Demographics
2.5. Reliability and Validity
3. Results
3.1. Direct Effects
3.2. Mediating Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, S.; Li, G.; Liu, N.; Hongwei, W. The impact of patient satisfaction on patient loyalty with the mediating effect of patient trust. Inquiry 2021, 58, 469580211007221. [Google Scholar] [CrossRef] [PubMed]
- Fatima, T.; Malik, S.A.; Shabbir, A. Hospital healthcare service quality, patient satisfaction and loyalty: An investigation in context of private healthcare systems. Int. J. Qual. Reliab. Manag. 2018, 35, 1195–1214. [Google Scholar] [CrossRef]
- Groth, M. Customers as good soldiers: Examining citizenship behaviors in internet service deliveries. J. Manag. 2005, 31, 7–27. [Google Scholar] [CrossRef]
- Fowler, J.G. Customer citizenship behavior: An expanded theoretical understanding. Int. J. Bus. Soc. Sci. 2013, 4, 1–8. Available online: https://ijbssnet.com/journals/Vol_4_No_5_May_2013/1.pdf (accessed on 1 August 2022).
- Jung, J.H.; Yoo, J.J. Customer-to-customer interactions on customer citizenship behavior. Serv. Bus. 2017, 11, 117–139. [Google Scholar] [CrossRef]
- Yi, Y.; Gong, T.; Lee, H. The impact of other customers on customer citizenship behavior. Psychol. Mark. 2013, 30, 341–356. [Google Scholar] [CrossRef]
- Hwang, J.; Han, H.; Choo, S.W. An investigation of the formation of rapport between players and dealers in the casino industry. J. Destin. Mark. Manag. 2016, 5, 97–106. [Google Scholar] [CrossRef]
- Yi, Y.; Gong, T. The antecedents and consequences of service customer citizenship and badness behavior. Seoul J. Bus. 2006, 12, 145–176. Available online: https://strathprints.strath.ac.uk/38577/1/2006_SJB.pdf (accessed on 5 August 2022).
- Rosenbaum, M.S.; Massiah, C.A. When customers receive support from other customers: Exploring the influence of inter-customer social support on customer voluntary performance. J. Serv. Res. 2007, 9, 257–270. [Google Scholar] [CrossRef]
- Ponnusamy, G. Customers as volunteers? E-customer citizenship behavior and its antecedents. Inf. Manag. Bus. Rev. 2015, 7, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Nagy, A.; Galal, E.S.; Marzouk, W. Factors affecting customer citizenship behavior: A model of university students. Int. J. Mark. Stud. 2018, 10, 54–70. [Google Scholar] [CrossRef] [Green Version]
- Cropanzano, R.; Mitchell, M.S. Social exchange theory: An interdisciplinary review. J. Manag. 2005, 31, 874–900. [Google Scholar] [CrossRef]
- Blau, P.M. Exchange and Power in Social Life, 2nd ed.; Routledge: New York, NY, USA, 1986; p. 372. [Google Scholar] [CrossRef]
- Ali, O.M. The Roles of Relationships and Service Quality as Drivers of Customer Loyalty: An Empirical Study. Open J. Soc. Sci. 2020, 8, 19. Available online: http://www.scirp.org/journal/Paperabs.aspx?PaperID=99313 (accessed on 7 August 2022).
- Singh, J.; Sirdeshmukh, D. Agency and trust mechanisms in consumer satisfaction and loyalty judgments. J. Acad. Mark. Sci. 2000, 28, 150–167. [Google Scholar] [CrossRef]
- Jin, H. Empirical study of impacts of intrinsic and extrinsic motivations on employee knowledge sharing: Crowding-out and crowding-in effect. J. Manag. Sci. 2013, 26, 31–44. Available online: http://jis.sagepub.com/content/33/2/135 (accessed on 7 August 2022).
- Guo, S.; Guo, X.; Fang, Y.; Vogel, D. How doctors gain social and economic returns in online health-care communities: A professional capital perspective. J. Manag. Inf. Syst. 2017, 34, 487–519. [Google Scholar] [CrossRef]
- Van Tonder, E.; Saunders, S.G.; Lisita, I.T.; de Beer, L.T. The importance of customer citizenship behavior in the modern retail environment: Introducing and testing a social exchange model. J. Retail. Consum. Serv. 2018, 45, 92–102. [Google Scholar] [CrossRef]
- Assiouras, I.; Skourtis, G.; Giannopoulos, A.; Buhalis, D.; Koniordos, M. Value co-creation and customer citizenship behavior. Ann. Tour. Res. 2019, 78, 102742. [Google Scholar] [CrossRef]
- Maqsood, M.; Maqsood, H.; Kousar, R.; jabeen, C.; Waqas, A.; Gillani, S.A. Effects of Hospital Service quality on Patients Satisfaction and Behavioral intention of Doctors and Nurses. Saudi J. Med. Pharm. Sci. 2017, 3, 556–567. Available online: https://www.researchgate.net/publication/318861112_Effects_of_hospital_service_quality_on_patients_satisfaction_and_behavioural_intention_of_doctors_and_nurses (accessed on 5 August 2022).
- Karsana, W.; Murhadi, W.R. Effect of Service Quality and Patient Satisfaction on Behavioral Intention. J. Entrep. Bus. 2021, 2, 25–36. [Google Scholar] [CrossRef]
- Zeithaml, V.A. Consumer perceptions of price, quality, and value: A means-end model and synthesis of evidence. J. Mark. 1988, 52, 35–48. [Google Scholar] [CrossRef]
- Rama, K.R.; Panda, R.K. Customer perceived service quality, satisfaction and customer loyalty: An empirical test of mediation in private hospitals. In Proceedings of the International Conference on Advances in Healthcare Management Services, Indian Institute of Management, Ahmedabad, India, 6–7 June 2015; Available online: http://hdl.handle.net/11718/14117 (accessed on 5 August 2022).
- Kotler, P.; Keller, K.L. Marketing Management; Pearson Education Limited: Edinburgh, UK, 2012; Volume 14, Available online: https://cdn.website-editor.net/25dd89c80efb48d88c2c233155dfc479/files/uploaded/Kotler_keller_-_marketing_management_14th_edition.pdf (accessed on 7 August 2022).
- Gruen, T.W. The outcome set of relationship marketing in consumer markets. Int. Bus. Rev. 1995, 4, 47–469. [Google Scholar] [CrossRef]
- Gong, T.; Yi, Y. A review of customer citizenship behaviors in the service context. Serv. Ind. J. 2021, 41, 169–199. [Google Scholar] [CrossRef]
- Bove, L.L.; Pervan, S.J.; Beatty, S.E.; Shiu, E. Service worker role in encouraging customer organizational citizenship behaviors. J. Bus. Res. 2009, 62, 698–705. [Google Scholar] [CrossRef]
- Burmann, C.; Jost-Benz, M.; Riley, N. Towards an identity-based brand equity model. J. Bus. Res. 2009, 62, 390–397. [Google Scholar] [CrossRef]
- Lengnick-Hall, C.A.; Claycomb, V.; Inks, L.W. From recipient to contributor: Examining customer roles and experienced outcomes. Eur. J. Mark. 2000, 34, 359–383. [Google Scholar] [CrossRef]
- Bettencourt, L.A. Customer voluntary performance: Customers as partners in service delivery. J. Retail. 1997, 73, 383–406. [Google Scholar] [CrossRef]
- Revilla-Camacho, M.Á.; Vega-Vázquez, M.; Cossío-Silva, F.J. Customer participation and citizenship behavior effects on turnover intention. J. Bus. Res. 2015, 68, 1607–1611. [Google Scholar] [CrossRef]
- Mandl, L.; Hogreve, J. Buffering effects of brand community identification in service failures: The role of customer citizenship behaviors. J. Bus. Res. 2020, 107, 130–137. [Google Scholar] [CrossRef]
- Anbori, A.; Ghani, S.N.; Yadav, H.; Daher, A.M.; Su, T.T. Patient satisfaction and loyalty to the private hospitals in Sana’a, Yemen. Int. J. Qual. Health Care 2010, 22, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Oliver Richard, L. Whence Consumer Loyalty? J. Mark. 1999, 63, 33–44. [Google Scholar] [CrossRef]
- Aliman, N.K.; Mohamad, W.N. Linking service quality, patients’ satisfaction and behavioral intentions: An investigation on private healthcare in Malaysia. Procedia-Soc. Behav. Sci. 2016, 224, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Yi, Y.; Nataraajan, R.; Gong, T. Customer participation and citizenship behavioral influences on employee performance, satisfaction, commitment, and turnover intention. J. Bus. Res. 2011, 64, 87–95. [Google Scholar] [CrossRef]
- Sharif, K.; Sidi Lemine, M. Customer service quality, emotional brand attachment and customer citizenship behaviors: Findings from an emerging higher education market. J. Mark. High. Educ. 2021, 1, 1–26. [Google Scholar] [CrossRef]
- Hu, H.-Y.; Cheng, C.-C.; Chiu, S.-I.; Hong, F.-Y. A study of Customer satisfaction, customer Loyalty and quality attributes in Taiwan’s Medical service industry. Afr. J. Bus. Manag. 2011, 5, 187–195. [Google Scholar]
- Kuo, Y.; Wu, C.; Deng, W. The relationship among service quality, perceived value, customer satisfaction, and post-purchase intention in mobile value-added services. Comput. Hum. Behav. 2009, 25, 887–896. [Google Scholar] [CrossRef]
- Setyawan, F.E.B.; Supriyanto, S.; Tunjungsari, F.; Hanifaty, W.O.N.; Lestari, R. Medical staff services quality to patients’ satisfaction based on SERVQUAL dimensions. Int. J. Public Health Sci. 2019, 8, 51–57. [Google Scholar] [CrossRef]
- Cavena, R.; Corbett, L.; Lo, Y. Developing zones of tolerance for managing passenger rail services. Int. J. Qual. Reliab. Manag. 2007, 24, 7–31. [Google Scholar] [CrossRef]
- Kumar, S.A.; Mani, B.T.; Mahaligam, S.; Vanjikovan, M. Influence of service quality on additional loyalty in private retail banking. An empirical study. IUP J. Manag. Res. 2010, 9, 21–38. Available online: https://web.s.ebscohost.com/ehost/pdfviewer/pdfviewer?vid=0&sid=c5d6b75c-7704-4d91-a019-4ae591670001%40redis (accessed on 12 October 2022).
- Tung, V.W.S.; Chen, P.J.; Schuckert, M. Managing customer citizenship behavior: The moderating roles of employee responsiveness and organizational reassurance. Tour. Manag. 2017, 59, 23–35. [Google Scholar] [CrossRef]
- Yesilyurt, O.; Tekin, M. Evaluation of the Effect of Dimensions of Perceived Service Quality, Perceived Risk and Perceived Value in Healthcare Enterprise on Patient Satisfaction and Behavioral Intention with Structural Equation Model. 2018; Unpublished thesis. Available online: https://tez.yok.gov.tr/UlusalTezMerkezi/tezDetay.jsp?id=ILVUi_K4dnjJYQW9bC3MLA&no=9yBZvChzYb-0OUROZ_cedA (accessed on 5 August 2022).
- Erdem, R.; Avcı, L.; Rahman, S.; Avci, L.; Demirel, B.; Köseoğlu, S.; Firat, G. The Effect of Patient Satisfaction On Patient Commitment. Erciyes Univ. J. Fac. Econ. Adm. Sci. 2008, 31, 95–110. Available online: https://dergipark.org.tr/en/download/article-file/66512 (accessed on 12 October 2022).
- Nambisan, P.; Gustafson, D.H.; Hawkins, R.; Pingree, S. Social support and responsiveness in online patient communities: Impact on service quality perceptions. Health Expect 2016, 19, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parasuraman, A.; Zeithaml, V.; Berry, L. SERVQUAL: A Multiple-item Scale for Measuring Consumer Perceptions of Service Quality. J. Retail. 1988, 64, 12–40. Available online: https://www.researchgate.net/profile/Valarie-Zeithaml-2/publication/225083802_SERVQUAL_A_multiple-_Item_Scale_for_measuring_consumer_perceptions_of_service_quality/links/5429a4540cf27e39fa8e6531/SERVQUAL-A-multiple-Item-Scale-for-measuring-consumer-perceptions-of-service-quality.pdf (accessed on 12 October 2022).
- Sututemiz, N.; Altunısık, R. Antecedents of Customer Loyalty and Comparison of Customer Loyalty Models: A study in Banking and Healthcare Sectors. Available online: https://hdl.handle.net/20.500.12619/77438 (accessed on 5 August 2022).
- Aracı, U.E.; Sezgin, E.K. The Study of Validity and Reliability of Customer Citizenship Behavior Scale. J. Turk. Tour. Res. 2020, 4, 1279–1293. Available online: https://tutad.org/index.php/tutad/article/view/237.09 (accessed on 19 October 2022).
- Robertson, N.L.; Bove, L.L.; Pervan, S.J. Exploring the relationship between customer loyalty to the service worker and customer citizenship behaviors to the service organization. In Proceedings of the Academy of Marketing Science Conference, Curtin Uiversity of Technology, Perth, WA, USA, 11–14 June 2003. [Google Scholar]
- Patterson, P.G.; Razzaque, M.A.; Terry, C.S.L. Customer Citizenship Behavior in Service Organizations: A Social Exchange Model. 2003. Available online: https://www.researchgate.net/profile/Paul-Patterson-6/publication/237770594_Customer_Citizenship_Behaviour_in_Service_Organisations_A_Social_Exchange_Model/links/540f88b10cf2d8daaad0a5d0/Customer-Citizenship-Behaviour-in-Service-Organisations-A-Social-Exchange-Model.pdf (accessed on 25 October 2022).
- Hennig Thurau, T.; Gwinner, K.P.; Gremler, D.D. Understanding relationship marketing outcomes. J. Serv. Res. 2002, 4, 230–247. [Google Scholar] [CrossRef] [Green Version]
- Bove, L.; Johnson, L. Predicting personal loyalty to a service worker. Australas. Mark. J. 2002, 10, 24–35. [Google Scholar] [CrossRef]
- Garba, O.A.; Babalol, a.M.T.; Guo, L. A social exchange perspective on why and when ethical leadership foster customer-oriented citizenship behavior. Int. J. Hosp. Manag. 2018, 70, 1–8. [Google Scholar] [CrossRef]
- Hamzah, Z.L.; Lee, S.P.; Moghavvemi, S. Elucidating perceived overall service quality in retail banking. Int. J. Bank Mark. 2017, 35, 781–804. [Google Scholar] [CrossRef]
- Abuosi, A.A.; Atinga, R.A. Service quality in healthcare institutions: Establishing the gaps for policy action. Int. J. Health Care Qual. Assur. 2013, 26, 481–492. [Google Scholar] [CrossRef]
- Pakurár, M.; Haddad, H.; Nagy, J.; Popp, J.; Oláh, J. The service quality dimensions that affect customer satisfaction in the Jordanian banking sector. Sustainability 2019, 11, 1113. [Google Scholar] [CrossRef] [Green Version]
- Kessler, D.P.; Mylod, D. Does patient satisfaction affect patient loyalty? Int. J. Health Care Qual. Assur. 2011, 24, 266–273. Available online: https://www.emerald.com/insight/content/doi/10.1108/09526861111125570/full/pdf?title=does-patient-satisfaction-affect-patient-loyalty (accessed on 15 September 2022). [CrossRef] [PubMed]
- Asadpoor, S.; Abolfazli, A. The Effect of electronic service quality on customer satisfaction and loyalty Saderat Bank’s customers. Int. J. Sci. Study 2017, 5, 407–411. Available online: http://www.ijss-sn.com/uploads/2/0/1/5/20153321/14_ijss-mahdi_jul_oa14_-_2017.pdf (accessed on 15 September 2022).
- Pratminingsih, S.A.; Astuty, E.; Widyatami, K. Increasing customer loyalty of ethnic restaurant through experiential marketing and service quality. J. Entrep. Educ. 2018, 21, 1–11. Available online: https://www.researchgate.net/profile/Eriana-Astuty/publication/335661869_INCREASING_CUSTOMER_LOYALTY_OF_ETHNIC_RESTAURANT_THROUGH_EXPERIENTIAL_MARKETING_AND_SERVICE_QUALITY/links/5d7260ea4585151ee4a0eedd/INCREASING-CUSTOMER-LOYALTY-OF-ETHNIC-RESTAURANT-THROUGH-EXPERIENTIAL-MARKETING-AND-SERVICE-QUALITY.pdf (accessed on 1 November 2022).
- Zaid, A.A.; Arqawi, S.M.; Mwais, R.M.A.; Al Shobaki, M.J.; Abu-Naser, S.S. The Impact of Total Quality Management and Perceived Service Quality on Patient Satisfaction and Behavior Intention in Palestinian Healthcare Organizations. Technol. Rep. Kansai Univ. 2020, 62, 221–232. [Google Scholar]
- Slack, N.J.; Singh, G. The effect of service quality on customer satisfaction and loyalty and the mediating role of customer satisfaction. TQM J. 2020, 32, 543–558. Available online: https://www.emerald.com/insight/1754-2731.htm (accessed on 6 November 2022). [CrossRef]
- Mahendrayana, I.M.A.; Yasa, P.N.S.; Indiani, L.P. The effect of service quality on patient loyalty mediated by patient satisfaction in Bali Siloam Hospital. J. Ekon. Bisnis JAGADITHA 2018, 5, 1–7. [Google Scholar] [CrossRef]
- Asnawi, A.A.; Awang, Z. Influence of hospital image and service quality on patients’ satisfaction and their loyalty intention. Int. J. Account. Financ. Bus. 2018, 3, 105–118. [Google Scholar] [CrossRef]
- Moreira, A.C.; Silva, P.M. The trust-commitment challenge in service quality-loyalty relationships. Int. J. Health Care Qual. Assur. 2015, 28, 253–266. [Google Scholar] [CrossRef]
- Meesala, A.; Paul, J. Service quality, consumer satisfaction and loyalty in hospitals: Thinking for the future. J. Retail. Consum. Serv. 2018, 40, 261–269. [Google Scholar] [CrossRef]
- Berinyuy, B.; Forje, L.C.; Dzekashu, L.G. Service Quality, a Correlation of Customer Expectation and Customer Perception of Services Received Responsiveness and Empathy in Shisong Hospital. Int. J. Soc. Sci. Hum. Res. 2021, 4, 3495–3505. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scale | Sub-Dimension | Questions | Authors |
|---|---|---|---|
| Service Quality | Physical properties—tangibles | 1–4 | (Yesilyurt and Tekin, 2018) [44] |
| Reliability | 5–9 | ||
| Responsiveness | 10–13 | ||
| Assurance | 14–17 | ||
| Empathy | 18–22 | ||
| Patient Satisfaction | - | 9 questions | (Yesilyurt and Tekin, 2018) [44] |
| Patient Loyalty | - | 11 questions | (Erdem et al. 2008) [45] |
| Employee Responsiveness | 2 questions | (Nambisan et al., 2016) [46] | |
| Patient Citizenship Behaviors | Helping customers | 1–4 | (Aracı and Sezgin, 2020) [49] |
| Flexibility—tolerance | 5–7 | ||
| Making recommendations | 8–10 | ||
| Providing feedback to the organization | 11–13 |
| Number of Participants (N) | % | ||
|---|---|---|---|
| Sex | Male | 173 | 42.19 |
| Female | 237 | 57.80 | |
| Total | 410 | 100 | |
| Education | Primary School | 32 | 7.8 |
| Secondary School | 6 | 1.4 | |
| High school | 156 | 38.04 | |
| University or higher | 216 | 52.68 | |
| Total | 410 | 100 | |
| Age | 18–25 | 189 | 46.09 |
| 26–35 | 99 | 23.62 | |
| 36–45 | 73 | 17.80 | |
| 46–55 | 32 | 7.8 | |
| 56–65 | 17 | 4.14 | |
| Total | 410 | 100 | |
| Region | Nicosia | 176 | 42.92 |
| Kyrenia | 39 | 9.5 | |
| Famagusta | 124 | 30.24 | |
| Iskele | 34 | 8.29 | |
| Lefke | 13 | 3.1 | |
| Guzelyurt | 24 | 5.85 | |
| Total | 410 | 100 | |
| Participant’s Hospital Preferences | Public Hospital | 170 | 41.46 |
| Private Hospital | 128 | 31.21 | |
| Both Public and Private Together | 112 | 27.31 | |
| Total | 410 | 100 |
| Parameter | Estimate | Lower | Upper | P | Hypothesis | Accepted/Rejected | ||
|---|---|---|---|---|---|---|---|---|
| SQ | → | PL | 0.852 | 0.808 | 0.897 | 0.010 | H2 | Accepted |
| SQ | → | PS | 0.882 | 0.844 | 0.916 | 0.010 | H1 | Accepted |
| SQ | → | ER | 0.821 | 0.768 | 0.878 | 0.010 | H3 | Accepted |
| PL | → | PCB | 0.586 | 0.418 | 0.717 | 0.010 | H2 | Accepted |
| PS | → | PCB | 0.424 | 0.264 | 0.595 | 0.010 | H1 | Accepted |
| ER | → | PCB | 0.177 | 0.088 | 0.303 | 0.010 | H3 | Accepted |
| SQ | → | PCB | −0.180 | −0.347 | −0.063 | 0.018 | ||
| Parameter | Estimate | Lower | Upper | P | Hypothesis | Accepted/Rejected |
|---|---|---|---|---|---|---|
| SQ --> PS --> PCB | 0.143 | 0.088 | 0.207 | 0.010 | H1 | Accepted |
| SQ --> PL --> PCB | 0.253 | 0.168 | 0.350 | 0.010 | H2 | Accepted |
| SQ --> ER --> PCB | 0.048 | 0.011 | 0.097 | 0.025 | H3 | Accepted |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulucayli, S.; Cek, K.; Oniz, A. The Effect of Service Quality on Patient Citizenship Behaviors: Evidence from the Health Sector. Healthcare 2023, 11, 370. https://doi.org/10.3390/healthcare11030370
Ulucayli S, Cek K, Oniz A. The Effect of Service Quality on Patient Citizenship Behaviors: Evidence from the Health Sector. Healthcare. 2023; 11(3):370. https://doi.org/10.3390/healthcare11030370
Chicago/Turabian StyleUlucayli, Saime, Kemal Cek, and Adile Oniz. 2023. "The Effect of Service Quality on Patient Citizenship Behaviors: Evidence from the Health Sector" Healthcare 11, no. 3: 370. https://doi.org/10.3390/healthcare11030370