
Effects of Nonpharmacological Interventions on Sleep Quality and Insomnia in Perimenopausal and Postmenopausal Women: A Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Criteria for Inclusion and Exclusion
2.2. Search Methods
2.3. Study Selection and Data Extraction
2.4. Risk of Bias in Individual Studies
2.5. Statistical Analysis
3. Results
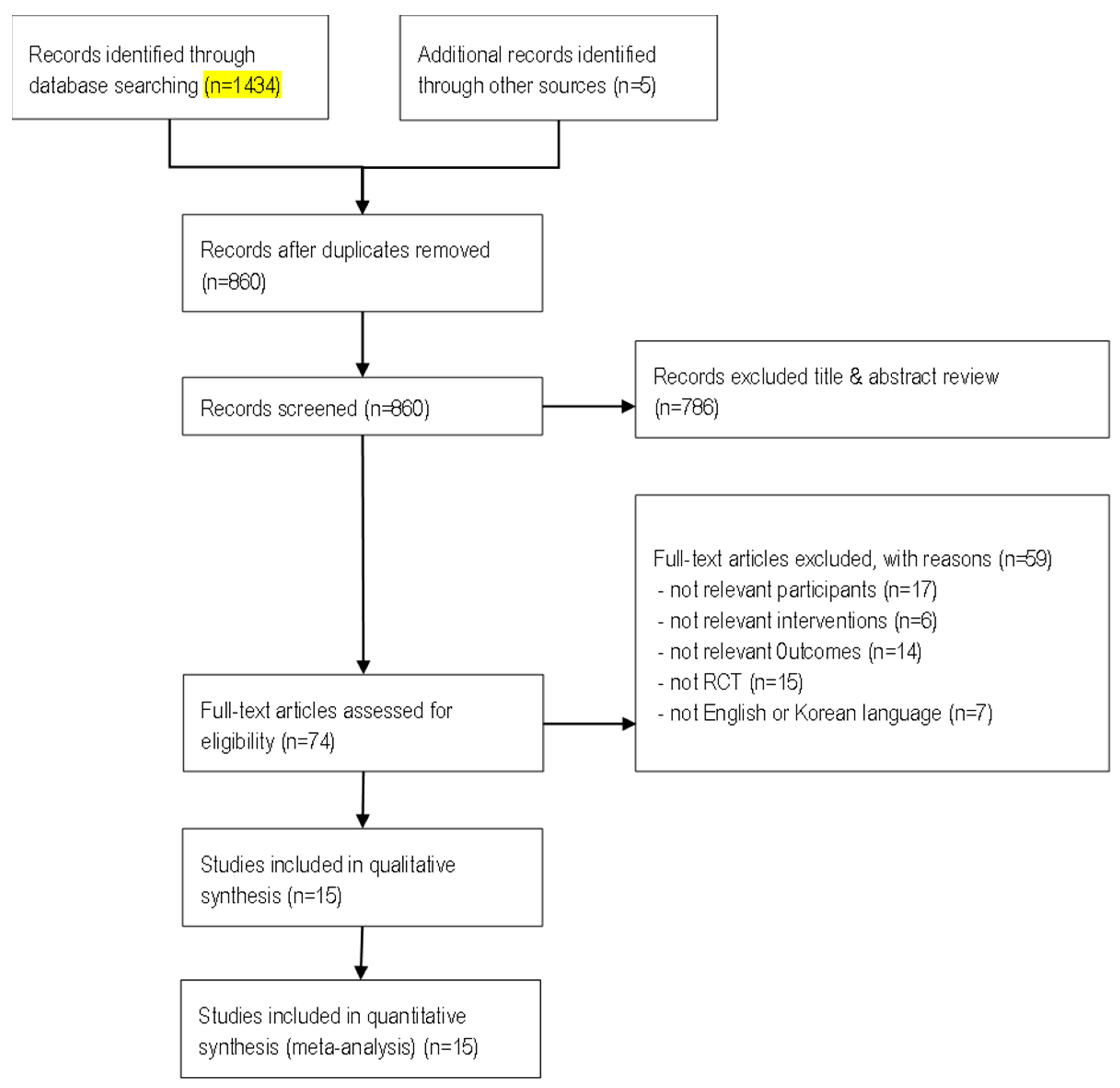
3.1. Study Selection
3.2. Characteristics of Selected Studies
3.3. Quality Assessment of Selected Studies
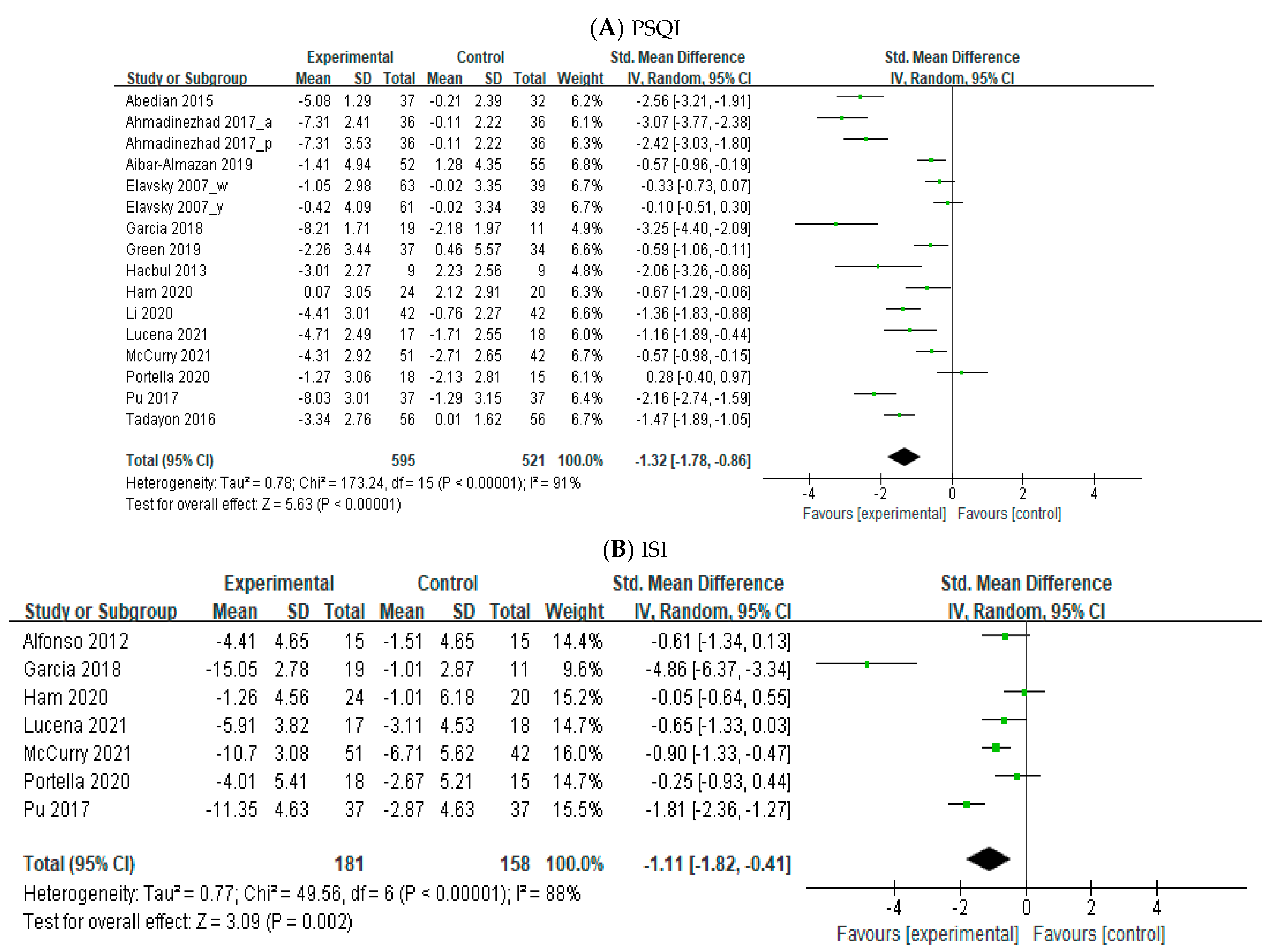
3.4. Overall Effects of Nonpharmacological Intervention
3.5. Moderator Analysis
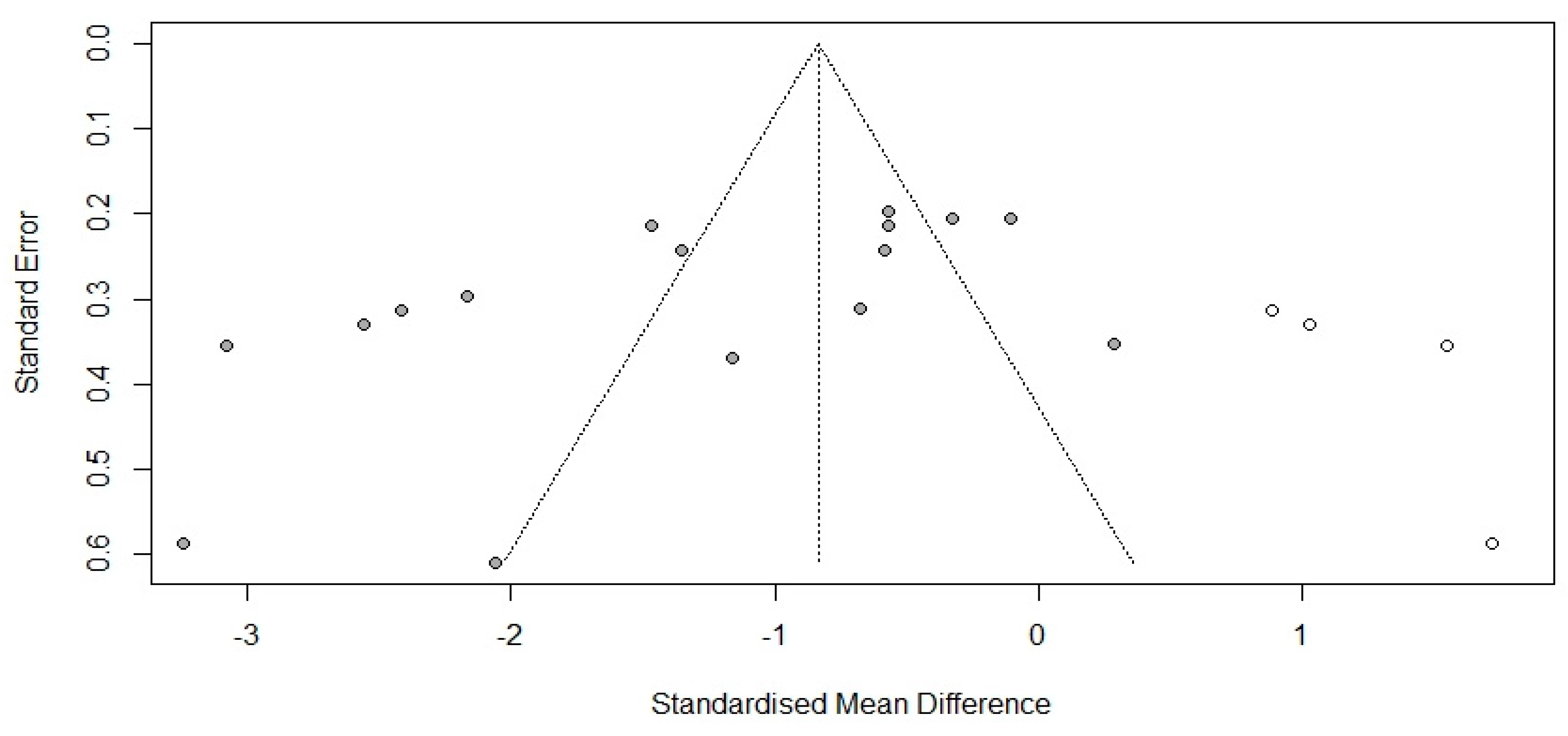
3.6. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.; Ahn, S. Impact of menopausal status, metabolic syndrome and its risk factors on impaired quality of life above middle-aged women. Korean J. Women Health Nurs. 2016, 22, 275–286. [Google Scholar] [CrossRef] [Green Version]
- Sussman, M.; Trocio, J.; Best, C.; Mirkin, S.; Bushmakin, A.G.; Yood, R.; Friedman, M.; Menzin, J.; Louie, M. Prevalence of menopausal symptoms among mid-life women: Findings from electronic medical records. BMC Women’s Health 2015, 15, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, N.F.; Mitchell, E.S. Symptoms during the perimenopause: Prevalence, severity, trajectory, and significance in women’s lives. Am. J. Med. 2005, 118, 14–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gozuyesil, E.; Gokyildiz Surucu, S.; Alan, S. Sexual function and quality-of-life related problems during menopausal period. J. Health Psychol. 2018, 23, 1769–1780. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.Y. The study of menopause-related quality of life and management climacteric in a middle-aged female population in Korea. Public Health Wkly. Rep. 2013, 6, 609–613. [Google Scholar]
- Baker, F.; De Zambotti, M.; Colrain, I.M.; Bei, B. Sleep problems during the menopausal transition: Prevalence, impact, and management challenges. Nat. Sci. Sleep 2018, 10, 73–95. [Google Scholar] [CrossRef] [Green Version]
- Grandner, M.A. Sleep, health, and society. Sleep Med. Clin. 2020, 15, 319–340. [Google Scholar] [CrossRef]
- Arakane, M.; Castillo, C.; Rosero, M.F.; Peñafiel, R.; Pérez-López, F.R.; Chedraui, P. Factors relating to insomnia during the menopausal transition as evaluated by the Insomnia Severity Index. Maturitas 2011, 69, 157–161. [Google Scholar] [CrossRef]
- Harris, A.L.; Harrison, A. A examining sleep disturbance during the menopausal period. Nurs. Women’s Health 2020, 24, 134–142. [Google Scholar] [CrossRef]
- Bierman, E.J.; Comijs, H.C.; Gundy, C.M.; Sonnenberg, C.; Jonker, C.; Beekman, A.T. The effect of chronic benzodiazepine use on cognitive functioning in older persons: Good, bad or indifferent? Int. J. Geriatr. Psychiatry 2007, 22, 1194–1200. [Google Scholar] [CrossRef]
- Davidson, J.R. Insomnia treatment options for women. Obstet. Gynecol. Clin. N. Am. 2009, 36, 831–846. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J. Pharmacotherapy of insomnia. J. Korean Med. Assoc. 2009, 52, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Schroeck, J.L.; Ford, J.; Conway, E.L.; Kurtzhalts, K.E.; Gee, M.E.; Vollmer, K.A.; Mergenhagen, K.A. Review of safety and efficacy of sleep medicines in older adults. Clin. Ther. 2016, 38, 2340–2372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, P.; Dennis, J. A systematic review of non-pharmacological therapies for sleep problems in later life. Sleep Med. Rev. 2004, 8, 47–62. [Google Scholar] [CrossRef]
- Patel, D.; Steinberg, J.; Patel, P. Insomnia in the elderly: A review. J. Clin. Sleep Med. 2018, 14, 1017–1024. [Google Scholar] [CrossRef] [Green Version]
- MacLeod, S.; Musich, S.; Kraemer, S.; Wicker, E. Practical non-pharmacological intervention approaches for sleep problems among older adults. Geriatr. Nurs. 2018, 39, 506–512. [Google Scholar] [CrossRef]
- Flaxer, J.M.; Heyer, A.; Francosis, D. Evidence-based review and evaluation of clinical significance: Nonpharmacological and pharmacological treatment of insomnia in the elderly. Am. J. Geriatr. Psychiatry 2021, 29, 585–603. [Google Scholar] [CrossRef]
- Chae, J.H.; Kim, Y.S.; Han, M.Y. Effects of non-pharmacological interventions on cancer patients with sleep disorder: A meta-analysis. Asian Oncol. Nurs. 2021, 21, 1–14. [Google Scholar] [CrossRef]
- Chung, B.Y.; Park, H.S. Effects of non-pharmacological interventions for adults with insomnia in Korea: A meta-analysis. J. Korea Acad.-Ind. Coop. Soc. 2017, 18, 95–106. [Google Scholar]
- Leysen, L.; Lahousse, A.; Nijs, J.; Adriaenssens, N.; Mairesse, O.; Ivakhnov, S.; Bilterys, T.; Van Looveren, E.; Pas, R.; Beckwée, D. Prevalence and risk factors of sleep disturbances in breast cancer survivors: Systematic review and meta-analyses. Support Care Cancer 2019, 27, 4401–4433. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: West Sussex, UK, 2009; pp. 15–32. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systemic Reviews of Interventions Version 6.2; Updated February 2021; Cochrane: London, UK, 2021; Available online: https://www.training.cochrane.org/handbook (accessed on 26 December 2022).
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abedian, Z.; Eskandari, L.; Abdi, H.; Ebrahimzadeh, S. The effect of acupressure on sleep quality in menopausal women: A randomized control trial. Iran. J. Med. Sci. 2015, 40, 328–334. [Google Scholar] [PubMed]
- Ahmadinezhad, M.; Kargar, M.; Vizeshfar, F.; Hadianfard, M.J. Comparison of the effect of acupressure and pilates-based exercises on sleep quality of postmenopausal women: A randomized controlled trial. Iran. J. Nurs. Midwifery Res. 2017, 22, 140–146. [Google Scholar]
- Aibar-Almazán, A.; Hita-Contreras, F.; Cruz-Díaz, D.; de la Torre-Cruz, M.; Jiménez-García, J.D.; Martínez-Amat, A. Effects of pilates training on sleep quality, anxiety, depression and fatigue in postmenopausal women: A randomized controlled trial. Maturitas 2019, 124, 62–67. [Google Scholar] [CrossRef]
- Elavsky, S.; McAuley, E. Lack of perceived sleep improvement after 4-month structured exercise programs. Menopause 2007, 14, 535–540. [Google Scholar] [CrossRef]
- Garcia, M.C.; Kozasa, E.H.; Tufik, S.; Mello, L.; Hachul, H. The effects of mindfulness and relaxation training for insomnia (MRTI) on postmenopausal women: A pilot study. Menopause 2018, 25, 992–1003. [Google Scholar] [CrossRef]
- Green, S.M.; Donegan, E.; Frey, B.N.; Fedorkow, D.M.; Key, B.L.; Streiner, D.L.; McCabe, R.E. Cognitive behavior therapy for menopausal symptoms (CBT-Meno): A randomized controlled trial. Menopause 2019, 26, 972–980. [Google Scholar] [CrossRef]
- Hachul, H.; Garcia, T.K.; Maciel, A.L.; Yagihara, F.; Tufik, S.; Bittencourt, L. Acupuncture improves sleep in postmenopause in a randomized, double-blind, placebo-controlled study. Climacteric 2013, 16, 36–40. [Google Scholar] [CrossRef]
- Ham, O.K.; Lee, B.G.; Choi, E.; Choi, S.J. Efficacy of cognitive behavioral treatment for insomnia: A randomized controlled trial. West. J. Nurs. Res. 2020, 42, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wang, Z.; Wu, H.; Yue, H.; Yin, P.; Zhang, W.; Lao, L.; Mi, Y.; Xu, S. Electroacupuncture versus sham acupuncture for perimenopausal insomnia: A randomized controlled clinical trial. Nat. Sci. Sleep. 2020, 12, 1201–1213. [Google Scholar] [CrossRef]
- Dos Reis Lucena, L.; Dos Santos-Junior, J.G.; Tufik, S.; Hachul, H. Lavender essential oil on postmenopausal women with insomnia: Double-blind randomized trial. Complement. Ther. Med. 2021, 59, 102726. [Google Scholar] [CrossRef] [PubMed]
- McCurry, S.M.; Guthrie, K.A.; Morin, C.M.; Woods, N.F.; Landis, C.A.; Ensrud, K.E.; Larson, J.C.; Joffe, H.; Cohen, L.S.; Hunt, J.R.; et al. Telephone-based cognitive behavioral therapy for insomnia in perimenopausal and postmenopausal women with vasomotor symptoms: A MsFLASH randomized clinical trial. JAMA Intern. Med. 2016, 176, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Portella, C.F.S.; Sorpreso, I.C.E.; Assis, A.D.S.M.; de Abreu, L.C.; Junior, J.M.S.; Baracat, E.C.; Moraes, S.D.A.; Tanaka, A.C.D.A. Meditation as an approach to lessen menopausal symptoms and insomnia in working women undergoing the menopausal transition period: A randomized controlled trial. Adv. Integr. Med. 2021, 8, 278–284. [Google Scholar] [CrossRef]
- Fu, C.; Zhao, N.; Liu, Z.; Yuan, L.H.; Xie, C.; Yang, W.J.; Yu, X.T.; Yu, H.; Chen, Y.F. Acupuncture improves peri-menopausal insomnia: A randomized controlled trial. Sleep 2017, 40, zsx153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadayon, M.; Abedi, P.; Farshadbakht, F. Impact of pedometer-based walking on menopausal women’s sleep quality: A randomized controlled trial. Climacteric 2016, 19, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Afonso, R.F.; Hachul, H.; Kozasa, E.H.; Oliveira, D.S.; Goto, V.; Rodrigues, D.; Tufik, S.; Leite, J.R. Yoga decreases insomnia in postmenopausal women: A randomized clinical trial. Menopause 2012, 19, 186–193. [Google Scholar] [CrossRef]
- Lee, B.; Shon, Y. The effects of statistical artifacts on outcomes in meta-analysis: The comparative analysis of Hedges-Olkin and Hunter-Schmidt meta-analysis approaches. Health Comm. Res. 2016, 15, 47–97. [Google Scholar]
- Chan, J.S.K.; Harky, A. The importance of risk of bias assessment in meta-analysis: Does controlling heterogeneity suffice? Eur. J. Cardiothorac. Surg. 2020, 58, 1102. [Google Scholar] [CrossRef]
- Johnson, A.; Roberts, L.; Elkins, G. Complementary and alternative medicine for menopause. J. Evid. Based Integr. Med. 2019, 24, 2515690X19829380. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Hyyppä, M.T.; Kronholm, E. Quality of sleep and chronic illnesses. J. Clin. Epidemiol. 1989, 42, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Arias, J.Á.; Marín-Cascales, E.; Ramos-Campo, D.J.; Hernandez, A.V.; Pérez-López, F.R. Effect of exercise on sleep quality and insomnia in middle-aged women: A systematic review and meta-analysis of randomized controlled trials. Maturitas 2017, 100, 49–56. [Google Scholar] [CrossRef]
- Wang, Z.; Zhai, F.; Zhao, X.; Zhao, G.; Li, N.; Zhang, F.; Liu, J. The efficacy and safety of acupuncture for perimenopausal insomnia: A protocol for a network meta-analysis. Medicine 2020, 99, e23741. [Google Scholar] [CrossRef]
- Owais, S.; Chow, C.H.T.; Furtado, M.; Frey, B.N.; Van Lieshout, R.J. Non-pharmacological interventions for improving postpartum maternal sleep: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 41, 87–100. [Google Scholar] [CrossRef]
- Chiu, H.Y.; Hsieh, Y.J.; Tasi, P.S. Accupuncture to reduce sleep disturbances in perimenopausal and postmenopausal women: A systemic review and meta-analysis. Obstet. Gynecol. 2016, 127, 507–515. [Google Scholar] [CrossRef]
- Liu, C.; Xi, H.; Wu, W.; Wang, X.; Qin, S.; Zhao, Y.; Zheng, S.; Wan, Q.; Xu, L. Placebo effect of acupuncture on insomnia: A systematic review and meta-analysis. Ann. Palliat. Med. 2020, 9, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, R.; Zee, P.; Lutsey, P.L.; Javaheri, S.; Alcántara, C.; Jackson, C.L.; Williams, M.A.; Redline, S. Racial/ethnic differences in sleep disturbances: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2015, 38, 877–888. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Greendale, G.; Crawford, S.L.; Avis, N.E.; Brooks, M.M.; Thurston, R.C.; Karvonen-Gutierrez, C.; Waetjen, L.E.; Matthews, K. The menopause transition and women’s health at midlife: A progress report from the Study of Women’s Health Across the Nation (SWAN). Menopause 2019, 26, 1213–1227. [Google Scholar] [CrossRef]
- Jang, S.J. Research trends in education for students with ADHD: A review of research from 1999 to 2008. Korean J. Special. Edu. 2010, 44, 259–291. [Google Scholar]
- Kim, J.H.; Oh, P.J. Effects of non-pharmacological interventions on primary insomnia in adults aged 55 and above: A meta-analysis. Korean J. Adult. Nurs. 2016, 28, 13–29. [Google Scholar] [CrossRef] [Green Version]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disturbances and chronic disease in older adults: Results of the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Lee, M.H.; Choi, J.W.; Kim, S.; Kim, J.; Lee, Y.J. Survey of insomnia treatment status for doctors. Sleep Med. Psychophysiol. 2016, 23, 77–83. [Google Scholar] [CrossRef]
- Lee, G.I.; Jeon, J.J.; Hahm, S.C. A comparison of the effects of barefoot walking and sneakers walking on a sandy beach on pain, disability, motor function, sleep satisfaction, and quality of life in the elderly with low back pain. J. Korean Soc. Integr. Med. 2020, 8, 29–38. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Country | Subjects | Interventions | Outcome Measure | Outcomes | Risk of Bias Summary | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Age (Year) | Sample Size (n) | ||||||||||||||
| Type of Intervention and Control Group | Length (min) | Session | Duration (Weeks) | R | D | M1 | M2 | S | O | ||||||
| Abedian (2015) | Iran | Exp1 = 50.7 Exp2 = 51.3 Cont = 51.4 | Exp1 = 37 Exp2 = 36 Cont = 32 | Exp1 = acupuncture Exp2 = sham acupuncture Cont = no intervention | 10 10 | 24 24 | 4 4 | PSQI | The total score of PSQI improved: Exp1 vs. Cont (p < 0.001); Exp1 vs. Exp2 (p < 0.001) | Ⓢ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓢ |
| Ahmadinezhad (2017) | Iran | 54.1 | Exp1 = 36 Exp2 = 36 Cont = 36 | Exp1 = Pilates Exp = acupuncture Cont = no intervention | 60 NA | 18 18 | 6 6 | PSQI | The total score of PSQI improved: Exp1 vs. Cont (p < 0.001); Exp2 vs. Cont (p < 0.001) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Aibar-Almazan (2019) | Spain | Exp = 70.0 Cont = 66.8 | Exp = 52 Cont = 55 | Exp = Pilates Cont = no intervention | 60 | 24 | 12 | PSQI | The total score of PSQI improved: Exp vs. Cont (p < 0.001) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Alfonso (2012) | Brazil | Exp1 = 50.7 Exp2 = 50.7 Cont = 51.4 | Exp1 = 15 Exp2 = 14 Cont = 15 | Exp1 = yoga Exp2 = passive stretching Cont = no intervention | 120 60 | 32 16 | 16 16 | ISI | The total score of ISI improved: Exp1 vs. Cont (p < 0.05); Exp2 vs. Cont (p < 0.05) | Ⓛ | Ⓛ | Ⓛ | Ⓢ | Ⓛ | Ⓢ |
| Elavsky (2007) | USA | 49.9 | Exp1 = 63 Exp2 = 61 Cont = 39 | Exp1 = walking Exp2 = yoga Cont = wait-list | 60 90 | 48 32 | 16 16 | PSQI | The total score of PSQI did not improve results significantly | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Garcia (2018) | Brazil | Exp = 55.2 Cont = 56.7 | Exp = 19 Cont = 11 | Exp = meditation Cont = usual counseling | 30 | 8 | 8 | PSQI, ISI | The total score of PSQI and ISI improved: Exp vs. Cont (p = 0.010) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Green (2019) | Canada | Exp = 53.3 Cont = 52.9 | Exp = 37 Cont = 34 | Exp = CBT Cont = wait-list | 120 | 12 | 12 | PSQI | The total score of PSQI improved: Exp vs. Cont (p = 0.001) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Hachul (2013) | Brazil | Exp = 58.0 Cont = 59.8 | Exp = 9 Cont = 9 | Exp = acupuncture Cont = sham acupuncture | NA | 10 | 5 | PSQI | The total score of PSQI improved: Exp1 vs. Cont (p < 0.001) | Ⓗ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓗ |
| Ham (2020) | South Korea | Exp = 53.8 Cont = 55.5 | Exp = 28 Cont = 30 | Exp = CBT Cont = usual education | 30–60 | 5 | 4 | PSQI, ISI | The total score of PSQI and ISI improved: Exp vs. Cont (p < 0.05) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Lee (2020) | China | Exp = 52.1 Cont = 53.1 | Exp = 42 Cont = 42 | Exp = acupuncture Cont = sham acupuncture | NA | 18 | 8 | PSQI | The total score of PSQI improved: Exp1 vs. Cont (p < 0.001) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Lucena (2021) | Brazil | Exp = 56.7 Cont = 55.9 | Exp = 17 Cont = 18 | Exp = aromatherapy Cont = placebo | NA | 28 | 4 | PSQI, ISI | The total score of PSQI and ISI improved: no statistically significant findings; Exp vs. Cont (p = 0.220) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| McCurry (2016) | USA | Exp = 55.0 Cont = 54.7 | Exp = 53 Cont = 53 | Exp = CBT Cont = usual education | 20–30 | 6 | 8 | PSQI, ISI | The total score of PSQI and ISI improved: Exp vs. Cont (p < 0.001) | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ | Ⓛ |
| Portella (2021) | Brazil | Exp = 46.7 Cont = 48.6 | Exp = 18 Cont = 15 | Exp = meditation + sleep hygiene Cont = sleep hygiene | 45 | 56 | 8 | PSQI, ISI | The total score of PSQI and ISI did not improve: Exp vs. Cont (p = 0.492) in PSQI Exp vs. Cont (p = 0.278) in ISI | Ⓢ | Ⓛ | Ⓛ | Ⓢ | Ⓛ | Ⓢ |
| Pu (2017) | China | Exp = 52.0 Cont = 52.5 | Exp = 37 Cont = 37 | Exp = acupuncture Cont = sham acupuncture | NA | 10 | 3 | PSQI, ISI | The total score of PSQI and ISI improved: Exp vs. Cont (p < 0.01) | Ⓛ | Ⓛ | Ⓗ | Ⓛ | Ⓢ | Ⓗ |
| Tadayon (2016) | Iran | Exp = 52.3 Cont = 52.5 | Exp = 56 Cont = 56 | Exp = walking Cont = no intervention | NA | NA | 12 | PSQI | The total score of PSQI improved: Exp1 vs. Cont (p = 0.001) | Ⓗ | Ⓛ | Ⓛ | Ⓗ | Ⓢ | Ⓗ |
| Categorical Modulators | PSQI | ISI | ||||||
|---|---|---|---|---|---|---|---|---|
| N | ES | 95% CI | p | N | ES | 95% CI | p | |
| Type of intervention | ||||||||
| Acupuncture | 5 | −2.11 | −3.04, −1.17 | 0.392 | 1 | −1.81 | −6.18, 2.55 | 0.624 |
| Pilates | 2 | −1.78 | −3.22, −0.33 | |||||
| Exercise | 2 | −0.90 | −2.32, 0.52 | |||||
| Yoga | 1 | −0.11 | −2.11, 1.90 | 1 | −0.61 | −4.99, 3.79 | ||
| Meditation | 2 | −3.24 | −2.86, 0.21 | 2 | −2.45 | −5.62, −0.72 | ||
| CBT | 3 | −0.61 | −1.78, 0.56 | 2 | −0.66 | −3.74, 2.43 | ||
| Aromatherapy | 1 | −1.16 | −3.26, 0.93 | 1 | −0.65 | −5.04, 3.73 | ||
| Study region | ||||||||
| Asia | 7 | −1.94 | −2.59, −1.30 | 0.010 * | 2 | −1.12 | −3.28, 1.05 | 0.866 |
| Western | 9 | −0.81 | −1.39, −0.23 | 5 | −1.34 | −2.74, 0.06 | ||
| Control type | ||||||||
| No intervention | 8 | −1.36 | −2.11, −0.61 | 0.664 | 1 | −0.61 | −4.09, 2.88 | 0.906 |
| Other | 4 | −0.96 | −2.05, 0.14 | 4 | −1.49 | −3.25, 0.27 | ||
| Placebo | 4 | −1.67 | −2.77, −0.57 | 2 | −1.24 | −3.69, 1.21 | ||
| Continuous modulators | ||||||||
| Sample size | 16 | −0.01, 0.06 | 0.169 | 7 | −0.09, 0.10 | 0.910 | ||
| Duration of intervention | 16 | 0.03, 0.25 | 0.010 * | 7 | −0.27, 0.30 | 0.903 | ||
| Total length of class | 9 | 0.00, 0.01 | 0.019 * | 5 | −0.01, 0.00 | 0.441 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, B.; Kim, J.; So, W.-Y.; Kim, S. Effects of Nonpharmacological Interventions on Sleep Quality and Insomnia in Perimenopausal and Postmenopausal Women: A Meta-Analysis. Healthcare 2023, 11, 327. https://doi.org/10.3390/healthcare11030327
Ha B, Kim J, So W-Y, Kim S. Effects of Nonpharmacological Interventions on Sleep Quality and Insomnia in Perimenopausal and Postmenopausal Women: A Meta-Analysis. Healthcare. 2023; 11(3):327. https://doi.org/10.3390/healthcare11030327
Chicago/Turabian StyleHa, Beomman, Jisoon Kim, Wi-Young So, and Seonho Kim. 2023. "Effects of Nonpharmacological Interventions on Sleep Quality and Insomnia in Perimenopausal and Postmenopausal Women: A Meta-Analysis" Healthcare 11, no. 3: 327. https://doi.org/10.3390/healthcare11030327