
Content, Mechanism, and Outcome of Effective Telehealth Solutions for Management of Chronic Obstructive Pulmonary Diseases: A Narrative Review


Abstract
:1. Introduction
2. Methods
3. Results
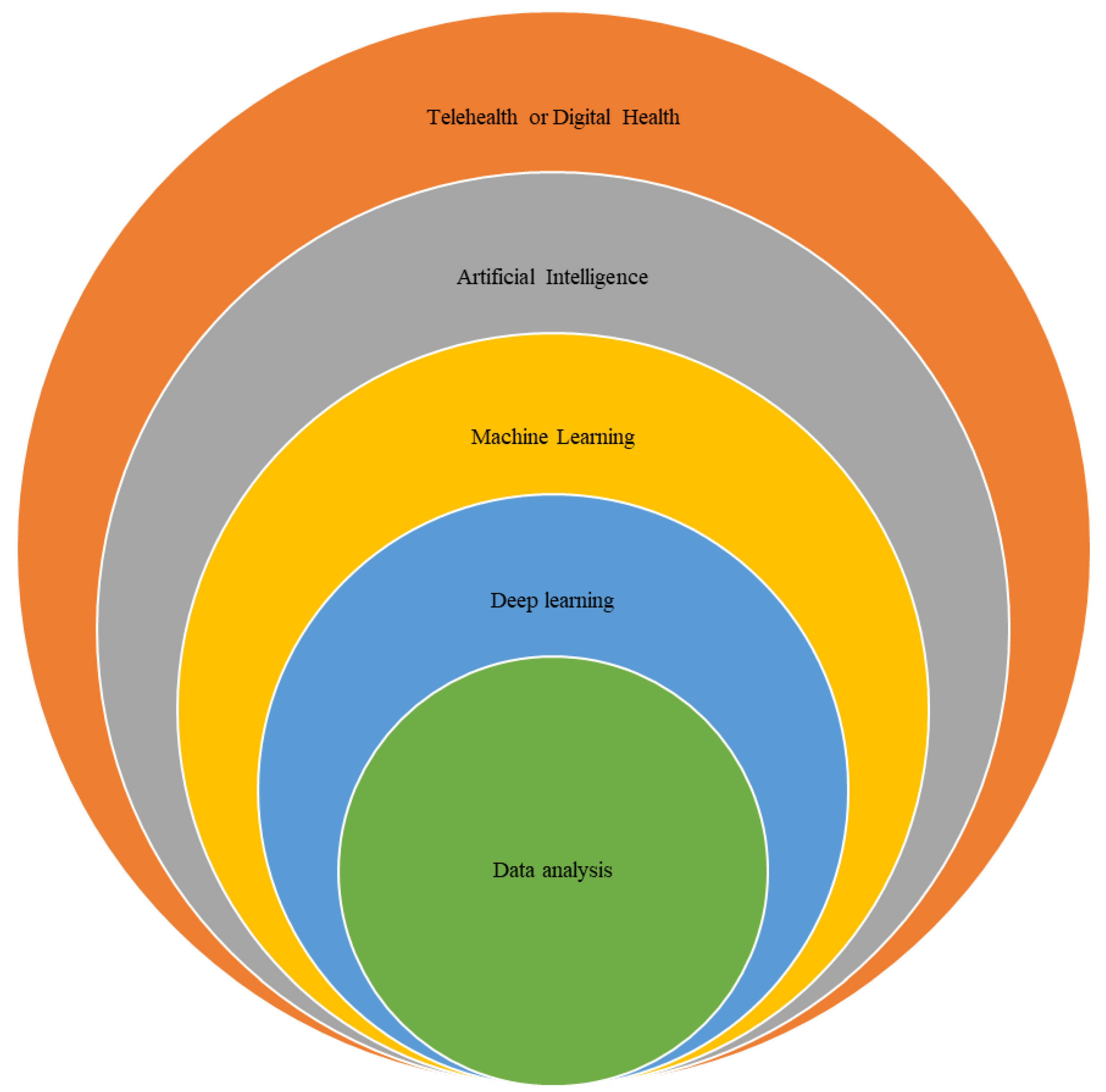
3.1. Digital Solutions in Healthcare Services
3.2. Benefits of TH with COPD Management
3.3. Structures of TH Solutions
3.4. Context of Digital Health Solutions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Settings | Intervention with TH | Mode of Delivery | Intensity | Control Group Treatment | Summary of TH Outcomes Compared to Control Group |
|---|---|---|---|---|---|---|
| Trappenburg et al., 2008 [24] | Patient home (n = 165) | Software COPD self-management education | Telephone | 1×/day for 6 months | Usual care | Reduction in AECOPD and hospitalization |
| Koff et al., 2009 [25] | Patient home (n = 40) | Online COPD self- management education | Web-based and telephone | 1×/day for 3 months | Usual care | Improved quality of life |
| Halpin et al., 2011 [26] | Patient home (n = 79) | Automated text messages system | Text message | 1×/day for 4 months | NR | Lower AECOPD but no change in quality of life |
| Lewis et al., 2011 [27] | Patient home (n = 40) | Home monitoring | Telephone | 2×/day for 6 months | Usual care | No difference in hospitalization or length of stay |
| Stickland et al., 2011 [25] | Community center (n = 409) | Online COPD self- management education | Web-based and video calls | 2×/week | In-person rehabilitation | Improvements in quality of life |
| Antoniades et al., 2012 [9] | Patient home (n = 44) | Online COPD self-management education | Web-based | 1×/day for 12 months | Usual care | No reduction in hospitalization or improvement in quality of life |
| Chau et al., 2012 [28] | Patient home (n = 40) | Telecare services | Web-based and telephone | 3×/day for 2 months | Community services | No difference in health-related quality of life |
| Dinesen et al., 2012 [29] | Patient home (n = 111) | Telerehabilitation | Video calls | 1×/day for 4 months | Instructional book | Reduced hospitalization |
| Nield et al., 2012 [30] | Patient home (n = 22) | Online COPD self- management education | Video calls | 1×/week for 1 month | Usual care and in-person education | Decreased dyspnea |
| De San Miguel et al., 2013 [31] | Patient home (n = 80) | Written COPD self- management education | Telephone | 1×/day for 6 months | Usual care | Reduced hospitalization and length of stay |
| Pedone et al., 2013 [32] | Patient home (n = 99) | Telemonitoring | Web-based, telephone, and algorithm | 1×/day for 9 months | Usual care | Reduced respiratory events and hospitalization |
| Pinnock et al., 2013 [33] | Patient home (n = 256) | Online COPD self- management education | Web-based, telephone, and algorithm | 1×/day for 12 months | Usual care | Reduced admission to hospital but no change in quality of life |
| Schou et al., 2013 [34] | Patient home (n = 44) | NR | Video calls | 1× /day for 3 months | Regular Hospitalization. | Improvements in lung volumes and oxygen saturation |
| Calvo et al., 2014 [17] | Patient home Medical center (n = 60) | Home care with TH | Web-based and telephone | 1×/day for 7 months | Usual care | Reduction in ER visits, hospitalization, and length of stay |
| Tabak et al., 2014 [35] | Patient home (n = 29) | Online COPD self- management education | Web-based and Video calls | 1×/day for 9 months | Usual care | Increased patient adherence to exercise |
| Berkhof et al., 2015 [36] | Medical center & patient home (n = 101) | Phonecalls, education and follow ups | Telephone | Call/2 weeks for 6 months | Usual care | No improvements in health status |
| Jakobsen et al., 2015 [6] | Patient home (n = 57) | Virtual hospital | NR | 1×/day for 6 months | Regular hospitalization | Reduced re-admission to hospital due to AECOPD |
| McDowell, 2015 [37] | Patient home (n = 110) | Home-based health care | Telephone | 1×/day for 6 months | Usual care | Improved health related quality of life. |
| Ringbeak et al., 2015 [38] | Patient home (n = 281) | Online COPD self- management education and home exercise | Video calls | 3×/week for 6 months | Usual care | No change in dropout or mortality |
| Tucker et al., 2016 [39] | Patient Home (n = 65) | Written home exercise with TH | Telephone | Call/2 weeks | Usual care | Improvement in physical activity |
| Ho et al., 2016 [40] | Patient home (n = 106) | Telemonitoring | Web-based and telephone | 1×/day for 2 months | Usual care | Reduced number of hospitalizations due to AECOPD |
| Ringbeak et al., 2016 [41] | Patient home and outpatient (n = 116) | Online COPD self- management education and home exercise | Web-based, video calls | NR | In-person rehabilitation | Improved physical capacity but no improvement in CAT score. |
| Vianello et al., 2016 [42] | Hospital (n = 334) | Online COPD self-management education | Web-based and telephone | 1×/day for 12 months | Usual care | Reduced readmission rate due to AECOPD |
| Farmer et al., 2017 [43] | Patient home (n = 116) | COPD self-management education with TH | Web-based | 1×/day for 12 months | COPD self- Management education without TH | Improved health status and quality of life |
| Lilholt et al., 2017 [44] | Patient home and community center (n = 1225) | Telerehabilitation | Web-based, and telephone | NR | In-person rehabilitation | No difference in quality of life |
| Shany et al. ,2017 [45] | Patient home (n = 42) | Online COPD self- management education | Web-based and telephone | 1×/day for 12 months | Home care | Reduction in hospitalization and length of stay |
| Tsai et al., 2017 [46] | Patient home (n = 37) | Online COPD self- management education and home exercise | Video calls | 3×/week | Usual PR | Improvements in physical capacity and quality of life |
| Soruano et al., 2018 [47] | Patient home (n = 237) | Telemonitoring | Internet modem | 1×/day for 12 months | Usual care | TH did not reduce hospitalization due to AECOPD |
| Jolly et al., 2019 [48] | Patient home (n = 58) | Multimedia COPD self- management education and telephone coaching | Telephone | 1×/day for 12 months | Usual care | Improvement in uptake in PR program |
| Jiang et al., 2020 [49] | Patient home (n = 106) | TelePR program | 3×/week for 6 months | Usual PR | No difference in symptoms score between TelePR and UC | |
| Rassouli et al., 2021 [50] | Patients home (n = 168) | Online COPD self- management education | Web-based and telephone | 5×/week for 6 months | Usual care | TH use improved CAT score and satisfaction with care. |
| Zanaboni et al., 2022 [51] | Patients home (n = 120) | TelePR | Video calls | 3×/week for 2 years | Treadmill at home | TH redued hospitalization. |
| Polo et al., 2023 [52] | Hospital and participants’ home (n = 209) | COPD TelePR program | Zoom and web-conferencing | 2×/week for 2 months | Usual PR | TH improved COPD symptoms, fatigue, self- management, and lung volumes. |
3.4.1. Clinical Settings
3.4.2. Digital Health Solutions Development
3.5. Mechanism
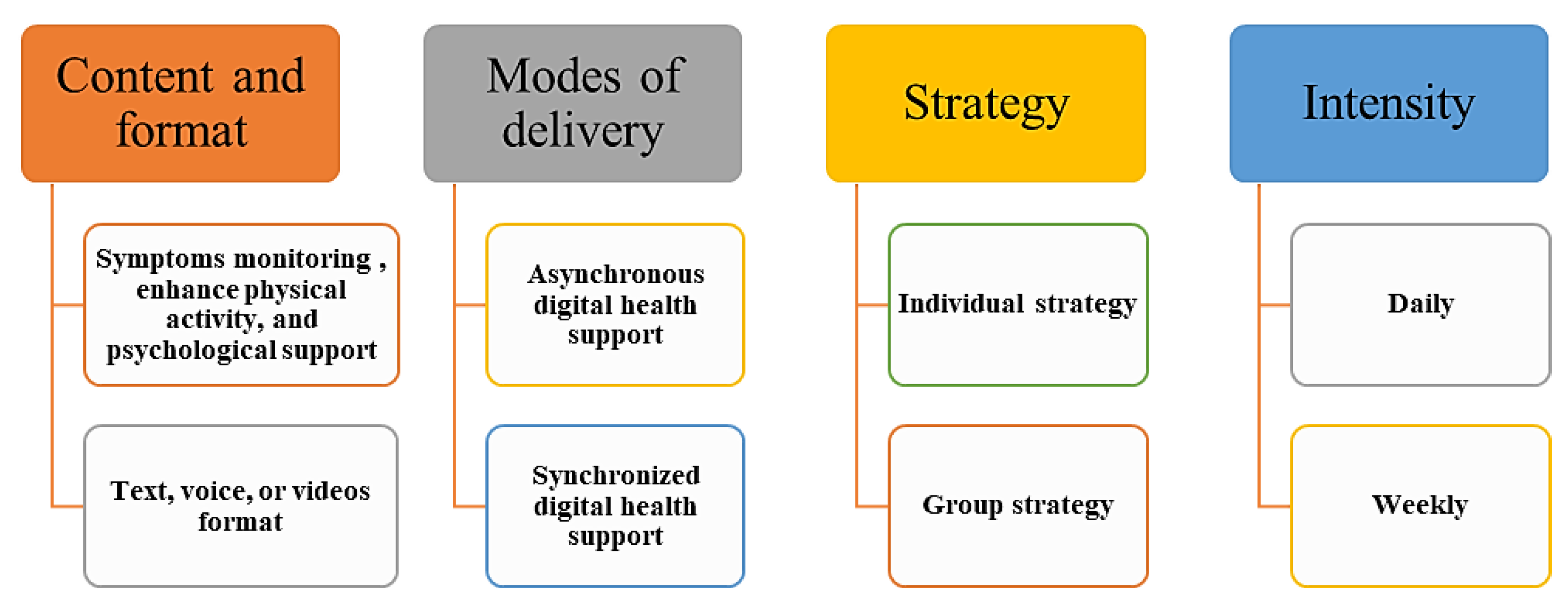
3.5.1. Content
3.5.2. Mode of Delivery
3.5.3. Strategy of Delivering Digital Health Support
- Individual strategy
- Group strategy
3.6. Intensity
Duration and Frequency
3.7. Health Outcomes
3.8. Determinants of TH Solutions
3.9. Other Promising Applications for TH in COPD Care
4. Discussion and Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Venkatesan, P. GOLD report: 2022 update. Lancet Respir. Med. 2022, 10, e20. [Google Scholar] [CrossRef]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; Montes de Oca, M. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef]
- Ur Rehman, A.; Hassali, M.A.A.; Abbas, S.; Ali, I.A.B.H.; Harun, S.N.; Muneswarao, J.; Hussain, R. Pharmacological and non-pharmacological management of COPD; limitations and future prospects: A review of current literature. J. Public Health 2020, 28, 357–366. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Alghamdi, S.M.; Aldhahir, A.M.; Althobiani, M.; Oyelade, T. Key toolkits of non-pharmacological management in COPD: During and beyond COVID-19. Front. Biosci. 2021, 26, 246–252. [Google Scholar] [CrossRef]
- Criner, G.J.; Bourbeau, J.; Diekemper, R.L.; Ouellette, D.R.; Goodridge, D.; Hernandez, P.; Curren, K.; Balter, M.S.; Bhutani, M.; Camp, P.G.; et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest 2015, 147, 894–942. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, A.S.; Laursen, L.C.; Rydahl-Hansen, S.; Ostergaard, B.; Gerds, T.A.; Emme, C.; Schou, L.; Phanareth, K. Home-Based Telehealth Hospitalization for Exacerbation of Chronic Obstructive Pulmonary Disease: Findings from “The Virtual Hospital” Trial. Telemed. E-Health 2015, 21, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Effing, T.W.; Vercoulen, J.H.; Bourbeau, J.; Trappenburg, J.; Lenferink, A.; Cafarella, P.; Coultas, D.; Meek, P.; van der Valk, P.; Bischoff, E.W.; et al. Definition of a COPD self-management intervention: International Expert Group consensus. Eur. Respir. J. 2016, 48, 46–54. [Google Scholar] [CrossRef]
- Zwerink, M.; Brusse-Keizer, M.; van der Valk, P.D.; Zielhuis, G.A.; Monninkhof, E.M.; van der Palen, J.; Frith, P.A.; Effing, T. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014, 2014, CD002990. [Google Scholar] [CrossRef] [PubMed]
- Antoniades, N.C.; Rochford, P.D.; Pretto, J.J.; Pierce, R.J.; Gogler, J.; Steinkrug, J.; Sharpe, K.; McDonald, C.F. Pilot study of remote telemonitoring in COPD. Telemed. J. E Health 2012, 18, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, S.M.; Alqahtani, J.S.; Aldhahir, A.M. Current status of telehealth in Saudi Arabia during COVID-19. J. Fam. Community Med. 2020, 27, 208–211. [Google Scholar] [CrossRef]
- Currell, R.; Urquhart, C.; Wainwright, P.; Lewis, R. Telemedicine versus face to face patient care: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2000, 2000, CD002098. [Google Scholar] [CrossRef]
- Alghamdi, S.M.; Rajah, A.M.A.; Aldabayan, Y.S.; Aldhahir, A.M.; Alqahtani, J.S.; Alzahrani, A.A. Chronic Obstructive Pulmonary Disease Patients’ Acceptance in E-Health Clinical Trials. Int. J. Environ. Res. Public Health 2021, 18, 5230. [Google Scholar] [CrossRef]
- Shaw, D.K.; Heggestad-Hereford, J.R.; Southard, D.R.; Sparks, K.E. American Association of Cardiovascular and Pulmonary Rehabilitation telemedicine position statement. J. Cardiopulm. Rehabil. 2001, 21, 261–262. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, S.M.; Alsulayyim, A.S.; Alqahtani, J.S.; Aldhahir, A.M. Digital Health Platforms in Saudi Arabia: Determinants from the COVID-19 Pandemic Experience. Healthcare 2021, 9, 1517. [Google Scholar] [CrossRef] [PubMed]
- Joseph, V.; West, R.M.; Shickle, D.; Keen, J.; Clamp, S. Key challenges in the development and implementation of telehealth projects. J. Telemed. Telecare 2011, 17, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Inskip, J.A.; Lauscher, H.N.; Li, L.C.; Dumont, G.A.; Garde, A.; Ho, K.; Hoens, A.M.; Road, J.D.; Ryerson, C.J.; Camp, P.G. Patient and health care professional perspectives on using telehealth to deliver pulmonary rehabilitation. Chronic Respir. Dis. 2018, 15, 71–80. [Google Scholar] [CrossRef]
- Calvo, G.S.; Gómez-Suárez, C.; Soriano, J.B.; Zamora, E.; Gónzatez-Gamarra, A.; González-Béjar, M.; Jordán, A.; Tadeo, E.; Sebastián, A.; Fernández, G.; et al. A home telehealth program for patients with severe COPD: The PROMETE study. Respir. Med. 2014, 108, 453–462. [Google Scholar] [CrossRef]
- Nguyen, H.Q.; Gill, D.P.; Wolpin, S.; Steele, B.G.; Benditt, J.O. Pilot study of a cell phone-based exercise persistence intervention post-rehabilitation for COPD. Int. J. Chronic Obs. Pulm. Dis. 2009, 4, 301–313. [Google Scholar] [CrossRef]
- Barlow, J. Managing Innovation in Healthcare; World Scientific Publishing Company: Singapore, 2016. [Google Scholar]
- Jonkman, N.H.; Westland, H.; Trappenburg, J.C.; Groenwold, R.H.; Bischoff, E.W.; Bourbeau, J.; Bucknall, C.E.; Coultas, D.; Effing, T.W.; Epton, M.; et al. Characteristics of effective self-management interventions in patients with COPD: Individual patient data meta-analysis. Eur. Respir. J. 2016, 48, 55–68. [Google Scholar] [CrossRef]
- Newham, J.J.; Presseau, J.; Heslop-Marshall, K.; Russell, S.; Ogunbayo, O.J.; Netts, P.; Hanratty, B.; Kaner, E. Features of self-management interventions for people with COPD associated with improved health-related quality of life and reduced emergency department visits: A systematic review and meta-analysis. Int. J. Chronic Obs. Pulmon Dis. 2017, 12, 1705–1720. [Google Scholar] [CrossRef]
- Alghamdi, S.M.; Alqahtani, J.S.; Aldhahir, A.M.; Alrajeh, A.M.; Aldabayan, Y.S. Effectiveness of Telehealth-Based Interventions with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Am. J. Respir. Crit. Care Med. 2020, 201, A4308. [Google Scholar]
- Alghamdi, S.M.; Al Rajeh, A. Top Ten Behavioral Change Techniques Used in Telehealth Intervention with COPD: A Systematic Review. Respir. Care 2019, 64, 3229948. [Google Scholar]
- Trappenburg, J.C.; Niesink, A.; de Weert-van Oene, G.H.; van der Zeijden, H.; van Snippenburg, R.; Peters, A.; Lammers, J.W.; Schrijvers, A.J. Effects of telemonitoring in patients with chronic obstructive pulmonary disease. Telemed. J. E Health 2008, 14, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Koff, P.B.; Jones, R.H.; Cashman, J.M.; Voelkel, N.F.; Vandivier, R.W. Proactive integrated care improves quality of life in patients with COPD. Eur. Respir. J. 2009, 33, 1031–1038. [Google Scholar] [CrossRef]
- Halpin, D.M.; Laing-Morton, T.; Spedding, S.; Levy, M.L.; Coyle, P.; Lewis, J.; Newbold, P.; Marno, P. A randomised controlled trial of the effect of automated interactive calling combined with a health risk forecast on frequency and severity of exacerbations of COPD assessed clinically and using EXACT PRO. Prim. Care Respir. J. 2011, 20, 324–331. [Google Scholar] [CrossRef]
- Lewis, K.E.; Annandale, J.A.; Warm, D.L.; Rees, S.E.; Hurlin, C.; Blyth, H.; Syed, Y.; Lewis, L. Does home telemonitoring after pulmonary rehabilitation reduce healthcare use in optimized COPD? A pilot randomized trial. COPD 2010, 7, 44–50. [Google Scholar] [CrossRef]
- Chau, J.P.; Lee, D.T.; Yu, D.S.; Chow, A.Y.; Yu, W.C.; Chair, S.Y.; Lai, A.S.; Chick, Y.L. A feasibility study to investigate the acceptability and potential effectiveness of a telecare service for older people with chronic obstructive pulmonary disease. Int. J. Med. Inform. 2012, 81, 674–682. [Google Scholar] [CrossRef]
- Dinesen, B.; Haesum, L.K.; Soerensen, N.; Nielsen, C.; Grann, O.; Hejlesen, O.; Toft, E.; Ehlers, L. Using preventive home monitoring to reduce hospital admission rates and reduce costs: A case study of telehealth among chronic obstructive pulmonary disease patients. J. Telemed. Telecare 2012, 18, 221–225. [Google Scholar] [CrossRef]
- Nield, M.; Hoo, G.W. Real-time telehealth for COPD self-management using Skype. COPD 2012, 9, 611–619. [Google Scholar] [CrossRef]
- De San Miguel, K.; Smith, J.; Lewin, G. Telehealth remote monitoring for community-dwelling older adults with chronic obstructive pulmonary disease. Telemed. E-Health 2013, 19, 652–657. [Google Scholar] [CrossRef]
- Pedone, C.; Chiurco, D.; Scarlata, S.; Incalzi, R.A. Efficacy of multiparametric telemonitoring on respiratory outcomes in elderly people with COPD: A randomized controlled trial. BMC Health Serv. Res. 2013, 13, 82. [Google Scholar] [CrossRef]
- Pinnock, H.; Hanley, J.; McCloughan, L.; Todd, A.; Krishan, A.; Lewis, S.; Stoddart, A.; van der Pol, M.; MacNee, W.; Sheikh, A.; et al. Effectiveness of telemonitoring integrated into existing clinical services on hospital admission for exacerbation of chronic obstructive pulmonary disease: Researcher blind, multicentre, randomised controlled trial. BMJ-Br. Med. J. 2013, 347, f6070. [Google Scholar] [CrossRef]
- Schou, L.; Ostergaard, B.; Rydahl-Hansen, S.; Rasmussen, L.S.; Emme, C.; Jakobsen, A.S.; Phanareth, K. A randomised trial of telemedicine-based treatment versus conventional hospitalisation in patients with severe COPD and exacerbation—Effect on self-reported outcome. J. Telemed. Telecare 2013, 19, 160–165. [Google Scholar] [CrossRef]
- Tabak, M.; Brusse-Keizer, M.; van der Valk, P.; Hermens, H.; Vollenbroek-Hutten, M. A telehealth program for self-management of COPD exacerbations and promotion of an active lifestyle: A pilot randomized controlled trial. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Berkhof, F.F.; van den Berg, J.W.; Uil, S.M.; Kerstjens, H.A. Telemedicine, the effect of nurse-initiated telephone follow up, on health status and health-care utilization in COPD patients: A randomized trial. Respirology 2015, 20, 279–285. [Google Scholar] [CrossRef] [PubMed]
- McDowell, J.E.; McClean, S.; FitzGibbon, F.; Tate, S. A randomised clinical trial of the effectiveness of home-based health care with telemonitoring in patients with COPD. J. Telemed. Telecare 2015, 21, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Ringbaek, T.; Green, A.; Laursen, L.C.; Frausing, E.; Brondum, E.; Ulrik, C.S. Effect of tele health care on exacerbations and hospital admissions in patients with chronic obstructive pulmonary disease: A randomized clinical trial. Int. J. Chronic Obs. Pulm. Dis. 2015, 10, 1801–1808. [Google Scholar] [CrossRef]
- Cameron-Tucker, H.L.; Wood-Baker, R.; Joseph, L.; Walters, J.A.; Schüz, N.; Walters, E.H. A randomized controlled trial of telephone-mentoring with home-based walking preceding rehabilitation in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1991–2000. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.-W.; Huang, C.-T.; Chiu, H.-C.; Ruan, S.-Y.; Tsai, Y.-J.; Yu, C.-J.; Lai, F.; Lin, Y.-F.; Tsai, H.-B.; Hsu, N.-C.; et al. Effectiveness of telemonitoring in patients with chronic obstructive pulmonary disease in Taiwan-a randomized controlled trial. Sci. Rep. 2016, 6, 23797. [Google Scholar] [CrossRef] [PubMed]
- Ringbaek, T.J.; Lavesen, M.; Lange, P. Tablet computers to support outpatient pulmonary rehabilitation in patients with COPD. Eur. Clin. Respir. J. 2016, 3, 31016. [Google Scholar] [CrossRef]
- Vianello, A.; Fusello, M.; Gubian, L.; Rinaldo, C.; Dario, C.; Concas, A.; Saccavini, C.; Battistella, L.; Pellizzon, G.; Zanardi, G. Home telemonitoring for patients with acute exacerbation of chronic obstructive pulmonary disease: A randomized controlled trial. BMC Pulm. Med. 2016, 16, 157. [Google Scholar] [CrossRef]
- Farmer, A.; Williams, V.; Velardo, C.; Shah, S.A.; Yu, L.M.; Rutter, H.; Jones, L.; Williams, N.; Heneghan, C.; Price, J.; et al. Self-Management Support Using a Digital Health System Compared With Usual Care for Chronic Obstructive Pulmonary Disease: Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e144. [Google Scholar] [CrossRef]
- Lilholt, P.H.; Udsen, F.W.; Ehlers, L.; Hejlesen, O.K. Telehealthcare for patients suffering from chronic obstructive pulmonary disease: Effects on health-related quality of life: Results from the Danish ‘TeleCare North’cluster-randomised trial. BMJ Open 2017, 7, e014587. [Google Scholar] [CrossRef]
- Shany, T.; Hession, M.; Pryce, D.; Roberts, M.; Basilakis, J.; Redmond, S.; Lovell, N.; Schreier, G. A small-scale randomised controlled trial of home telemonitoring in patients with severe chronic obstructive pulmonary disease. J. Telemed. Telecare 2017, 23, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Tsai, L.L.; McNamara, R.J.; Moddel, C.; Alison, J.A.; McKenzie, D.K.; McKeough, Z.J. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: The randomized controlled TeleR Study. Respirology 2017, 22, 699–707. [Google Scholar] [CrossRef]
- Soriano, J.B.; García-Río, F.; Vázquez-Espinosa, E.; Conforto, J.I.; Hernando-Sanz, A.; López-Yepes, L.; Galera-Martínez, R.; Peces-Barba, G.; Gotera-Rivera, C.M.; Pérez-Warnisher, M.T. A multicentre, randomized controlled trial of telehealth for the management of COPD. Respir. Med. 2018, 144, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Jolly, K.; Sidhu, M.; Bower, P.; Madurasinghe, V. Improving recruitment to a study of telehealth management for COPD: A cluster randomised controlled ‘study within a trial’(SWAT) of a multimedia information resource. Trials 2019, 20, 453. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Liu, F.; Guo, J.; Sun, P.; Chen, Z.; Li, J.; Cai, L.; Zhao, H.; Gao, P.; Ding, Z. Evaluating an intervention program using WeChat for patients with chronic obstructive pulmonary disease: Randomized controlled trial. J. Med. Internet Res. 2020, 22, e17089. [Google Scholar] [CrossRef]
- Rassouli, F.; Germann, A.; Baty, F.; Kohler, M.; Stolz, D.; Thurnheer, R.; Brack, T.; Kähler, C.; Widmer, S.; Tschirren, U. Telehealth mitigates COPD disease progression compared to standard of care: A randomized controlled crossover trial. J. Intern. Med. 2021, 289, 404–410. [Google Scholar] [CrossRef]
- Zanaboni, P.; Dinesen, B.; Hoaas, H.; Wootton, R.; Burge, A.T.; Philp, R.; Oliveira, C.C.; Bondarenko, J.; Tranborg Jensen, T.; Miller, B.R. Long-term telerehabilitation or unsupervised training at home for patients with chronic obstructive pulmonary disease: A randomized controlled trial. Am. J. Respir. Crit. Care Med. 2023, 207, 865–875. [Google Scholar] [CrossRef]
- Polo, J.; Basile, M.J.; Zhang, M.; Ordonez, K.; Rodriguez, D.; Boye-Codjoe, E.; Williams, M.; Tsang, D.; Medina, R.; Jacome, S. Application of the RE-AIM framework to evaluate the implementation of telehealth pulmonary rehabilitation in a randomized controlled trial among African-American and Hispanic patients with advanced stage Chronic Obstructive Pulmonary Disease. BMC Health Serv. Res. 2023, 23, 515. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.Y.; Zhang, P. Telemedicine in clinical setting. Exp. Ther. Med. 2016, 12, 2405–2407. [Google Scholar] [CrossRef] [PubMed]
- Velardo, C.; Shah, S.A.; Gibson, O.; Clifford, G.; Heneghan, C.; Rutter, H.; Farmer, A.; Tarassenko, L.; Team, E.C. Digital health system for personalised COPD long-term management. BMC Med. Inform. Decis. Mak. 2017, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- Slevin, P. Human-Centred Recommendations to Maximise the Potential for Digital Health in the Management of Chronic Obstructive Pulmonary Disease. Ph.D. Thesis, University College Dublin, Dublin, Ireland, 2020. [Google Scholar]
- Fromer, L. Implementing chronic care for COPD: Planned visits, care coordination, and patient empowerment for improved outcomes. Int. J. Chronic Obs. Pulmon Dis. 2011, 6, 605–614. [Google Scholar] [CrossRef]
- Sorknaes, A.D.; Bech, M.; Madsen, H.; Titlestad, I.L.; Hounsgaard, L.; Hansen-Nord, M.; Jest, P.; Olesen, F.; Lauridsen, J.; Ostergaard, B. The effect of real-time teleconsultations between hospital-based nurses and patients with severe COPD discharged after an exacerbation. J. Telemed. Telecare 2013, 19, 466–474. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Mendes, R.G.; Alghamdi, S.M.; Miravitlles, M.; Mandal, S.; Hurst, J.R. Reduction in hospitalised COPD exacerbations during COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0255659. [Google Scholar] [CrossRef]
- Aldhahir, A.M.; Alqahtani, J.S.; Althobiani, M.A.; Alghamdi, S.M.; Alanazi, A.F.; Alnaim, N.; Alqarni, A.A.; Alwafi, H. Current Knowledge, Satisfaction, and Use of E-Health Mobile Application (Seha) Among the General Population of Saudi Arabia: A Cross-Sectional Study. J. Multidiscip. Health 2022, 15, 667–678. [Google Scholar] [CrossRef]
- Pare, G.; Sicotte, C.; St-Jules, D.; Gauthier, R. Cost-minimization analysis of a telehomecare program for patients with chronic obstructive pulmonary disease. Telemed. J. E Health 2006, 12, 114–121. [Google Scholar] [CrossRef]
- Eysenbach, G.; CONSORT-EHEALTH Group. CONSORT-EHEALTH: Improving and standardizing evaluation reports of Web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef]
- Marquis, N.; Larivee, P.; Saey, D.; Dubois, M.F.; Tousignant, M. In-Home Pulmonary Telerehabilitation for Patients with Chronic Obstructive Pulmonary Disease: A Pre-experimental Study on Effectiveness, Satisfaction, and Adherence. Telemed. J. E Health 2015, 21, 870–879. [Google Scholar] [CrossRef]
- British Lung Foundation. COPD (Chronic Obstructive Pulmonary Disease). 2022. Available online: https://www.blf.org.uk/support-for-you/copd (accessed on 10 October 2023).
- Lundell, S.; Toots, A.; Sonnerfors, P.; Halvarsson, A.; Wadell, K. Participatory methods in a digital setting: Experiences from the co-creation of an eHealth tool for people with chronic obstructive pulmonary disease. BMC Med. Inform. Decis. Mak. 2022, 22, 68. [Google Scholar] [CrossRef] [PubMed]
- Pearce, G.; Parke, H.L.; Pinnock, H.; Epiphaniou, E.; Bourne, C.L.; Sheikh, A.; Taylor, S.J. The PRISMS taxonomy of self-management support: Derivation of a novel taxonomy and initial testing of its utility. J. Health Serv. Res. Policy 2016, 21, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Dale, J.; Connor, S.; Tolley, K. An evaluation of the west Surrey telemedicine monitoring project. J. Telemed. Telecare 2003, 9 (Suppl. S1), S39–S41. [Google Scholar] [CrossRef]
- Wagner, F.M.; Weber, A.; Park, J.W.; Schiemanck, S.; Tugtekin, S.M.; Gulielmos, V.; Schuler, S. New telemetric system for daily pulmonary function surveillance of lung transplant recipients. Ann. Thorac. Surg. 1999, 68, 2033–2038. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.K.; Nguyen, H.Q.; Wolpin, S. Designing and Testing a Web-based Interface for Self-Monitoring of Exercise and Symptoms for Older Adults with COPD. Comput. Inform. Nurs. CIN 2009, 27, 166. [Google Scholar] [CrossRef]
- Stewart, J.I.; Moyle, S.; Criner, G.J.; Wilson, C.; Tanner, R.; Bowler, R.P.; Crapo, J.D.; Zeldin, R.K.; Make, B.J.; Regan, E.A.; et al. Automated telecommunication to obtain longitudinal follow-up in a multicenter cross-sectional COPD study. COPD 2012, 9, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Jodar-Sanchez, F.; Ortega, F.; Parra, C.; Gomez-Suarez, C.; Jordan, A.; Perez, P.; Bonachela, P.; Leal, S.; Barrot, E. Implementation of a telehealth programme for patients with severe chronic obstructive pulmonary disease treated with long-term oxygen therapy. J. Telemed. Telecare 2013, 19, 11–17. [Google Scholar] [CrossRef]
- Den Brinker, A.C.; van Dinther, R.; Crooks, M.; Thackray-Nocera, S.; Morice, A.H. Alert system design based on experimental findings from long-term unobtrusive monitoring in COPD. Biomed. Signal Process. Control 2021, 63, 102205. [Google Scholar] [CrossRef]
- Velickovski, F.; Ceccaroni, L.; Roca, J.; Burgos, F.; Galdiz, J.B.; Marina, N.; Lluch-Ariet, M. Clinical Decision Support Systems (CDSS) for preventive management of COPD patients. J. Transl. Med. 2014, 12 (Suppl. S2), S9. [Google Scholar] [CrossRef]
- Baldwin, J.L.; Singh, H.; Sittig, D.F.; Giardina, T.D. Patient portals and health apps: Pitfalls, promises, and what one might learn from the other. Healthcare 2017, 5, 81–85. [Google Scholar] [CrossRef]
- Barbosa, M.T.; Sousa, C.S.; Morais-Almeida, M.; Simoes, M.J.; Mendes, P. Telemedicine in COPD: An Overview by Topics. COPD 2020, 17, 601–617. [Google Scholar] [CrossRef] [PubMed]
- Shaw, G.; Whelan, M.E.; Armitage, L.C.; Roberts, N.; Farmer, A.J. Are COPD self-management mobile applications effective? A systematic review and meta-analysis. NPJ Prim. Care Respir. Med. 2020, 30, 11. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A.; Cao, H.; FitzGerald, J.M.; Iannotti, N.; Yang, E.; Kocks, J.W.H.; Kostikas, K.; Price, D.; Reddel, H.K.; Tsiligianni, I.; et al. Artificial Intelligence/Machine Learning in Respiratory Medicine and Potential Role in Asthma and COPD Diagnosis. J. Allergy Clin. Immunol. Pract. 2021, 9, 2255–2261. [Google Scholar] [CrossRef]
- Hasnain, M.; Hayat, A.; Hussain, A. Revolutionizing Chronic Obstructive Pulmonary Disease Care with the Open AI Application: ChatGPT. Ann. Biomed. Eng. 2023, 51, 2100–2102. [Google Scholar] [CrossRef] [PubMed]
- Franke, K.J.; Domanski, U.; Schroeder, M.; Jansen, V.; Artmann, F.; Weber, U.; Ettler, R.; Nilius, G. Telemonitoring of home exercise cycle training in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2821–2829. [Google Scholar] [CrossRef]
- Sicotte, C.; Pare, G.; Morin, S.; Potvin, J.; Moreault, M.P. Effects of home telemonitoring to support improved care for chronic obstructive pulmonary diseases. Telemed. J. E Health 2011, 17, 95–103. [Google Scholar] [CrossRef]
- Scalvini, S.; Baratti, D.; Assoni, G.; Zanardini, M.; Comini, L.; Bernocchi, P. Information and communication technology in chronic diseases: A patient’s opportunity. J. Med. Pers. 2014, 12, 91–95. [Google Scholar] [CrossRef]
- Stickland, M.; Jourdain, T.; Wong, E.Y.; Rodgers, W.M.; Jendzjowsky, N.G.; Macdonald, G.F. Using Telehealth technology to deliver pulmonary rehabilitation in chronic obstructive pulmonary disease patients. Can. Respir. J. 2011, 18, 216–220. [Google Scholar] [CrossRef]
- Alwakeel, A.J.; Sicondolfo, A.; Robitaille, C.; Bourbeau, J.; Saad, N. The Accessibility, Feasibility, and Safety of a Standardized Community-based Tele-Pulmonary Rehab Program for Chronic Obstructive Pulmonary Disease: A 3-Year Real-World Prospective Study. Ann. Am. Thorac. Soc. 2022, 19, 39–47. [Google Scholar] [CrossRef]
- Barlow, J.; Wright, C.; Sheasby, J.; Turner, A.; Hainsworth, J. Self-management approaches for people with chronic conditions: A review. Patient Educ. Couns. 2002, 48, 177–187. [Google Scholar] [CrossRef]
- Bourbeau, J. Disease-specific self-management programs in patients with advanced chronic obstructive pulmonary disease—A comprehensive and critical evaluation. Dis. Manag. Health Out. 2003, 11, 311–319. [Google Scholar] [CrossRef]
- Vassilev, I.; Rowsell, A.; Pope, C.; Kennedy, A.; O’Cathain, A.; Salisbury, C.; Rogers, A. Assessing the implementability of telehealth interventions for self-management support: A realist review. Implement. Sci. 2015, 10, 59. [Google Scholar] [CrossRef]
- Mekov, E.; Miravitlles, M.; Petkov, R. Artificial intelligence and machine learning in respiratory medicine. Expert Rev. Respir. Med. 2020, 14, 559–564. [Google Scholar] [CrossRef]
- Sobnath, D.D.; Philip, N.; Kayyali, R.; Nabhani-Gebara, S.; Pierscionek, B.; Vaes, A.W.; Spruit, M.A.; Kaimakamis, E. Features of a Mobile Support App for Patients With Chronic Obstructive Pulmonary Disease: Literature Review and Current Applications. JMIR Mhealth Uhealth 2017, 5, e17. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Wang, Y.C.; Yang, C.M.; Hu, H.; Xiong, Z.F. Mobile health applications in self-management of patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis of their efficacy. BMC Pulm. Med. 2018, 18, 147. [Google Scholar] [CrossRef] [PubMed]
- Boer, L.; Bischoff, E.; van der Heijden, M.; Lucas, P.; Akkermans, R.; Vercoulen, J.; Heijdra, Y.; Assendelft, W.; Schermer, T. A Smart Mobile Health Tool Versus a Paper Action Plan to Support Self-Management of Chronic Obstructive Pulmonary Disease Exacerbations: Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e14408. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Giangreco, A.; Duffy, M.; Finlayson, E.; Hamilton, S.; Swanson, M.; Colligan, J.; Gilliatt, J.; McIvor, M.; Sage, E.K. Evaluation of myCOPD Digital Self-management Technology in a Remote and Rural Population: Real-world Feasibility Study. JMIR Mhealth Uhealth 2022, 10, e30782. [Google Scholar] [CrossRef] [PubMed]
- Steurer-Stey, C.; Dalla Lana, K.; Braun, J.; ter Riet, G.; Puhan, M.A. Effects of the “Living well with COPD” intervention in primary care: A comparative study. Eur. Respir. J. 2018, 51, 1701375. [Google Scholar] [CrossRef] [PubMed]
- Bohingamu Mudiyanselage, S.; Stevens, J.; Watts, J.J.; Toscano, J.; Kotowicz, M.A.; Steinfort, C.L.; Bell, J.; Byrnes, J.; Bruce, S.; Carter, S.; et al. Personalised telehealth intervention for chronic disease management: A pilot randomised controlled trial. J. Telemed. Telecare 2019, 25, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Tanguay, P.; Marquis, N.; Gaboury, I.; Kairy, D.; Touchette, M.; Tousignant, M.; Decary, S. Telerehabilitation for Post-Hospitalized COVID-19 Patients: A Proof-of-Concept Study During a Pandemic. Int. J. Telerehabil. 2021, 13, e6383. [Google Scholar] [CrossRef]
- Marquis, N.; Larivee, P.; Dubois, M.F.; Tousignant, M. Are improvements maintained after in-home pulmonary telerehabilitation for patients with chronic obstructive pulmonary disease? Int. J. Telerehabil. 2014, 6, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Tarigan, A.P.; Pandia, P.; Tarigan, A.H.; Eyanoer, P.C. Effectiveness of upper limb exercises and breathing exercises in COPD stable patients during COVID-19 pandemic era. Adv. Respir. Med. 2022, 90, 68–76. [Google Scholar] [CrossRef]
- Wade, V.; Gray, L.; Carati, C. Theoretical frameworks in telemedicine research. J. Telemed. Telecare 2017, 23, 181–187. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. Mis Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Baker, E.; Fatoye, F. Clinical and cost effectiveness of nurse-led self-management interventions for patients with copd in primary care: A systematic review. Int. J. Nurs. Stud. 2017, 71, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Chmiel, F.P.; Burns, D.K.; Pickering, J.B.; Blythin, A.; Wilkinson, T.M.; Boniface, M.J. Prediction of Chronic Obstructive Pulmonary Disease Exacerbation Events by Using Patient Self-reported Data in a Digital Health App: Statistical Evaluation and Machine Learning Approach. JMIR Med. Inf. 2022, 10, e26499. [Google Scholar] [CrossRef] [PubMed]
- Slevin, P.; Kessie, T.; Cullen, J.; Butler, M.W.; Donnelly, S.C.; Caulfield, B. Exploring the potential benefits of digital health technology for the management of COPD: A qualitative study of patient perceptions. ERJ Open Res. 2019, 5, 00239-2018. [Google Scholar] [CrossRef] [PubMed]
- Ancochea, J.; Garcia-Rio, F.; Vazquez-Espinosa, E.; Hernando-Sanz, A.; Lopez-Yepes, L.; Galera-Martinez, R.; Peces-Barba, G.; Perez-Warnisher, M.T.; Segrelles-Calvo, G.; Zamarro, C.; et al. Efficacy and costs of telehealth for the management of COPD: The PROMETE II trial. Eur. Respir. J. 2018, 51, 1800354. [Google Scholar] [CrossRef]
- Leonard, R.; Forte, M.; Mehta, D.; Mujahid, H.; Stansbury, R. The impact of a telemedicine intervention on home non-invasive ventilation in a rural population with advanced COPD. Clin. Respir. J. 2021, 15, 728–734. [Google Scholar] [CrossRef]
- Bhatt, S.P.; Patel, S.B.; Anderson, E.M.; Baugh, D.; Givens, T.; Schumann, C.; Sanders, J.G.; Windham, S.T.; Cutter, G.R.; Dransfield, M.T. Video Telehealth Pulmonary Rehabilitation Intervention in Chronic Obstructive Pulmonary Disease Reduces 30-Day Readmissions. Am. J. Respir. Crit. Care Med. 2019, 200, 511–513. [Google Scholar] [CrossRef]
- Guerra-Paiva, S.; Dias, F.; Costaa, D.; Santos, V.; Santos, C. DPO Project: Telehealth to enhance the social role of physical activity in people living with COPD. Procedia Comput. Sci. 2021, 181, 869–875. [Google Scholar] [CrossRef]
- Gregersen, T.L.; Green, A.; Frausing, E.; Ringbaek, T.; Brøndum, E.; Ulrik, C.S. Do telemedical interventions improve quality of life in patients with COPD? A systematic review. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 809. [Google Scholar]
- Sharma, D.; Bhaskar, S. Addressing the Covid-19 Burden on Medical Education and Training: The Role of Telemedicine and Tele-Education During and Beyond the Pandemic. Front. Public Health 2020, 8, 589669. [Google Scholar] [CrossRef] [PubMed]
- Amorim, P.; Brito, D.; Castelo-Branco, M.; Fàbrega, C.; Gomes da Costa, F.; Martins, H.; Gonçalves, L.; Gonçalves, L.M.; Martin, V.; Milner, J. Telehealth opportunities in the COVID-19 pandemic early days: What happened, did not happen, should have happened, and must happen in the near future? Telemed. E-Health 2021, 27, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, S.; Kim, H.; Kim, K.; Lee, C.T.; Yang, S.; Kong, H.J.; Shin, Y.; Lee, K. Acceptability of the consumer-centric u-health services for patients with chronic obstructive pulmonary disease. Telemed. J. E Health 2012, 18, 329–338. [Google Scholar] [CrossRef]
- Dhala, A.; Sasangohar, F.; Kash, B.; Ahmadi, N.; Masud, F. Rapid Implementation and Innovative Applications of a Virtual Intensive Care Unit During the COVID-19 Pandemic: Case Study. J. Med. Internet Res. 2020, 22, e20143. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.; Yu, L.; Casey, J.; Cook, A.; Metaxa, V.; Pattison, N.; Rafferty, A.M.; Ramsay, P.; Saha, S.; Xyrichis, A.; et al. Communication and Virtual Visiting for Families of Patients in Intensive Care during the COVID-19 Pandemic: A UK National Survey. Ann. Am. Thorac. Soc. 2021, 18, 1685–1692. [Google Scholar] [CrossRef]
- Rutkowski, S.; Rutkowska, A.; Kiper, P.; Jastrzebski, D.; Racheniuk, H.; Turolla, A.; Szczegielniak, J.; Casaburi, R. Virtual Reality Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Int. J. Chronic Obs. Pulmon Dis. 2020, 15, 117–124. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, Y.; Zeng, C.; Mao, H. Artificial Intelligence and Machine Learning in Chronic Airway Diseases: Focus on Asthma and Chronic Obstructive Pulmonary Disease. Int. J. Med. Sci. 2021, 18, 2871–2889. [Google Scholar] [CrossRef]




| Clinical Settings | Objective and Summary of the Potential Benefits |
|---|---|
| Primary care settings | Evaluate the acceptability and feasibility of real-time interactive voice and video calls via Skype for teaching breathing exercises and decreasing dyspnea compared to usual care. People who received the teaching via Skype reported less dyspnea than those receiving usual care [30]. Evaluate the effects of exercise coaching via digital health versus self-training without coaching in COPD. Ref. [46] Professionals provided the coaching in the study as part of the telerehabilitation program. The study found that exercise coaching via digital health helped COPD patients to increase their adherence and exercise capacity compared to self-coaching without digital health [46]. |
| Secondary care settings | Determine the effects of The Health Buddy (HB) telemonitoring device on health consumption and health-related quality of life (HRQoL) in patients with moderate to severe COPD. Using HB resulted in decreased hospital days and outpatient visits, but no significant changes were observed in HRQoL [24]. Determine the effect of supervised, home-based, real-time videoconferencing telerehabilitation on exercise capacity, self-efficacy, HRQoL and physical activity in patients with COPD compared with usual care without exercise training. The study showed that telerehabilitation improved endurance, exercise capacity, and self-efficacy in COPD when compared with usual care [46]. |
| Type of Support/Technology | Content (Covered One or a Combination of the Following Subjects) |
|---|---|
|
|
| Mode of delivery | Strategy and intensity |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alghamdi, S.M. Content, Mechanism, and Outcome of Effective Telehealth Solutions for Management of Chronic Obstructive Pulmonary Diseases: A Narrative Review. Healthcare 2023, 11, 3164. https://doi.org/10.3390/healthcare11243164
Alghamdi SM. Content, Mechanism, and Outcome of Effective Telehealth Solutions for Management of Chronic Obstructive Pulmonary Diseases: A Narrative Review. Healthcare. 2023; 11(24):3164. https://doi.org/10.3390/healthcare11243164
Chicago/Turabian StyleAlghamdi, Saeed Mardy. 2023. "Content, Mechanism, and Outcome of Effective Telehealth Solutions for Management of Chronic Obstructive Pulmonary Diseases: A Narrative Review" Healthcare 11, no. 24: 3164. https://doi.org/10.3390/healthcare11243164