
Changes in the Impacts of COVID-19 over Time on Families with Older Adults Living on Remote Islands in Japan: A Study in Family Ethnographic Research



Abstract
:1. Introduction
2. Methods
2.1. Research Design
- Impact: “The result of an action by one thing on another” [17]. Impact has a direction (positive or negative) and a magnitude (amount of change). A primary impact may be accompanied by another impact (secondary impact), and such a chain of impacts (secondary impact, tertiary impact, etc.) is also included in the generic term “impact”.
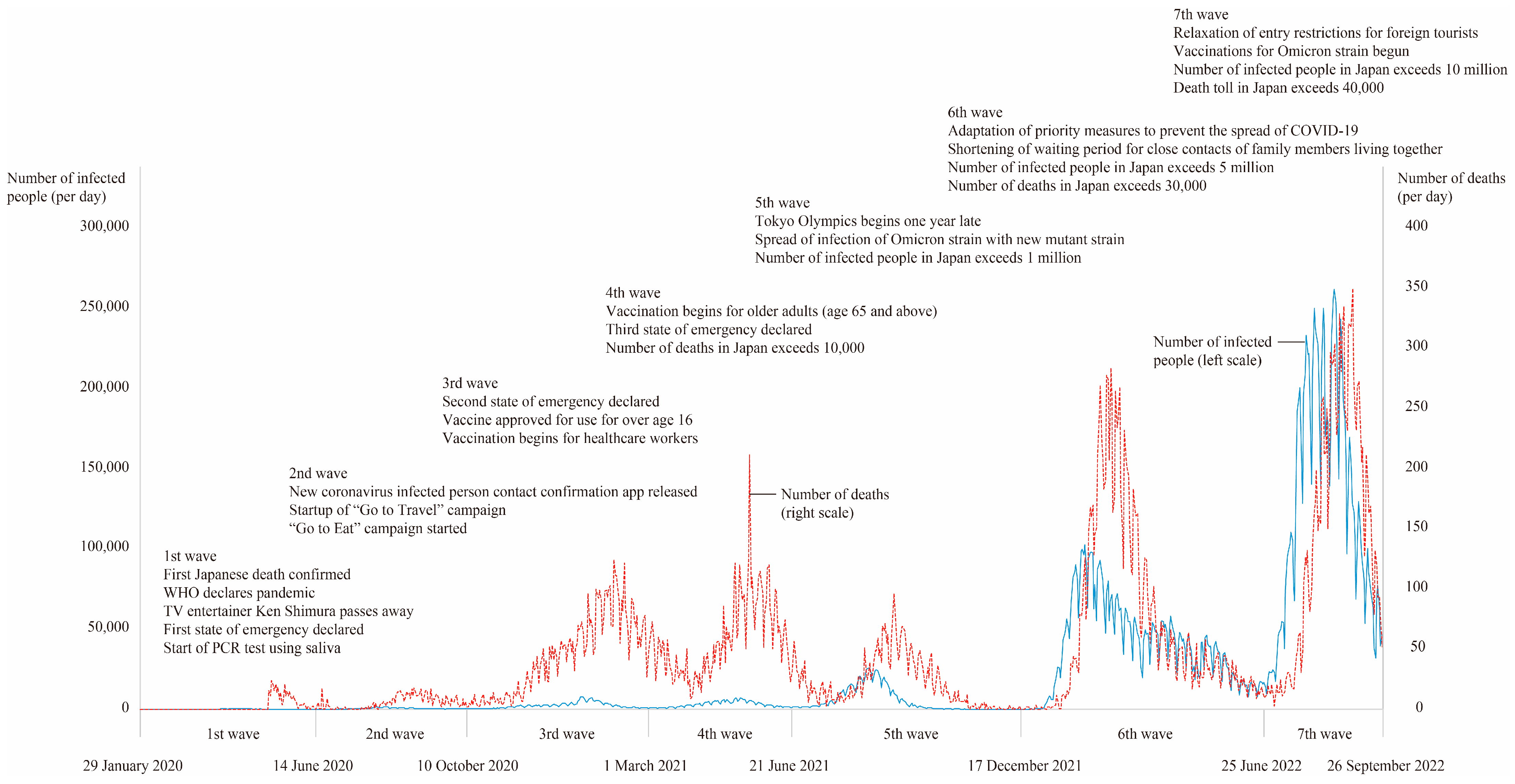
- Periods of increased infection (waves): 1st wave, from 29 January 2020 to 13 June 2020; 2nd wave, from 14 June 2020 to 9 October 2020; 3rd wave, from 10 October 2020 to 28 February 2021; 4th wave, from 1 March 2021 to 20 June 2021; 5th wave, 21 June 2021 to 16 December 2021; 6th wave, from 17 December 2021 to 24 June 2022; and 7th wave, 25 June to 26 September 2022 [18].
- Family: “A unit/organization as a system of the OR operation (logical operation) of individuals, that is, living people, having the cognition of belonging by other constituent member(s)” [19].
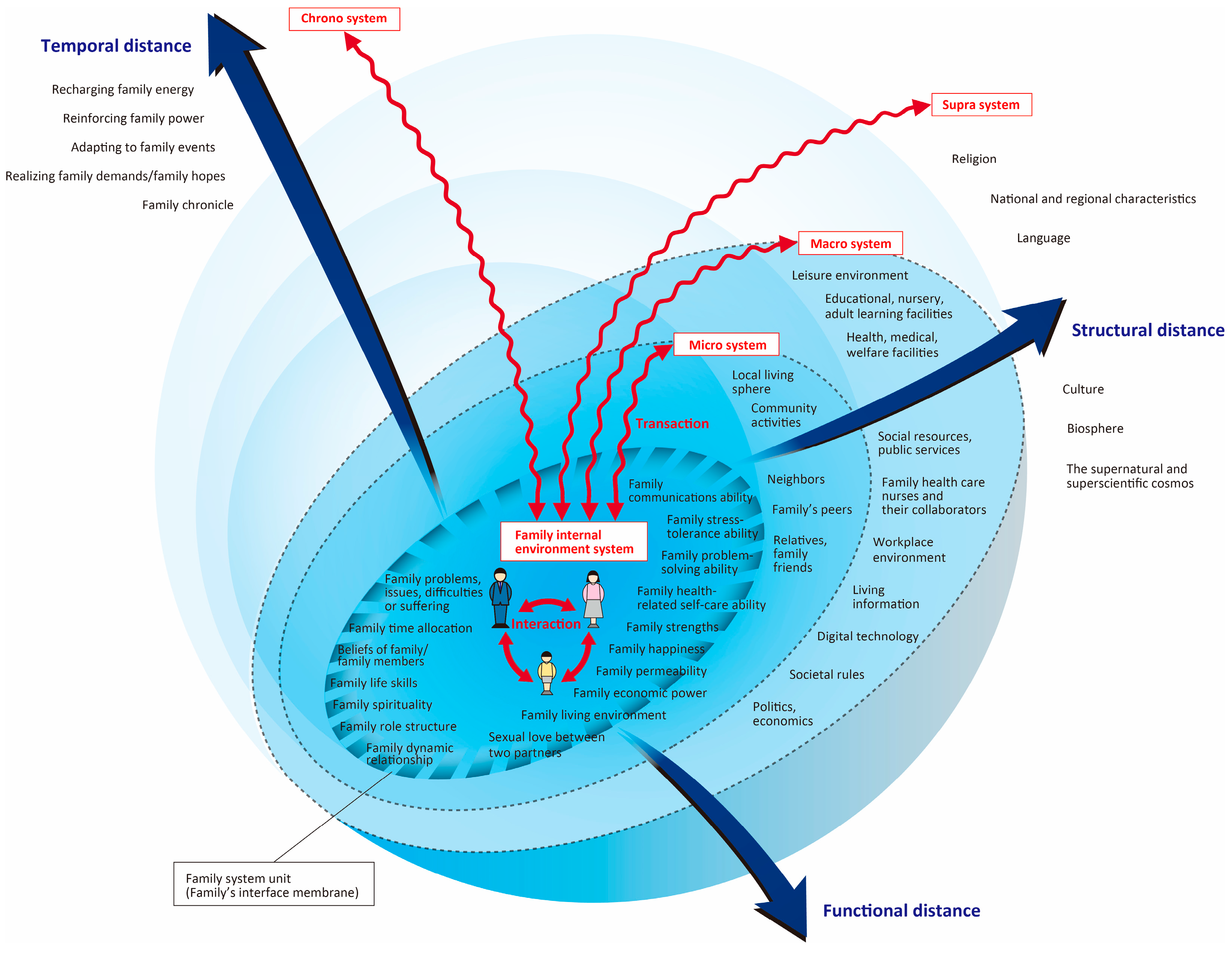
- Family internal environment system: “The environment that includes family communications ability; family time allocation; beliefs of family/family members; family health-related self-care ability; family economic power; family living environment and others” [12].
- Family system unit: “A family existing as a system and a unit” [12].
- Family external environment system: “The 3 environments consisting of supra system, macro system, and micro system” [12].
- Micro system: “The environments that include the local living sphere; relatives, family friends; neighbors and others” [12].
- Macro system: “The environments that include educational, nursery, adult learning facilities; health, medical, welfare facilities; workplace environment; social resources, public services; politics, economics and others” [12].
- Supra system: “The environments that include religion; culture; the supernatural and superscientific cosmos and others” [12].
- Family chrono-environment system: “The environments that include adapting to family events; family chronicle; realizing family demands/family hopes and others” [12].
2.2. Participants and Setting
2.3. Data Collection
2.4. Data Analysis
2.5. Trustworthiness
2.6. Ethical Consideration
3. Results
3.1. Impact of the First Wave
3.2. Impact of the Second Wave
3.3. Impact of the Third Wave
3.4. Impact of the Fourth Wave
3.5. Impact of the Fifth Wave
3.6. Impact of the Sixth Wave
3.7. Impact of the Seventh Wave
4. Discussion
4.1. Overall Picture of the Impact of COVID-19 on Families
4.2. Positive and Negative Impacts of COVID-19 on the Families and Their Changes
4.3. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Outbreak of a Patient with Pneumonia Attributed to Novel Coronavirus Infection (1st Case). Available online: https://www.mhlw.go.jp/stf/newpage_08906.html (accessed on 13 October 2023).
- Watanabe, T.; Yabu, T. Japan’s voluntary lockdown. PLoS ONE 2021, 16, e0252468. [Google Scholar] [CrossRef]
- Hayashi, T.; Noguchi, T.; Kubo, Y.; Tomiyama, N.; Ochi, A.; Hayashi, H. Social frailty and depressive symptoms during the COVID-19 pandemic among older adults in Japan: Role of home exercise habits. Arch. Gerontol. Geriatr. 2022, 98, 104555. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, M.E.; Mogle, J.A.; Lee, J.K.; Tornello, S.L.; Hostetler, M.L.; Cifelli, J.A.; Bai, S.; Hotez, E. Impact of the COVID-19 pandemic on parent, child, and family functioning. Fam. Process 2022, 61, 361–374. [Google Scholar] [CrossRef]
- Arai, Y.; Oguma, Y.; Abe, Y.; Takayama, M.; Hara, A.; Urushihara, H.; Takebayashi, T. Behavioral changes and hygiene practices of older adults in Japan during the first wave of COVID-19 emergency. BMC Geriatr. 2021, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Gough, C.; Lewis, L.K.; Barr, C.; Maeder, A.; George, S. Community participation of community dwelling older adults: A cross-sectional study. BMC Public Health 2021, 21, 612. [Google Scholar] [CrossRef] [PubMed]
- Manoiu, R.; Hammond, N.G.; Yamin, S.; Stinchcombe, A. Religion/spirituality, mental health, and the lifespan: Findings from a representative sample of Canadian adults. Can. J. Aging 2023, 42, 115–125. [Google Scholar] [CrossRef]
- Visualizing the Data: Information on COVID-19 Infections. Available online: https://covid19.mhlw.go.jp/ (accessed on 13 October 2023).
- López, J.; Pérez-Rojo, G.; Noriega, C.; Martínez-Huertas, J.A.; Velasco, C. Longitudinal impact of the COVID-19 pandemic on older adults’ wellbeing. Front. Psychiatry 2022, 13, 837533. [Google Scholar] [CrossRef]
- Soejima, T. Impact of the coronavirus pandemic on family well-being: A rapid and scoping review. Open J. Nurs. 2021, 11, 1064–1085. [Google Scholar] [CrossRef]
- Hohashi, N.; Honda, J. Development of the Concentric Sphere Family Environment Model and companion tools for culturally congruent family assessment. J. Transcult. Nurs. 2011, 22, 350–361. [Google Scholar] [CrossRef]
- Hohashi, N. Understanding Family Health Care Nursing through Applicable Terminology: Concentric Sphere Family Environment Theory; Version 3.4; Editex: Kawasaki, Japan, 2023; ISBN 978-4-903320-66-3. [Google Scholar]
- The Number of Japanese Islands Was Counted. Available online: https://www.gsi.go.jp/kihonjohochousa/pressrelease20230228.html (accessed on 13 October 2023).
- Cohen, S.A.; Greaney, M.L. Aging in rural communities. Curr. Epidemiol. Rep. 2023, 10, 1–16. [Google Scholar] [CrossRef]
- Marutani, M.; Kodama, S.; Harada, N. Japanese public health nurses’ culturally sensitive disaster nursing for small island communities. Island Stud. J. 2020, 15, 371–386. [Google Scholar] [CrossRef]
- Hohashi, N.; Ota, H.; Lin, Q.; Watsuji, T. Procedures for conducting ethnographic research and research case studies. J. Jpn. Soc. Nurs. Res. 2022, 45, 159–175. [Google Scholar] [CrossRef]
- Hohashi, N. Understanding Family Health Care Nursing through Applicable Terminology: Family Symptomatology; Version 3.4; Editex: Kawasaki, Japan, 2023; ISBN 978-4-903320-69-4. [Google Scholar]
- Figure Related to Epidemiology of New Coronavirus Infections to Date and Anticipated Transmission and Transmission Dynamics in the Future. Available online: https://www.mhlw.go.jp/content/10900000/001088930.pdf (accessed on 13 October 2023).
- Hohashi, N. Understanding Family Health Care Nursing through Applicable Terminology: Studies on Fundamental Family Nursing and Family Functioning; Version 3.1; Editex: Kawasaki, Japan, 2023; ISBN 978-4-903320-71-7. [Google Scholar]
- 2021 Population Census: Basic Complete Tabulation on Population and Households: Outline of Goto City. Available online: https://www.city.goto.nagasaki.jp/s007/040/010/020/160/R2_kokuseigaiyou.pdf (accessed on 13 October 2023).
- Hohashi, N.; Watanabe, M. Family Environment Assessment Index (FEAI-JA); Version 3.4; Hohashi, N., Ed.; Editex: Kawasaki, Japan, 2023; ISBN 978-4-903320-62-5. [Google Scholar]
- Number of New Positives (Daily), Number of Deaths (Cumulative). Available online: https://www.mhlw.go.jp/stf/covid-19/open-data.html (accessed on 13 October 2023).
- Hohashi, N. The Japanese Version of the Family Environment Map (FEM-JA); Version 3.2JA; Editex: Kawasaki, Japan, 2023; ISBN 978-4-903320-63-2. [Google Scholar]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Brear, M. Process and outcomes of a recursive, dialogic member checking approach: A project ethnography. Qual. Health Res. 2019, 29, 944–957. [Google Scholar] [CrossRef] [PubMed]
- Raoofi, A.; Takian, A.; Haghighi, H.; Rajizadeh, A.; Rezaei, Z.; Radmerikhi, S.; Olyaeemanesh, A.; Akbari Sari, A. COVID-19 and comparative health policy learning; The experience of 10 countries. Arch. Iran. Med. 2021, 24, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Eales, L.; Ferguson, G.M.; Gillespie, S.; Smoyer, S.; Carlson, S.M. Family resilience and psychological distress in the COVID-19 pandemic: A mixed methods study. Dev. Psychol. 2021, 57, 1563–1581. [Google Scholar] [CrossRef] [PubMed]
- Lebow, J.L. The challenges of COVID-19 for divorcing and post-divorce families. Fam. Process 2020, 59, 967–973. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of social isolation due to COVID-19 on health in older people: Mental and physical effects and recommendations. J. Nutr. Health Aging 2020, 24, 9380–9947. [Google Scholar] [CrossRef]
- Shekhawat, R.S.; Meshram, V.P.; Kanchan, T.; Misra, S. Privacy and patient confidentiality in times of COVID-19. Med. Leg. J. 2020, 88, 229–230. [Google Scholar] [CrossRef]
- Awijen, H.; Ben Zaied, Y.; Nguyen, D.K. COVID-19 vaccination, fear and anxiety: Evidence from Google search trends. Soc. Sci. Med. 2022, 297, 114820. [Google Scholar] [CrossRef] [PubMed]
- Delgado, C.E.; Silva, E.A.; Castro, E.A.B.; Carbogim, F.D.C.; Püschel, V.A.A.; Cavalcante, R.B. COVID-19 infodemic and adult and elderly mental health: A scoping review. Rev. Esc. Enferm. USP 2021, 55, e20210170. [Google Scholar] [CrossRef] [PubMed]
- Corpuz, J.C.G. Reflection: Spirituality during COVID-19. J. Pastoral Care Counsel. 2021, 75, 133–134. [Google Scholar] [CrossRef]
- Dhawan, D.; Bekalu, M.; Pinnamaneni, R.; McCloud, R.; Viswanath, K. COVID-19 news and misinformation: Do they matter for public health prevention? J. Health Commun. 2021, 26, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Ingadottir, B.; Bragadottir, B.; Zoëga, S.; Blondal, K.; Jonsdottir, H.; Hafsteinsdottir, E.J.G. Sense of security during COVID-19 isolation improved with better health literacy: A cross-sectional study. Patient Educ. Couns. 2023, 114, 107788. [Google Scholar] [CrossRef]
- Stilos, K.K.; Ford, R.B.; Wynnychuk, L. Call to action: The need to expand spiritual care supports during the COVID-19 pandemic. Can. Oncol. Nurs. J. 2021, 31, 347–349. [Google Scholar] [PubMed]
- Jun, S.P.; Yoo, H.S.; Lee, C. Young people are not blameworthy: The generation’s awareness of COVID-19 and behavioral responses. Sci. Rep. 2021, 11, 23595. [Google Scholar] [CrossRef]
- Moritsu, C. The discourse of newspaper sponsorship in the Tokyo 2020 Olympics. Jpn. J. Sport Sociol. 2022, 30, 85–99. [Google Scholar] [CrossRef]
- Evertsson, P.; Rosengren, K. Political experiences of changing the focus in elderly care in one municipality. J. Nurs. Manag. 2015, 23, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Namiki, H.; Kobayashi, T. The ecology of medical care on the westernmost remote island, Yonaguni Island, Japan: A cross-sectional study. PLoS ONE 2018, 13, e0199871. [Google Scholar] [CrossRef]
- Tanabe, K. Society coexisting with COVID-19. Infect. Control Hosp. Epidemiol. 2020, 41, 988–989. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Category (System) | Subcategory | ||||||
|---|---|---|---|---|---|---|---|
| 1st Wave | 2nd Wave | 3rd Wave | 4th Wave | 5th Wave | 6th Wave | 7th Wave | |
| Int | (P9) Improving awareness of health-related activities, including infection prevention among family members | (P17) Strengthen awareness of infection prevention among family members as the island lacks good medical facilities | (P31) Psychological stability of family members enabled by information exchange between family members | (P41) Despite the increase in the number of infected people, resumption of return of family members living outside the island thanks to dropping of restrictions | |||
| Fsu | (P1) Fostering a feeling of mutually helping one another as a family (P2) Strengthening family bonds living on the same islands by discouraging the return of family members living off-island (P3) Reduced burden on household finances due to restrictions on leisure activities | (P10) Shifting the family’s thinking to a more positive orientation about restrictions on activities (P11) Appearance of a family belief that health comes first (P12) Improvement in family self-care skills through increased frequency of contact between family members | (P18) Family’s secure feelings about infection prevention with the advent of vaccines (P19) Family cooperation to alleviate loneliness from restrictions toward family members living off-island from returning | (P24) Reducing family’s concerns over the risk of infection through vaccination and testing (P25) Family’s relief that no one became infected at a funeral | (P32) Family’s sense of security concerning family members avoiding infection through additional vaccinations (P33) Family’s closer feelings towards family members who have become a close contact of a case of coronavirus | (P38) Recovery of family economy thanks to increase in number of tourists | (P42) Experiencing family’s happiness from being reunited with family members who returned to the island from outside the island |
| Mic | (P4) Maintaining a sense of community solidarity despite the cancellation of local events | (P20) Providing support to relatives using SNS | (P26) Family promoting infection-prevention behavior to other family and friends | (P39) Easing neighbors’ views toward people leaving the island by implementing antigen tests | (P43) Relief from stress caused by concerns for neighbors | ||
| Mac | (P5) Strengthening the sense of norms regarding family respectability | (P13) Development of a sense of crisis regarding COVID-19 through consideration of the island’s characteristics (P14) Improvement of family members’ sense of crisis regarding infectious diseases by policies | (P21) Strengthening family awareness of infection prevention through information gathering (P22) Request for disclosure of details such as the district name where infections occurred | (P27) Sense of security for movement to and from the island through vaccination and testing (P28) Diminishing of fear of infection through gathering of information | (P34) Utilization of disaster prevention radio as a means of obtaining information (P35) Increased sense of security among family members toward island visitors who have undergone antigen testing | (P40) Family members providing mutual help via SNS when a family member living off the island became infected | (P44) Closer psychological proximity with island visitors |
| Sup | (P6) Increased free time among family members due to business closures (P7) Due to the death of a prominent person from COVID-19, families became more aware of infection control measures | (P15) Improving awareness of infection prevention through changes in the ways of holding funerals | (P23) Strengthening mutual help between people and families on the island through a religious-based spirit of mutual help | (P36) Generation of positive feelings among families by holding a global festival | |||
| Chr | (P8) Increase awareness of the presence of families living on the island | (P16) Increase in time with family thanks to more opportunities to go out together | (P29) Deeper consideration concerning lifespans of older family members (P30) Changes in the practice of visits to family graves based on infection status | (P37) Hope for reunion with family members living off the island thanks to the ban on homecoming | (P45) Lives not wishing to change infection control measures even after the pandemic | ||
| Category (System) | Subcategory | ||||||
|---|---|---|---|---|---|---|---|
| 1st Wave | 2nd Wave | 3rd Wave | 4th Wave | 5th Wave | 6th Wave | 7th Wave | |
| Int | (N1) Fear of infection among family members with illnesses/disabilities or older adults (N2) Loss of opportunities to meet family members who live apart | (N7) Restrictions on work and facility use for family members after their return to the island (N8) Psychological burden on family members due to changes in work | (N23) Difficulty in receiving vaccinations for older family members on their own | (N30) Difficulty in maintaining distance from close contacts who are quarantined at home (N31) Increased fear of side effects from vaccine | (N35) Reduced sense of crisis due to asymptomatic infection | ||
| Fsu | (N3) Imbalance in family members’ roles due to lack of change in family role apportionment (N4) Family concerns about members living outside the island | (N9) Decrease in family income due to drop-off in number of tourists (N10) Occurrence of loneliness caused by cancellation of family events (N11) Family’s fear of becoming a source of infection on the island | (N20) Differences of opinion within the family regarding the pros and cons of vaccination | (N24) Family distress over infection prevention for funeral attendees from outside the island | (N32) Occurrence of family acclimatization to infection due to infection of family members | (N38) Increased anxiety of families due to the rapid increase in COVID-19 infections on the island | |
| Mic | (N5) Disappearance of opportunities for interaction with neighbors and family | (N12) Negative comments from neighbors about an off-island trip (N13) Discriminatory treatment due to suspicion of infection from neighbors after returning to the island | (N25) Decrease in daily mutual assistance between neighbors | (N33) Increase in rumors about infected people in the neighborhood | |||
| Mac | (N14) Decrease in family happiness due to loss of opportunity for family members living away from the island to return (N15) Increased fear of infection caused by rumors concerning the first person to be infected on the island (N16) Difficulty in obtaining face masks due to rising prices stemming from a nationwide mask shortage | (N21) Difficulty meeting grandchildren born outside the island for the first time | (N26) Dissatisfaction with lack of information via disaster prevention radio (N27) Family concerns over lack of medical facilities on the island (N28) Decreased sense of urgency due to lack infected people in proximity | (N39) Expectations that payment of benefits will exacerbate the decline in economic strength | |||
| Sup | (N17) Psychological instability within family due to cancellations of local and traditional events (N18) Cancellation of family members living outside the island to return and participate in religious events | (N22) Family spiritual suffering due to cancellation of religious events | (N34) Sharp differences in awareness of the risk of infection between generations | (N36) Increased sense of crisis due to news of exploding rate of infection | |||
| Chr | (N6) Family anxiety about the unknown aspects of COVID-19 | (N19) Family anxiety about inability to adopt ‘perfect’ infection prevention measures | (N29) Anxiety about vaccination side effects | (N37) Concerns over infection caused by at-home treatment of infected family members | (N40) Resignation toward becoming infected as the number of infections is increasing | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hohashi, N.; Watanabe, M.; Taniguchi, M.; Araki, S. Changes in the Impacts of COVID-19 over Time on Families with Older Adults Living on Remote Islands in Japan: A Study in Family Ethnographic Research. Healthcare 2023, 11, 3088. https://doi.org/10.3390/healthcare11233088
Hohashi N, Watanabe M, Taniguchi M, Araki S. Changes in the Impacts of COVID-19 over Time on Families with Older Adults Living on Remote Islands in Japan: A Study in Family Ethnographic Research. Healthcare. 2023; 11(23):3088. https://doi.org/10.3390/healthcare11233088
Chicago/Turabian StyleHohashi, Naohiro, Mikio Watanabe, Minami Taniguchi, and Shiho Araki. 2023. "Changes in the Impacts of COVID-19 over Time on Families with Older Adults Living on Remote Islands in Japan: A Study in Family Ethnographic Research" Healthcare 11, no. 23: 3088. https://doi.org/10.3390/healthcare11233088