

Segmental Rib Index and Spinal Deformity: Scoliogenic Implications

 ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
3. Results
3.1. Segmental Rib Index and Surface Deformity (RHD) Correlations
3.2. Segmental Rib Index and Cobb Angle Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIS | Adolescent Idiopathic Scoliosis |
| ANS | Autonomic Nerve System |
| ATR | Angle of Trunk Rotation |
| ATI | Angle of Trunk Inclination |
| CNS | Central Nervous System |
| DRCI | Double Rib Contour Sign |
| EOS | Early Onset Scoliosis (EOS) |
| IS | Idiopathic Scoliosis |
| LSP | Lateral Spinal Profile |
| LSR | Lateral Standing Radiographs |
| RC | Rib Cage |
| RH | Rib Hump |
| RHD | Rib Hump Deformity |
| RI | Rib Index |
| RVA | Rib Vertebra Angle |
| SRI | Segmental Rib Index |
| SSS | School Scoliosis Screening |
| TA | Truncal Asymmetry |
References
- Nissinen, M.; Heliövaara, M.; Ylikoski, M.; Poussa, M. Trunk asymmetry and screening for scoliosis: A longitudinal cohort study of pubertal schoolchildren. Acta Paediatr. 1993, 82, 77–82. [Google Scholar] [CrossRef]
- Grivas, T.B. Thorax and the idiopathic Scoliosis. Int. J. Adv. Res. 2023, 11, 1252–1290. [Google Scholar] [CrossRef] [PubMed]
- Labelle, H.; Richards, S.B.; De Kleuver, M.; Grivas, T.B.; Luk, K.D.; Wong, H.K.; Thometz, J.; Beauséjour, M.; Turgeon, I.; Fong, D.Y. Screening for adolescent idiopathic scoliosis: An information statement by the scoliosis research society international task force. Scoliosis 2013, 8, 17. [Google Scholar] [CrossRef] [PubMed]
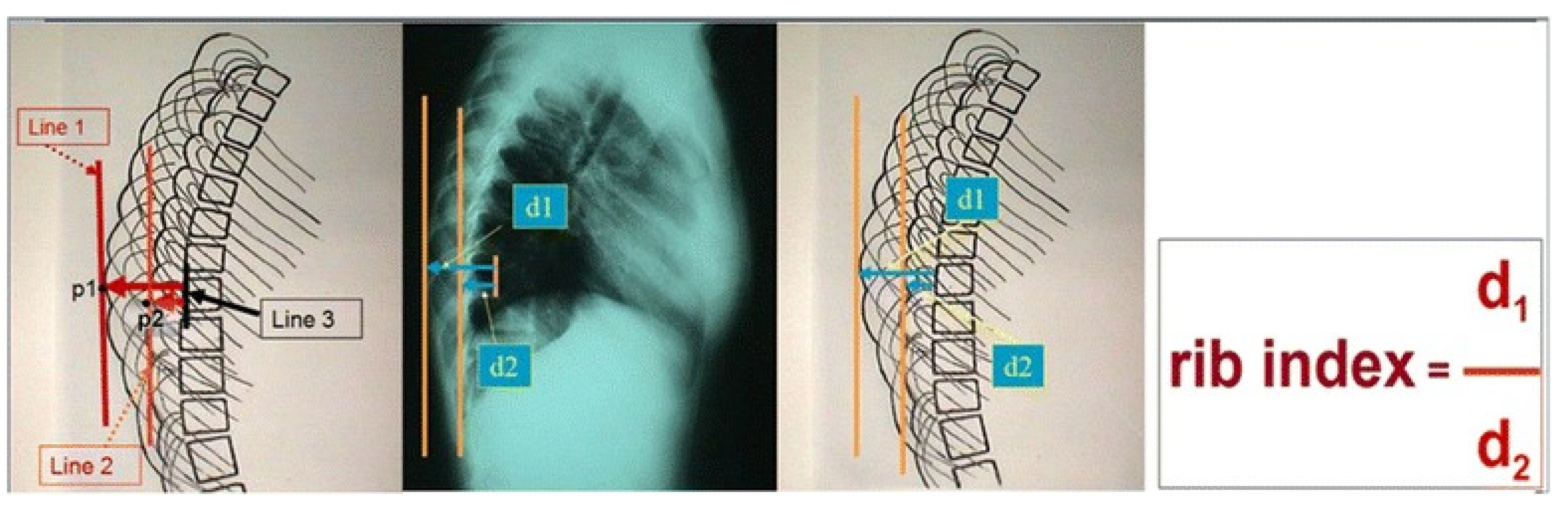
- Grivas, T.B. Rib index. Scoliosis 2014, 9, 20. [Google Scholar] [CrossRef]
- Lebel, A.; Lebel, V. Rib index, an objective measure to document changes of the rib hump deformity in a Risser 4 progressive AIS patient treated with the Schroth method. Scoliosis 2014, 9 (Suppl. S1), O18. [Google Scholar] [CrossRef]
- Grivas, T.B. Radiological appraisal of thoracic deformity—Improvement or deterioration using the convex/concave rib-hump index (‘double rib contour sign’) in curves Lenke Type 1, 3, 5 and 6. In Scoliosis Research Society. Half-Day Courses; SRS 2012–2013 Education Committee, Ed.; Scoliosis Research Society: Milwaukee, WI, USA, 2013; pp. 29–30. [Google Scholar]
- Haber, L.L.; Adams, T.M.; Briski, D.C.; Celestre, P.C.; Robbins, D.J.; Waldron, S.R. Long-Term Results of Spine Stapling for AIS to Skeletal Maturity and Beyond. J. Pediatr. Orthop. 2020, 40, e37–e41. [Google Scholar] [CrossRef]
- Tsirikos, A.I.; McMillan, T.E. All Pedicle Screw versus Hybrid Hook–Screw Instrumentation in the Treatment of Thoracic Adolescent Idiopathic Scoliosis (AIS): A Prospective Comparative Cohort Study. Healthcare 2022, 10, 1455. [Google Scholar] [CrossRef]
- Sevastik, J.; Burwell, R.G.; Dangerfield, P.H. A new concept for the etiopathogenesis of the thoracospinal deformity of idiopathic scoliosis: Summary of an electronic focus group debate of the IBSE. Eur. Spine J. 2003, 12, 440–450. [Google Scholar] [CrossRef]
- Burwell, R.G.; Dangerfield, P.H.; Moulton, A.; Grivas, T.B.; Cheng, J.C. Whither the etiopathogenesis (and scoliogeny) of adolescent idiopathic scoliosis? Incorporating presentations on scoliogeny at the 2012 IRSSD and SRS meetings. Scoliosis 2013, 8, 4. [Google Scholar] [CrossRef]
- Cobb, J. Outline for the study of scoliosis. Instr. Course Lect. 1948, 5, 261–275. [Google Scholar]
- Grivas, T.B.; Vasiliadis, E.S.; Kouropoulos, G.; Segos, D.; Triantafyllopoulos, G.; Mouzakis, V. Study of trunk asymmetry in normal children and adolescents. Scoliosis 2006, 1, 19. [Google Scholar] [CrossRef] [PubMed]
- Cheung, M.-C.; Yip, J.; Lai, J.S.K. Biofeedback Posture Training for Adolescents with Mild Scoliosis. BioMed Res. Int. 2022, 2022, 5918698. [Google Scholar] [CrossRef]
- Monticone, M.; Ambrosini, E.; Cazzaniga, D.; Rocca, B.; Ferrante, S. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomized controlled trial. Eur. Spine J. 2014, 23, 1204–1214. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; De Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of bracing in adolescents with idiopathic. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef]
- Kuznia, A.L.; Hernandez, A.K.; Lee, L.U. Adolescent Idiopathic Scoliosis: Common Questions and Answers. Am. Fam. Physician 2020, 101, 19–23. [Google Scholar] [PubMed]
- Courvoisier, A.; Drevelle, X.; Dubousset, J.; Skalli, W. Transverse plane 3D analysis of mild scoliosis. Eur. Spine J. 2013, 22, 2427–2432. [Google Scholar] [CrossRef]
- Pruijs, J.E.; Keessen, W.; van der Meer, R.; van Wieringen, J.C.; Hageman, M.A. School screening for scoliosis: Methodologic considerations. Part 1, External measurements. Spine 1992, 17, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Pruijs, J.E.; Keessen, W.; van der Meer, R.; van Wieringen, J.C. School screening for scoliosis: The value of quantitative measurement. Eur. Spine J. 1995, 4, 226–230. [Google Scholar] [CrossRef]
- Nissinen, M.; Heliovaara, M.; Tallroth, K.; Poussa, M. Trunk asymmetry and scoliosis. Anthropometric measurements in prepubertal school children. Acta Paediatr. Scand. 1989, 78, 747–753. [Google Scholar] [CrossRef]
- Nissinen, M.; Heliovaara, M.; Seltsamo, J.; Poussa, M. Trunk Asymmetry, Posture, Growth, and Risk of Scoliosis. A Three-Year Follow-Up of Finnish Prepubertal School Children. Spine 1993, 18, 99. [Google Scholar] [CrossRef]
- Sevastik, J.A.; Aaro, S.; Normelli, H. Scoliosis. Experimental and clinical studies. Clin. Orthop. Relat. Res. 1984, 191, 27–34. [Google Scholar] [CrossRef]
- Normelli, H.; Sevastik, J.; Wallberg, H. The thermal emission from the skin and the vascularity of the breasts in normal and scoliotic girls. Spine 1986, 11, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Sevastik, J.A.; Aaro, S.; Lindholm, S.T.; Dalhborn, M. Experimental scoliosis in growing rabbits by operations on the rib cage. Clin. Orthop. 1987, 136, 282–286. [Google Scholar]
- Agadir, M.; Sevastik, B.; Sevastik, J.A.; Persson, A.; Isberg, B. Induction of scoliosis in the growing rabbit by unilateral rib-growth stimulation. Spine 1988, 13, 1065–1069. [Google Scholar] [CrossRef]
- Normelli, H.; Sevastik, J.A.; Ljung, G.; Jönsson-Söderström, A.M. The symmetry of the breasts in normal and scoliotic girls. Spine 1986, 11, 749–752. [Google Scholar] [CrossRef]
- Sevastik, J.; Agadir, M.; Sevastik, B. Effects of rib elongation on the spine: I. Distortion of the vertebral alignment in the rabbit. Spine 1990, 15, 822–825. [Google Scholar] [CrossRef]
- Sevastik, J.; Agadir, M.; Sevastik, B. Effects of rib elongation on the spine: II. Correction of scoliosis in the rabbit. Spine 1990, 15, 826–829. [Google Scholar] [CrossRef] [PubMed]
- Agadir, M.; Sevastik, B.; Reinholt, F.P.; Perbeck, L.; Sevastik, J. Vascular Changes in the Chest Wall After Unilateral Resection of the Intercostal Nerves in the Growing Rabbit. J. Orthop. Res. 1990, 8, 283–290. [Google Scholar] [CrossRef]
- Sevastik, B.; Xiong, B.; Lundberg, A.; Sevastik, J.A. In vitro opto-electronic analysis of 3-D segmental vertebral movements during gradual rib lengthening in the pig. Acta Orthop. Belg. 1995, 61, 218–225. [Google Scholar] [PubMed]
- Gréalou, L.; Aubin, C.E.; Sevastik, J.A.; Labelle, H. Simulations of rib cage surgery for the management of scoliotic deformities. Stud. Health Technol. Inform. 2002, 88, 345–349. [Google Scholar] [PubMed]
- Sevastik JA Dysfunction of the autonomic nerve system (ANS) in the aetiopathogenesis of adolescent idiopathic scoliosis. Stud. Health Technol. Inform. 2002, 88, 20–23.
- Normelli, H.; Sevastik, J.; Ljung, G.; Aaro, S.; Jönsson-Söderström, A.M. Anthropometric data relating to normal and scoliotic Scandinavian girls. Spine 1985, 10, 123–126. [Google Scholar] [CrossRef]
- Sevastik, J.A. Right convex thoracic female adolescent scoliosis in the light of the thoracospinal concept. Stud. Health Technol. Inform. 2006, 123, 552–558. [Google Scholar]
- Xiong, B.; Sevastik, J.A. A physiological approach to surgical treatment of progressive early idiopathic scoliosis. Eur. Spine J. 1998, 7, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Βurwell, R.G.; Cole, A.A.; Cook, T.A.; Grivas, T.B.; Kiel, A.W.; Moulton, A.; Thirlwall, A.S.; Upadhyay, S.S.; Webb, J.K.; Wemyss-Holden, S.A.; et al. 1991–1992. Pathogenesis of Idiopathic Scoliosis. The Nottingham Concept. Acta Orthop. Belg. 1992, 58 (Suppl. S1), 33–58. [Google Scholar]
- Dansereau, J.; Stokes, I.A.F. Measurements of three-dimensional shape of the rib cage. J. Biomech. 1988, 21, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Hierholzer, E.; Hackenberg, L. Three-dimensional shape analysis of the scoliotic spine using MR tomography and rasterstereography. Stud. Health Technol. Inform. 2002, 91, 184–189. [Google Scholar]
- Sangole, A.P.; Aubin, C.E.; Labelle, H.; Stokes, I.A.; Lenke, L.G.; Jackson, R.; Newton, P. Three-dimensional classification of thoracic scoliotic curves. Spine 2009, 34, 91–99. [Google Scholar] [CrossRef]
- Donzelli, S.; Poma, S.; Balzarini, L.; Borboni, A.; Respizzi, S.; Villafane, J.H.; Zaina, F.; Negrini, S. State of the art of current 3-D scoliosis classifications: A systematic review from a clinical perspective. J. Neuroeng. Rehabil. 2015, 12, 91. [Google Scholar] [CrossRef]
- Dansereau, J.; Stokes, I.A.F.; Moreland, M.S. Radiographic reconstruction of 3D human rib cage. In Surface Topography and Spinal Deformity; Stokes, I.A.F., Pekelsky, J.R., Moreland, M.S., Eds.; Gustav Fischer: Stuttgart, Germany, 1987; pp. 67–76. [Google Scholar]
- Grivas, T.B.; Jevtic, N.; Ljubojevic, D.; Pjanic, P.; Golic, F.; Vasiliadis, E. Segmental Rib Index and Spinal Deformity: Aetiological Implications to Idiopathic Scoliosis. 2023. Available online: https://fizijatri.org/ (accessed on 10 September 2023).
- Barrett, D.S.; MacLean, J.G.B.; Bettany, J.; Ransford, A.O.; Edgar, M.A. Costoplasty in adolescent idiopathic scoliosis. Objective results in 55 patients. J. Bone Joint Surg. Br. 1993, 75, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Harvey, C.J., Jr.; Betz, R.R.; Clements, D.H.; Huss, G.K.; Clancy, M. Are there indications for partial rib resection in patients with adolescent idiopathic scoliosis treated with Cotrel-Dubousset instrumentation? Spine 1993, 18, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Shufflebarger, H.L.; Smiley, K.; Roth, H.J. Internal thoracoplasties. A new procedure. Spine 1994, 19, 840–842. [Google Scholar] [CrossRef] [PubMed]
- Steel, H.H. Rib resection and spine fusion in correction of convex deformity in scoliosis. J. Bone Joint Surg. Am. 1983, 65, 920–992. [Google Scholar] [CrossRef] [PubMed]
- Erkula, G.; Sponseller, P.D.; Kiter, A.E. Rib deformity in scoliosis. Eur. Spine J. 2003, 12, 281–287. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Female | Male | p Value | |
|---|---|---|---|---|
| N | 83 | 63 (75.9%) | 20 (24.1%) | |
| Age (years) | 12.3 ± 2.7 | 12.5 ± 2.5 | 11.5 ± 3.5 | 0.241 a |
| Risser stage | 2 (4) | 2 (4) | 0 (2.8) | 0.023 b |
| Cobb angle | 26.3 ± 10.8 | 27.7 ± 11.2 | 22.7 ± 7.8 | 0.068 a |
| ATR | 7.6 ± 4.3 | 8.0 ± 4.4 | 7.3 ± 4.6 | 0.514 a |
| Gender | Curve Type | n | Mean ± SD |
|---|---|---|---|
| Male | Thoracic | 6 (7.2%) | 25.4 ± 8.1 |
| Thoracolumbar | 6 (7.2%) | 22.0 ± 10.4 | |
| Lumbar | 8 (9.6%) | 21.1 ± 5.6 | |
| Female | Thoracic | 19 (22.9%) | 29.0 ± 12.2 |
| Thoracolumbar | 26 (31.3%) | 27.7 ± 9.8 | |
| Lumbar | 18 (21.7%) | 26.2 ± 12.5 |
| n = 83 | Pearson Correlation | p Value |
|---|---|---|
| T6 | 0.292 | 0.007 * |
| T7 | 0.220 | 0.046 * |
| T8 | 0.240 | 0.029 * |
| n = 25 | Pearson Correlation | p Value |
|---|---|---|
| T6 | 0.432 | 0.031 * |
| T7 | 0.419 | 0.037 * |
| T8 | 0.520 | 0.008 * |
| T9 | 0.424 | 0.034 * |
| T10 | 0.491 | 0.013 * |
| T11 | 0.556 | 0.004 * |
| T12 | 0.485 | 0.014 * |
| Female | Thoracic n = 19 | Thoracolumbar n = 26 | Lumbar n = 18 | p Value |
|---|---|---|---|---|
| T1 | 1.30 (0.48) | 1.20 (0.43) | 1.15 (0.50) | 0.444 a |
| T2 | 1.40 (0.54) | 1.67 (0.72) | 1.24 (0.71) | 0.310 a |
| T3 | 1.51 (0.51) | 1.57 (0.59) | 1.38 (0.64) | 0.233 a |
| T4 | 1.59 (0.58) | 1.57 (0.40) | 1.38 (0.51) | 0.201 a |
| T5 | 1.67 (0.95) | 1.46 (0.35) | 1.45 (0.48) | 0.404 a |
| T6 | 1.60 (0.60) | 1.42 (0.40) | 1.40 (0.42) | 0.322 a |
| T7 | 1.54 (0.51) | 1.40 (0.29) | 1.39 (0.47) | 0.133 a |
| T8 | 1.60 (0.50) | 1.39 (0.30) | 1.34 (0.45) | 0.054 a |
| T9 | 1.73 (0.52) TL | 1.38 (0.33) | 1.42 (0.41) | 0.018 a |
| T10 | 1.75 (0.57) | 1.42 (0.55) | 1.20 (0.66) | 0.052 a |
| T11 | 1.43 (0.70) | 1.49 (0.50) | 1.20 (0.54) | 0.091 a |
| T12 | 1.22 (0.67) | 1.41 (0.50) L | 1.11 (0.32) | 0.021 a |
| Female | Thoracic vs. Thoracolumbar | Thoracic vs. Lumbar | Thoracolumbar vs. Lumbar | |
| T9 | 0.011 * | - | - | |
| T12 | - | - | 0.005 * | |
| Male | Thoracic (n = 6) | TL (n = 6) | Lumbar (n = 8) | p Value |
|---|---|---|---|---|
| T1 | 1.11 (0.20) | 1.18 (0.39) | 1.21 (0.49) | 0.487 a |
| T2 | 1.13 (0.51) | 1.29 (0.42) | 1.32 (0.63) | 0.768 a |
| T3 | 1.26 (0.58) | 1.52 (1.17) | 1.36 (0.47) | 0.691 a |
| T4 | 1.26 (0.66) | 1.50 (1.13) | 1.44 (0.51) | 0.372 a |
| T5 | 1.22 (0.88) | 1.50 (1.02) | 1.36 (0.62) | 0.215 a |
| T6 | 1.52 (0.59) | 1.39 (0.88) | 1.26 (0.58) | 0.352 a |
| T7 | 1.43 (0.35) | 1.58 (0.82) | 1.32 (0.60) | 0.331 a |
| T8 | 1.47 (0.28) | 1.61 (1.01) | 1.39 (0.66) | 0.411 a |
| T9 | 1.50 (0.17) | 1.61 (0.97) | 1.40 (0.59) | 0.371 a |
| T10 | 1.53 (0.41) | 1.70 (0.95) | 1.41 (0.34) | 0.300 a |
| T11 | 1.43 (0.66) | 1.59 (0.54) | 1.29 (0.33) | 0.219 a |
| T12 | 1.19 (0.38) | 1.63 (0.90) | 1.38 (0.43) | 0.274 a |
| All Patients | Age < 13 | Age > 13 | Age < 14 | Age > 14 | |
|---|---|---|---|---|---|
| r (p value) | r (p value) | r (p value) | r (p value) | r (p value) | |
| Thoracic curve | n = 25 | n = 13 | n = 12 | n = 14 | n = 11 |
| T8 | - | - | - | - | 0.703 (0.016) |
| T9 | - | - | - | - | 0.679 (0.022) |
| T10 | 0.462 (0.020) | - | - | - | 0.703 (0.016) |
| T11 | 0.465 (0.019) | - | 0.587 (0.045) | - | 0.745 (0.009) |
| T12 | 0.547 (0.005) | - | 0.591 (0.043) | - | - |
| Thoracolumbar curve | n = 32 | n = 15 | n = 17 | n = 19 | n = 10 |
| T1 | - | - | - | - | 0.642 (0.046) |
| T4 | −0.388 (0.031) | −0.571 (0.026) | - | −0.623 (0.004) | - |
| T6 | - | - | −0.503 (0.039) | - | - |
| T7 | - | - | −0.527 (0.030) | - | - |
| T8 | - | - | −0.582 (0.014) | - | - |
| T9 | - | - | −0.561 (0.019) | - | - |
| Lumbar curve | n = 26 | n = 10 | n = 16 | n = 10 | n = 16 |
| T1 | - | −0.835 (0.010) | - | - | - |
| T2 | - | −0.938 (0.001) | - | - | - |
| T8 | - | - | 0.527 (0.036) | 0.613 (0.020) | - |
| T9 | 0.394 (0.046) | - | 0.662 (0.005) | - | - |
| T11 | - | - | 0.507 (0.045) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grivas, T.B.; Jevtic, N.; Ljubojevic, D.; Pjanic, S.; Golic, F.; Vasiliadis, E. Segmental Rib Index and Spinal Deformity: Scoliogenic Implications. Healthcare 2023, 11, 3004. https://doi.org/10.3390/healthcare11223004
Grivas TB, Jevtic N, Ljubojevic D, Pjanic S, Golic F, Vasiliadis E. Segmental Rib Index and Spinal Deformity: Scoliogenic Implications. Healthcare. 2023; 11(22):3004. https://doi.org/10.3390/healthcare11223004
Chicago/Turabian StyleGrivas, Theodoros B., Nikola Jevtic, Danka Ljubojevic, Samra Pjanic, Filip Golic, and Elias Vasiliadis. 2023. "Segmental Rib Index and Spinal Deformity: Scoliogenic Implications" Healthcare 11, no. 22: 3004. https://doi.org/10.3390/healthcare11223004