
Polish Adaptation and Psychometric Validation of the PREM-C9 Questionnaire for Patients with Chronic Obstructive Pulmonary Disease
 ,
,
Abstract
:1. Introduction
- To create a Polish adaptation of the PREM-C9.
- To determine the psychometric characteristics of the questionnaire used under Polish conditions.
- To provide knowledge regarding the characteristics and the role of the PREM-C9 in non-English-speaking countries, allowing for cross-cultural comparisons, determining further possibilities of using it, and generalizing the results obtained to other populations.
2. Materials and Methods
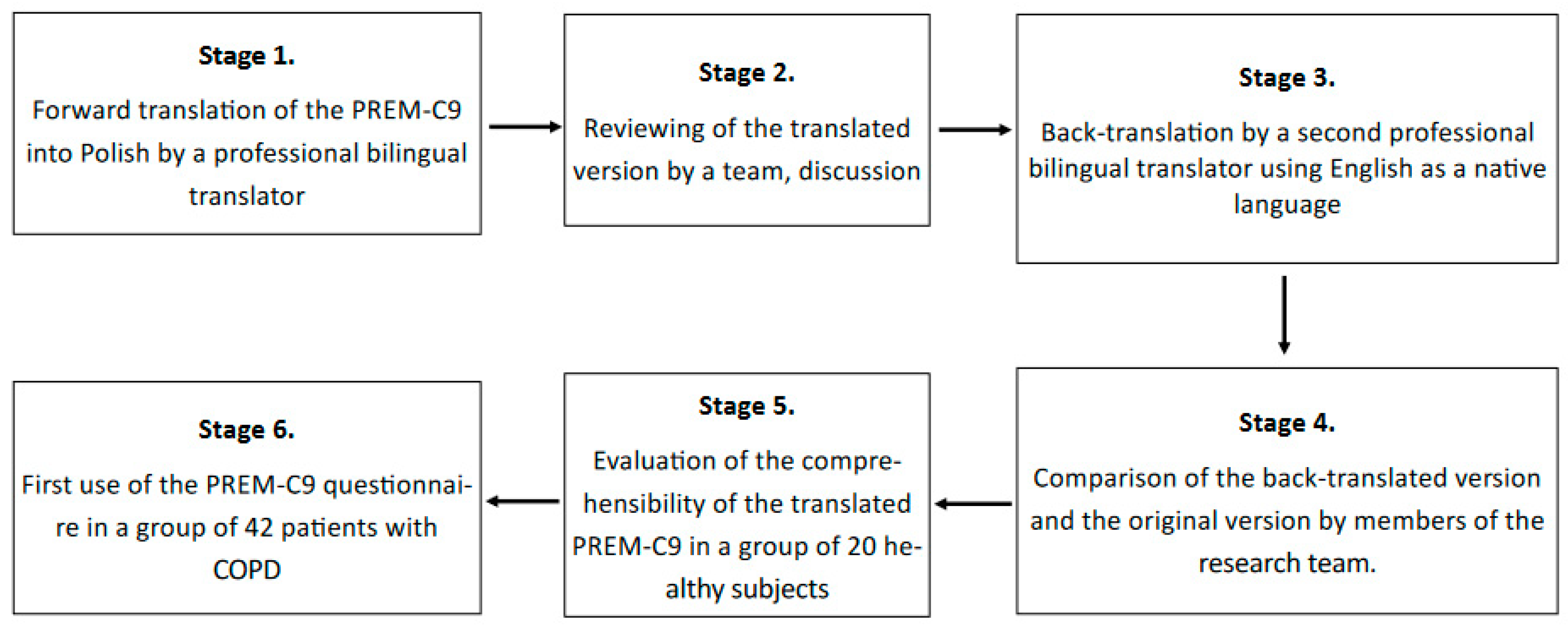
2.1. The Adaptation Procedure
- Forward translation of the PREM-C9 into Polish by a professional bilingual translator with Polish as a native language.
- Reviewing the translated version of the PREM-C9 by the team, including pneumonologists and the research team members. This stage did not provide any significant changes to the Polish version of the questionnaire.
- Back translation made by a professional bilingual translator with English as a native language.
- Comparison of the back-translated version with the original text. This stage did not provide any significant changes; only minor revisions were introduced.
- Evaluation of the comprehensibility of the translated version in a group of 20 healthy volunteers who assessed whether each of the questions was understandable to them.
- The first use of the PREM-C9 questionnaire in a group of 42 patients with COPD to validate the tool and test its psychometric features. The material was collected from patients by a trained interviewer, or patients answered by themselves by filling out a paper version of the questionnaire. The questionnaire was made available both in paper form and in a digital version. The use of the electronic version of the questionnaire was caused by the COVID-19 pandemic and resulted from the need to limit interpersonal contacts.
2.2. Participants
- -
- A patient diagnosed with COPD according to the GOLD criteria from 2022;
- -
- A patient expressing informed consent to participate in the study;
- -
- A patient not hospitalized at the time of the study due to COPD exacerbation or other reasons;
- -
- A patient who was able to answer questions.
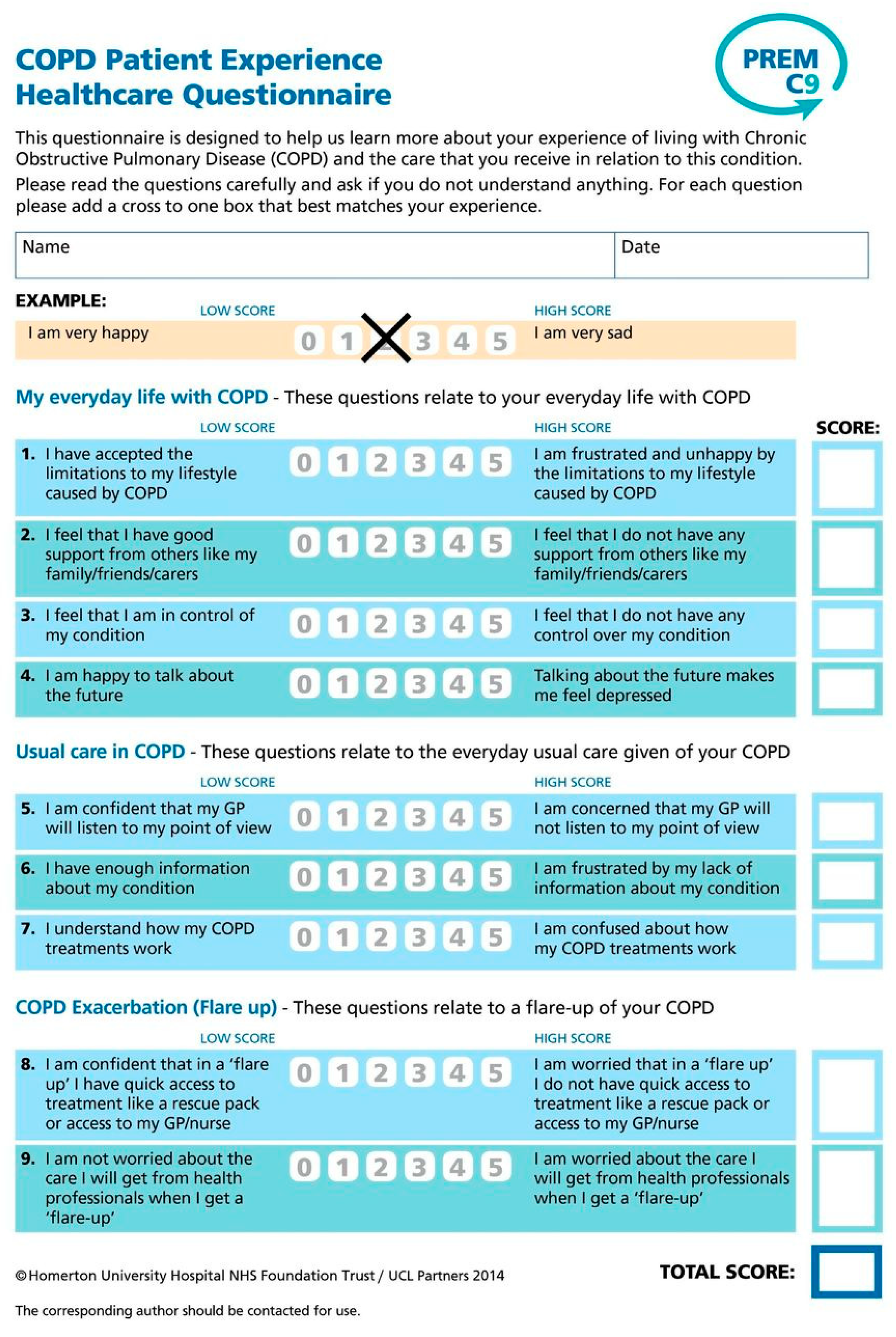
2.3. Measures
- -
- My everyday life with COPD (4 questions);
- -
- Usual care in COPD (3 questions);
- -
- COPD exacerbations/flare-ups (2 questions).
2.4. Statistical Methods and Calculations
3. Results
3.1. Assessment of Psychometric Characteristics
Validity of the PREM-C9 Questionnaire
3.2. The Reliability of PREM-C9 Questionnaire
4. Discussion
5. Implications and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; Montes de Oca, M.; et al. Global initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Melén, E.; DeMeo, D.L.; Breyer-Kohansal, R.; Faner, R. Pathogenesis of chronic obstructive pulmonary disease: Understanding the contributions of gene-environment interactions across the lifespan. Lancet Respir. Med. 2022, 10, 512–524. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, S.; Jarvis, D.; Darnton, A.; Hutchings, S.; Sadhra, S.; Fishwick, D.; Rushton, L.; Cullinan, P. The occupations at increased risk of COPD: Analysis of lifetime job-histories in the population-based UK Biobank Cohort. Eur. Respir. J. 2019, 54, 1900186. [Google Scholar] [CrossRef]
- Bourbeau, J.; Doiron, D.; Biswas, S.; Smith, B.M.; Benedetti, A.; Brook, J.R.; Aaron, S.D.; Chapman, K.R.; Hernandez, P.; Maltais, F.; et al. Ambient air pollution and dysanapsis: Associations with lung function and chronic obstructive pulmonary disease in the Canadian Cohort Obstructive Lung Disease Study. Am. J. Respir. Crit. Care Med. 2022, 206, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Wytyczne Oceny Technologii Medycznych. Agencja Oceny Technologii Medycznych i Taryfikacji, Warsaw. 2016. Available online: https://www.aotm.gov.pl/media/2020/07/20160913_Wytyczne_AOTMiT-1.pdf (accessed on 15 August 2023).
- Patient Charter. Global Allergy & Airways Patient Platform. Available online: https://gaapp.org/diseases/copd/patient-charter/?_gl=1*att4co*_ga*MTc2NzQ3MzU1OS4xNjkyODEwNTc0*_ga_8GH0BEJX5C*MTY5MjgxMDU3NC4xLjEuMTY5MjgxMDU3NS41OS4wLjA.&_ga=2.182628398.901915781.1692810578-1767473559.1692810574 (accessed on 22 August 2023).
- Food and Drug Administration. Value and Use of Patient-Reported Outcomes (PROs) in Assessing Effects of Medical Devices CDRH Strategic Priorities. CDRH Strategic Priorities 2016–2017. Available online: https://www.fda.gov/downloads/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacco/CDRH/CDRHVisionandMission/UCM588576.pdf (accessed on 18 August 2023).
- Valderas, J.M.; Alonso, J.; Guyatt, G.H. Measuring patient-reported outcomes: Moving from clinical trials into clinical practice. Med. J. Aust. 2008, 189, 93–94. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, J.; Gooding, K.; Gibbons, E.; Dalkin, S.; Wright, J.; Valderas, J.; Black, N. How do patient reported outcome measures (PROMs) support clinician-patient communication and patient care? A realist synthesis. J. Patient Rep. Outcomes 2018, 2, 42. [Google Scholar] [CrossRef]
- Jamieson Gilmore, K.; Corazza, I.; Coletta, L.; Allin, S. The uses of Patient Reported Experience Measures in health systems: A systematic narrative review. Health Policy 2023, 128, 1–10. [Google Scholar] [CrossRef]
- Sarri, G.; Freitag, A.; Szegvari, B.; Mountian, I.; Brixner, D.; Bertelsen, N.; Kaló, Z.; Upadhyaya, S. The role of patient experience in the value assessment of complex technologies—Do HTA Bodies need to reconsider how value is assessed? Health Policy 2021, 125, 593–601. [Google Scholar] [CrossRef]
- Flott, K.M.; Graham, C.; Darzi, A.; Mayer, E. The challenges of using patient-reported feedback and how they might be addressed. BJM Qual. Saf. 2017, 26, 502–507. [Google Scholar] [CrossRef]
- De Rosis, S.; Cerasuolo, D.; Nuti, S. Using patient-reported measures to drive change in healthcare: The experience of the digital, continuous and systematic PREMs observatory in Italy. BMC Serv. Res. 2020, 20, 315. [Google Scholar] [CrossRef]
- Hodson, M.; Roberts, C.M.; Andrew, S.; Graham, L.; Jones, P.W.; Yorke, J. Development and first validation of a patient-reported experience measure in chronic obstructive pulmonary disease (PREM-C9). Thorax 2019, 74, 600–603. [Google Scholar] [CrossRef]
- Młyńczak, K.; Golicki, D. Przegląd właściwości psychometrycznych kwestionariuszy oceny jakości życia związanych ze zdrowiem (HRQOL). Pol. Prz. Nauk. Zdr. 2016, 4, 415–421. [Google Scholar]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation and cultural adaptation process for Patient-Reported outcomes (PRO) Measures: Report of the ISPOR Task Force for translation and cultural adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Fletcher, C.M. The clinical diagnosis of pulmonary emphysema—An experimental study. Proc. R. Soc. Med. 1952, 45, 577–584. [Google Scholar]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Leidy, N.K. Development and first validation of the COPD assessment test. Eur. Resp. J. 2009, 34, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Majkowicz, M.; de Walden-Gałuszko, K.; Chojnacka-Szawłowska, G. Model Oceny Jakości Opieki Paliatywnej Realizowanej w Warunkach Stacjonarnych; Akademia Medyczna w Gdańsku: Gdańsk, Poland, 2021; p. 94. [Google Scholar]
- EQ-5D-5L. Available online: https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/ (accessed on 20 August 2023).
- Gerlinger, C.; Bamber, L.; Leverkus, F.; Schwenke, C.; Haberland, C.; Schmidt, G.; Endrikat, J. Comparing the EQ-5D-5L utility index based on value sets of different countries: Impact on the interpretation of clinical study results. BMC Res. Notes 2019, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.A.; Evans, R.A.; Greening, N.J.; Roberts, M.C.; Toms, N.; Hodson, M.; Steiner, M.C. Measuring the experience of living with COPD and receiving medical care in people with COPD. Eur. Respir. J. 2020, 56, 956. [Google Scholar] [CrossRef]
- Bandurska, E. The voice of patients really matters: Using Patient-Reported Outcomes and Experiences Measures to assess effectiveness of home-based integrated care—A scoping review of practice. Healthcare 2023, 11, 98. [Google Scholar] [CrossRef] [PubMed]
- Moharra, M.; Bayes, B.; Llupia, A.; Almazan, C. Cross-cultural adaptation and face validity of the PREM-C9 version of the Patient Reported Experience Measure in patients with Chronic Obstructive Pulmonary Disease. XPA Health Com. 2021, 4, 1–9. [Google Scholar]
- Chaplin, E.; Coope, D.; Zatloukal, J.; Ward, S.; Singh, S.J.; Houchen-Wolloff, L. The minimum important difference for the PREM-9 following a course of Pulmonary Rehabilitation (PR). Eur. Resp. J. 2022, 60, 2899. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press, Inc.: New York, NY, USA, 2008. [Google Scholar]
- Bosworth, A.; Cox, M.; O’Brien, A.; Jones, P.; Sargeant, I.; Elliott, A.; Bukhari, M. Development and validation of a Patient Reported Experience Measure (PREM) for patients with rheumatoid arthritis (RA) and other rheumatic conditions. Curr. Rheumatol. Rev. 2015, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Moody, L.; Benn, S.; Luciano, I.; Ingale, S.; Singh, S. Validation of a real-time patient-reported experience measurement tool for cancer patients in Ontario. J. Clin. Oncol. 2016, 34, 174. [Google Scholar] [CrossRef]
- Waldreus, N.; Jaarsma, T.; Ivarsson, B.; Stromberg, A.; Arestedt, K.; Kiellstrom, B. Development and validation of a questionnaire to measure patients experiences of health care in pulmonary arterial hypertension outpatient clinics. Heart Lung Circ. 2019, 28, 1074–1081. [Google Scholar] [CrossRef]
- Mihaljevic, A.L.; Doerr-Harim, C.; Kalkum, E.; Strunk, G. Measuring patient centeredness with German language Patient-Reported Experience Measures (PREM)—A systematic review and qualitative analysis according to COSMIN. PLoS ONE 2022, 17, e0264045. [Google Scholar] [CrossRef]
- Hinami, K.; Smith, J.; Deamant, C.D.; DuBeshter, K.; Trick, W.E. When do patient-reported outcome measures inform readmission risk? J. Hosp. Med. 2015, 10, 294–300. [Google Scholar] [CrossRef]
- El Miedany, Y.; El Gaafary, M.; El Arousy, N.; Ahmed, I.; Youssef, S.; Palmer, D. Arthritis education: The integration of patient-reported outcome measures and patient self-management. Clin. Exp. Rheumatol. 2012, 30, 899–904. [Google Scholar]
- Santana, M.J.; Feeny, D. Framework to assess the effects of using patient-reported outcome measures in chronic care management. Qual. Life Res. 2014, 23, 1505–1513. [Google Scholar] [CrossRef]
- Greenhalgh, J.; Meadows, K. The effectiveness of the use of patient-based measures of health in routine practice in improving the process and outcomes of patient care: A literature review. J. Eval. Clin. Pract. 1999, 5, 401–416. [Google Scholar] [CrossRef]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaest. 2017, 11, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Aithal, A.; Aithal, P.S. Development and validation of survey questionnaire & experimental data—A systematical review-based statistical approach. Int. J. Manag. Technol. Soc. Sci. 2020, 5, 233–251. [Google Scholar]



{kind=link}
{kind=link}
| Parameter | Sub-Parameter | Number | Percent (%) |
|---|---|---|---|
| Gender | Female | 21 | 50.00 |
| Male | 21 | 50.00 | |
| Place of living | City | 39 | 92.86 |
| Village | 3 | 7.14 | |
| Education level | Primary | 1 | 2.38 |
| Vocational | 15 | 35.71 | |
| Secondary | 23 | 54.76 | |
| Higher | 3 | 7.14 | |
| Self-assessment of material status | Very good | 7 | 16.57 |
| Average | 25 | 59.52 | |
| Poor | 10 | 23.81 | |
| Very poor | 0 | 0.00 | |
| Living alone | Yes | 11 | 26.19 |
| No | 31 | 73.81 |
| Questionnaire | The Average of the Points Obtained | % of Max Points (Showing The Worst State) | Median | SD |
|---|---|---|---|---|
| PREM-C9 | 9.33 | 20.73 | 6.5 | 6.98 |
| CAT | 17.02 | 42.63 | 16 | 8.90 |
| EQ-5D-5L | 10.07 | 40.28 | 9 | 4.27 |
| HADS A (Anxiety) | 4.09 | 19.48 | 3 | 4.05 |
| HADS D (Depression) | 3.29 | 15.67 | 2 | 3.27 |
| Kaiser–Meyer–Olkin Test and Bartlett’s Test | ||
|---|---|---|
| KMO measure of sampling adequacy | 0.675 | |
| Bartlett’s sphericity test | Approximated chi-squared value | 108.382 |
| Df | 36 | |
| Significance | 0.000 | |
| Pair of Variables (Questionnaires) | Spearman’s Rank Order Correlation | ||
|---|---|---|---|
| N | Rho | p | |
| CAT and PC-9 | 42 | 0.440 | 0.003 |
| EQ-5D-5L and PC-9 | 42 | 0.387 | 0.011 |
| EQ VAS and PC-9 | 41 | −0.346 | 0.027 |
| HADS-A and PC-9 | 42 | 0.371 | 0.015 |
| HADS-D and PC-9 | 42 | 0.387 | 0.011 |
| P-C9 1 | P-C9 2 | P-C9 3 | P-C9 4 | P-C9 5 | P-C9 6 | P-C9 7 | P-C9 8 | P-C9 9 | |
|---|---|---|---|---|---|---|---|---|---|
| P-C9 1 | 0.51 | 0.48 | 0.28 | −0.07 | 0.45 | 0.33 | 0.06 | 0.25 | |
| p = 0.001 | p = 0.001 | p = 0.072 | p = 0.672 | p = 0.003 | p = 0.034 | p = 0.723 | p = 0.104 | ||
| P-C9 2 | 0.51 | 0.38 | 0.16 | 0.15 | 0.48 | 0.15 | 0.20 | 0.16 | |
| p = 0.001 | p = 0.014 | p = 0.313 | p = 0.351 | p = 0.001 | p = 0.345 | p = 0.211 | p = 0.313 | ||
| P-C9 3 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | |
| p = 0.001 | p = 0.014 | p = 0.000 | p = 0.566 | p = 0.009 | p = 0.184 | p = 0.108 | p = 0.014 | ||
| P-C9 4 | 0.28 | 0.16 | 0.54 | −0.14 | 0.26 | 0.08 | −0.05 | 0.09 | |
| p = 0.072 | p = 0.313 | p = 0.000 | p = 0.365 | p = 0.102 | p = 0.607 | p = 0.755 | p = 0.557 | ||
| P-C9 5 | −0.07 | 0.15 | −0.09 | −0.14 | 0.17 | 0.08 | 0.43 | 0.20 | |
| p = 0.672 | p = 0.351 | p = 0.566 | p = 0.365 | p = 0.285 | p = 0.614 | p = 0.005 | p = 0.204 | ||
| P-C9 6 | 0.45 | 0.48 | 0.40 | 0.26 | 0.17 | 0.53 | 0.27 | 0.31 | |
| p = 0.003 | p = 0.001 | p = 0.009 | p = 0.102 | p = 0.285 | p = 0.000 | p = 0.081 | p = 0.046 | ||
| P-C9 7 | 0.33 | 0.15 | 0.21 | 0.08 | 0.08 | 0.53 | 0.41 | 0.51 | |
| p = 0.034 | p = 0.345 | p = 0.184 | p = 0.607 | p = 0.614 | p = 0.000 | p = 0.006 | p = 0.001 | ||
| P-C9 8 | 0.06 | 0.20 | 0.25 | −0.05 | 0.43 | 0.27 | 0.41 | 0.48 | |
| p = 0.723 | p = 0.211 | p = 0.108 | p = 0.755 | p = 0.005 | p = 0.081 | p = 0.006 | p = 0.001 | ||
| P-C9 9 | 0.25 | 0.16 | 0.38 | 0.09 | 0.20 | 0.31 | 0.51 | 0.48 | |
| p = 0.104 | p = 0.313 | p = 0.014 | p = 0.557 | p = 0.204 | p = 0.046 | p = 0.001 | p = 0.001 |
| The Question Number in PREM-C9 | Correlation with the Sum for P-C9 | p |
|---|---|---|
| P-C9 1 | 0.6 | 0.000 |
| P-C9 2 | 0.6 | 0.000 |
| P-C9 3 | 0.7 | 0.000 |
| P-C9 4 | 0.4 | 0.000 |
| P-C9 5 | 0.4 | 0.000 |
| P-C9 6 | 0.7 | 0.000 |
| P-C9 7 | 0.6 | 0.000 |
| P-C9 8 | 0.6 | 0.000 |
| P-C9 9 | 0.6 | 0.000 |
| Questionnaire | PREM-C9 Total (Damps-Konstanska et al.) | PREM-C9 Total (Hodson et al., 2019) [14] | PREM-C9 Total (Jones et al., 2020) [23] |
|---|---|---|---|
| CAT | Rho = 0.44 p = 0.003 | Rho = 0.42 p = 0.03 | Rho = 0.27 p = 0.03 |
| HADS-Anxiety | Rho = 0.370864 p = 0.016 | Rho = 0.30 p < 0.005 | Rho = 0.4 p = 0.001 |
| HADS-Depression | Rho = 0.387405 p = 0.011 | Rho = 0.41 p < 0.005 | Rho = 0.21 p = 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damps-Konstańska, I.; Ciećko, W.; Jassem, E.; Bandurski, T.; Bosek, D.; Olszewska-Karaban, M.; Bandurska, E. Polish Adaptation and Psychometric Validation of the PREM-C9 Questionnaire for Patients with Chronic Obstructive Pulmonary Disease. Healthcare 2023, 11, 2746. https://doi.org/10.3390/healthcare11202746
Damps-Konstańska I, Ciećko W, Jassem E, Bandurski T, Bosek D, Olszewska-Karaban M, Bandurska E. Polish Adaptation and Psychometric Validation of the PREM-C9 Questionnaire for Patients with Chronic Obstructive Pulmonary Disease. Healthcare. 2023; 11(20):2746. https://doi.org/10.3390/healthcare11202746
Chicago/Turabian StyleDamps-Konstańska, Iwona, Weronika Ciećko, Ewa Jassem, Tomasz Bandurski, Dominika Bosek, Marzena Olszewska-Karaban, and Ewa Bandurska. 2023. "Polish Adaptation and Psychometric Validation of the PREM-C9 Questionnaire for Patients with Chronic Obstructive Pulmonary Disease" Healthcare 11, no. 20: 2746. https://doi.org/10.3390/healthcare11202746