
Assessment of Saudi Society’s Knowledge Regarding Hypothyroidism and Its Neuropsychiatric Clinical Manifestations
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van der Spek, A.H.; Fliers, E.; Boelen, A. The classic pathways of thyroid hormone metabolism. Mol. Cell. Endocrinol. 2017, 458, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Alyahya, A.; AlNaim, A.; AlBahr, A.W.; Almansour, F.; Elshebiny, A. Knowledge of Thyroid Disease Manifestations and Risk Factors Among Residents of the Eastern Province, Saudi Arabia. Cureus 2021, 13, e13035. [Google Scholar] [CrossRef] [PubMed]
- Samuels, M.H. Psychiatric and cognitive manifestations of hypothyroidism. Curr. Opin. Endocrinol. Diabetes Obes. 2014, 21, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.D.; Tremont, G. Neuropsychiatric aspects of hypothyroidism and treatment reversibility. Minerva Endocrinol. 2007, 32, 49–65. [Google Scholar] [PubMed]
- Almousa, A.I.S.; Alotaibi, A.M.D. Survey of awareness of thyroid disorders among the Riyadh population, Central Region of Saudi Arabia. Egypt. J. Hosp. Med. 2018, 72, 4039–4044. [Google Scholar] [CrossRef]
- Almuzaini, A.; Alshareef, B.; Alghamdi, S.; Munshy, A.A.; Aljarallah, A.K.; Salman, S.A.; Alroqi, K.S.; Alkhaldi, R.D. Assessment of knowledge and awareness regarding thyroid disorders among Saudi people. IJDMC 2019, 3, 1070–1076. [Google Scholar] [CrossRef]
- Alqahtani, S.M. Awareness of thyroid disorders among the Saudi population. Age 2021, 20, 377. [Google Scholar]
- Sethi, B.; Khandelwal, D.; Vyas, U. A cross-sectional survey to assess knowledge, attitude, and practices in patients with hypothyroidism in India. Thyroid. Res. Pract. 2018, 15, 15–22. [Google Scholar] [CrossRef]
- Strikić Đula, I.; Pleić, N.; Babić Leko, M.; Gunjača, I.; Torlak, V.; Brdar, D.; Punda, A.; Polašek, O.; Hayward, C.; Zemunik, T. Epidemiology of Hypothyroidism, Hyperthyroidism and Positive Thyroid Antibodies in the Croatian Population. Biology 2022, 11, 394. [Google Scholar] [CrossRef] [PubMed]
- Abu-Helalah, M.; Alshraideh, H.A.; Al-Sarayreh, S.A.; Al Shawabkeh, A.H.K.; Nesheiwat, A.; Younes, N.; Al-Hader, A. A cross-sectional study to assess the prevalence of adult thyroid dysfunction disorders in Jordan. Thyroid 2019, 29, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Aljabri, K.S.J.; Alnasser, I.M.; Facharatz, B.S.; Bokhari, S.A.; Alshareef, M.A.; Khan, P.M. The frequency of hypothyroidism in Saudi community-based hospital: A retrospective single centre study. Trends Diabetes Metab 2019, 2, 1–4. [Google Scholar] [CrossRef]
- Qiu, Y.; Hu, Y.; Xing, Z.; Fu, Q.; Zhu, J.; Su, A. Birth control pills and risk of hypothyroidism: A cross-sectional study of the National Health and Nutrition Examination Survey, 2007–2012. BMJ Open 2021, 11, e046607. [Google Scholar] [CrossRef] [PubMed]
- Center, C.T. Hypothyroidism. Available online: https://columbiasurgery.org/conditions-and-treatments/hypothyroidism (accessed on 24 May 2022).
- Randolph, G.W. Surgery of the Thyroid and Parathyroid Glands; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Mathew, P.; Rawla, P.; Fortes, K. Hyperthyroidism (Nursing). In StatPearls [Internet]; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]



{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Age (years) | 38.86 ± 13.84 |
| Gender | |
| Females | 1571 (77.9%) |
| Males | 445 (22.1%) |
| Region | |
| Central region | 1384 (68.7%) |
| Eastern region | 145 (7.2%) |
| Western region | 253 (12.5%) |
| Northern region | 31 (1.5%) |
| Southern region | 203 (10.1%) |
| Marital status | |
| Married | 1254 (62.2%) |
| Unmarried | 762 (37.8%) |
| Educational level | |
| School education | 378 (18.8%) |
| University | 1430 (70.9%) |
| Postgraduate | 208 (10.3%) |
| Income | |
| Enough and can save | 666 (33%) |
| Enough | 1141 (56.6%) |
| Not enough | 144 (7.1%) |
| Not enough/in debt | 65 (3.2%) |
| Resources of information | |
| Health care practitioners | 218 (10.8%) |
| Family/Friends | 1179 (58.4%) |
| Social media platforms | 217 (10.8%) |
| Scientific and Medical Journals/Books | 404 (20%) |
| Health care worker? | |
| Yes | 133 (6.6%) |
| No | 1883 (93.4%) |
| Items for Knowledge Assessment | Correct n (%) | Incorrect n (%) | I Do Not Know n (%) |
|---|---|---|---|
| General Knowledge | |||
| Hypothyroidism is caused by reduced levels of thyroid hormone levels | 1521 (75.4%) | 74 (3.7%) | 421 (20.9%) |
| The ability to live without the thyroid gland | 966 (47.9%) | 508 (25.2%) | 542 (26.9%) |
| Hypothyroidism is a communicable disease | 1913 (94.9%) | 8 (0.4%) | 95 (4.7%) |
| Males are more likely to develop hypothyroidism | 1156 (57.3%) | 58 (2.9%) | 802 (39.8%) |
| Females are more likely to develop hypothyroidism | 1204 (59.7%) | 111 (5.5%) | 701 (34.8%) |
| Those with a positive family history are more likely to develop hypothyroidism | 1136 (56.3%) | 318 (15.8%) | 562 (27.9%) |
| Decreased iodine intake leads to hypothyroidism | 942 (46.7%) | 87 (4.3%) | 987 (49%) |
| Children can develop hypothyroidism | 943 (46.8%) | 217 (10.8%) | 856 (42.5%) |
| Risk Factors of Hypothyroidism | |||
| Smoking | 260 (12.9%) | 575 (28.5%) | 1181 (58.6%) |
| Autoimmune disease | 519 (25.7%) | 229 (11.4%) | 1268 (62.9%) |
| Intake of oral contraceptive pills | 455 (22.6%) | 322 (16.0%) | 1239 (61.5%) |
| Being over 60 increases the risk of developing hypothyroidism | 534 (26.5%) | 518 (25.7%) | 964 (47.8%) |
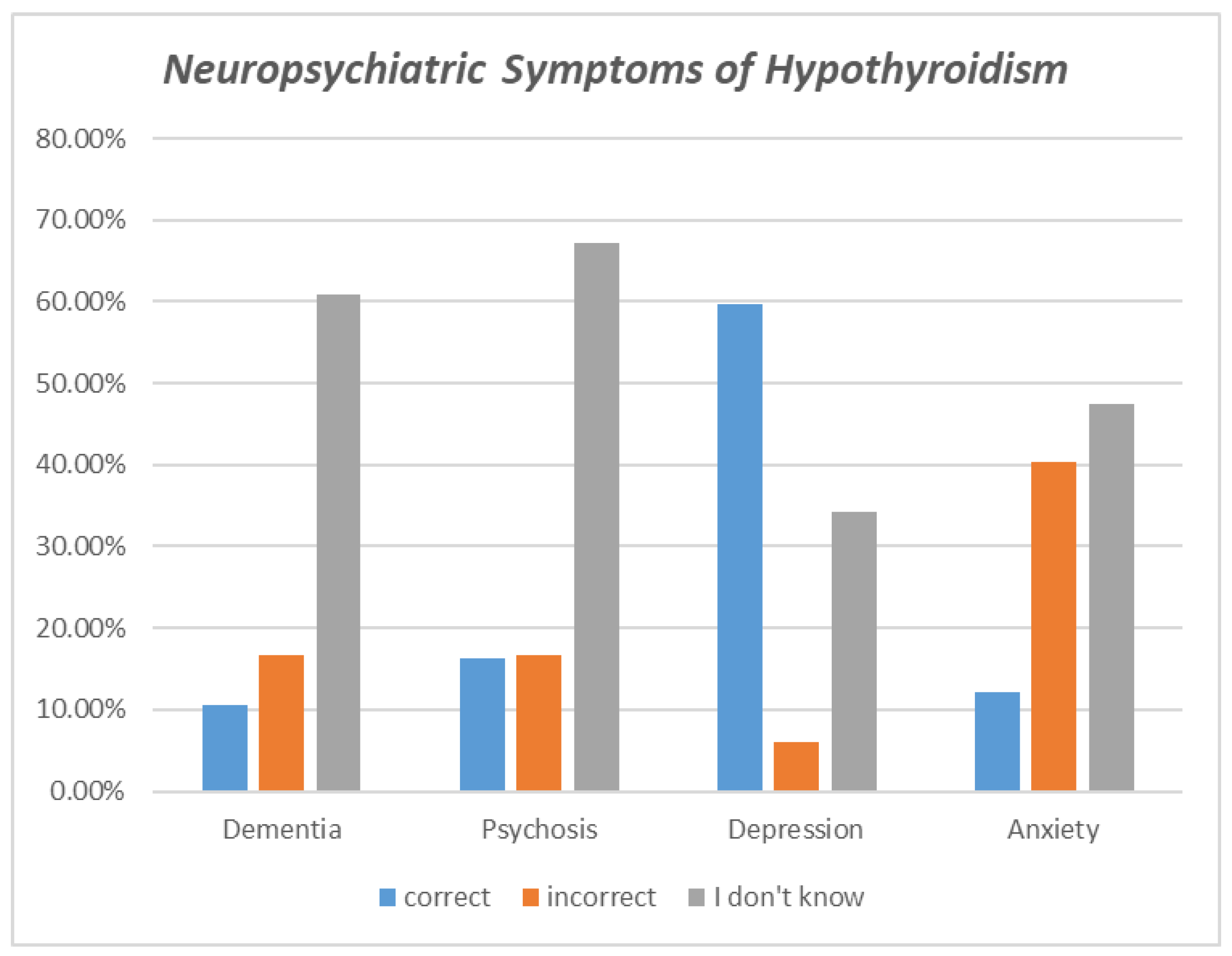
| Neuropsychiatric Symptoms of Hypothyroidism | |||
| Dementia | 212 (10.5%) | 334 (16.6%) | 1225 (60.8%) |
| Psychosis | 329 (16.3%) | 334 (16.6%) | 1353 (67.1%) |
| Depression | 1202 (59.6%) | 122 (6.1%) | 692 (34.3%) |
| Anxiety | 245 (12.2%) | 814 (40.4%) | 957 (47.5%) |
| Symptoms of Hypothyroidism | |||
| Cold intolerance | 1095 (54.3%) | 194 (9.6%) | 727 (36.1%) |
| Constipation | 607 (30.1%) | 322 (13.0%) | 1087 (53.9%) |
| Increased sweating | 437 (21.7%) | 688 (34.1%) | 891 (44.2%) |
| Increased need to urinate | 569 (28.2%) | 286 (14.2%) | 1161 (57.6%) |
| Palpitations | 383 (19.0%) | 693 (34.4%) | 940 (46.6%) |
| Swelling of the neck | 1224 (60.7%) | 240 (11.9%) | 552 (27.4%) |
| Weight gain | 1634(81.1%) | 100 (5%) | 282 (14%) |
| Hand tremors | 399 (19.8%) | 534 (26.5%) | 1083 (53.7%) |
| Complications of Hypothyroidism | |||
| Thyroid cancer | 433 (21.5%) | 352 (17.5%) | 1231 (61.1%) |
| Irregularities of the menstrual cycle | 1215 (60.3%) | 352 (17.5%) | 716 (35.5%) |
| Increased levels of cholesterol in the blood | 614 (30.5%) | 222 (11%) | 1180 (58.5%) |
| Osteoporosis | 250 (12.4%) | 688 (34.1%) | 1078 (53.5%) |
| Diabetes | 514 (25.5%) | 365 (18.1%) | 1137 (56.4%) |
| Nerve damage | 363 (18%) | 355 (17.6%) | 1298 (64.4%) |
| Infertility | 738 (36.6%) | 286 (14.2%) | 992 (49.2%) |
| Sight issues | 443 (22%) | 374 (18.6%) | 1199 (59.5%) |
| Excessive body hair in females | 415 (20.6%) | 570 (28.3%) | 1031 (51.1%) |
| Hypothyroidism Treatment | |||
| Biopsy must be performed to diagnose hypothyroidism | 976 (48.4%) | 438 (21.7%) | 602 (29.9%) |
| Thyroid-stimulating oral medication | 1616 (80.2%) | 45 (2.2%) | 355(17.6%) |
| Surgical removal of the thyroid gland | 935 (46.4%) | 432 (21.4%) | 649 (32.2%) |
| Variables | Mean ± SD | p-Value |
|---|---|---|
| Age (years) | ||
| 18–26 (n = 567) | 16.22 ± 7.15 | 0.037 * |
| 27–40 (n = 491) | 15.32 ± 6.95 | |
| 41 and above (n = 958) | 15.37 ± 6.83 | |
| Gender | ||
| Females (n = 1571) | 16.44 ± 6.22 | <0.001 * |
| Males (n = 445) | 12.61 ± 7.96 | |
| Region | ||
| Central region (n = 1384) | 15.76 ± 6.86 | 0.177 |
| Eastern region (n = 145) | 14.74 ± 6.37 | |
| Western region (n = 253) | 14.91 ± 7.24 | |
| Northern region (n = 31) | 15.42 ± 7.01 | |
| Southern region (n = 203) | 15.98 ± 6.36 | |
| Marital status | ||
| Married (n = 1254) | 15.42 ± 6.65 | 0.110 |
| Unmarried (n = 762) | 15.90 ± 7.12 | |
| Educational level | ||
| No education (n = 20) | 14.95 ± 6.53 | 0.562 |
| School education (n = 358) | 15.34 ± 6.86 | |
| University (n = 1430) | 15.59 ± 6.77 | |
| Higher education (n = 208) | 16.15 ± 7.24 | |
| Income | ||
| Enough and can save (n = 666) | 16.21 ± 7.08 | 0.012 * |
| Enough (n = 1141) | 15.33 ± 6.61 | |
| Not enough (n = 144) | 15.65 ± 6.91 | |
| Not enough/ in debt (n = 65) | 13.90 ± 7.57 | |
| Source of information | ||
| Healthcare practitioners (n = 218) | 18.8 ± 6.5 | <0.001 * |
| Family and Friends (n = 1179) | 14.5 ± 6.2 | |
| Social media platforms (n = 217) | 14.3 ± 7.3 | |
| Scientific and Medical Journals/Books (n = 404) | 17.8 ± 7.5 | |
| Health care worker | ||
| Yes (n = 133) | 20.24 ± 7.14 | 0.494 |
| No (n = 1883) | 15.27 ± 6.69 | |
| Variables | Coefficients | Standard Error | t Stat | p-Value | Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower 95% | Upper 95% | |||||
| Age | ||||||
| 18–26 | Reference | |||||
| 27–40 | −0.054 | 0.403 | −0.134 | 0.893 | −0.844 | 0.736 |
| 46 and up | −0.066 | 0.347 | −0.192 | 0.848 | −0.748 | 0.615 |
| Gender | ||||||
| Female | Reference | |||||
| male | −3.686 | 0.349 | −10.564 | 0.0001 * | −4.370 | −3.002 |
| Income | ||||||
| Enough | Reference | |||||
| Enough and can save | 0.731 | 0.315 | 2.32 | 0.02 * | 0.113 | 1.349 |
| Not enough | 0.229 | 0.571 | 0.402 | 0.688 | −0.891 | 1.35 |
| In debt | −1.143 | 0.821 | −1.393 | 0.164 | −2.754 | 0.467 |
| Source of information | ||||||
| Family and Friends | Reference | |||||
| Healthcare practitioners | 4.092 | 0.477 | 8.585 | 0.0001 * | 3.158 | 5.027 |
| Social media platforms | −0.2481 | 0.478 | −0.519 | 0.604 | −1.185 | 0.689 |
| Scientific and Medical Journals/Books | 3.101 | 0.375 | 8.271 | 0.0001 * | 2.366 | 3.836 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzahrani, H.S.; Alshabnan, R.A.; Mokhtar, F.M.; Aleisa, A.I.; AlHedaithi, N.A.; Alotaibi, G.K.; Alamri, T.M.; Aluthaim, W.D.; Alyousef, J.M.; AlSarhan, R.S.; et al. Assessment of Saudi Society’s Knowledge Regarding Hypothyroidism and Its Neuropsychiatric Clinical Manifestations. Healthcare 2023, 11, 277. https://doi.org/10.3390/healthcare11020277
Alzahrani HS, Alshabnan RA, Mokhtar FM, Aleisa AI, AlHedaithi NA, Alotaibi GK, Alamri TM, Aluthaim WD, Alyousef JM, AlSarhan RS, et al. Assessment of Saudi Society’s Knowledge Regarding Hypothyroidism and Its Neuropsychiatric Clinical Manifestations. Healthcare. 2023; 11(2):277. https://doi.org/10.3390/healthcare11020277
Chicago/Turabian StyleAlzahrani, Hayat Saleh, Rand Abdalla Alshabnan, Fatmah Mamdooh Mokhtar, Aljoharah Ibrahim Aleisa, Nora Abdulrahman AlHedaithi, Ghadah Khalid Alotaibi, Tif Meshref Alamri, Wejdan Dia Aluthaim, Jana Mahmoud Alyousef, Reem Saeed AlSarhan, and et al. 2023. "Assessment of Saudi Society’s Knowledge Regarding Hypothyroidism and Its Neuropsychiatric Clinical Manifestations" Healthcare 11, no. 2: 277. https://doi.org/10.3390/healthcare11020277