The Effectiveness of Family Medicine-Driven Interprofessional Collaboration on the Readmission Rate of Older Patients



Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Participants
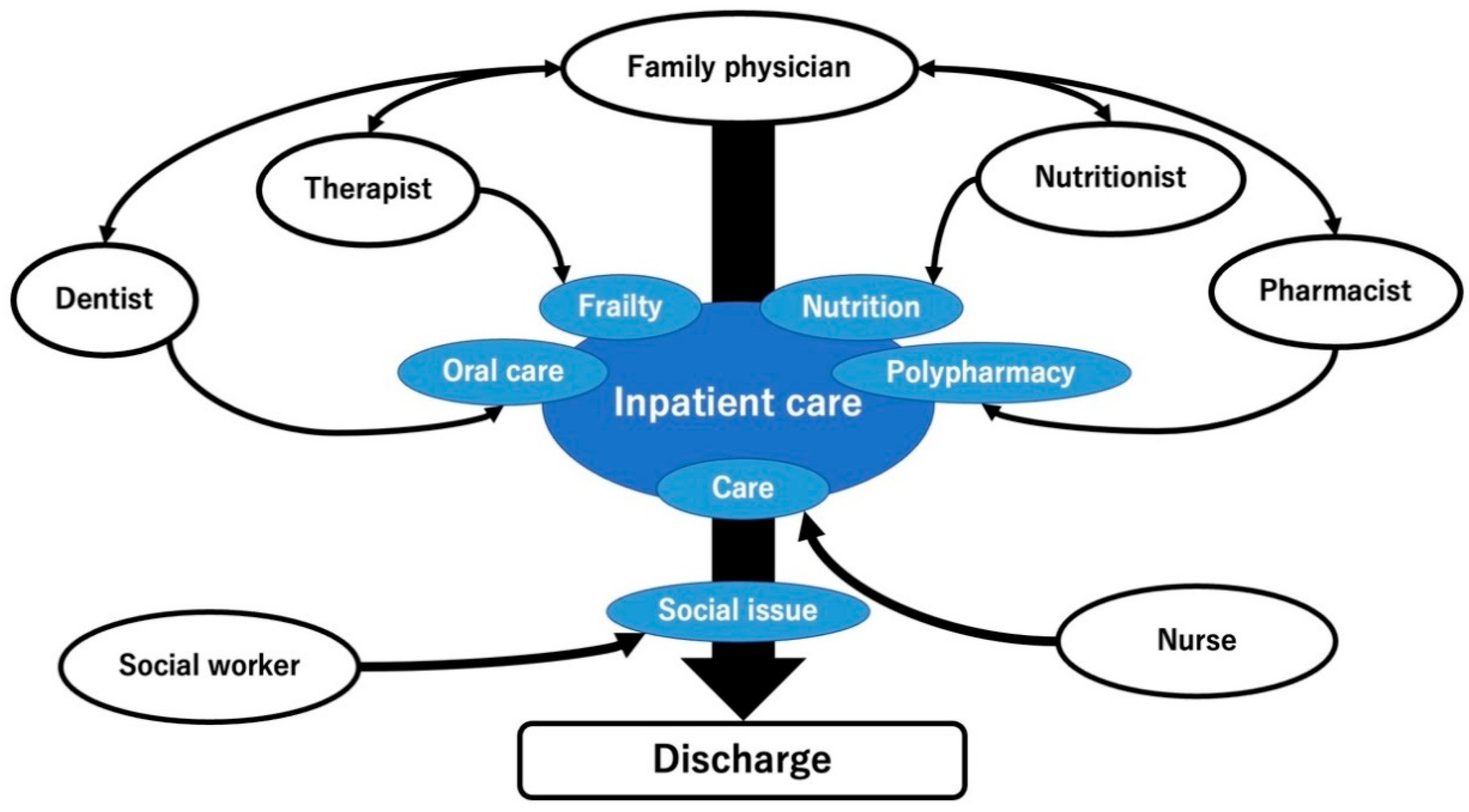
2.3. IPC Intervention in the Rural Hospital
2.3.1. Collaboration with Dentists
2.3.2. Collaboration with Physical and Occupational Therapists
2.3.3. Collaboration with Pharmacists
2.3.4. Collaboration with Nutritionists
2.3.5. Collaboration with Nurses
2.4. Measurements
2.4.1. Primary Outcome
2.4.2. Covariates
2.5. Data Analysis
2.6. Ethical Consideration
3. Results
3.1. Participant Selection
3.2. Demographics of the Participants
3.3. Relationship between IPC and Readmission
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Supper, I.; Catala, O.; Lustman, M.; Chemla, C.; Bourgueil, Y.; Letrilliart, L. Interprofessional collaboration in primary health care: A review of facilitators and barriers perceived by involved actors. J. Public Health 2015, 37, 716–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johannessen, A.K.; Steihaug, S. The significance of professional roles in collaboration on patients’ transitions from hospital to home via an intermediate unit. Scand. J. Caring Sci. 2014, 28, 364–372. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, D.E.; Doucet, S.; Nasser, S.; Godden-Webster, A.L.; Andrews, C.; Kephart, G. Collaboration behind-the-scenes: Key to effective interprofessional education. J. Interprof. Care 2014, 28, 381–383. [Google Scholar] [CrossRef]
- Lygre, H.; Kjome, R.L.S.; Choi, H.; Stewart, A.L. Dental providers and pharmacists: A call for enhanced interprofessional collaboration. Int. Dent. J. 2017, 67, 329–331. [Google Scholar] [CrossRef] [PubMed]
- Ewig, S.; Welte, T.; Chastre, J.; Torres, A. Rethinking the concepts of community-acquired and health-care-associated pneumonia. Lancet Infect. Dis. 2010, 10, 279–287. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Tsuji, S.; Nagai, K.; Sakuramoto-Sadakane, A.; Tamaoka, J.; Oshitani, M.; Ono, T.; Sawada, T.; Shinmura, K.; Kishimoto, H. The relationship between bone density and the oral function in older adults: A cross-sectional observational study. BMC Geriatr. 2021, 21, 591. [Google Scholar] [CrossRef]
- Wiener, R.C.; Shen, C.; Sambamoorthi, N.; Sambamoorthi, U. Preventive dental care in older adults with diabetes. J. Am. Dent. Assoc. 2016, 147, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Müller, F. Oral hygiene reduces the mortality from aspiration pneumonia in frail elders. J. Dent. Res. 2015, 94, 14S–16S. [Google Scholar] [CrossRef] [Green Version]
- Azami-Aghdash, S.; Pournaghi-Azar, F.; Moosavi, A.; Mohseni, M.; Derakhshani, N.; Kalajahi, R.A. Oral health and related quality of life in older people: A systematic review and meta-analysis. Iran. J. Public Health 2021, 50, 689–700. [Google Scholar] [CrossRef]
- Drevet, S.; Bornu, B.C.; Boudissa, M.; Bioteau, C.; Mazière, S.; Merloz, P.; Couturier, P.; Tonetti, J.; Gavazzi, G. One-year mortality after a hip fracture: Prospective study of a cohort of patients aged over 75 years old. Geriatr. Psychol. Neuropsychiatr. Vieil. 2019, 17, 369–376. [Google Scholar] [CrossRef]
- Ohta, R.; Sano, C. Risk of hospital readmission among older patients discharged from the rehabilitation unit in a rural community hospital: A retrospective cohort study. J. Clin. Med. 2021, 10, 659. [Google Scholar] [CrossRef]
- Zhao, Q.; Wang, J.; Nicholas, S.; Maitland, E.; Sun, J.; Jiao, C.; Xu, L.; Leng, A. Health-related quality of life and health service use among multimorbid middle-aged and older-aged adults in China: A cross-sectional study in Shandong Province. Int. J. Environ. Res. Public Health 2020, 17, 9261. [Google Scholar] [CrossRef] [PubMed]
- Sonoda, S. Immobilization and disuse syndrome. Jpn. J. Rehabil. Med. 2015, 52, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Kato, D.; Ryu, H.; Matsumoto, T.; Abe, K.; Kaneko, M.; Ko, M.; Irving, G.; Ramsay, R.; Kondo, M. Building primary care in Japan: Literature review. J. Gen. Fam. Med. 2019, 20, 170–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer-Massetti, C.; Meier, C.R.; Guglielmo, B.J. The scope of drug-related problems in the home care setting. Int. J. Clin. Pharm. 2018, 40, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Chi, W.C.; Wolff, J.; Greer, R.; Dy, S. Multimorbidity and decision-making preferences among older adults. Ann. Fam. Med. 2017, 15, 546–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, M.; van der Borght, C.; Leithaus, M.; Flamaing, J.; Goderis, G. Patients’ perceptions of frequent hospital admissions: A qualitative interview study with older people above 65 years of age. BMC Geriatr. 2020, 20, 332. [Google Scholar] [CrossRef]
- Longman, J.; Passey, M.; Singer, J.; Morgan, G. The role of social isolation in frequent and/or avoidable hospitalisation: Rural community-based service providers’ perspectives. Aust. Health Rev. 2013, 37, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Reeves, S.; Xyrichis, A.; Zwarenstein, M. Teamwork, collaboration, coordination, and networking: Why we need to distinguish between different types of interprofessional practice. J. Interprof. Care 2018, 32, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Sangaleti, C.; Schveitzer, M.C.; Peduzzi, M.; Zoboli, E.L.C.P.; Soares, C.B. Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 2723–2788. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Sakuma, K. Rehabilitation nutrition for sarcopenia with disability: A combination of both rehabilitation and nutrition care management. J. Cachexia Sarcopenia Muscle 2014, 5, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H. Rehabilitation nutrition in general and family medicine. J. Gen. Fam. Med. 2017, 18, 153–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Sarcopenia is associated with worse recovery of physical function and dysphagia and a lower rate of home discharge in Japanese hospitalized adults undergoing convalescent rehabilitation. Nutrition 2019, 61, 111–118. [Google Scholar] [CrossRef]
- Doornebosch, A.J.; Smaling, H.J.A.; Achterberg, W.P. Interprofessional collaboration in long-term care and rehabilitation: A systematic review. J. Am. Med. Dir. Assoc. 2022, 23, 764–777. [Google Scholar] [CrossRef] [PubMed]
- Bingham, J.; Campbell, P.; Schussel, K.; Taylor, A.M.; Boesen, K.; Harrington, A.; Leal, S.; Warholak, T. The discharge companion program: An interprofessional collaboration in transitional care model delivery. Pharmacy 2019, 7, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White-Williams, C.; Shirey, M.; Eagleson, R.; Clarkson, S.; Bittner, V. An interprofessional collaborative practice can reduce heart failure hospital readmissions and costs in an underserved population. J. Card. Fail. 2021, 27, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.H.; Kaldan, G.; Nielsen, B.H.; Kristensen, G.J.; Shiv, L.; Egerod, I. Intensive care professionals’ perspectives on dysphagia management: A focus group study. Aust. Crit. Care 2022, S1036–7314, 00060–00061. [Google Scholar] [CrossRef]
- Shimizu, A.; Ohta, R.; Otani, H.; Sano, C. The contribution of temporal flat lateral position on the mortality and discharge rates of older patients with severe dysphagia. Int. J. Environ. Res. Public Health 2021, 18, 8443. [Google Scholar] [CrossRef]
- Beuscart, J.B.; Petit, S.; Gautier, S.; Wierre, P.; Balcaen, T.; Lefebvre, J.M.; Kambia, N.; Bertoux, E.; Mascaut, D.; Barthélémy, C.; et al. Polypharmacy in older patients: Identifying the need for support by a community pharmacist. BMC Geriatr. 2019, 19, 277. [Google Scholar] [CrossRef] [Green Version]
- Hoel, R.W.; Giddings Connolly, R.M.; Takahashi, P.Y. Polypharmacy Management in Older Patients. Mayo Clin. Proc. 2021, 96, 242–256. [Google Scholar] [CrossRef]
- Corsonello, A.; Abbatecola, A.M.; Fusco, S.; Luciani, F.; Marino, A.; Catalano, S.; Maggio, M.G.; Lattanzio, F. The Impact of Drug Interactions and Polypharmacy on Antimicrobial Therapy in the Elderly. Clin. Microbiol. Infect. 2015, 21, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Visade, F.; Babykina, G.; Puisieux, F.; Bloch, F.; Charpentier, A.; Delecluse, C.; Loggia, G.; Lescure, P.; Attier-Żmudka, J.; Gaxatte, C.; et al. Risk Factors for Hospital Readmission and Death After Discharge of Older Adults from Acute Geriatric Units: Taking the Rank of Admission into Account. Clin. Interv. Aging 2021, 16, 1931–1941. [Google Scholar] [CrossRef] [PubMed]
- Counter, D.; Millar, J.W.T.; McLay, J.S. Hospital Readmissions, Mortality and Potentially Inappropriate Prescribing: A Retrospective Study of Older Adults Discharged from Hospital. Br. J. Clin. Pharmacol. 2018, 84, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Klinge, M.; Aasbrenn, M.; Öztürk, B.; Christiansen, C.F.; Suetta, C.; Pressel, E.; Nielsen, F.E. Readmission of Older Acutely Admitted Medical Patients after Short-Term Admissions in Denmark: A Nationwide Cohort Study. BMC Geriatr. 2020, 20, 203. [Google Scholar] [CrossRef]
- Lu, C.H.; Clark, C.M.; Tober, R.; Allen, M.; Gibson, W.; Bednarczyk, E.M.; Daly, C.J.; Jacobs, D.M. Readmissions and Costs Among Younger and Older Adults for Targeted Conditions During the Enactment of the Hospital Readmission Reduction Program. BMC Health Serv. Res. 2021, 21, 386. [Google Scholar] [CrossRef] [PubMed]
- Perni, S.; Pollack, L.R.; Gonzalez, W.C.; Dzeng, E.; Baldwin, M.R. Moral Distress and Burnout in Caring for Older Adults during Medical School Training. BMC Med. Educ. 2020, 20, 84. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.E.; Cho, S.H. The Influence of Social Support on the Relationship between Emotional Demands and Health of Hospital Nurses: A Cross-Sectional Study. Healthcare 2021, 9, 115. [Google Scholar] [CrossRef]
- Dos Santos, L.M. Stress, Burnout, and Low Self-Efficacy of Nursing Professionals: A Qualitative Inquiry. Healthcare 2020, 8, 424. [Google Scholar] [CrossRef]
- Amin, A.; Deitelzweig, S.; Christian, R.; Friend, K.; Lin, J.; Belk, K.; Baumer, D.; Lowe, T.J. Evaluation of Incremental Healthcare Resource Burden and Readmission Rates Associated with Hospitalized Hyponatremic Patients in the US. J. Hosp. Med. 2012, 7, 634–639. [Google Scholar] [CrossRef]
- Li, R.; Geng, J.; Liu, J.; Wang, G.; Hesketh, T. Effectiveness of Integrating Primary Healthcare in Aftercare for Older Patients after Discharge from Tertiary Hospitals—A Systematic Review and Meta-analysis. Age Ageing 2022, 51, afac151. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Yoshimura, M. Realist evaluation of interprofessional education in primary care through transprofessional role play: What primary care professionals learn together. Educ. Prim. Care 2021, 32, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Kataoka, D.; Sano, C. Effectiveness and challenges in local self-governance: Multifunctional autonomy in Japan. Int. J. Environ. Res. Public Health 2021, 18, 574. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Sano, C. Family medicine education at a rural hospital in Japan: Impact on institution and trainees. Int. J. Environ. Res. Public Health 2021, 18, 6122. [Google Scholar] [CrossRef]
- Ohta, R.; Yawata, M.; Sano, C. Doctor clerk implementation in rural community hospitals for effective task shifting of doctors: A grounded theory approach. Int. J. Environ. Res. Public Health 2022, 19, 9944. [Google Scholar] [CrossRef]
- Koike, T.; Ohta, R.; Matsuda, Y.; Sano, C.; Kanno, T. Oral care awareness and factors related to the burden of nurses at a community hospital in Japan. Healthcare 2022, 10, 1073. [Google Scholar] [CrossRef]
- Ohta, R.; Maeki, N.; Maniwa, S.; Miyakoshi, K. Predicting factors of elderly patients’ discharge to home after rehabilitation in rural Japan: A retrospective cohort study. Rural Remote Health 2021, 21, 6406. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Maejma, S.; Sano, C. Nurses’ contributions in rural family medicine education: A mixed-method approach. Int. J. Environ. Res. Public Health 2022, 19, 3090. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Sano, C. Bedside teaching in rural family medicine education in Japan. Int. J. Environ. Res. Public Health 2022, 19, 6807. [Google Scholar] [CrossRef]
- Olivares-Tirado, P.; Tamiya, N.; Kashiwagi, M.; Kashiwagi, K. Predictors of the highest long-term care expenditures in Japan. BMC Health Serv. Res. 2011, 11, 103. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Bernard, S.; Inderjeeth, C.; Raymond, W. Higher Charlson comorbidity Index scores do not influence Functional Independence Measure score gains in older rehabilitation patients. Australas. J. Ageing 2016, 35, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Touma, E.; Bisharat, N. Trends in admission serum albumin and mortality in patients with hospital readmission. Int. J. Clin. Pract. 2019, 73, e13314. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.L.; Phillips, C.; Hall, S. Building social capital with interprofessional student teams in rural settings: A service-learning model. Aust. J. Rural Health 2016, 24, 271–277. [Google Scholar] [CrossRef] [Green Version]
- Ohta, R.; Ryu, Y.; Otani, J. Rural physicians’ perceptions about the challenges of participating in interprofessional collaboration: Insights from a focus group study. J. Interprof. Educ. Pract. 2020, 20, 100345. [Google Scholar] [CrossRef]
- Nall, R.W.; Herndon, B.B.; Mramba, L.K.; Vogel-Anderson, K.; Hagen, M.G. An interprofessional primary care-based transition of care clinic to reduce hospital readmission. Am. J. Med. 2020, 133, e260–e268. [Google Scholar] [CrossRef]
- Baldwin, S.M.; Zook, S.; Sanford, J. Implementing posthospital interprofessional care team visits to improve care transitions and decrease hospital readmission rates. Prof. Case Manag. 2018, 23, 264–271. [Google Scholar] [CrossRef]
- Busari, J.O.; Moll, F.M.; Duits, A.J. Understanding the impact of interprofessional collaboration on the quality of care: A case report from a small-scale resource limited health care environment. J. Multidiscip. Healthc. 2017, 10, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Ohta, R.; Ryu, Y.; Sano, C. Older people’s help-seeking behaviors in rural contexts: A systematic review. Int. J. Environ. Res. Public Health 2022, 19, 3233. [Google Scholar] [CrossRef]
- Labra, O.; Wright, R.; Tremblay, G.; Maltais, D.; Bustinza, R.; Gingras-Lacroix, G. Men’s help-seeking attitudes in rural communities affected by a natural disaster. Am. J. Mens. Health 2019, 13, 1557988318821512. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Sano, C. Improvement in quality of life through self-management of mild symptoms during the COVID-19 pandemic: A prospective cohort study. Int. J. Environ. Res. Public Health 2022, 19, 6652. [Google Scholar] [CrossRef] [PubMed]
- Ogino, N.; Aridome, G.; Oshima, J.; Shibata, M.; Watanabe, T.; Kume, K.; Yoshikawa, I.; Harada, M. Serum albumin concentrations predict hypovolaemia caused by polyethylene glycol plus ascorbic acid prior to colonoscopy in elderly patients. Drugs Aging 2016, 33, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Kim, M.; Lee, Y.; Won, C.W. Prevalence of physical frailty and its multidimensional risk factors in Korean community-dwelling older adults: Findings from Korean frailty and aging cohort study. Int. J. Environ. Res. Public Health 2020, 17, 7883. [Google Scholar] [CrossRef]
- Greco, E.A.; Pietschmann, P.; Migliaccio, S. Osteoporosis and sarcopenia increase frailty syndrome in the elderly. Front. Endocrinol. 2019, 10, 255. [Google Scholar] [CrossRef]
- Fujishima, I.; Fujiu-Kurachi, M.; Arai, H.; Hyodo, M.; Kagaya, H.; Maeda, K.; Mori, T.; Nishioka, S.; Oshima, F.; Ogawa, S.; et al. Sarcopenia and dysphagia: Position paper by four professional organizations. Geriatr. Gerontol. Int. 2019, 19, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Ohta, R.; Weiss, E.; Mekky, M.; Sano, C. Relationship between dysphagia and home discharge among older patients receiving hospital rehabilitation in rural Japan: A retrospective cohort study. Int. J. Environ. Res. Public Health 2022, 19, 10125. [Google Scholar] [CrossRef]
- Nguyen, T.; Wong, E.; Ciummo, F. Polypharmacy in older adults: Practical applications alongside a patient case. J. Nurse Pract. 2020, 16, 205–209. [Google Scholar] [CrossRef] [Green Version]
- Pu, D.; Wong, M.C.H.; Yiu, E.M.L.; Chan, K.M.K. Profiles of polypharmacy in older adults and medication associations with signs of aspiration. Expert Rev. Clin. Pharmacol. 2021, 14, 643–649. [Google Scholar] [CrossRef]
- Aoki, T.; Urushibara-Miyachi, Y. A qualitative study of socially isolated patients’ perceptions of primary care. J. Gen. Fam. Med. 2019, 20, 185–189. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Gomi, T.; Katsube, T. Challenges and solutions in the continuity of home care for rural older people: A thematic analysis. Home Health Care Serv. Q. 2020, 39, 126–139. [Google Scholar] [CrossRef]
- Traphagan, J.W. Power, family, and filial responsibility related to elder care in rural Japan. Care Manag. J. 2006, 7, 205–212. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Katsube, T.; Sano, C. Rural homecare nurses’ challenges in providing seamless patient care in rural Japan. Int. J. Environ. Res. Public Health 2020, 17, 9330. [Google Scholar] [CrossRef]
- King, N.; Ross, A. Professional identities and interprofessional relations: Evaluation of collaborative community schemes. Soc. Work Health Care 2003, 38, 51–72. [Google Scholar] [CrossRef]
- Angell, B.; Khan, M.; Islam, R.; Mandeville, K.; Naher, N.; Hutchinson, E.; McKee, M.; Ahmed, S.M.; Balabanova, D. Incentivising doctor attendance in rural Bangladesh: A latent class analysis of a discrete choice experiment. BMJ Glob. Health 2021, 6, e006001. [Google Scholar] [CrossRef] [PubMed]
- Ostini, R.; McGrail, M.R.; Kondalsamy-Chennakesavan, S.; Hill, P.; O’Sullivan, B.; Selvey, L.A.; Eley, D.S.; Adegbija, O.; Boyle, F.M.; Dettrick, Z.; et al. Building a sustainable rural physician workforce. Med. J. Aust. 2021, 215, S5–S33. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.M.; Mizooka, M.; Tazuma, S. General Practice Departments of University Hospitals and Certified Training Programs for General Practitioners in Japan: A Nationwide Questionnaire Survey. J. Gen. Fam. Med. 2017, 18, 244–248. [Google Scholar] [CrossRef] [Green Version]
- Mitsuyama, T.; Son, D.; Eto, M. Competencies Required for General Practitioners/Family Physicians in Urban Areas versus Non-Urban Areas: A Preliminary Study. BMC Fam. Pract. 2018, 19, 186. [Google Scholar] [CrossRef]
- Gibson, C.; Arya, N.; Ponka, D.; Rouleau, K.; Woollard, R. Approaching a Global Definition of Family Medicine: The Besrour Papers: A Series on the State of Family Medicine in the World. Can. Fam. Phys. Med. Fam. Can. 2016, 62, 891–896. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Healthcare Professionals | Purpose | Collaboration |
|---|---|---|
| Dentists | To improve the oral care of older patients | Family medicine physicians assessed the admitted patients and discussed the need for oral care with patients and their families. Family physicians informed the dentist and dental hygienists about the reasons for the admission of patients. Dentists intensively assessed the condition of the teeth, gingiva, and mucosa of the mouth. |
| Physical and occupational therapists | To improve conditions of frailty and adjust effective rehabilitation for each patient | Family physicians and therapists discussed their patients from each other’s perspectives and shared ideas for the care and discharge plan of hospitalized patients once a week. They adjusted the rehabilitation methods and goals. |
| Pharmacists | To reduce the negative effects of polypharmacy | Family physicians and pharmacists discussed medications of admitted patients to identify unnecessary medications for the patients. |
| Nutritionists | To improve nutritional conditions | Nutritionists screened the nutritional condition of admitted patients and discussed with family physicians alterations of patient meals upon observation of patient food intake and changes in the nutritional condition based on laboratory nutritional assessment. |
| Nurses and social workers | To mitigate the difficulty of patients’ lives post-discharge | Weekly discussions were performed regarding patient care and discharge management in each ward among family physicians and chief nurses. The contents of the discussion were shared with social workers. Social workers considered ways to mitigate the difficulty of patient lives post-discharge |
| Factor | Total | Intervention Group | Comparison Group | p-Value |
|---|---|---|---|---|
| N | 1612 | 863 | 749 | |
| Age (years), mean (SD) | 79.86 (15.38) | 79.16 (16.19) | 80.68 (14.34) | 0.047 |
| Male sex (%) | 726 (45.0) | 399 (46.2) | 327 (43.7) | 0.316 |
| Serum albumin (g/dL), mean (SD) | 3.70 (2.35) | 3.76 (2.79) | 3.63 (1.71) | 0.266 |
| Hemoglobin (g/dL), mean (SD) | 12.23 (7.47) | 12.31 (8.33) | 12.15 (6.33) | 0.680 |
| eGFR (mL/min/1.73 m2) | 58.93 (22.47) | 58.83 (22.93) | 59.04 (21.94) | 0.849 |
| BMI (kg/m2), mean (SD) | 21.63 (33.03) | 22.27 (45.01) | 20.90 (4.05) | 0.405 |
| Medicines taken, median, (IQR) | 6.00 (0.00, 19.00) | 6.00 (0.00, 19.00) | 6.00 (0.00, 19.00) | 0.420 |
| Patients with polypharmacy, n (%) | 1035 (64.2) | 557 (64.5) | 478 (63.8) | 0.795 |
| FIM score at admission | ||||
| Motor domain score, median, (IQR) | 63.00 (3.00, 91.00) | 61.00 (13.00, 91.00) | 65.00 (3.00, 91.00) | 0.932 |
| Cognitive domain score, median, (IQR) | 32.00 (0.00, 64.00) | 32.00 (0.00, 64.00) | 31.00(5.00, 43.00) | 0.610 |
| Readmission (%) | 391 (24.3) | 172 (19.9) | 219 (29.2) | <0.001 |
| Care level (%) | ||||
| 0 | 975 (60.5) | 518 (60.0) | 457 (61.1) | |
| 1 | 116 (7.2) | 61 (7.1) | 55 (7.4) | |
| 2 | 151 (9.4) | 79 (9.2) | 72 (9.6) | |
| 3 | 147 (9.1) | 79 (9.2) | 68 (9.1) | |
| 4 | 123 (7.6) | 67 (7.8) | 56 (7.5) | |
| 5 | 99 (6.1) | 59 (6.8) | 40 (5.3) | |
| Dependent condition (%) | 636 (39.5) | 345 (40.0) | 291 (38.9) | 0.683 |
| CCI score (%) | ||||
| 0 | 90 (5.6) | 59 (6.8) | 31 (4.1) | |
| 1 | 42 (2.6) | 20 (2.3) | 22 (2.9) | |
| 2 | 81 (5.0) | 40 (4.6) | 41 (5.5) | |
| 3 | 135 (8.4) | 79 (9.2) | 56 (7.5) | |
| 4 | 325 (20.2) | 157 (18.2) | 168 (22.4) | |
| 5 | 315 (19.5) | 162 (18.8) | 153 (20.4) | |
| 6 | 283 (17.6) | 173 (20.0) | 110 (14.7) | |
| 7 | 181 (11.2) | 83 (9.6) | 98 (13.1) | |
| 8 | 85 (5.3) | 51 (5.9) | 34 (4.5) | |
| 9 | 51 (3.2) | 26 (3.0) | 25 (3.3) | |
| 10 | 16 (1.0) | 11 (1.3) | 5 (0.7) | |
| 11 | 4 (0.2) | 2 (0.2) | 2 (0.3) | |
| 12 | 2 (0.1) | 0 (0.0) | 2 (0.3) | |
| 13 | 1 (0.1) | 0 (0.0) | 1 (0.1) | |
| 15 | 1 (0.1) | 0 (0.0) | 1 (0.1) | |
| CCI score ≥5 (%) | 939 (58.3) | 508 (58.9) | 431 (57.5) | 0.613 |
| Heart failure (%) | 304 (18.9) | 180 (20.9) | 124 (16.6) | |
| Myocardial infarction (%) | 133 (8.3) | 81 (9.4) | 52 (6.9) | |
| Asthma (%) | 74 (4.6) | 37 (4.3) | 37 (4.9) | |
| Kidney diseases (%) | 145 (9.0) | 85 (9.8) | 60 (8.0) | |
| Peptic ulcer (%) | 107 (6.6) | 40 (4.6) | 67 (9.0) | |
| Liver diseases (%) | 70 (4.3) | 41 (4.8) | 29 (3.9) | |
| COPD (%) | 89 (5.5) | 51 (5.9) | 38 (5.1) | |
| DM (%) | 254 (15.8) | 144 (16.7) | 110 (14.7) | |
| Brain hemorrhage (%) | 125 (7.8) | 75 (8.7) | 50 (6.7) | |
| Brain infarction (%) | 284 (17.6) | 150 (17.4) | 134 (17.9) | |
| Hemiplegia (%) | 25 (1.6) | 6 (0.7) | 19 (2.5) | |
| Dementia (%) | 263 (16.3) | 137 (15.9) | 126 (16.8) | |
| Connective tissue diseases (%) | 74 (4.6) | 45 (5.2) | 29 (3.9) | |
| Cancer (%) | 293 (18.2) | 148 (17.2) | 145 (19.4) |
| Factor | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Presence of intervention | 0.66 | 0.54–0.81 | <0.001 |
| Age | 1 | 0.99–1.01 | 0.74 |
| Male sex | 1.28 | 1.04–1.58 | 0.019 |
| Serum albumin | 1.15 | 1.01–1.31 | 0.031 |
| BMI | 0.94 | 0.92–0.97 | <0.001 |
| Hemoglobin | 0.96 | 0.92–1.00 | 0.056 |
| Polypharmacy | 1.56 | 1.22–2.00 | <0.001 |
| FIM score at admission | |||
| Motor domain score | 1 | 1.00–1.01 | 0.24 |
| Cognitive domain score | 1.01 | 0.99–1.02 | 0.21 |
| Dependent condition | 1.34 | 1.03–1.76 | 0.031 |
| CCI score ≥5 (%) | 1.97 | 1.50–2.59 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohta, R.; Sano, C. The Effectiveness of Family Medicine-Driven Interprofessional Collaboration on the Readmission Rate of Older Patients. Healthcare 2023, 11, 269. https://doi.org/10.3390/healthcare11020269
Ohta R, Sano C. The Effectiveness of Family Medicine-Driven Interprofessional Collaboration on the Readmission Rate of Older Patients. Healthcare. 2023; 11(2):269. https://doi.org/10.3390/healthcare11020269
Chicago/Turabian StyleOhta, Ryuichi, and Chiaki Sano. 2023. "The Effectiveness of Family Medicine-Driven Interprofessional Collaboration on the Readmission Rate of Older Patients" Healthcare 11, no. 2: 269. https://doi.org/10.3390/healthcare11020269