
Acquisition Status of Basic Clinical Skills in Japanese Novice Rehabilitation Therapists: A Preliminary Single-Center Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Analysis
3. Results
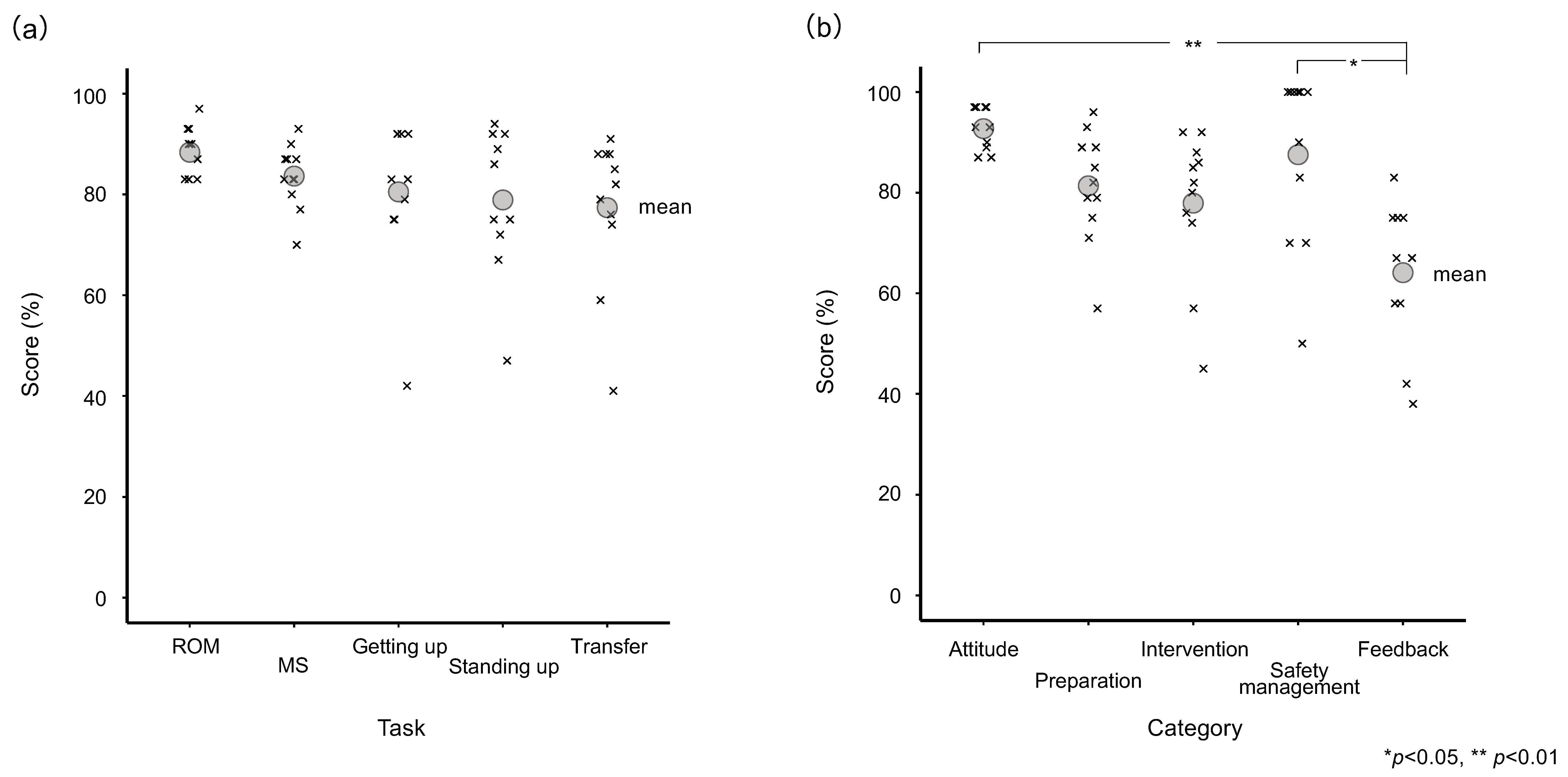
3.1. Comparison of the Total Scores for Each Task
3.2. Comparison of the Total Scores for Each Category
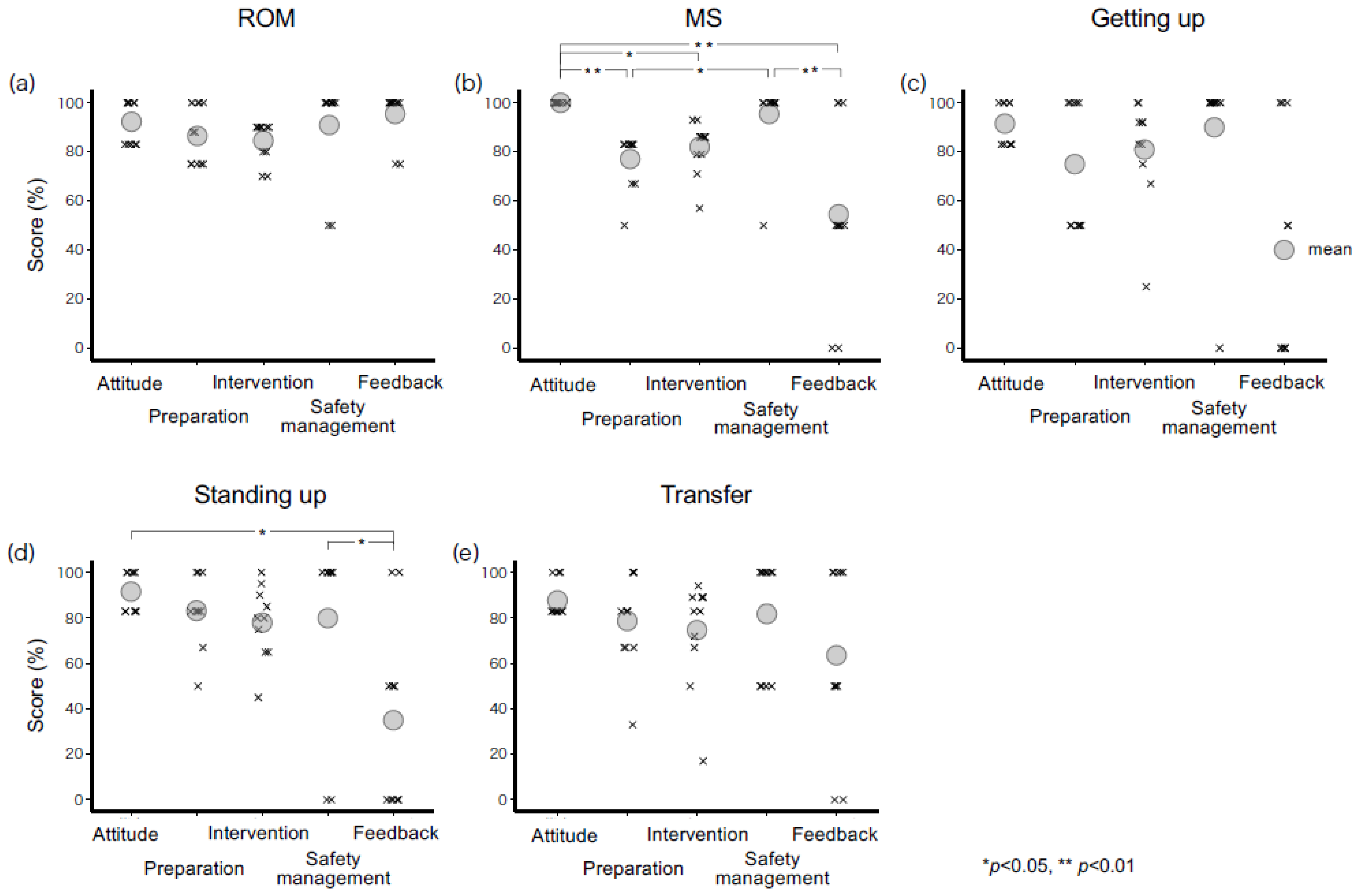
3.3. Comparison of the Total Score Percentage for Each Category of Each Task
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs. Population Dynamics. World Population Prospects. 2019. Available online: https://population.un.org/wpp/ (accessed on 4 January 2022).
- Ministry of Finance Japan. Social Security Expenses, etc. Available online: https://www.mof.go.jp/about_mof/councils/fiscal_system_council/sub-of_fiscal_system/proceedings/material/zaiseia20210415/02.pdf (accessed on 4 January 2022). (In Japanese)
- Yoshino, J. Study of the Levels and Secular Changes of Clinical Competencies of Physical Therapists. Rigakuryoho Kagaku 2021, 36, 699–704. (In Japanese) [Google Scholar] [CrossRef]
- Japanese Association of Occupational Therapists. Member Statistics. J. Jpn. Assoc. Occupat. Ther. 2020, 102, 5–18. Available online: https://www.jaot.or.jp/files/page/jimukyoku/kaiintoukei2019.pdf. (accessed on 4 January 2022). (In Japanese).
- Japanese Physical Therapy Association. Statistics. Site for Citizens. Available online: https://www.japanpt.or.jp/activity/data/ (accessed on 4 January 2022). (In Japanese).
- Ministry of Health, Labour, and Welfare of Japan. Announcement of Passing the 56th National Examination for Physical Therapists and the 56th National Examination for Occupational Therapists. Available online: https://www.mhlw.go.jp/general/sikaku/successlist/2021/siken08_09/about.html (accessed on 4 January 2022). (In Japanese)
- Ministry of Health, Labour, and Welfare of Japan. Announcement of Passing of the 54th National Examination for Physical Therapists and the 54th National Examination for Occupational Therapists. Available online: https://www.mhlw.go.jp/general/sikaku/successlist/2019/siken08_09/about.html (accessed on 4 January 2022). (In Japanese)
- Yoshino, J. New hire education goals. Jpn. J. Physic. Ther. 2010, 44, 357–363. (In Japanese) [Google Scholar]
- Ministry of Education, Culture, Sports, Science, and Technology Japan. Regulations for Designation of Establishing Training Schools for Physical and Occupational Therapists. Available online: https://elaws.e-gov.go.jp/document?lawid=341M50000180003 (accessed on 23 July 2022). (In Japanese)
- Japanese Association of Occupational Therapists. Occupational Therapy Clinical Practice Guidelines. Available online: https://www.jaot.or.jp/files/page/wp-content/uploads/2013/12/shishin-tebiki2018-2.pdf (accessed on 6 January 2022). (In Japanese).
- Suzuki, Y.; Nagai, S. The actual situation of clinical training in physical therapy education: Suggestive of actual status of student learning by questionnaire survey. Med. Health Sci. Res. 2012, 3, 103–114. (In Japanese) [Google Scholar]
- Yoshino, J.; Usuda, S. Current state of physical therapist continuing education in medical facilities. J. Phys. Ther. Sci. 2010, 25, 55–60. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Motoya, I.; Takeda, K.; Koyama, S.; Kojima, R.; Hirakawa, Y.; Sakurai, H.; Kanada, Y.; Kawamura, N.; Tanabe, S. The characteristics of the clinical competence of novice physical therapists and occupational therapists at the time of hiring in a single institution in Japan. Health Prof. Educ. 2020, 6, 538–551. [Google Scholar] [CrossRef]
- Saitoh, H.; Koseki, M. Recent clinical education techniques and clinical skills assessment—Application and practical report of OSCE in post-graduate education. Physic. Ther. Jpn. 2008, 35, 455–456. (In Japanese) [Google Scholar]
- Harden, R.M.; Stevenson, M.; Downie, W.W.; Wilson, G.M. Assessment of clinical competence using objective structured examination. Br. Med. J. 1975, 1, 447–451. [Google Scholar] [CrossRef] [Green Version]
- Ito, F.; Suzuki, K.; Muraki, T.; Saito, S.; Tsuchisawa, K. A trial of objective structured clinical examination (OSCE) before clinical practice in our occupational therapy education. Jpn. J. Res. Occup. Ther. Educ. 2006, 6, 18–26. (In Japanese) [Google Scholar]
- Kohno, M.; Watanabe, A.; Sakurai, H. Practice of OSCE in therapist education. Jpn. J. Res. Occupat. Ther. Educ. 2004, 4, 38–41. (In Japanese) [Google Scholar]
- Yamaji, T.; Watanabe, J.; Asakawa, Y.; Matsuda, Y.; Usuda, S.; Endo, F.; Uchiyama, Y.; Sakamoto, M.; Yamaguchi, H.; Nakazawa, T.; et al. Development and trial of objective structured clinical examination in physical therapy education. J. Jpn. Physic. Ther. Assoc. 2004, 31, 348–358. (In Japanese) [Google Scholar]
- SSimon, S.R.; Bui, A.; Day, S.; Berti, D.; Volkan, K. The relationship between second-year medical students’ OSCE scores and USMLE Step 2 scores. J. Eval. Clin. Pract. 2007, 13, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, E. Clinical Skills for PT/OT and OSCE—Intervention for Functional Disorders and Reduced Capabilities Edition; KANEHARA & CO., LTD.: Tokyo, Japan, 2017. (In Japanese) [Google Scholar]
- Bewick, V.; Cheek, L.; Ball, J. Statistics review 9: One-way analysis of variance. Crit. Care 2004, 8, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Sheldon, M.R.; Fillyaw, M.J.; Thompson, W.D. The use and interpretation of the Friedman test in the analysis of ordinal-scale data in repeated measures designs. Physiother. Res. Int. 1996, 1, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Koshino, H. Neural basis of dual-tasking. Jpn. J. Psychonomic. Sci. 2009, 28, 59–71. (In Japanese) [Google Scholar]
- Watanabe, K.; Funahashi, S. Neural mechanisms of dual-task interference and cognitive capacity limitation in the prefrontal cortex. Nat. Neurosci. 2014, 17, 601–611. [Google Scholar] [CrossRef] [Green Version]
- Japanese Physical Therapy Association. Clinical Training Educational Guide, 6th ed.; JPTA: Tokyo, Japan, 2020; Available online: https://www.japanpt.or.jp/assets/pdf/activity/books/education_01/tebiki6_201225.pdf (accessed on 6 January 2022). (In Japanese)
- Shinohara, T.; Gokan, H.; Hiraishi, T.; Yagi, I.; Tani, T. Internal consistency and factor structure of the therapist achievement evaluation scale developed as an education tool for on-the-job training: Consideration of attainment of target of providing physical therapy based on the advice of a tutor. J. Jpn. Physic. Ther. Assoc. 2018, 33, 331–336. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Tani, H. Are instructions and feedback by a therapist effective in the motor learning? Physic. Ther. Jpn. 2006, 21, 69–73. (In Japanese) [Google Scholar] [CrossRef]
- Yoshino, J.; Futawatari, T.; Otani, K. Qualitative study of the primary goals of continuing education in physical therapy. J. Jpn. Physic. Ther. Assoc. 2010, 37, 410–416. (In Japanese) [Google Scholar]
- Black, L.L.; Jensen, G.M.; Mostrom, E.; Perkins, J.; Ritzline, P.D.; Hayward, L.; Blackmer, B. The first year of practice: An investigation of the professional learning and development of promising novice physical therapists. Physic. Ther. 2010, 90, 1758–1773. [Google Scholar] [CrossRef]
- Hayward, L.M.; Black, L.L.; Mostrom, E.; Jensen, G.M.; Ritzline, P.D.; Perkins, J. The first two years of practice: A longitudinal perspective on the learning and professional development of promising novice physical therapists. Physic. Therap 2013, 93, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, J.; Usuda, S. Development and reliability of a clinical competence evaluation scale in physical therapy. J. Jpn. Physic. Ther. Assoc. 2012, 27, 651–655. (In Japanese) [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Category/Task | ROM 1 | MS 2 | Getting Up 3 | Standing Up 4 | Transfer 5 | Total |
|---|---|---|---|---|---|---|
| Attitude | 3 | 3 | 3 | 3 | 3 | 15 |
| Preparation | 4 | 3 | 1 | 3 | 3 | 14 |
| Intervention | 5 | 7 | 6 | 10 | 9 | 37 |
| Safety management | 1 | 1 | 1 | 1 | 1 | 5 |
| Feedback | 2 | 1 | 1 | 1 | 1 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujimura, K.; Sakurai, H.; Koyama, S.; Takeda, K.; Ii, T.; Suzumura, S.; Tanabe, S.; Kanada, Y. Acquisition Status of Basic Clinical Skills in Japanese Novice Rehabilitation Therapists: A Preliminary Single-Center Study. Healthcare 2023, 11, 254. https://doi.org/10.3390/healthcare11020254
Fujimura K, Sakurai H, Koyama S, Takeda K, Ii T, Suzumura S, Tanabe S, Kanada Y. Acquisition Status of Basic Clinical Skills in Japanese Novice Rehabilitation Therapists: A Preliminary Single-Center Study. Healthcare. 2023; 11(2):254. https://doi.org/10.3390/healthcare11020254
Chicago/Turabian StyleFujimura, Kenta, Hiroaki Sakurai, Soichiro Koyama, Kazuya Takeda, Takuma Ii, Shota Suzumura, Shigeo Tanabe, and Yoshikiyo Kanada. 2023. "Acquisition Status of Basic Clinical Skills in Japanese Novice Rehabilitation Therapists: A Preliminary Single-Center Study" Healthcare 11, no. 2: 254. https://doi.org/10.3390/healthcare11020254