
Patient Unpunctuality’s Effect on Appointment Scheduling: A Scenario-Based Analysis
 ,
,
Abstract
:1. Introduction
2. Literature Review
3. Methodology
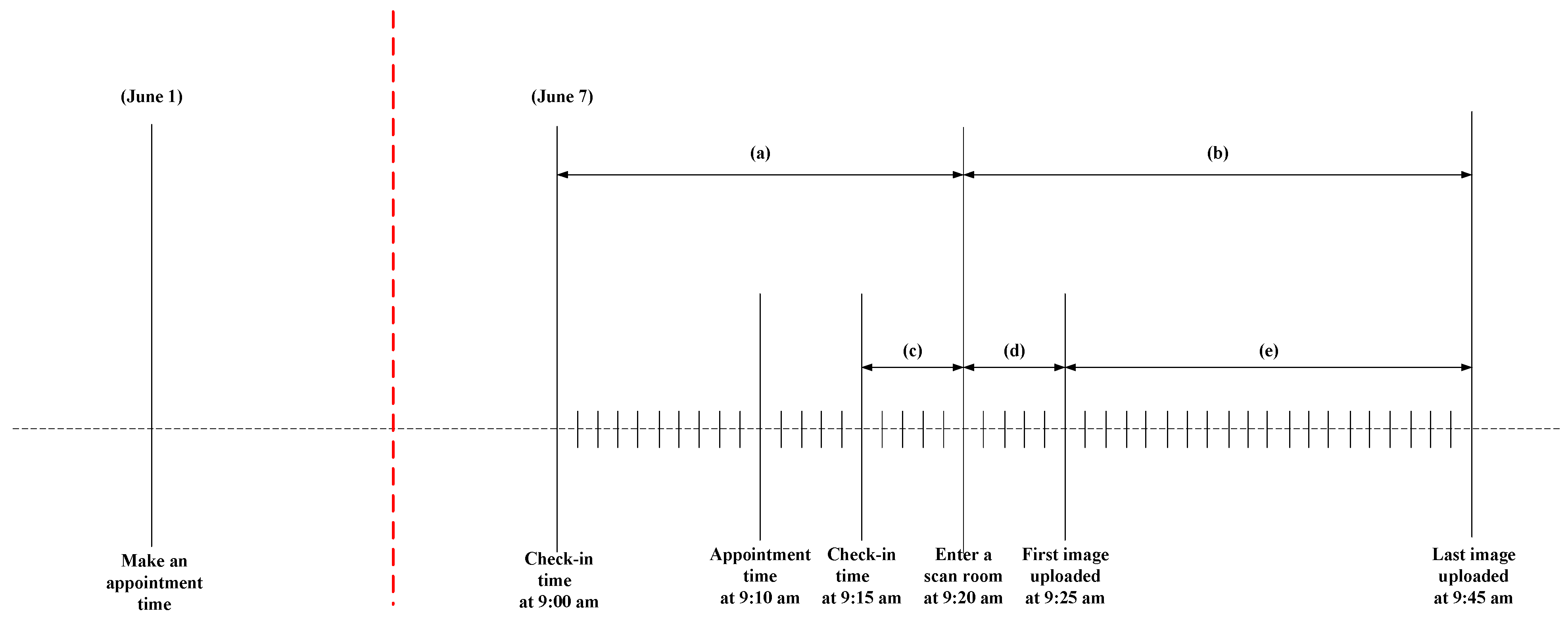
3.1. Problem Statement
3.2. Data Collection
3.3. Data Fitting
+ [0.0537 × (−45.5 + 8 × BETA (1.440, 1.030))]
+ [0.0440 × (−37.5 + 4 × BETA (1.050, 0.903))]
+ [ 0.0438 × (−33.5 + 4 × BETA (1.540, 1.430))]
+ [0.2007 × (−29.5 + 10 × BETA (1.130, 0.822))]
+ [0.6400 × (−19.5 + 19 × BETA (0.981, 0.922))]
3.4. Simulation Model Assumptions
- This study considered patients with a scheduled appointment at the case hospital. Only outpatients and inpatients were included. Emergent patients were excluded since they are considered walk-in patients.
- Patients may arrive unpunctually. Patients who arrived exactly at their appointment time were considered on-time patients. When a radiological technician is ready to serve the next ultrasound scan, the radiological technician will call the patient’s name (or patient’s appointment number). If the patient does not show up within 1 min, the radiological technician will call the next patient’s name. Therefore, patients who arrived 1 min earlier or 1 min later were considered unpunctual in this study.
- The case hospital’s scanning rooms for inpatients and outpatients operate Monday to Friday, from 9:00 am to 3:00 pm, with a 1-h break from 12:00 pm to 1:00 pm. Therefore, the scanning rooms operate 5 h per day for inpatients and outpatients.
- The case hospital has six rooms (rooms 5, 6, 7, 8, 9, and 10) that can provide any type of service to the patients. Six radiological technicians provide services. One radiological technician is assigned to each room. Eight types of services are provided to outpatients: Shoulder, scrotum, neck, prostate, thyroid, urotract, EXT DVT, and abdomen. Six types of services are provided to inpatients: EXT DVT, liver, prostate, urotract, thyroid, and abdomen.
- Patients’ walking times were not considered due to the adjacent locations between the check-in counter and scanning rooms. The probability distribution of the service time is given per body part based on the results of the data-fitting procedures.
- Patients were assumed to undergo the proper procedure when receiving the service.
- A constant arrival policy of 20 min was applied as the appointment scheduling policy used in the simulation system.
3.5. Verification and Validation of the Simulation Model
3.6. What-If Scenarios
- The hospital opens at 9:00 am, at which point patients can wait inside for their appointment time.
- The example hospital only has two rooms, which means that two patients are booked for each appointment slot.
- The arrival time of each patient is independent.
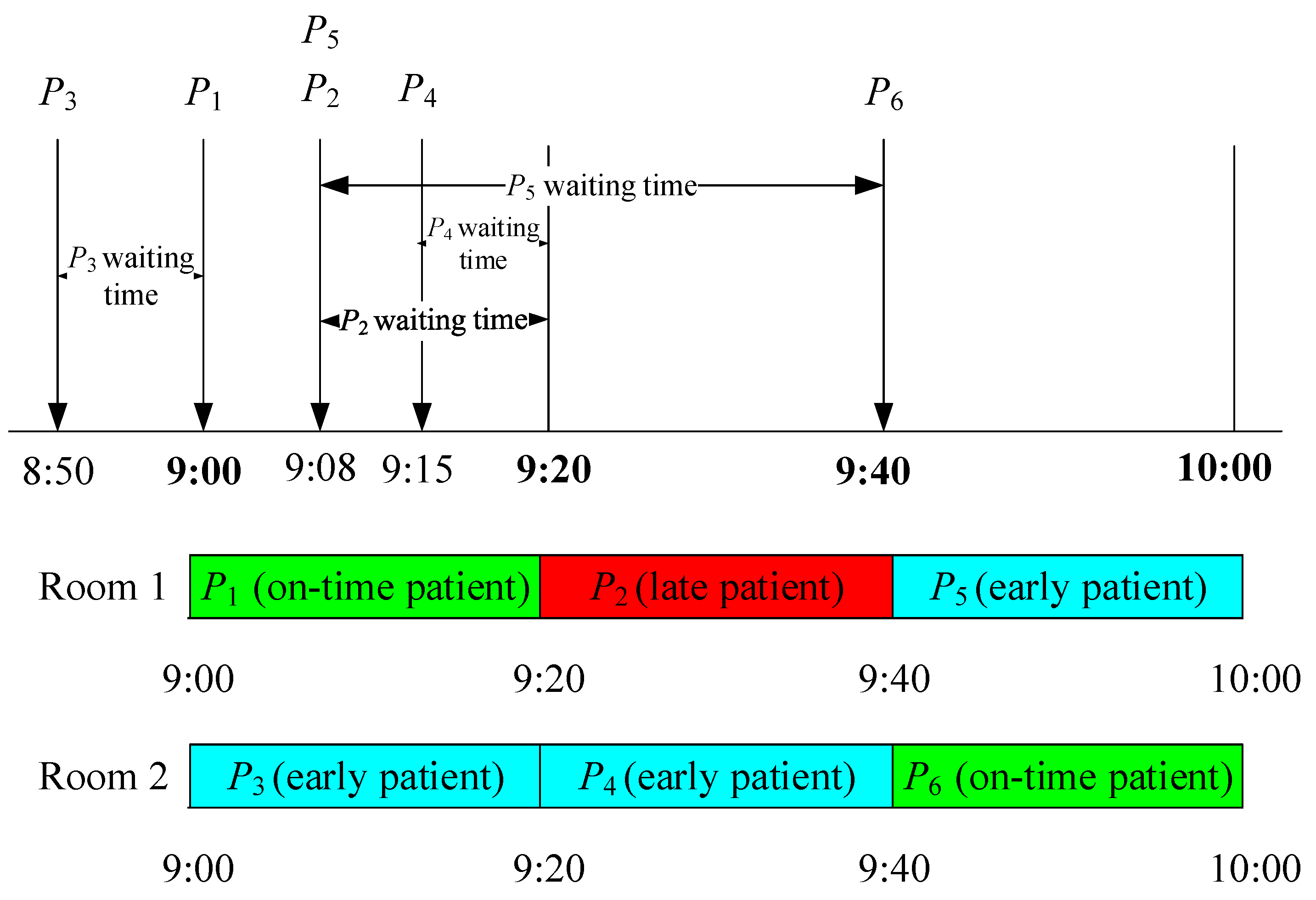
3.6.1. Preempt Policy
3.6.2. Examples of the Preempt Policy with Constant Service Time
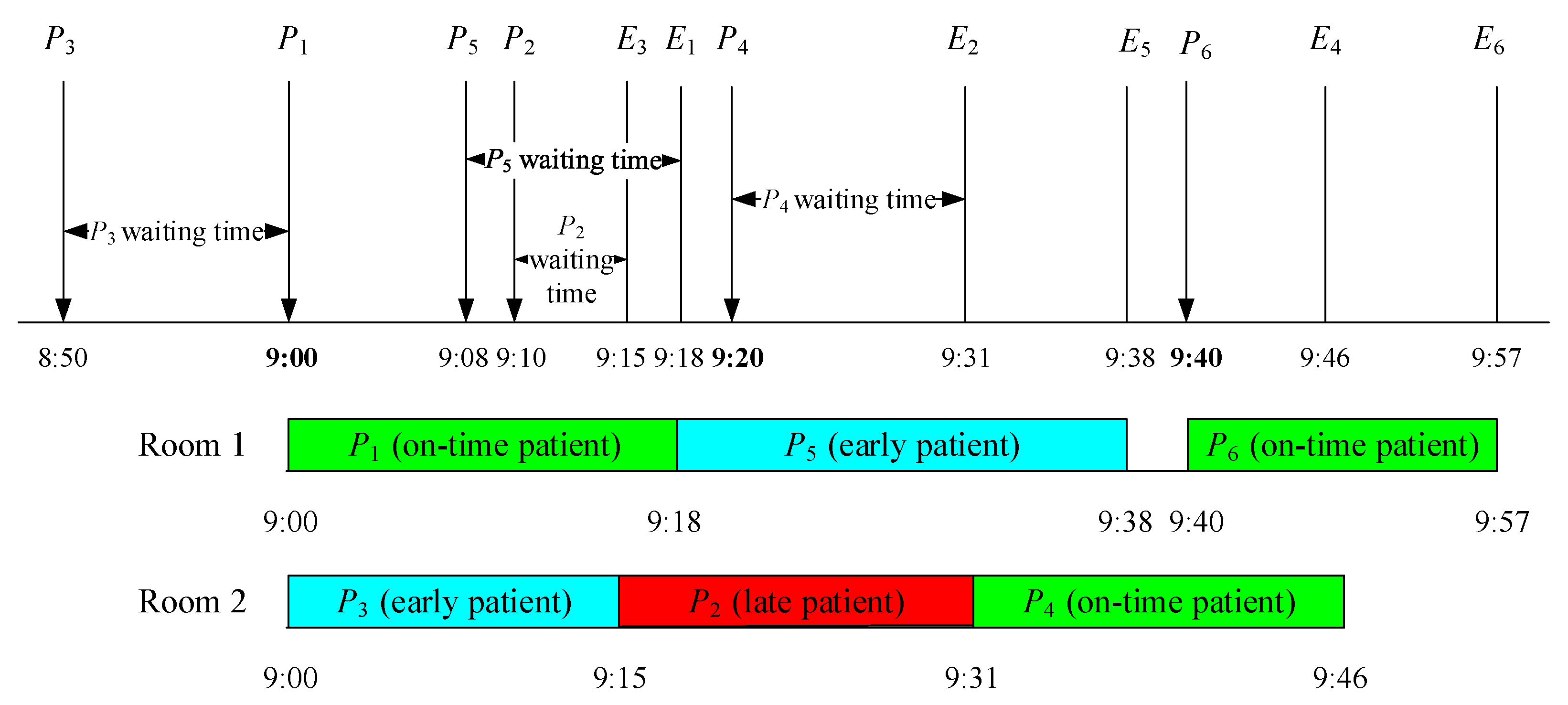
3.6.3. Examples of the Preempt Policy with Variable Service Time
3.6.4. Wait Policy
4. Results
4.1. Preempt and Wait Policies
4.2. Sensitivity Analyses
4.2.1. Base-Parameter Model Analysis
4.2.2. Sensitivity Analysis 1
4.2.3. Sensitivity Analysis 2
4.2.4. Sensitivity Analysis 3
4.2.5. Sensitivity Analysis 4
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rastegar, D.A. Health care becomes an industry. Ann. Fam. Med. 2004, 2, 79–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.Y.; Morrice, D.J.; Muthuraman, K.; Bard, J.F.; Leykum, L.K.; Noorily, S.H. Coordinated scheduling for a multi-server network in outpatient pre-operative care. Prod. Oper. Manag. 2018, 27, 458–479. [Google Scholar] [CrossRef]
- Wang, D.Y.; Muthuraman, K.; Morrice, D. Coordinated patient appointment scheduling for a multistation healthcare network. Oper. Res. 2019, 67, 599–618. [Google Scholar] [CrossRef]
- Huang, Y.-L. Appointment standardization evaluation in a primary care facility. Int. J. Health Care Qual. Assur. 2016, 29, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.S.; Robielos, R.A.C.; Palana, P.K.V.C.; Valencia, P.L.L.; Chen, G.Y.H. Scheduling patients’ appointments: Allocation of healthcare service using simulation optimization. J. Healthc. Eng. 2015, 6, 259–280. [Google Scholar] [CrossRef] [Green Version]
- Abdoli, M.; Bahadori, M.; Ravangard, R.; Babaei, M.; Aminjarahi, M. Comparing 2 appointment scheduling policies using discrete-event simulation. Qual. Manag. Health Care 2021, 30, 112–120. [Google Scholar] [CrossRef]
- Cayirli, T.; Yang, K.K.; Quek, S.A. A universal appointment rule in the presence of no-shows and walk-ins. Prod. Oper. Manag. 2012, 21, 682–697. [Google Scholar] [CrossRef]
- Diamant, A.; Milner, J.; Quereshy, F. Dynamic patient scheduling for multi-appointment health care programs. Prod. Oper. Manag. 2018, 27, 58–79. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Ziya, S.; Kulkarni, V.G. Dynamic scheduling of outpatient appointments under patient no-shows and cancellations. Manuf. Serv. Oper. Manag. 2010, 12, 347–364. [Google Scholar] [CrossRef] [Green Version]
- Lowery, J.C.; Martin, J.B. Evaluation of an advance surgical scheduling system. J. Med. Syst. 1989, 13, 11–23. [Google Scholar] [CrossRef]
- Li, Y.T.; Tang, S.Y.; Johnson, J.; Lubarsky, D.A. Individualized no-show predictions: Effect on clinic overbooking and appointment reminders. Prod. Oper. Manag. 2019, 28, 2068–2086. [Google Scholar] [CrossRef]
- Srinivas, S.; Salah, H. Consultation length and no-show prediction for improving appointment scheduling efficiency at a cardiology clinic: A data analytics approach. Int. J. Med. Inform. 2021, 145, 104290. [Google Scholar] [CrossRef] [PubMed]
- Klassen, K.J.; Yoogalingam, R. Strategies for appointment policy design with patient unpunctuality. Decis. Sci. 2014, 45, 881–911. [Google Scholar] [CrossRef]
- White, M.J.B.; Pike, M.C. Appointment systems in out-patients’ clinics and the effect of patients’ unpunctuality. Medical. Care 1964, 2, 133–141+144–145. [Google Scholar] [CrossRef]
- Samorani, M.; Ganguly, S. Optimal sequencing of unpunctual patients in high-service-level clinics. Prod. Oper. Manag. 2016, 25, 330–346. [Google Scholar] [CrossRef]
- Cayirli, T.; Veral, E.; Rosen, H. Designing appointment scheduling systems for ambulatory care services. Health Care Manag. Sci. 2006, 9, 47–58. [Google Scholar] [CrossRef]
- Deceuninck, M.; Fiems, D.; De Vuyst, S. Outpatient scheduling with unpunctual patients and no-shows. Eur. J. Oper. Res. 2018, 265, 195–207. [Google Scholar] [CrossRef]
- Bailey, N.T.J. A study of queues and appointment systems in hospital outpatient departments with special reference to waiting times. J. R. Stat. Soc. Ser. B (Methodol.) 1952, 14, 185–199. [Google Scholar]
- Ahmadi-Javid, A.; Jalali, Z.; Klassen, K.J. Outpatient appointment systems in healthcare: A review of optimization studies. Eur. J. Oper. Res. 2017, 258, 3–34. [Google Scholar] [CrossRef]
- Klassen, K.J.; Yoogalingam, R. Improving performance in outpatient appointment services with a simulation optimization approach. Prod. Oper. Manag. 2009, 18, 447–458. [Google Scholar] [CrossRef]
- Zhu, H.; Chen, Y.H.; Leung, E.; Liu, X. Outpatient appointment scheduling with unpunctual patients. Int. J. Prod. Res. 2018, 56, 1982–2002. [Google Scholar] [CrossRef]
- Deceuninck, M.; De Vuyst, S.; Fiems, D. An efficient control variate method for appointment scheduling with patient unpunctuality. Simul. Model. Pract. Theory 2019, 90, 116–129. [Google Scholar] [CrossRef]
- Jiang, B.W.; Tang, J.F.; Yan, C.J. A stochastic programming model for outpatient appointment scheduling considering unpunctuality. Omega 2019, 82, 70–82. [Google Scholar] [CrossRef]
- Pan, X.; Geng, N.; Xie, X. A benders decomposition approach for appointment scheduling of unpunctual patients in a multi-server setting. In Proceedings of the IEEE International Conference on Industrial Engineering and Engineering Management, Macau, China, 15–18 December 2019; pp. 64–68. [Google Scholar]
- Pan, X.W.; Geng, N.; Xie, X.L. Appointment scheduling and real-time sequencing strategies for patient unpunctuality. Eur. J. Oper. Res. 2021, 295, 246–260. [Google Scholar] [CrossRef]
- Pan, X.W.; Geng, N.; Xie, X.L. A stochastic approximation approach for managing appointments in the presence of unpunctual patients, multiple servers and no-shows. Int. J. Prod. Res. 2021, 59, 2996–3016. [Google Scholar] [CrossRef]
- Sanoubar, S.; He, K.; Maillart, L.M.; Prokopyev, O.A. Optimal age-replacement in anticipation of time-dependent, unpunctual policy implementation. IEEE 2021, 70, 1177–1192. [Google Scholar] [CrossRef]
- Fetter, R.B.; Thompson, J.D. Patients’ waiting time and doctor’s idle time in the outpatient setting. Health Serv. Res. 1966, 1, 66–90. [Google Scholar]
- Harper, P.R.; Gamlin, H.M. Reduced outpatient waiting times with improved appointment scheduling: A simulation modelling approach. Or Spectr. 2003, 25, 207–222. [Google Scholar] [CrossRef]
- Alexopoulos, C.; Goldsman, D.; Fontanesi, J.; Kopald, D.; Wilson, J.R. Modeling patient arrivals in community clinics. Omega 2008, 36, 33–43. [Google Scholar] [CrossRef]
- Tai, G.F.; Williams, P. Optimization of scheduling patient appointments in clinics using a novel modelling technique of patient arrival. Comput. Meth. Prog. Biol. 2012, 108, 467–476. [Google Scholar] [CrossRef]
- Luo, L.; Zhou, Y.; Han, B.T.; Li, J.L. An optimization model to determine appointment scheduling window for an outpatient clinic with patient no-shows. Health Care Manag. Sci. 2019, 22, 68–84. [Google Scholar] [CrossRef]
- Shnits, B.; Bendavid, I.; Marmor, Y.N. An appointment scheduling policy for healthcare systems with parallel servers and pre-determined quality of service. Omega 2020, 97, 102095. [Google Scholar] [CrossRef]
- Srinivas, S.; Ravindran, A.R. Designing schedule configuration of a hybrid appointment system for a two-stage outpatient clinic with multiple servers. Health Care Manag. Sci. 2020, 23, 360–386. [Google Scholar] [CrossRef]
- Fan, X.Z.; Tang, J.F.; Yan, C.J.; Guo, H.N.; Cao, Z.F. Outpatient appointment scheduling problem considering patient selection behavior: Data modeling and simulation optimization. J. Comb. Optim. 2021, 42, 677–699. [Google Scholar] [CrossRef]
- Lin, C.K.Y.; Ling, T.W.C.; Yeung, W.K. Resource allocation and outpatient appointment scheduling using simulation optimization. J. Healthc. Eng. 2017, 2017, 9034737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentayeb, D.; Lahrichi, N.; Rousseau, L.M. On integrating patient appointment grids and technologist schedules in a radiology center. Health Care Manag. Sci. 2022, 84, 1–17. [Google Scholar] [CrossRef]
- Shehadeh, K.S.; Cohn, A.E.M.; Jiang, R.W. Using stochastic programming to solve an outpatient appointment scheduling problem with random service and arrival times. Nav. Res. Log. 2021, 68, 89–111. [Google Scholar] [CrossRef]
- Heshmat, M.; Eltawil, A. Solving operational problems in outpatient chemotherapy clinics using mathematical programming and simulation. Ann. Oper. Res. 2021, 298, 289–306. [Google Scholar] [CrossRef]
- Chen, P.S.; Chen, G.Y.H.; Liu, L.W.; Zheng, C.P.; Huang, W.T. Using simulation optimization to solve patient appointment scheduling and examination room assignment problems for patients undergoing ultrasound examination. Healthcare 2022, 10, 164. [Google Scholar] [CrossRef]
- Ala, A.L.; Simic, V.; Pamucar, D.; Tirkolaee, E.B. Appointment scheduling problem under fairness policy in healthcare services: Fuzzy ant lion optimizer. Expert Syst. Appl. 2022, 207, 117949. [Google Scholar] [CrossRef]
- Issabakhsh, M.; Lee, S.; Kang, H.J. Scheduling patient appointment in an infusion center: A mixed integer robust optimization approach. Health Care Manag. Sci. 2021, 24, 117–139. [Google Scholar] [CrossRef]
- Guido, R.; Ielpa, G.; Conforti, D. Scheduling outpatient day service operations for rheumatology diseases. Flex Serv. Manuf. J. 2020, 32, 102–128. [Google Scholar] [CrossRef]
- Chen, P.-S.; Juan, K.-L. Applying simulation optimization for solving a collaborative patient-referring mechanism problem. J. Ind. Prod. Eng. 2013, 30, 405–413. [Google Scholar] [CrossRef]
- Chen, P.S.; Lin, M.H. Development of simulation optimization methods for solving patient referral problems in the hospital-collaboration environment. J. Biomed. Inform. 2017, 73, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Lyu, J.; Chen, P.S.; Huang, W.T. Combining an automatic material handling system with lean production to improve outgoing quality assurance in a semiconductor foundry. Prod. Plan Control 2021, 32, 829–844. [Google Scholar] [CrossRef]
- Kelton, D.W.; Sadowski, R.P.; Zupick, N.B. Simulation with Arena; McGraw-Hill Education: New York, NY, USA, 2015. [Google Scholar]
- Peres, I.T.; Hamacher, S.; Oliveira, F.L.C.; Barbosa, S.D.J.; Viegas, F. Simulation of appointment scheduling policies: A study in a Bariatric clinic. Obes. Surg. 2019, 29, 2824–2830. [Google Scholar] [CrossRef]
- Moradi, S.; Najafi, M.; Mesgari, S.; Zolfagharinia, H. The utilization of patients’ information to improve the performance of radiotherapy centers: A data-driven approach. Comput. Ind. Eng. 2022, 172, 108547. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Range of Patient Waiting Time (Minutes) | Percentage (%) | Cumulative Percentage (%) | Probability Distribution | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| −50 | −46 | 1.78 | 1.78 | −50.5 + 8 × BETA (1.120, 0.918) |
| −45 | −36 | 5.37 | 7.15 | −45.5 + 8 × BETA (1.440, 1.030) |
| −37 | −34 | 4.40 | 11.55 | −37.5 + 4 × BETA (1.050, 0.903) |
| −33 | −30 | 4.38 | 15.93 | −33.5 + 4 × BETA (1.540, 1.430) |
| −29 | −20 | 20.07 | 36.00 | −29.5 + 10 × BETA (1.130, 0.822) |
| −19 | −1 | 64.00 | 100.00 | −19.5 + 19 × BETA (0.981, 0.922) |
| Range of Patient Waiting Time (Minutes) | Percentage (%) | Cumulative Percentage (%) | Probability Distribution | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| 1 | 12 | 83.27 | 83.27 | 0.5 + 12 × BETA (0.699, 1.390) |
| 13 | 20 | 16.73 | 100.00 | 12.5 + 8 × BETA (0.754, 1.060) |
| Range of Patient Waiting Time (Minutes) | Percentage (%) | Cumulative Percentage (%) | Probability Distribution | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| −15 | −9 | 27.70 | 27.70 | −15.5 + 7 × BETA (1.560, 0.776) |
| −8 | −1 | 72.30 | 100.00 | −8.5 + 8 × BETA (1.020, 1.130) |
| Range of Patient Waiting Time (Minutes) | Percentage (%) | Cumulative Percentage (%) | Probability Distribution | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| 1 | 10 | 100.00 | 100.00 | 0.5 + 10 × BETA (0.747, 1.530) |
| Patient Type | Half-Width at 95% Confidence Interval (h) | in % | |
|---|---|---|---|
| Outpatients | 262.63 | 0.46 | 0.18 |
| Inpatients | 50.07 | 0.28 | 0.56 |
| Patient Type | Actual Average Number of Patients | Simulated Average Number of Patients | Range at 95% Confidence Interval of Simulated Model | |
|---|---|---|---|---|
| Minimum | Maximum | |||
| Early Outpatients | 224.65 * | 219.07 | 216.52 | 221.62 |
| On-time Outpatients | 8.22 | 8.23 | 7.05 | 9.41 |
| Late Outpatients | 41.01 | 38.70 | 36.28 | 41.12 |
| Patient Type | Actual Average Number of Patients | Simulated Average Number of Patients | Range at 95% Confidence Interval of Simulated Model | |
|---|---|---|---|---|
| Minimum | Minimum | |||
| Early Inpatients | 38.33 | 39.37 | 38.09 | 40.65 |
| On-time Inpatients | 2.33 | 2.53 | 1.92 | 3.14 |
| Late Inpatients | 9.30 | 9.10 | 7.90 | 10.30 |
| Patient Type | Actual Average Number of Patients | Simulated Average Number of Patients | Range at 95% Confidence Interval | |
|---|---|---|---|---|
| Minimum | Minimum | |||
| Early Outpatients | 17.02 | 17.06 | 16.89 | 17.23 |
| Late Outpatients | 6.50 | 6.60 | 6.33 | 6.87 |
| Patient Type | Actual Average Number of Patients | Simulated Average Number of Patients | Range at 95% Confidence Interval | |
|---|---|---|---|---|
| Minimum | Minimum | |||
| Early Inpatients | 6.43 * | 6.25 | 6.10 | 6.40 |
| Late Inpatients | 3.79 | 3.66 | 2.87 | 4.45 |
| Patient | Appointment Time | Arrival Time | Early, Late, or On-Time | Start of Service Time | End of Service Time | Waiting Time (Minutes) | Room No. |
|---|---|---|---|---|---|---|---|
| P1 | 9:00 | 9:00 | On-time | 9:00 | 9:20 | 0 | 1 |
| P3 | 9:20 | 8:50 | Early | 9:00 | 9:20 | 10 | 2 |
| P2 | 9:00 | 9:08 | Late | 9:20 | 9:40 | 12 | 1 |
| P4 | 9:20 | 9:15 | Early | 9:20 | 9:40 | 5 | 2 |
| P5 | 9:40 | 9:08 | Early | 9:40 | 10:00 | 32 | 1 |
| P6 | 9:40 | 9:40 | On-time | 9:40 | 10:00 | 0 | 2 |
| Patient | Appointment Time | Arrival Time | Early, Late, or On-Time | Start of Service Time | End of Service Time | Waiting Time (Minutes) | Room No. |
|---|---|---|---|---|---|---|---|
| P1 | 9:00 | 9:00 | On-time | 9:00 | 9:18 | 0 | 1 |
| P3 | 9:20 | 8:50 | Early | 9:00 | 9:15 | 10 | 2 |
| P2 | 9:00 | 9:10 | Late | 9:15 | 9:31 | 5 | 2 |
| P5 | 9:40 | 9:08 | Early | 9:18 | 9:38 | 10 | 1 |
| P4 | 9:20 | 9:20 | On-time | 9:31 | 9:46 | 11 | 2 |
| P6 | 9:40 | 9:40 | On-time | 9:40 | 9:57 | 0 | 1 |
| Cost | Preempt Policy | Wait Policy |
|---|---|---|
| Radiological Technician’s Idle Time Cost | NT 5809.97 | NT 5872.74 |
| Patient Waiting Time Cost | NT 888.87 | NT 916.95 |
| Total Cost | NT 3349.41 | NT 3394.85 |
| Key Performance Index | Patient’s Inter-Arrival Time (Minutes) | ||||
|---|---|---|---|---|---|
| 16 | 18 | 20 | 22 | 24 | |
| Radiological Technician’s Idle Time Cost (NT Dollars) | 5762.35 | 5863.52 | 5809.94 | 5718.61 | 5716.29 |
| Patient Waiting Time Cost (NT Dollars) | 1623.80 | 1352.32 | 888.87 | 817.28 | 826.05 |
| Total Cost (NT Dollars) | 3693.08 | 3607.92 | 3349.41 | 3267.95 | 3271.17 |
| No. of Patients Served (Patients) | 54 | 54 | 54 | 54 | 54 |
| Average Number of Patients Waiting (Patients) | 0.99 | 0.84 | 0.54 | 0.49 | 0.49 |
| No. of Early patients (Patients) | 44.27 | 45.07 | 44.80 | 44.40 | 44.13 |
| No. of Late patients (Patients) | 8.07 | 7.20 | 7.67 | 7.80 | 8.13 |
| No. of On-time patients (Patients) | 1.66 | 1.73 | 1.53 | 1.80 | 1.74 |
| Average Waiting Time (Minutes) | 12.89 | 10.73 | 7.05 | 6.49 | 6.56 |
| Average total Time in System (Minutes) | 32.93 | 30.75 | 27.13 | 26.33 | 26.17 |
| Utilization of Scanning Rooms (%) | 53.72 | 53.86 | 53.72 | 53.55 | 52.58 |
| Key Performance Index | Patient’s Inter-Arrival Time (Minutes) | ||||
|---|---|---|---|---|---|
| 16 | 18 | 20 | 22 | 24 | |
| Radiological Technician’s Idle Time Cost (NT Dollars) | 3457.41 | 3518.11 | 3485.98 | 3431.17 | 3429.77 |
| Patient Waiting Time Cost (NT Dollars) | 649.52 | 540.93 | 355.55 | 326.91 | 330.42 |
| Total Cost (NT Dollars) | 1772.68 | 1731.80 | 1607.72 | 1568.61 | 1570.16 |
| Key Performance Index | Patient’s Inter-Arrival Time (Minutes) | ||||
|---|---|---|---|---|---|
| 16 | 18 | 20 | 22 | 24 | |
| Radiological Technician’s Idle Time Cost (NT Dollars) | 4033.65 | 4104.46 | 4066.98 | 4003.03 | 4001.40 |
| Patient Waiting Time Cost (NT Dollars) | 487.14 | 405.70 | 266.66 | 245.18 | 247.82 |
| Total Cost (NT Dollars) | 1551.09 | 1515.33 | 1406.76 | 1372.54 | 1373.89 |
| Key Performance Index | Patient’s Inter-Arrival Time (Minutes) | ||||
|---|---|---|---|---|---|
| 16 | 18 | 20 | 22 | 24 | |
| Radiological Technician’s Idle Time Cost (NT Dollars) | 4609.88 | 4690.82 | 4647.98 | 4574.89 | 4573.03 |
| Patient Waiting Time Cost (NT Dollars) | 324.76 | 270.46 | 177.77 | 163.46 | 165.21 |
| Total Cost (NT Dollars) | 1181.78 | 1154.53 | 1071.81 | 1045.75 | 1046.77 |
| Key Performance Index | Patient’s Inter-Arrival Time (Minutes) | ||||
|---|---|---|---|---|---|
| 16 | 18 | 20 | 22 | 24 | |
| Radiological Technician’s Idle Time Cost (NT Dollars) | 5186.12 | 5277.17 | 5228.97 | 5146.75 | 5144.66 |
| Patient Waiting Time Cost (NT Dollars) | 162.38 | 135.23 | 88.89 | 81.73 | 82.61 |
| Total Cost (NT Dollars) | 664.75 | 649.42 | 602.90 | 588.23 | 588.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.-S.; Chen, H.-W.; Abiog, M.D.M.; Guerrero, R.M.B.; Latina, C.G.E. Patient Unpunctuality’s Effect on Appointment Scheduling: A Scenario-Based Analysis. Healthcare 2023, 11, 231. https://doi.org/10.3390/healthcare11020231
Chen P-S, Chen H-W, Abiog MDM, Guerrero RMB, Latina CGE. Patient Unpunctuality’s Effect on Appointment Scheduling: A Scenario-Based Analysis. Healthcare. 2023; 11(2):231. https://doi.org/10.3390/healthcare11020231
Chicago/Turabian StyleChen, Ping-Shun, Hsiu-Wen Chen, Marielle Donice M. Abiog, Roxanne Mae B. Guerrero, and Christine Grace E. Latina. 2023. "Patient Unpunctuality’s Effect on Appointment Scheduling: A Scenario-Based Analysis" Healthcare 11, no. 2: 231. https://doi.org/10.3390/healthcare11020231