Fibromyalgia Syndrome Pain in Men and Women: A Scoping Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Selection of the Studies
2.4. Data Extraction
2.5. Process Followed to Determine the Categories and Subcategories of Pain in the Qualitative Studies
3. Results

3.1. Pain Qualities
3.2. Uncertainty and Chaos
3.3. Pain as an Aggravating Factor
3.4. Adaptations to the New Reality
3.5. Communication of Pain
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Section | Item | Prisma-ScR Checklist Item | Page |
|---|---|---|---|
| Title | 1 | Fibromyalgia Syndrome Pain in Men and Women: A Scoping Review | 1 |
| Abstract | |||
| Structured summary | 2 | Fibromyalgia syndrome (FMS) is a chronic musculoskeletal disorder of unknown etiology that affects up to 5.0% of the world population. It has a high female predominance, between 80 and 96%. Due to the low number of diagnosed men, research work has focused mainly on women. The extensive body of literature on sex differences in pain in the general population suggests that men and women differ in their responses to pain, with greater sensitivity to pain and a higher risk of clinical pain commonly observed among women. This review aims to (1) determine how pain is assessed or what types of questionnaires are used, (2) examine whether there are differences in pain characteristics between men and women with FMS and (3) describe how pain is conceptualized or manifested in patients at a qualitative level. In this study, the scoping review method of articles published in the last 5 years (2016–2022) was used. Ten articles were included. The most used questionnaires and scales to assess pain were the PVAS (Pain Visual Analogue Scale) and the FIQ (Fibromyalgia Impact Questionnaire). On the other hand, five categories were obtained: (1) qualities of pain, (2) uncertainty and chaos, (3) pain as an aggravating factor, (4) adaptation to the new reality and (5) communication of pain. It has been observed that both subjective perception and widespread pain are higher in women. Men, on the other hand, have a worse impact of the pathology, more painful experiences and more catastrophic thoughts about pain. In any case, the results have little statistical significance. To obtain higher quality results, it is essential to increase the sample of men with FMS in future studies in order to be able to deepen these differences. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | The choice of the scoping review was mainly due to the heterogeneous nature of FMS in existing studies to date. The scoping review allows us to better group the literature according to its characteristics. | 2 |
| Objectives | 4 | The present review has focused the study of pain in men and women in FMS. Our objectives focused on (1) determining how pain is assessed or what types of questionnaires are used, (2) examining whether there are differences in pain characteristics between men and women with FMS and (3) describing how pain is conceptualized or manifested in the participants at a qualitative level. | 3 |
| Methods | |||
| Protocol and registration | 5 | Not applicable. The review protocol is in the process of being accepted by PROSPERO: www.crd.york.ac.uk/prospero/, accessed on 10 November 2022 | |
| Eligibility criteria | 6 | The identified studies were subjected to inclusion and exclusion criteria. To be included, studies had to be published from January 2016 to July 2022, available in full text, written in English or Spanish and use both quantitative (observational studies) and qualitative methodology. | 3 |
| Information sources | 7 | The bibliographic search was carried out during the months of February and July 2022. The electronic databases used for the search were PubMed, SCOPUS, CINAHL, Web of Science and Google Scholar. In each of these, an exhaustive search was performed using a combination of Boolean logic and truncations for the following keywords: “pain”, “fibromyalgia”, “men”, “women”, “conceptualization”, “manifestation”, “score” and “assessment”. | 3 |
| Search | 8 | The following search string was used for PubMed database, we used ((((“Fibromyalgia”(Mesh)) AND “Pain”(Mesh)) AND “Men”(Mesh)) OR “Women”(Mesh)) OR (“Pain Measurement/classification”(Mesh) OR “Pain Measurement/instrumentation”(Mesh) OR “Pain Measurement/nursing”(Mesh) OR “Pain Measurement/psychology”(Mesh)) OR (score) OR (concept*) OR (manifestation) OR (assessment). | 3 |
| Selection of sources of evidence | 9 | The electronic databases selected for the search were PubMed, SCOPUS, CINAHL, Web of Science and Google Scholar. | 3 |
| Data charting process | 10 | Data were extracted from full-text articles that met the objectives and inclusion criteria. Definitive data were obtained using a data extraction form with the following information: author(s), year of publication, country, study design, study objective(s), participants (sex and age range). In the case of quantitative studies, the types of questionnaires used were also considered. In the qualitative articles, for the review of the experiences of men and women with FMS, the authors proceeded to analyze the discourses related to the conceptualization or manifestation of pain by means of categories and subcategories. | 4 |
| Data items | 11 | The variables used for the data search were “pain”, “fibromyalgia”, “men”, “women”, “conceptualization”, “manifestation”, “score” and “assessment”. | |
| Results | |||
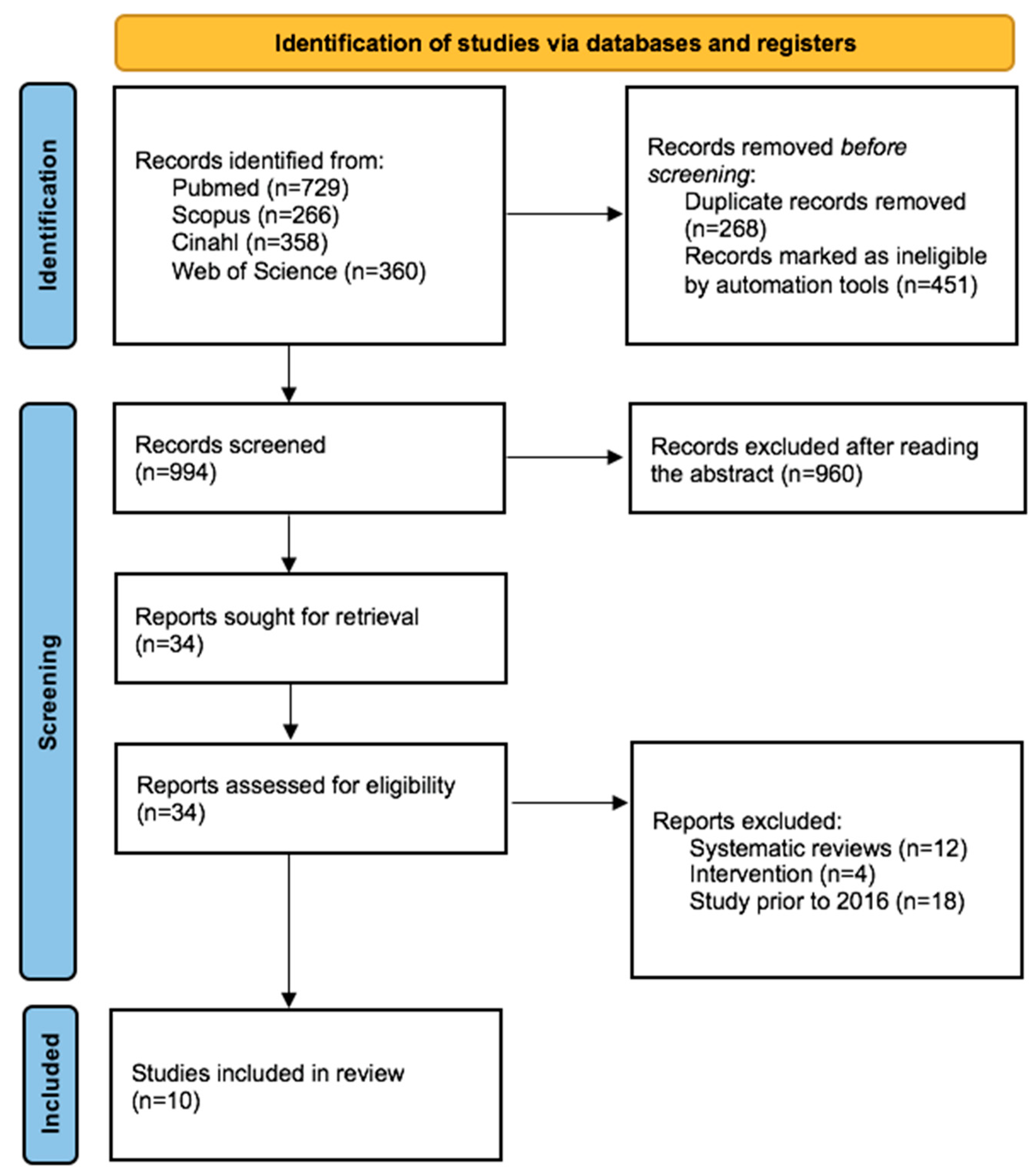
| Selection of sources of evidence | 12 | Figure 1 | 4 |
| Synthesis of results | 13 | Of the 10 studies that met the inclusion criteria, 7 were quantitative, 2 qualitative and 1 mixed. Sample sizes ranged from 5 to 4.342 participants. The female sex predominated with 56.7%. In all studies, the age range was 18 years or older; older subjects had a mean age of 56.6 ± 12.6 years. The pain assessment of the selected quantitative studies included a wide variety of questionnaires and scales. The most used were the PVAS (out of 10 or out of 100) and the FIQ. On the other hand, qualitative studies used tools such as focus groups, interviews, narrative and life history to describe how pain manifests itself in men and women with FMS. The PVAS and WPI were higher in female participants. In Wolfe’s study, males were older (64.9 ± 12.0 years) than females (59.7 ± 13.5 years). In contrast, in the Jiao study men were significantly younger p = 0.027 (43.6 years) than women (50.1 years). The FIQ and PCS were somewhat higher in men than in women in the Segura-Jiménez study, but without statistical significance. There were no differences for the rest of the scales. The review of the qualitative literature allowed us to identify the existence of categories related to pain. A total of five categories were obtained: (1) qualities of pain, (2) uncertainty and chaos, (3) pain as an aggravating factor, (4) adaptation to the new reality and (5) communication of pain. In the first category—pain qualities—we integrated the results related to the pain characteristics reported by patients in the chosen studies. The second category—uncertainty and chaos—describes how patients cope with chronic pain. The third category—pain as an aggravating factor—reflects the different causes of chronic pain in patients. In the fourth category—adaptation to the new reality—we show how patients make vital changes to continue living with pain. Finally, in the last category—pain communication—we show the importance of expressing emotions and sharing the experience of pain as a benefit for the person. | 4–11 |
| Discussion | |||
| Summary of evidence | 14 | This review provides an updated synthesis of fibromyalgia pain from different approaches to better understand it. The first objective of this review was to determine how pain is assessed, i.e., which questionnaires are commonly used. The results show that the PVAS (which assesses the subjective perception of global pain) and the FIQ (which assesses the impact of illness) were the most used tools. We contrasted whether there were differences in pain characteristics according to sex. We detected that the subjective perception of pain was higher in women, as was the generalized pain index (WPI). In contrast, FMS impact was higher in men as were painful experiences and PCS pain thoughts. Although several examples of epidemiological evidence have shown that chronic pain conditions are more prevalent among women than among men, in our review we only detected this in Jiao’s study, which revealed significant differences in pain according to sex. Women with FMS had worse values in the WPI questionnaire (generalized pain) and men with FMS had worse values in the SSS (severity of symptoms). Finally, through the use of qualitative methodology this review wanted to describe how pain is conceptualized or manifested in affected individuals. Pain, according to male participants in the studies by Sallinen and Mengshoel and Kueny, has qualities of being fluctuating. Also, agonizing and unbearable at the worst times. Unlike other studies, the pain of the men in Kueny et al. is of a localized type, not generalized and has a stabbing characteristic such as an arrow or sword. According to Ruschak’s study, the pain of men with FMS was also described as “like an arrow or heart attack” and of a fluctuating type; i.e., it was present in different parts of the body, not generalized. The chronicity and random nature of fibromyalgia pain causes much uncertainty and chaos in the lives of these patients. Fatigue and insomnia also entail major problems in their lives, which are closely linked to pain, which is their direct aggravating factor, a phenomenon also shared by the study of Ruschak et al. These in turn also limit them at all levels of their social relationships because the invisible nature of pain means that patients have to be their own advocates in front of others, because they do not believe them. These challenging situations full of negative attitudes have been previously described in other studies on FMS. According to Ruschak and colleagues, the lack of empathy shown by some healthcare professionals, as well as their family and friends, have had a very negative impact on patients’ health, especially mental health. Sallinen suggests that there is also a consequence on their identity, especially their masculinity, as it has to be renegotiated and reconstructed. All these changes in their lives are difficult to face, but necessary. Acceptance of the new reality helps people to move on, mainly with the help of others. This help begins with communicating their discomfort and finding a receptive listener so that they can talk about their pain. | 12–13 |
| Limitations | 15 | Some limitations must be mentioned. First, reducing the review to the last 5 years has led us to identify that there are fewer studies than we thought related to the subject. Secondly, in most of the mixed studies, the proportion of men to women is unbalanced; the low male representation is detrimental to them and limits their perspective. Finally, there are biases in some regions; we detected that there are countries in which FMS is not studied as much, for example Asian countries. This is probably due to the type of healthcare access they have or their cultural beliefs. In short, FMS remains an area that needs more awareness and investigation by researchers. | 14 |
| Conclusions | 16 | The results of this review provide updated information on FMS pain in both sexes. To date, we can see that pain remains a very complex, internal and private sensory experience and more so in men because FMS is still mostly conceptualized as a women’s disease. It has been observed in a few studies that both subjective perception and the generalized pain index are higher for women, but a worse impact, more painful and more severe experiences and also more catastrophic thoughts about pain in men should be considered. In any case, the results have little statistical significance and we consider that it is necessary to increase the sample of men in the studies so that these differences can be studied in greater depth. To improve pain care in these patients, we believe that there is a need for multidisciplinary management including educational interventions aimed at health care personnel on the different concepts of pain (subjective perception, impact of pain, widespread pain, localized pain, severity of symptoms, catastrophic thoughts about pain) to thus help to improve the understanding of individual and gender differences in pain. The results of this review have been made possible by the increasing inclusion of men with FMS and the awareness that the male experience and perspective is just as important as the female. Even so, we encourage further expansion of the male sample in future studies, because with the current results the significative differences in male and female pain did not reach statistical significance in all studies, probably due to the small sample of men. | 13 |
References
- Jiao, J.; Cheng, Z.; Wang, W.; Zhao, Y.; Jiang, Q. Demographic Characteristics and Clinical Features of Fibromyalgia in China: A Cross-Sectional Study. Rheumatol. Ther. 2021, 8, 817–831. [Google Scholar] [CrossRef]
- Queiroz, L.P. Worldwide Epidemiology of Fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 356. [Google Scholar] [CrossRef]
- Gayà, T.F.; Ferrer, C.B.; Mas, A.J.; Seoane-Mato, D.; Reyes, F.; Sánchez, M.D.; Dubois, C.M.; Sánchez-Fernández, S.A.; Vargas, L.M.R.; Morales, P.V.G.; et al. Prevalence of fibromyalgia and associated factors in Spain. Clin. Exp. Rheumatol. 2020, 123, 47–52. [Google Scholar]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J. Fibromialgia: Prevalencia, perfiles epidemiológicos y costes económicos. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef]
- Montesó-Curto, P.; Rosselló Aubach, L. (Eds.) Compartir Experiencias, Combatir el Dolor. Publicaciones urv: Tarragona, Spain, 2017. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of fibromyalgia in general population and patients, a systematic review and meta-analysis. Rheumatol. Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef]
- Miró, E.; Martínez, M.P.; Sánchez, A.I.; Prados, G.; Lupiáñez, J. Men and women with fibromyalgia: Relation between attentional function and clinical symptoms. Br. J. Health Psychol. 2014, 20, 632–647. [Google Scholar] [CrossRef]
- Paulson, M.; Norberg, A.; Danielson, E. Men living with fibromyalgia-type pain: Experiences as patients in the Swedish health care system. J. Adv. Nurs. 2002, 40, 87–95. [Google Scholar] [CrossRef]
- Bartley, E.J.; Fillingim, R.B. Sex differences in pain: A brief review of clinical and experimental findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Fauchon, C.; Meunier, D.; Rogachov, A.; Hemington, K.S.; Cheng, J.C.; Bosma, R.L.; Osborne, N.R.; Kim, J.A.; Hung, P.S.-P.; Inman, R.D.; et al. Sex differences in brain modular organization in chronic pain. Pain 2020, 162, 1188–1200. [Google Scholar] [CrossRef]
- Kang, J.-H.; Choi, S.-E.; Park, D.-J.; Lee, S.-S. Disentangling Diagnosis and Management of Fibromyalgia. J. Rheum. Dis. 2022, 29, 4–13. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Araya-Quintanilla, F.; Gutiérrez-Espinoza, H.; Muñoz-Yánez, M.J.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Martinez-Vizcaíno, V. Effectiveness of a multicomponent treatment versus conventional treatment in patients with fibromyalgia. Medicine 2020, 99, e18833. [Google Scholar] [CrossRef]
- Giusti, E.M.; Castelnuovo, G.; Molinari, E. Differences in Multidisciplinary and Interdisciplinary Treatment Programs for Fibromyalgia: A Mapping Review. Pain Res. Manag. 2017, 2017, 7261468. [Google Scholar] [CrossRef] [Green Version]
- Sallinen, M.; Mengshoel, A.M. “I just want my life back!”—Men’s narratives about living with fibromyalgia. Disabil. Rehabil. 2017, 41, 422–429. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Mease, P.; Arnold, L.M.; Bennett, R.; Boonen, A.; Buskila, D.; Carville, S.; Chappell, A.; Choy, E.; Clauw, D.; Dadabhoy, D.; et al. Fibromyalgia síndrome. J. Rheumatol. 2007, 34, 1415–1425. [Google Scholar]
- Trouvin, A.-P.; Perrot, S. New concepts of pain. Best Pract. Res. Clin. Rheumatol. 2019, 33, 101415. [Google Scholar] [CrossRef]
- Moher, D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Trico, A.; Khalil, H. Chapter 11: Scoping Reviews. JBI Man. Evid. Synth. 2020, 1, 419–420. [Google Scholar] [CrossRef]
- Sandelowski, M. What’s in a name? Qualitative description revisited. Res. Nurs. Health 2010, 33, 77–84. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Estévez-López, F.; Soriano-Maldonado, A.; Álvarez-Gallardo, I.C.; Delgado-Fernández, M.; Ruiz, J.R.; Aparicio, V.A. Gender Differences in Symptoms, Health-Related Quality of Life, Sleep Quality, Mental Health, Cognitive Performance, Pain-Cognition, and Positive Health in Spanish Fibromyalgia Individuals: The Al-Ándalus Project. Pain Res. Manag. 2016, 2016, 5135176. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F.; Walitt, B.; Perrot, S.; Rasker, J.J.; Häuser, W. Fibromyalgia diagnosis and biased assessment: Sex, prevalence and bias. PLoS ONE 2018, 13, e0203755. [Google Scholar] [CrossRef] [Green Version]
- Prateepavanich, P.; Yeephu, S.; Suttiruksa, S.; Suthisisang, C.; Saisavoey, N. Demographic and Clinical Characteristics of Thai Patients with Fibromyalgia Syndrome. J. Med. Assoc. Thai. 2018, 101, S164–S170. [Google Scholar]
- De Roa, P.; Paris, P.; Poindessous, J.L.; Maillet, O.; Héron, A. Subjective Experiences and Sensitivities in Women with Fibromyalgia: A Quantitative and Comparative Study. Pain Res. Manag. 2018, 2018, 8269564. [Google Scholar] [CrossRef] [Green Version]
- Úbeda-D’Ocasar, E.; Valera-Calero, J.A.; Hervás-Pérez, J.P.; Caballero-Corella, M.; Ojedo-Martín, C.; Gallego-Sendarrubias, G.M. Pain Intensity and Sensory Perception of Tender Points in Female Patients with Fibromyalgia: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 1461. [Google Scholar] [CrossRef]
- Iannuccelli, C.; Lucchino, B.; Gioia, C.; Dolcini, G.; Rabasco, J.; Venditto, T.; Ioppolo, F.; Santilli, V.; Conti, F.; Di Franco, M. Gender influence on clinical manifestations, depressive symptoms and brain-derived neurotrophic factor (BDNF) serum levels in patients affected by fibromyalgia. Clin. Rheumatol. 2022, 41, 2171–2178. [Google Scholar] [CrossRef]
- Kueny, A.; Montesó-Curto, P.; Lunn, S.; Mohabbat, A.B.; Clark, S.; Luedtke, C.; Vincent, A.; Ruschak, I.; Mateu-Gil, M.L.; Panisello-Chavarria, M.L.; et al. Fibromyalgia Pain and Fatigue Symptoms in Spanish and U.S. Men. Pain Manag. Nurs. 2021, 22, 423–428. [Google Scholar] [CrossRef]
- Sendra, A.; Farré, J. Communicating the experience of chronic pain through social media: Patients’ narrative practices on Instagram. J. Commun. Healthc. 2020, 13, 46–54. [Google Scholar] [CrossRef]
- Bennett, R.M.; Bushmakin, A.G.; Cappelleri, J.C.; Zlateva, G.; Sadosky, A.B. Minimal Clinically Important Difference in the Fibromyalgia Impact Questionnaire. J. Rheumatol. 2009, 36, 1304–1311. [Google Scholar] [CrossRef]
- Wolfe, F.; Brähler, E.; Hinz, A.; Häuser, W. Fibromyalgia Prevalence, Somatic Symptom Reporting, and the Dimensionality of Polysymptomatic Distress: Results from a Survey of the General Population. Arthritis Care Res. 2013, 65, 777–785. [Google Scholar] [CrossRef]
- Huskisson, E.C. Visual analogue scale. In Pain Measurement and Assessment; Melzack, R., Ed.; Raven Press: New York, NY, USA, 1983; pp. 33–37. [Google Scholar]
- Fillingim, R.B. Individual differences in pain: Understanding the mosaic that makes pain personal. Pain 2016, 158, S11. [Google Scholar] [CrossRef] [Green Version]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L. Sex, Gender, and Pain: A Review of Recent Clinical and Experimental Findings. J. Pain 2009, 10, 447–485. [Google Scholar] [CrossRef] [Green Version]
- Ruschak, I.; Toussaint, L.; Rosselló, L.; Aguilar Martín, C.; Fernández-Sáez, J.; Montesó-Curto, P. Symptomatology of Fibromyalgia Syndrome in Men: A Mixed-Method Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 1724. [Google Scholar] [CrossRef]
- Conrad, P.; Barker, K.K. The Social Construction of Illness: Key Insights and Policy Implications. J. Health Soc. Behav. 2010, 51 (Suppl. S1), S67–S79. [Google Scholar] [CrossRef]
- Katz, J.D.; Mamyrova, G.; Guzhva, O.; Furmark, L. Gender bias in diagnosing fibromyalgia. Gend. Med. 2010, 7, 19–27. [Google Scholar] [CrossRef]
- Ressler, P.K.; Bradshaw, Y.S.; Gualtieri, L.; Chui, K.K.H. Communicating the Experience of Chronic Pain and Illness Through Blogging. J. Med. Internet Res. 2012, 14, e143. [Google Scholar] [CrossRef]
| Reference (Country) Study Type | Aim | Sample | Questionnaires and Scales | Findings |
|---|---|---|---|---|
| Segura-Jiménez et al., 2016 (Spain) [24] Comparative Cross-Sectional Study Quantitative | To examine gender differences in sensitivity, fibromyalgia impact, health-related quality of life, fatigue, sleep quality, mental health, cognitive performance, pain cognition and positive health in Spanish fibromyalgia patients and non-fibromyalgia individuals of the same age and region. To observe the optimal cut-off score of the different sensitive items for women and men. | FM patients = 388 W = 367 M = 21 No FM patients = 285 W = 232 M = 53 | Tender Points (0–18) | FM-W: 16.8 ± 0.1 FM-M: 16.8 ± 0.4 p = 0.877 NS No FM-W: 3.3 ± 0.2 No FM-M: 0.8 ± 0.4 p < 0.001 Women reported greater pain sensitivity |
| Fibromyalgia Impact Questionnaire (0–100) | FM-W: 64.7 ± 0.9 FM-M: 65.5 ± 3.6 p = 0.837 NS No FM-W:20.7 ± 0.9 No FM-M:18.7 ± 1.9 p = 0.339 NS | |||
| Pain Catastrophizing Scale (0–52) | FM-W: 25.1 ± 0.7 FM-M: 26.2 ± 2.7 p = 0.712 NS No FM-W: 11.2 ± 0.7 No FM-M: 9.9 ± 1.5 p = 0.427 NS | |||
| Wolfe et al., 2018 (EE. UU.) [25] Longitudinal Study Quantitative | To compare CritFM with ClinFM to investigate gender and other biases in fibromyalgia diagnosis. | FM patients = 4342 W = 2171 M = 2171 Age = 56.6 ± 12.6 years W = 59.7 ± 13.5 years M = 64.9 ± 12.0 years | Widespread Pain Index (0–19) | FM-W:5.9 ± 0.7 FM-M:4.9 ± 1.3 |
| Symptom Severity Scale (0–12) | FM-W = 4.3 ± 0.7 FM-M = 3.4 ± 1.1 | |||
| Polysymptomatic Distress (0–31) | FM-W = 10.2 ± 1.6 FM-M = 8.2 ± 1.6 | |||
| Pain Visual Analogue Scale (0–10) | FM-W = 3.9 ± 0.3 FM-M = 3.4 ± 1.0 | |||
| Higher values of pain and symptom severity were detected in women relative to men. Since FMS is defined based on pain and symptom severity, women will always be more likely to be diagnosed. In short, there is a relationship between being female and being diagnosed with FMS. | ||||
| Prateepavanich et al., 2018 (Thailand) [26] Cross-Sectional Study Quantitative | To obtain demographic data, clinical characteristics and investigate correlations of clinical features in Thai patients with FMS. | FM patients = 71 W = 69 M = 2 Age = 44.83 (±10.81) years | Pain Visual Analogue Scale (0–100) | 63.39 ± 17.8 |
| Fibromyalgia Impact Questionnaire (0–100) | 45.48 ± 16.83 | |||
| De Roa et al., 2018 (France) [27] Comparative Cross-Sectional Study Quantitative | To characterize childhood experiences, perceived lack of parental affection, hypersensitivity to stimuli, life stressors, anxio-depression and ergomania. | FM-W patients = 44 Migraine-W patients= 34 Age = 45 ± 12 years | Pain Visual Analogue Scale (0–10) | Better moments: FM-W = 3.3 ± 1.9 Migraine-W= 1.8 ± 2.3 Worse moments: FM-W = 8.9 ± 1.4 Migraine-W= 8.7 ± 1.2 NS Scores |
| Jiao et al., 2021 (China) [1] Cross-Sectional Study Quantitative | To characterize the demographics, severity of fibromyalgia-related symptoms and quality of life (QoL) among Chinese fibromyalgia patients. | FM patients = 124 FM-W = 107 FM-M = 17 Age-W = 50.1 years Age-M = 43.6 years P = 0.027 M significantly younger Mean age= 49.4 years | Pain Visual Analogue Scale (0–100) | FM-W: 56.2 ± 21.7 FM-M: 54.1 ± 25.5 p = 0.72 NS |
| Widespread Pain Index (0–19) | FM-W = 11.1 ± 4.7 FM-M = 8.6 ± 3.9 p = 0.038 Women higher values of pain | |||
| Symptom Severity Scale (0–12) | FM-W = 7.4 ± 2.6 FM-M = 8.7 ± 1.8 p = 0.06 Males higher values of symptom severity | |||
| Polysymptomatic Distress (0–31) | FM-W = 18.5 ± 5.9 FM-M = 17.2 ± 4.6 p = 0.40 NS No gender differences in either group | |||
| Úbeda-D’Ocasar et al., 2021 (Spain) [28] Descriptive Exploratory Study Quantitative | To assess the pain pressure thresholds (PPT) and subjective pain perception (SPP) of the 18 PTs while applying standardized pressure. | n= 30 W Mean age = 55.1 ± 8.7 years | Fibromyalgia Impact Questionnaire (0–100) | FM-W: 64.1 ± 14.4 Nine locations were examined bilaterally: TP1 forehead; TP2 intertransverse space of C5-C7; TP3 midpoint of the trapezius muscle; TP4 supraspinatus muscle; TP5 second costochondral junction; TP6 2 cm distal to the lateral epicondyle; TP7 upper outer quadrant buttocks; TP8 trochanteric prominence; TP9 in the medial fat of the knee. |
| Pain Visual Analogue Scale (0–100) | The most painful points located in: TP7: 69.6 ± 19.4 TP8: 68.0 ± 21.5 TP4: 65.1 ± 21.1 The lowest points located in: TP5: 1.28 ± 0.42 TP1: 1.52 ± 0.34 TP8: 1.61 ± 0.59 p > 0.05 NS | |||
| Iannuccelli et al., 2022 (Italy) [29] Cross-Sectional Study Quantitative | To evaluate the influence of gender on clinical manifestations, with special attention to the neuropsychiatric features of FMS. | n = 172 W n = 29 M Mean age = 49.13 years | Pain Visual Analogue Scale (0–10) | FM-W = 7.5 ± 1.64 FM-M = 6.52 ± 2.06 p = 0.0130 |
| Fibromyalgia Impact Questionnaire (0–100) | FM-W = 68.07 ± 16.06 FM-M = 55.17 ± 18.26 p = 0.0005 | |||
| Widespread Pain Index (0–19) | FM-W = 10.67 ± 3.91 FM-M = 10.90 ± 4.81 p = NS No gender differences in either group | |||
| Symptom Severity Scale (0–12) | FM-W = 9.24 ± 1.72 FM-M = 8.724 ± 1.79 p = NS No gender differences in either group | |||
| Kueny et al., 2021 (EEUU, Spain) [30] Mixed
| To describe the pain and fatigue experiences of men with MFS from Spain and the United States. | n = 17 M Spain-M = 10 USA-M = 7 Age range = 30–63 years Mean Age = 52 years | Fibromyalgia Impact Questionnaire (0–100) | Spain M: 81.93 ± 5.89 USA M: 67.99 ± 15.33 p = 0.08 The difference only approached statistical significance. |
| To describe the pain and fatigue experiences of men with MFS from Spain and the United States. | n = 17 M Spain-M = 10 USA-M = 7 Age range = 30–63 years Mean Age = 52 years | Focus groups and interviews |
|
| Sallinen and Mengshoel, 2017 (Finland) [16] Qualitative | To elucidate the impacts of FMS on men’s daily life and work capacity. | n = 5 M | Life story |
|
| Sendra and Farré, 2020 (Global) [31] Qualitative | To identify how and why patients use online platforms for pain communication. | n= 350 M and W | Narrative |
|
| N° | Category | Questionnaires and Scales |
|---|---|---|
| 1 | Total number of Tender Points | TP (0–18): Patients were considered to have fibromyalgia if they had 11 or more positive tender points [24]. |
| 2 | Fibromyalgia Impact Questionnaire | FIQ (0–100): Comprises 21 individual questions with a rating scale of 0 to 10. These questions comprise three different domains: function, overall impact and symptoms score (ranging 0–30, 0–20 and 0–50, resp.). The FIQR total score ranges from 0 to 100, with a higher score indicating greater impact [32]. |
| 3 | Pain Catastrophizing Scale | PCS (0–52): Was used to assess painful experiences and thoughts or feelings about pain. It contains 13 items on a 5-point scale. For this study, the total score (ranging from 0 to 52) was used, where higher score represents a more negative appraisal of pain [24]. |
| 4 | Widespread Pain Index | WPI (0–19): The widespread pain index is a summary count of the number of 19 painful regions, a self-reported list of painful regions [29]. |
| 5 | Symptom Severity Scale | SSS (0–12): The symptom severity scale is the sum of the severity scores of three symptoms (fatigue, waking without rest and cognitive symptoms) (0–9) plus the sum (0–3) of the number of the following symptoms that have bothered the patient and occurred during the previous 6 months: (1) headaches (0–1), (2) lower abdominal pain or cramps (0–1) and (3) depression (0–1 [29]). |
| 6 | Polysymptomatic Distress | PSD (0–31): The polysymptomatic discomfort scale (known as FM severity), is the sum of the WPI and SSS. The PSD measures the magnitude and severity of FM symptoms [33]. |
| 7 | Pain Visual Analogue Scale | PVAS (0–10) or (0–100): Assesses the subjective perception of global pain (from 0, no pain, to 10 or 100, maximum pain) [34]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruschak, I.; Montesó-Curto, P.; Rosselló, L.; Aguilar Martín, C.; Sánchez-Montesó, L.; Toussaint, L. Fibromyalgia Syndrome Pain in Men and Women: A Scoping Review. Healthcare 2023, 11, 223. https://doi.org/10.3390/healthcare11020223
Ruschak I, Montesó-Curto P, Rosselló L, Aguilar Martín C, Sánchez-Montesó L, Toussaint L. Fibromyalgia Syndrome Pain in Men and Women: A Scoping Review. Healthcare. 2023; 11(2):223. https://doi.org/10.3390/healthcare11020223
Chicago/Turabian StyleRuschak, Ilga, Pilar Montesó-Curto, Lluís Rosselló, Carina Aguilar Martín, Laura Sánchez-Montesó, and Loren Toussaint. 2023. "Fibromyalgia Syndrome Pain in Men and Women: A Scoping Review" Healthcare 11, no. 2: 223. https://doi.org/10.3390/healthcare11020223