
Effects of Physical Activity Program on Body Composition, Physical Performance, and Neuromuscular Strategies during Walking in Older Adults with Sarcopenic Obesity: Randomized Controlled Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.2.1. Eligibility Criteria
2.2.2. Sample Size
2.2.3. Randomization Procedure
2.3. Intervention: PSM Program
- Name: The PSM program
- Why: The PSM program aimed to enhance physical performance, walking capacity in older adults with SO.
- What (Materials): The PSM program employed various physical materials to aid in the performance of the exercises; chairs for exercises such as sit-to-stands, balls for coordination and balance training, a stopwatch for timing exercises, markers, slats, and cups for creating obstacles or guiding movement paths, hoops, elastic bands, and weighted bags to increase resistance and challenge in the exercises.
- What (Procedures): The PSM program spanned 24 weeks, including two 60-min sessions per week, for a total of 48 sessions. Each session includes a warm-up (10 min), motor skill exercises (duration based on the pre-set training volume), strengthening/posture exercises (duration based on the pre-set training volume), and a cool-down phase (5 min). Motor Skill exercises form an interactive segment involving dynamic movements such as interactive walking, where participants maintain eye contact as they walk towards each other or retreat to their original positions. These exercises also include various obstacle courses that require participants to navigate through specified areas, stepping over objects like cups or hoops without making contact. Additionally, participants engage in weight-fetching drills, which require rising from a seated position, navigating obstacles, retrieving weighted bags, and returning to the start point. To add a layer of complexity and competitive spirit, these exercises are varied by increasing the number of objects, timing tasks, or introducing competitive elements among groups. Simultaneously, strength training exercises focus on enhancing various muscle groups. Participants execute a wide array of movements, including ankle dorsiflexion, plantar flexion, and exercises that emphasize upper body and postural muscles such as arm flexion/extension and lumbar muscle strengthening. Resistance training is also integrated using weights and balls, adding an additional challenge to the exercises. Progressive challenges are introduced by adjusting the speed of execution, altering arm positions, and incrementally adding weights to amplify the difficulty level. The program also incorporates posture exercises designed to enhance the proprioceptive system and improve balance. Participants engage in exercises such as balancing on unstable surfaces and resisting mild pressure exerted on various body parts by a partner. They also perform exercises like traversing obstacles with added weights, stimulating their balance and postural control. Multi-directional pressure resistance exercises further enhance balance, sometimes incorporating unexpected pushes to present an added layer of challenge.
- Who: By a kinesiologist specialized in adapted physical activity.
- How: In collective, face-to-face sessions.
- Where: In the fitness hall of each respective structure.
- When and how much: The PSM program begins on the 21st of March and concludes on the 21st of September 2022, spanning a total of 24 weeks. Each week includes two sessions, making a cumulative total of 48 sessions. Each session is 60 min long. The design of all exercise types within the program was based on each session’s specific training load (see item 9) and on pre-set training intensity and volume for each session (see item 11). The regimen for each exercise type involved anywhere between 1 to 5 sets, with the repetitions for each set ranging from a minimum of 3 to a maximum of 15.
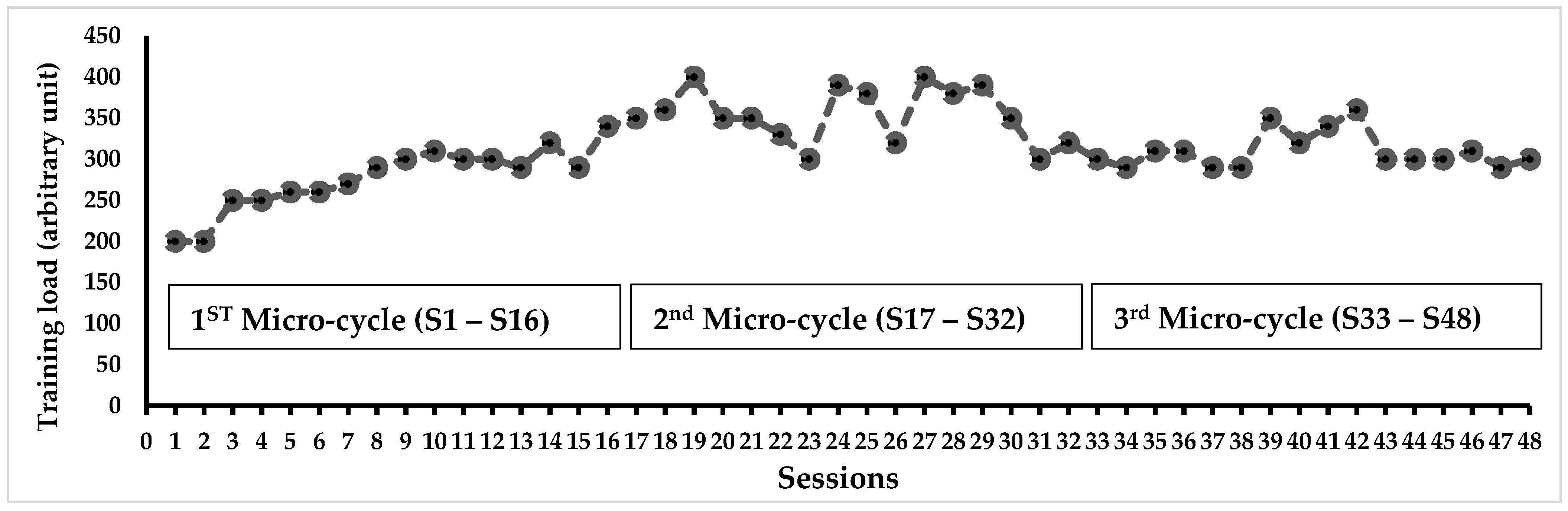
- Tailoring: The variation in training load was determined after each session, based on the rating of perceived exertion scale (RPE) [54]. The RPE scale ranges from 0 (no difficulty) to 10 (extremely difficult), and the training load of the group was calculated by multiplying the session’s RPE score by its duration (e.g., for a group with an average RPE score of 6 in a 60-min session, the training load would be equal to 360 arbitrary units (a.u.). This method ensures the training’s efficiency, especially regarding the progression of solicitation, and allows for the monitoring of a possible overtraining syndrome. When the training load exceeded 300 a.u. (equivalent to 5 × 60 min), it was maintained for the next session. When the training load was below 300, the number of series and repetitions was increased by 25% in the next session.
- Modifications: Adjustments were made to the exercises in each session, with an increase in the number of series or repetitions based on the training load. The difficulty was also progressively enhanced by adding obstacles, setting a time limit for task completion, and other means to ensure gradual progression and increasing solicitation.
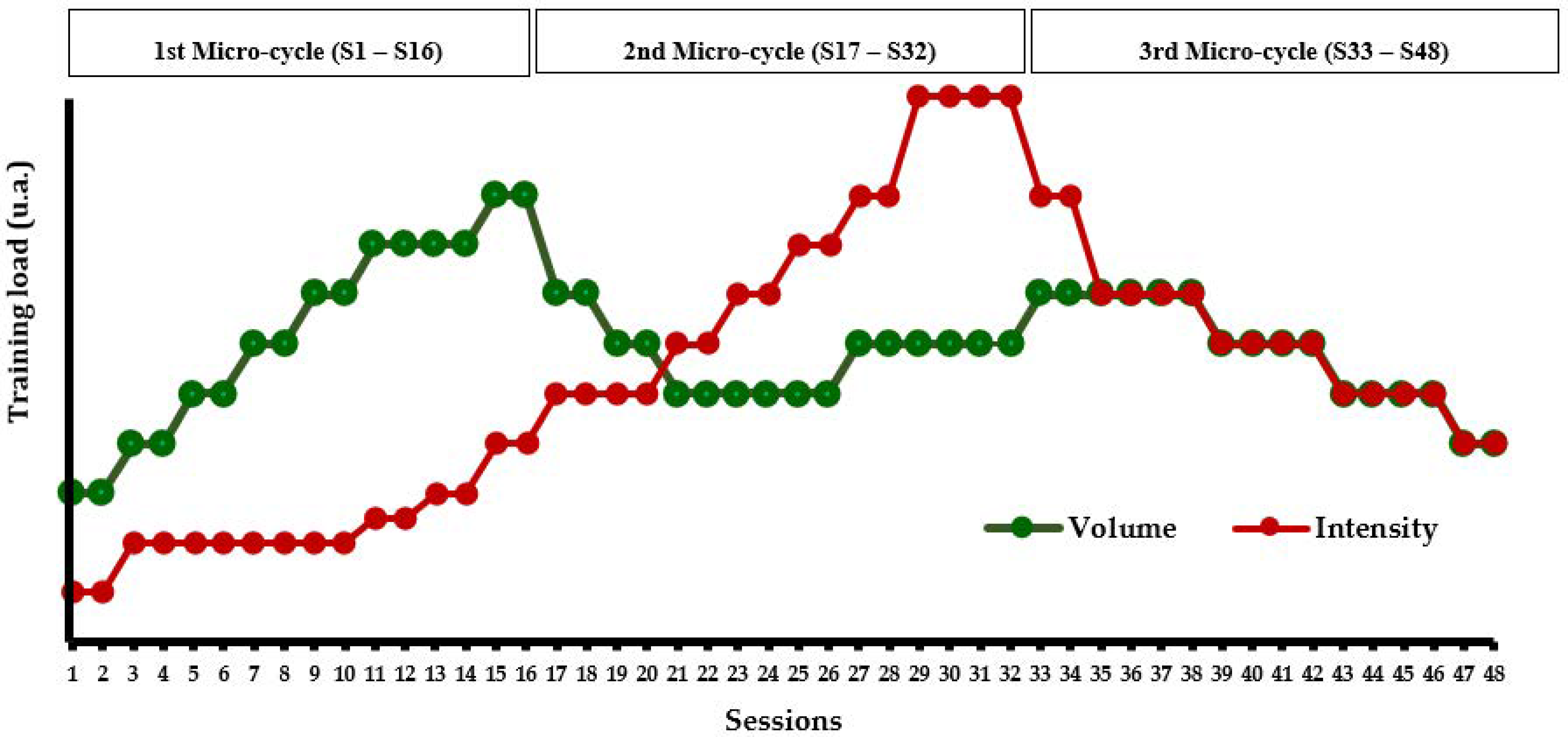
- How well (planned): The program’s progressiveness was based on two aspects: a quantitative aspect related to the training load (volume/intensity) and a qualitative aspect related to the type of exercises (muscle strengthening, balance, and motor skills exercises). According to the quantitative aspect, the PSM program was structured into 3 micro-cycles of 16 sessions each: the first micro-cycle focused on volume, the second on intensity, and the third micro-cycle aimed to balance both volume and intensity (Figure 2). According to the qualitative aspect, the PSM program was divided into 3 micro-cycles based on the type of exercises. The first cycle mainly focused on motor skills exercises (i.e., higher duration), the second on balance and muscle strengthening exercises, and the third cycle offered all types of exercises in a balanced way. The quantity of the different types of exercise was regulated every week (Figure 3).
- How well (actual): the TG attended all sessions.
2.4. Evaluation Protocol
2.4.1. Anthropometric Measurements and Clinical Tests
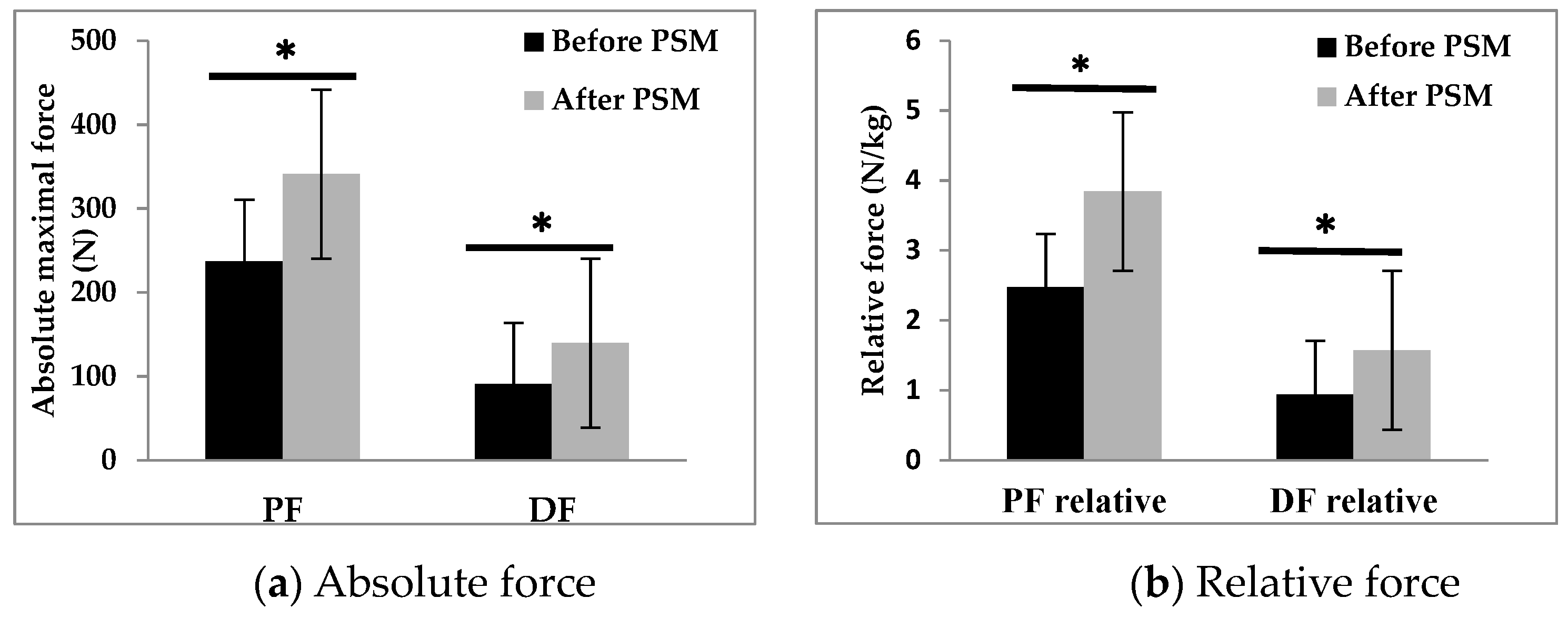
2.4.2. Maximal Voluntary Contraction Test
2.4.3. Walking Test
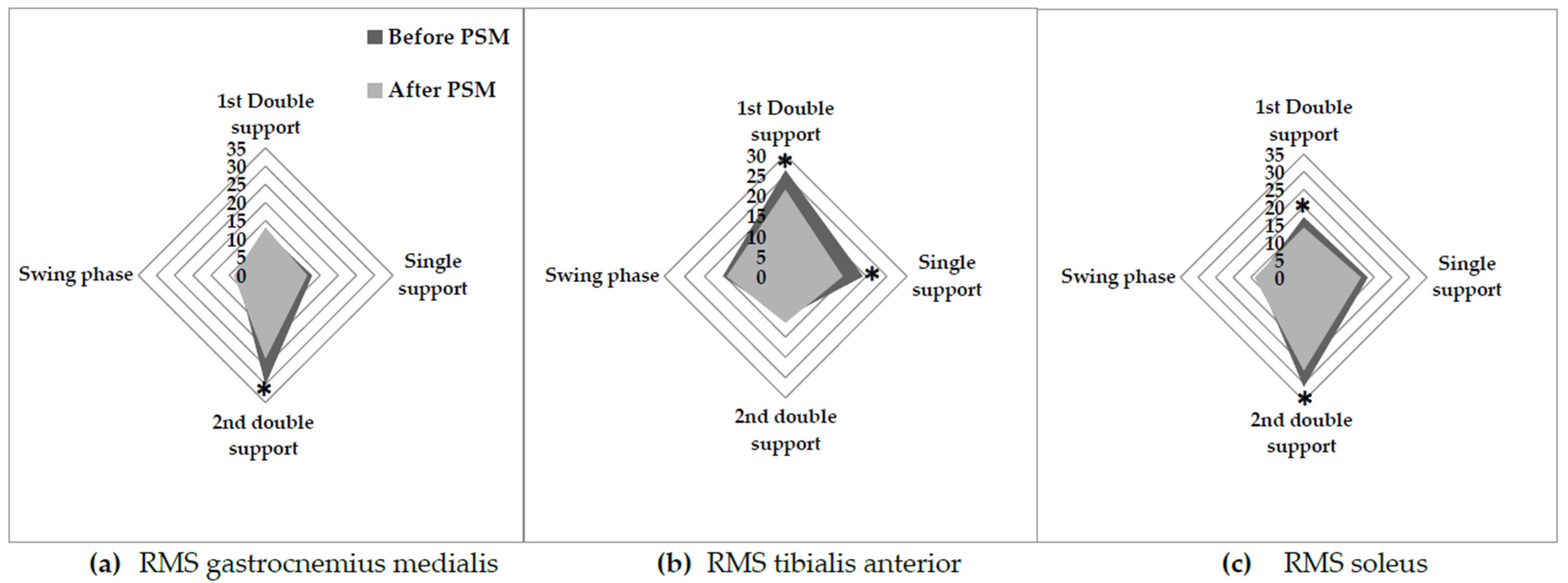
2.4.4. Electromyography Test
2.5. Statistical Analysis
3. Results
3.1. Recruitment
3.2. Gait Parameters
3.3. EMG Muscle Activity
3.4. Pearson’s Correlation Analysis
4. Discussion
4.1. Effect of the PSM Program on Body Composition and Physical Performance
4.2. Effect of the PSM Program on Ankle Muscle Strength and Neuromuscular Strategies during Walking
4.3. Practical Recommendations
4.4. Limitations and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colleluori, G.; Villareal, D.T. Aging, Obesity, Sarcopenia and the Effect of Diet and Exercise Intervention. Exp. Gerontol. 2021, 155, 111561. [Google Scholar] [CrossRef]
- Li, C.; Yu, K.; Shyh-Chang, N.; Jiang, Z.; Liu, T.; Ma, S.; Luo, L.; Guang, L.; Liang, K.; Ma, W.; et al. Pathogenesis of Sarcopenia and the Relationship with Fat Mass: Descriptive Review. J. Cachexia. Sarcopenia Muscle 2022, 13, 781–794. [Google Scholar] [CrossRef]
- Zamboni, M.; Rubele, S.; Rossi, A.P. Sarcopenia and Obesity. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Kopelman, P.G. Obesity as a Medical Problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A. Medical Consequences of Obesity. J. Clin. Endocrinol. Metab. 2004, 89, 2583–2589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, C.D.; Chen, H.C.; Liou, T.H.; Lin, C.L.; Huang, S.W. Impact of Sarcopenia and Obesity on Gait Speed after Total Knee Replacement. J. Am. Med. Dir. Assoc. 2022, 23, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Huang, S.W.; Huang, Y.Y.; Lin, C.L. Effects of Sarcopenic Obesity and Its Confounders on Knee Range of Motion Outcome after Total Knee Replacement in Older Adults with Knee Osteoarthritis: A Retrospective Study. Nutrients 2021, 13, 3817. [Google Scholar] [CrossRef] [PubMed]
- Kalinkovich, A.; Livshits, G. Sarcopenic Obesity or Obese Sarcopenia: A Cross Talk between Age-Associated Adipose Tissue and Skeletal Muscle Inflammation as a Main Mechanism of the Pathogenesis. Ageing Res. Rev. 2017, 35, 200–221. [Google Scholar] [CrossRef]
- Bilski, J.; Pierzchalski, P.; Szczepanik, M.; Bonior, J.; Zoladz, J.A. Multifactorial Mechanism of Sarcopenia and Sarcopenic Obesity. Role of Physical Exercise, Microbiota and Myokines. Cells 2022, 11, 160. [Google Scholar] [CrossRef]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The Biomechanics of Restricted Movement in Adult Obesity. Obes. Rev. 2006, 7, 13–24. [Google Scholar] [CrossRef]
- Frontera, W.R. Physiologic Changes of the Musculoskeletal System with Aging: A Brief Review. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Ortega, J.D.; Farley, C.T. Effects of Aging on Mechanical Efficiency and Muscle Activation during Level and Uphill Walking. J. Electromyogr. Kinesiol. 2015, 25, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frimenko, R.; Goodyear, C.; Bruening, D. Interactions of Sex and Aging on Spatiotemporal Metrics in Non-Pathological Gait: A Descriptive Meta-Analysis. Physiotherapy 2015, 101, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Doherty, T.J. Invited Review: Aging and Sarcopenia. J. Appl. Physiol. 2003, 95, 1717–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, C.; O’ Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of Physical Inactivity in Older Adults: A Systematic Review of Reviews and Meta-Analyses. Scand. J. Med. Sci. Sport. 2020, 30, 816–827. [Google Scholar] [CrossRef]
- Van den Beld, A.W.; Kaufman, J.M.; Zillikens, M.C.; Lamberts, S.W.J.; Egan, J.M.; van der Lely, A.J. The Physiology of Endocrine Systems with Ageing. Lancet Diabetes Endocrinol. 2018, 6, 647–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campisi, J.; Kapahi, P.; Lithgow, G.J.; Melov, S.; Newman, J.C.; Verdin, E. From Discoveries in Ageing Research to Therapeutics for Healthy Ageing. Nature 2020, 571, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Norman, K.; Haß, U.; Pirlich, M. Malnutrition in Older Adults-Recent Advances and Remaining Challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef]
- Tezuka, T.; Inoue, A.; Hoshi, T.; Weatherbee, S.D.; Burgess, R.W.; Ueta, R.; Yamanashi, Y. The MuSK Activator Agrin Has a Separate Role Essential for Postnatal Maintenance of Neuromuscular Synapses. Proc. Natl. Acad. Sci. USA 2014, 111, 16556–16561. [Google Scholar] [CrossRef]
- Li, L.; Xiong, W.C.; Mei, L. Neuromuscular Junction Formation, Aging, and Disorders. Annu. Rev. Physiol. 2018, 80, 159–188. [Google Scholar] [CrossRef]
- Beck Jepsen, D.; Robinson, K.; Ogliari, G.; Montero-Odasso, M.; Kamkar, N.; Ryg, J.; Freiberger, E.; Tahir, M. Predicting Falls in Older Adults: An Umbrella Review of Instruments Assessing Gait, Balance, and Functional Mobility. BMC Geriatr. 2022, 22, 615. [Google Scholar] [CrossRef]
- Chen, S.H.; Chou, L.S. Gait Balance Control after Fatigue: Effects of Age and Cognitive Demand. Gait Posture 2022, 95, 129–134. [Google Scholar] [CrossRef]
- Macie, A.; Matson, T.; Schinkel-Ivy, A. Age Affects the Relationships between Kinematics and Postural Stability during Gait. Gait Posture 2023, 102, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.D.M.; Gouveia, É.R.; Gouveia, B.R.; Marques, A.; Martins, F.; Przednowek, K.; França, C.; Peralta, M.; Ihle, A. Associations of Gait Speed, Cadence, Gait Stability Ratio, and Body Balance with Falls in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 13926. [Google Scholar] [CrossRef]
- Kim, D.; Lewis, C.L.; Gill, S.V. The Effect of Obesity on Whole-Body Angular Momentum during Steady-State Walking. Gait Posture 2022, 94, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Capodaglio, P.; Gobbi, M.; Donno, L.; Fumagalli, A.; Buratto, C.; Galli, M.; Cimolin, V. Effect of Obesity on Knee and Ankle Biomechanics during Walking. Sensors 2021, 21, 7114. [Google Scholar] [CrossRef]
- Deforche, B.I.; Hills, A.P.; Worringham, C.J.; Davies, P.S.W.; Murphy, A.J.; Bouckaert, J.J.; De Bourdeaudhuij, I.M. Balance and Postural Skills in Normal-Weight and Overweight Prepubertal Boys. Int. J. Pediatr. Obes. 2009, 4, 175–182. [Google Scholar] [CrossRef]
- Hue, O.; Simoneau, M.; Marcotte, J.; Berrigan, F.; Doré, J.; Marceau, P.; Marceau, S.; Tremblay, A.; Teasdale, N. Body Weight Is a Strong Predictor of Postural Stability. Gait Posture 2007, 26, 32–38. [Google Scholar] [CrossRef]
- Berrigan, F.; Simoneau, M.; Tremblay, A.; Hue, O.; Teasdale, N. Influence of Obesity on Accurate and Rapid Arm Movement Performed from a Standing Posture. Int. J. Obes. 2006, 30, 1750–1757. [Google Scholar] [CrossRef] [Green Version]
- Vankrunkelsven, W.; Derde, S.; Gunst, J.; Vander Perre, S.; Declerck, E.; Pauwels, L.; Derese, I.; Van den Berghe, G.; Langouche, L. Obesity Attenuates Inflammation, Protein Catabolism, Dyslipidaemia, and Muscle Weakness during Sepsis, Independent of Leptin. J. Cachexia. Sarcopenia Muscle 2022, 13, 418–433. [Google Scholar] [CrossRef]
- Pérez-Torres, I.; Castrejón-Téllez, V.; Soto, M.E.; Rubio-Ruiz, M.E.; Manzano-Pech, L.; Guarner-Lans, V. Oxidative Stress, Plant Natural Antioxidants, and Obesity. Int. J. Mol. Sci. 2021, 22, 1786. [Google Scholar] [CrossRef] [PubMed]
- Al-Sulaiti, H.; Diboun, I.; Agha, M.V.; Mohamed, F.F.S.; Atkin, S.; Dömling, A.S.; Elrayess, M.A.; Mazloum, N.A. Metabolic Signature of Obesity-Associated Insulin Resistance and Type 2 Diabetes. J. Transl. Med. 2019, 17, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, I.M.; Perrard, X.Y.D.; Brunner, G.; Lui, H.; Sparks, L.M.; Smith, S.R.; Wang, X.; Shi, Z.Z.; Lewis, D.E.; Wu, H.; et al. Intermuscular and Perimuscular Fat Expansion in Obesity Correlates with Skeletal Muscle T Cell and Macrophage Infiltration and Insulin Resistance. Int. J. Obes. 2015, 39, 1607–1618. [Google Scholar] [CrossRef] [PubMed]
- Maktouf, W.; Durand, S.; Boyas, S.; Pouliquen, C.; Beaune, B. Interactions among Obesity and Age-Related Effects on the Gait Pattern and Muscle Activity across the Ankle Joint. Exp. Gerontol. 2020, 140, 111054. [Google Scholar] [CrossRef]
- De Oliveira Máximo, R.; De Oliveira, D.C.; Ramírez, P.C.; Luiz, M.M.; De Souza, A.F.; Delinocente, M.L.B.; Steptoe, A.; De Oliveira, C.; Da Silva Alexandre, T. Dynapenia, Abdominal Obesity or Both: Which Accelerates the Gait Speed Decline Most? Age Ageing 2021, 50, 1616–1625. [Google Scholar] [CrossRef]
- Yang, M.; Jiang, J.; Hao, Q.; Luo, L.; Dong, B. Dynapenic Obesity and Lower Extremity Function in Elderly Adults. J. Am. Med. Dir. Assoc. 2015, 16, 31–36. [Google Scholar] [CrossRef]
- Meng, H.; Gorniak, S.L. Obesity Is Associated With Gait Alterations and Gait Asymmetry in Older Adults. Mot. Control 2022, 27, 6–19. [Google Scholar] [CrossRef]
- Maktouf, W.; Durand, S.; Boyas, S.; Pouliquen, C.; Beaune, B. Combined Effects of Aging and Obesity on Postural Control, Muscle Activity and Maximal Voluntary Force of Muscles Mobilizing Ankle Joint. J. Biomech. 2018, 79, 198–206. [Google Scholar] [CrossRef]
- Melzer, I.; Oddsson, L.I.E. Altered Characteristics of Balance Control in Obese Older Adults. Obes. Res. Clin. Pract. 2016, 10, 151–158. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Agosti, F.; Proietti, M.; Riva, D.; Resnik, M.; Lafortuna, C.L.; Sartorio, A. Postural Instability of Extremely Obese Individuals Improves after a Body Weight Reduction Program Entailing Specific Balance Training. J. Endocrinol. Investig. 2005, 28, 2–7. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Bueno-Notivol, J.; Martínez-Amat, A.; Cruz-Díaz, D.; Hernandez, A.V.; Pérez-López, F.R. Effect of Exercise Alone or Combined with Dietary Supplements on Anthropometric and Physical Performance Measures in Community-Dwelling Elderly People with Sarcopenic Obesity: A Meta-Analysis of Randomized Controlled Trials. Maturitas 2018, 116, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, K.J.; Liao, C.D.; Tsai, M.W.; Chen, C.N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theodorakopoulos, C.; Jones, J.; Bannerman, E.; Greig, C.A. Effectiveness of Nutritional and Exercise Interventions to Improve Body Composition and Muscle Strength or Function in Sarcopenic Obese Older Adults: A Systematic Review. Nutr. Res. 2017, 43, 3–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maktouf, W.; Durand, S.; Beaune, B.; Boyas, S. Influence of Obesity and Impact of a Physical Activity Program on Postural Control and Functional and Physical Capacities in Institutionalized Older Adults: A Pilot Study. J. Phys. Act. Health 2019, 17, 169–176. [Google Scholar] [CrossRef]
- Chiu, S.C.; Yang, R.S.R.J.; Yang, R.S.R.J.; Chang, S.F.; Kim, H.; Kim, M.; Kojima, N.; Fujino, K.; Hosoi, E.; Kobayashi, H.; et al. Effects of Resistance Training on Body Composition and Functional Capacity among Sarcopenic Obese Residents in Long-Term Care Facilities: A Preliminary Study. BMC Geriatr. 2018, 18, 21. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Kwon, Y.; Park, H. Effects of 24-Week Aerobic and Resistance Training on Carotid Artery Intima-Media Thickness and Flow Velocity in Elderly Women with Sarcopenic Obesity. J. Atheroscler. Thromb. 2017, 24, 1117–1124. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.-Z.; Guo, Y.-B.; Lou, J.-H. Effects of Home Exercise on Sarcopenia Obesity for Aging People. Chin. J. Rehabil. Theory Pract. 2019, 12, 90–96. [Google Scholar] [CrossRef]
- Liao, C.-D.; Tsauo, J.-Y.; Lin, L.-F.; Huang, S.-W.; Ku, J.-W.; Chou, L.-C.; Liou, T.-H. Effects of Elastic Resistance Exercise on Body Composition and Physical Capacity in Older Women with Sarcopenic Obesity. Medicine 2017, 96, e7115. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Barbour, V.; Macdonald, H. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. Bmj 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. Ann. Intern. Med. 2010, 152, 26–32. [Google Scholar]
- Zulfiqar, A.-A.; Habchi, H.; Habchi, P.; Dembele, I.A.; Andres, E. Physical Activity in the Elderly and Frailty Syndrome: A Retrospective Study in Primary Care. Medicines 2022, 9, 51. [Google Scholar] [CrossRef]
- Smith, T.; Gildeh, N.; Holmes, C. The Montreal Cognitive Assessment: Validity and Utility in a Memory Clinic Setting. Can. J. Psychiatry 2007, 52, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [PubMed]
- Foster, C. Monitoring Training in Athletes with Reference to Overtraining Syndrome. Med. Sci. Sports Exerc. 1998, 30, 1164–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gartner, A.; Dioum, A.; Delpeuch, F.; Maire, B.; Schutz, Y. Use of Hand-to-Hand Impedancemetry to Predict Body Composition of African Women as Measured by Air Displacement Plethysmography. Eur. J. Clin. Nutr. 2004, 58, 523–531. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.D.; Quach, B.; Chung, P.K. Understanding of The Senior Fitness Test: Evidence From Community-Dwelling High Function Older Adults in Hong Kong. Arch. Gerontol. Geriatr. 2019, 82, 186–292. [Google Scholar] [CrossRef]
- Nagai, K.; Yamada, M.; Mori, S.; Tanaka, B.; Uemura, K.; Aoyama, T.; Ichihashi, N.; Tsuboyama, T. Effect of the Muscle Coactivation during Quiet Standing on Dynamic Postural Control in Older Adults. Arch. Gerontol. Geriatr. 2013, 56, 129–133. [Google Scholar] [CrossRef]
- De Luca, C.J.; Gilmore, L.D.; Kuznetsov, M.; Roy, S.H. Filtering the Surface EMG Signal: Movement Artifact and Baseline Noise Contamination. J. Biomchanics 2010, 43, 1573–1579. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disstelhorst-Klug, C.; Rau, G. Development of Recommendations for SEMG Sensors and Sensor. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Kim, H.; Kim, M.; Kojima, N.; Fujino, K.; Hosoi, E.; Kobayashi, H.; Somekawa, S.; Niki, Y.; Yamashiro, Y.; Yoshida, H. Exercise and Nutritional Supplementation on Community-Dwelling Elderly Japanese Women With Sarcopenic Obesity: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2016, 17, 1011–1019. [Google Scholar] [CrossRef]
- Lee, Y.H.; Lee, P.H.; Lin, L.F.; Liao, C.D.; Liou, T.H.; Huang, S.W. Effects of Progressive Elastic Band Resistance Exercise for Aged Osteosarcopenic Adiposity Women. Exp. Gerontol. 2021, 147, 111272. [Google Scholar] [CrossRef] [PubMed]
- Jung, U.J. Sarcopenic Obesity: Involvement of Oxidative Stress and Beneficial Role of Antioxidant Flavonoids. Antioxidants 2023, 12, 1063. [Google Scholar] [CrossRef] [PubMed]
- Nygren, J.; Nair, K.S. Differential Regulation of Protein Dynamics in Splanchnic and Skeletal Muscle Beds by Insulin and Amino Acids in Healthy Human Subjects. Diabetes 2003, 52, 1377–1385. [Google Scholar] [CrossRef] [Green Version]
- Moller-Loswick, A.C.; Zachrisson, H.; Hyltander, A.; Korner, U.; Matthews, D.E.; Lundholm, K. Insulin Selectively Attenuates Breakdown of Nonmyofibrillar Proteins in Peripheral Tissues of Normal Men. Am. J. Physiol. 1994, 266, E645–E652. [Google Scholar] [CrossRef] [PubMed]
- Wijesinghe, S.N.; Nicholson, T.; Tsintzas, K.; Jones, S.W. Involvements of Long Noncoding RNAs in Obesity-Associated Inflammatory Diseases. Obes. Rev. 2021, 22, e13156. [Google Scholar] [CrossRef]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodriguez-Mañas, L.; Izquierdo, M. Multicomponent Exercises Including Muscle Power Training Enhance Muscle Mass, Power Output, and Functional Outcomes in Institutionalized Frail Nonagenarians. Age 2014, 36, 773–785. [Google Scholar] [CrossRef] [Green Version]
- Rossi-Izquierdo, M.; Santos-Pérez, S.; Faraldo-García, A.; Vaamonde-Sánchez-Andrade, I.; Gayoso-Diz, P.; Del-Río-Valeiras, M.; Lirola-Delgado, A.; Soto-Varela, A. Impact of Obesity in Elderly Patients with Postural Instability. Aging Clin. Exp. Res. 2015, 28, 423–428. [Google Scholar] [CrossRef]
- Blaszczyk, J.; Lowe, D.; Hansen, P. Ranges of Postural Stability and Their Changes in the Elderly. Gait Posture 1994, 2, 11–17. [Google Scholar] [CrossRef]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Van Hoecke, J.; Gremeaux, V.; Martin, A. Ankle Muscle Strength Discriminates Fallers from Non-Fallers. Front. Aging Neurosci. 2014, 6, 336. [Google Scholar] [CrossRef] [Green Version]
- Laroche, D.P.; Marques, N.R.; Shumila, H.N.; Logan, C.R.; Laurent, R.S.; Goncąlves, M. Excess Body Weight and Gait Influence Energy Cost of Walking in Older Adults. Med. Sci. Sports Exerc. 2015, 47, 1017–1025. [Google Scholar] [CrossRef] [Green Version]
- Peyrot, N.; Morin, J.B.; Thivel, D.; Isacco, L.; Taillardat, M.; Belli, A.; Duche, P. Mechanical Work and Metabolic Cost of Walking after Weight Loss in Obese Adolescents. Med. Sci. Sports Exerc. 2010, 42, 1914–1922. [Google Scholar] [CrossRef]
- Hortobágyi, T.; Devita, P. Muscle Pre- and Coactivity during Downward Stepping Are Associated with Leg Stiffness in Aging. J. Electromyogr. Kinesiol. 2000, 10, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Nene, A.; Mayagoitia, R.; Veltink, P. Assessment of Rectus Femoris Function during Initial Swing Phase. Gait Posture 1999, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Paróczai, R.; Bejek, Z.; Illyés, Á. Gait Parameters of Healthy, Elderly People. Phys. Educ. Sport 2006, 4, 49–58. [Google Scholar]
- Winter, D.A.; Patla, A.E.; Frank, J.S.; Walt, S.E. Biomechanical Walking Pattern Changes in the Fit and Healthy Elderly. Phys. Ther. 1990, 70, 340–347. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CG | TG | p | CG | TG | p | |
|---|---|---|---|---|---|---|
| At the Baseline | After the Intervention | |||||
| Characteristics | Anthropometric parameters | |||||
| Age (years) | 76.6 ± 5.6 | 74.1 ± 3.7 | NS | 77.1 ± 5.6 | 74.6 ± 3.7 | NS |
| Body height (cm) | 160.3 ± 4.5 | 164.5 ± 5.5 | NS | 160.3 ± 4.5 | 164.5 ± 5.5 | NS |
| Body mass (kg) | 91.7 ± 6.7 | 95.9 ± 4.3 | NS | 93.7 ± 5.7 | 88.7 ± 5.7 | NS |
| BMI (kg/m2) | 35.8 ± 2.7 | 35.8 ± 2.1 | NS | 36.6 ± 2.7 | 34.6 ± 2.7 | NS |
| Body fat (%) | 42.1 ± 4.5 | 43.0 ± 3.5 | NS | 44.3 ± 7.5 | 34.2 ± 2.5 * | p < 0.05 |
| FBM (kg) | 38.6 ± 3.8 | 41.2 ± 3.3 | NS | 41.6 ± 3.8 | 30.3 ± 4.1 * | p < 0.05 |
| LBM (kg) | 53.1 ± 4.4 | 54.7 ± 5.4 | NS | 52.1 ± 4.4 | 58.4 ± 4.4 * | p < 0.05 |
| Hip circumference (cm) | 96.8 ± 6.8 | 96.8 ± 6.8 | NS | 96.8 ± 6.4 | 94.8 ± 2.8 | NS |
| Waist circumference (cm) | 99.8 ± 5.1 | 99.8 ± 6.1 | NS | 99.8 ± 5.1 | 97.8 ± 4.1 | NS |
| Handgrip force (N) | 13.5 ± 3.1 | 12.9 ± 2.4 | NS | 13.1 ± 2.9 | 14.1 ± 3.2 * | p < 0.05 |
| Maximal gait speed (m/s) | 0.7 ± 0.2 | 0.7 ± 0.2 | NS | 0.8 ± 0.2 | 1.2 ± 0.3 * | p < 0.05 |
| Tests | Senior fitness test | |||||
| 30 s—Arm flexion (n) | 18.2 ± 3.9 | 17.3 ± 3.9 | NS | 19.2 ± 4.9 | 23.5 ±5.4 * | p < 0.05 |
| 30 s—Sit to stand (n) | 10.1 ± 3.3 | 11.1 ± 3.3 | NS | 9.4 ± 2.3 | 14.7 ± 3.5 * | p < 0.05 |
| Trunk flexibility (cm) | 12.4 ± 9.9 | 11.4 ± 7.8 | NS | 11.4 ± 7.9 | 7.0 ± 5.4 | NS |
| Walking back and forth (s) | 21.1 ± 3.9 | 20.5 ± 3.9 | NS | 20.1 ± 4.9 | 14.2 ± 4.5 * | p < 0.05 |
| Upper body flexibility (cm) | 26.4 ± 8.1 | 27.4 ± 7.9 | NS | 26.1 ± 8.7 | 22.0 ± 9.8 * | p < 0.05 |
| 2 min—Walk (m) | 72.3 ± 20.1 | 75.5 ± 21.4 | NS | 72.3 ± 19.5 | 131.0 ± 45.2 * | p < 0.05 |
| 2 min—Knee lifts (n) | 82.4 ± 55.5 | 86.5 ± 56.3 | NS | 77.4 ± 47.5 | 121.4 ± 62.1 * | p < 0.05 |
| Tests | Before PSM | After PSM | Ϫ (%) | p |
|---|---|---|---|---|
| 30 s—Arm flexion (n) | 17.3 ± 3.9 | 23.5 ± 5.4 * | +29.1 | p < 0.01 |
| 30 s—Sit to stand (n) | 11.1 ± 3.3 | 14.7 ± 3.5 * | +45.5 | p < 0.001 |
| Trunk flexibility (cm) | 11.4 ± 7.8 | 7.0 ± 5.4 | −32.7 | NS |
| Walking back and forth (s) | 20.5 ± 3.9 | 14.2 ± 4.5 * | −16.0 | p < 0.001 |
| Upper body flexibility (cm) | 27.4 ± 7.9 | 22.0 ± 9.8 * | −12.4 | p < 0.05 |
| 2 min—Walk (m) | 75.5 ± 21.4 | 131.0 ± 45.2 * | +81.2 | p < 0.001 |
| 2 min—Knee lifts (n) | 86.5 ± 56.3 | 121.4 ± 62.1 * | +47.3 | p < 0.001 |
| TG | ||||
|---|---|---|---|---|
| Gait Parameters | Before PSM | After PSM | Ϫ (%) | p |
| Preferred gait speed (m/s) | 14.2 ± 4.5 * | 1.0 ± 0.2 * | +66 | p < 0.001 |
| Step length (cm) | 14.2 ± 4.5 * | 33.1 ± 4.2 * | +38 | p < 0.01 |
| Walking cycle | ||||
| Support phase (%) Left | 78.3 ± 2.8 | 73.3 ± 1.8 * | −5.0 | p < 0.05 |
| Support phase (%) Right | 77.5 ± 3.8 | 72.5 ± 2.8 * | −5.0 | p < 0.05 |
| 1st double support (%) Left | 26.5 ± 5.2 | 26.8 ± 2.2 * | −4.1 | p < 0.05 |
| 1st double support (%) Right | 25.3 ± 4.0 | 21.3 ± 2.0 * | −4.0 | p < 0.05 |
| Single support (%) Left | 24.8 ± 5.9 | 26.8 ± 2.9 | - | - |
| Single support (%) Right | 25.4 ± 6.1 | 27.3 ± 3.1 | - | - |
| 2nd double support (%) Left | 27.0 ± 3.1 | 24.0 ± 2.1 * | −3.0 | p < 0.05 |
| 2nd double support (%) Right | 26.9 ± 3.7 | 23.9 ± 2.7 * | −3.0 | p < 0.05 |
| Swing phase (%) Left | 21.8 ± 2.8 | 26.7 ± 1.9 * | +4.9 | p < 0.05 |
| Swing phase (%) Right | 22.5 ± 3.8 | 27.5 ± 2.8 * | +5.0 | p < 0.05 |
| CoP parameters | ||||
| Maximal speed (cm/s) | 158.5 ± 26.5 | 117.7 ± 21.4 * | −26.0 | p < 0.01 |
| GRFv parameters | ||||
| Relative P1 (N/kg) Left | 9.4 ± 1.5 | 10.9 ± 1.6 * | +16.0 | p < 0.05 |
| Relative P1 (N/kg) Right | 9.5 ± 1.4 | 10.8 ± 1.2 * | +14.0 | p < 0.05 |
| Relative P2 (N/kg) Left | 9.3 ± 1.2 | 11.5 ± 1.8 * | +24.0 | p < 0.05 |
| Relative P2 (N/kg) Right | 9.0 ± 1.5 | 11.8 ± 1.9 * | +31.0 | p < 0.05 |
| Maximal Voluntary Contraction | Muscle Activity | Body Composition | |||||
|---|---|---|---|---|---|---|---|
| Gait Parameters | Ϫ Absolute PF Force | Ϫ Absolute DF Force | Ϫ RMS GM | Ϫ RMS SOL | Ϫ RMS TA | Ϫ LBM | Ϫ FM |
| Ϫ Maximal gait speed | 0.23 | 0.25 | 0.21 | 0.24 | 0.24 | 0.11 | 0.25 |
| Ϫ Step length | 0.36 | 0.29 | 0.13 | 0.27 | 0.28 | 0.15 | 0.19 |
| Ϫ CoP velocity | 0.61 * | 0.63 * | 0.17 | 0.57 * | 0.54 * | 0.11 | 0.09 |
| Ϫ Relative P1 | 0.11 | 0.74 * | 0.15 | 0.14 | 0.19 | 0.25 | 0.33 |
| Ϫ Relative P2 | 0.76 * | 0.13 | 0.21 | 0.27 | 0.12 | 0.17 | 0.21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferhi, H.; Gaied Chortane, S.; Durand, S.; Beaune, B.; Boyas, S.; Maktouf, W. Effects of Physical Activity Program on Body Composition, Physical Performance, and Neuromuscular Strategies during Walking in Older Adults with Sarcopenic Obesity: Randomized Controlled Trial. Healthcare 2023, 11, 2294. https://doi.org/10.3390/healthcare11162294
Ferhi H, Gaied Chortane S, Durand S, Beaune B, Boyas S, Maktouf W. Effects of Physical Activity Program on Body Composition, Physical Performance, and Neuromuscular Strategies during Walking in Older Adults with Sarcopenic Obesity: Randomized Controlled Trial. Healthcare. 2023; 11(16):2294. https://doi.org/10.3390/healthcare11162294
Chicago/Turabian StyleFerhi, Hamza, Sabri Gaied Chortane, Sylvain Durand, Bruno Beaune, Sébastien Boyas, and Wael Maktouf. 2023. "Effects of Physical Activity Program on Body Composition, Physical Performance, and Neuromuscular Strategies during Walking in Older Adults with Sarcopenic Obesity: Randomized Controlled Trial" Healthcare 11, no. 16: 2294. https://doi.org/10.3390/healthcare11162294