
Interviews with HIV Experts for Development of a Mobile Health Application in HIV Care—A Qualitative Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
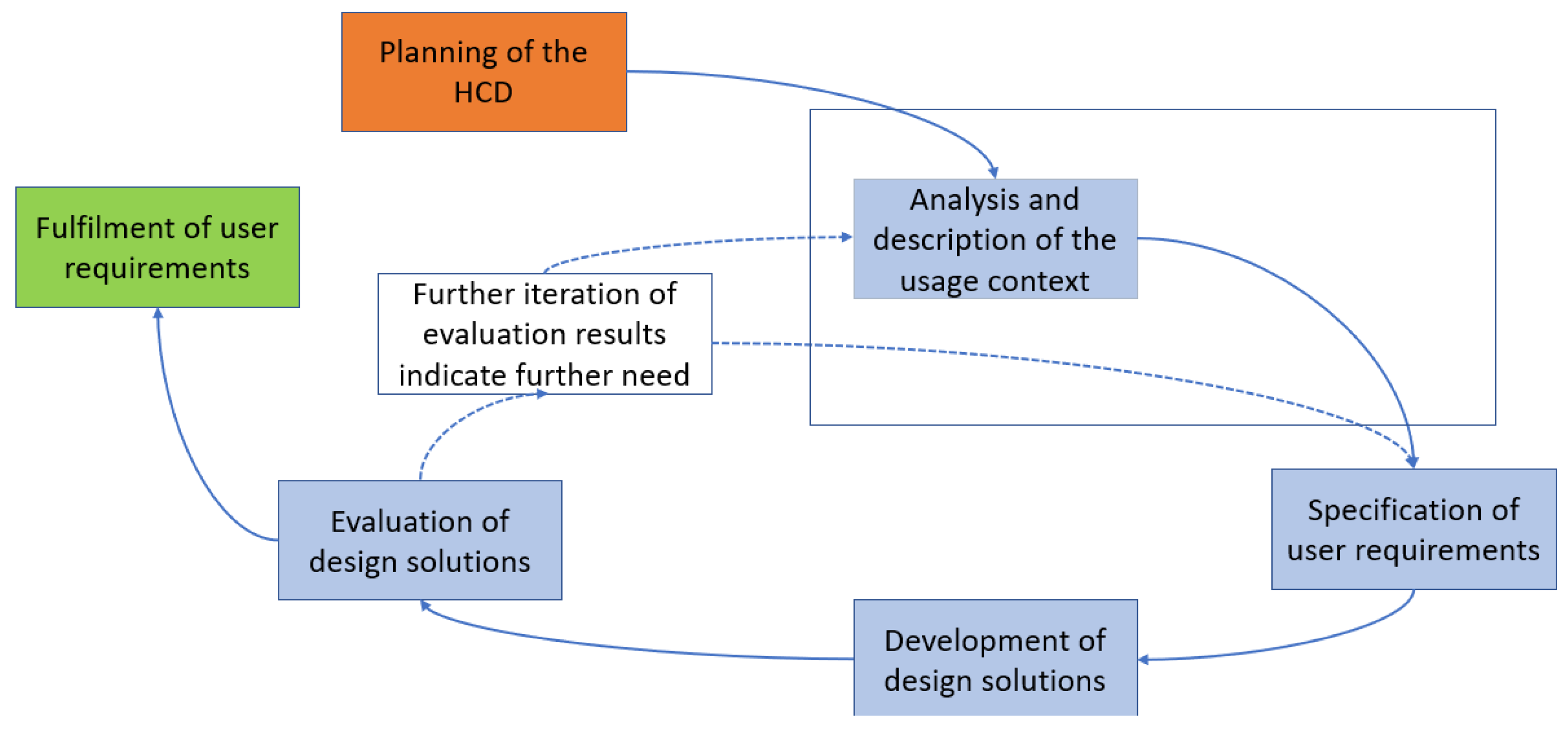
2.1. Design
- Socio-demographic characteristics: Age, gender, and other socio-demographics.
- Task-related characteristics: Tasks, as well as knowledge, skills, resources, and motivation to perform tasks with the planned system.
- Organizational characteristics: Current organizational aspects, reliability, skills, and willingness for change.
- Psychological and social characteristics: Cognitive skills, cultural background, language, and literacy.
- Physical and sensory characteristics: Physical and sensory condition of the users.
- The extracted usage context information was applied to construct task models that the app should contain and that form the basis for the app functionalities. A task model includes both tasks and related subtasks. It is used to clarify which tasks are to be performed with the app and to understand which paths the user chooses when performing the task and allows for designing a system that is suitable for the application [33].
2.2. Setting and Sampling
2.3. Data Collection
- Current care workflow: Organization of patient care of LPs and PrEP users and current form of communication with the patients.
- App functionalities and possible benefits for LPs and PrEP users.
- Further app functionalities: Additional information or medical findings whose entry in the app could have special significance for physicians or patients.
- Problems/disadvantages: Any possible negative impact of the planned app on patient care.
- Benefits for HIV experts: Possible incentive that the app offers for the physicians providing care.
- Possible adaptation of the clinical workflow: Adaptation of typical clinical processes in everyday medical practice using the app.
2.4. Data Analysis and Processing
3. Results
3.1. Interviews
3.1.1. Participants
3.1.2. Main Themes by Category
Current Care Workflow
LPs are often individuals who go from one doctor to another for months/years without an HIV diagnosis and have repeated HIV indicator diseases that are not detected, such as recurrent herpes zoster, recurrent infections, B-symptomatology, and lymph node swelling, and who are not offered HIV diagnostics.(P1)
Some patients have the participant’s phone number and send photos of problems without restraint—bad in terms of privacy.(P13)
App Functionalities and Possible Benefits for PrEP Users and LPs
A telemedical app is conceivable for well-established/admitted HIV patients with a viral load below the detection limit. However, this requires good mutual knowledge and enables communication based on the available information.(P17)
For PrEP users who are afraid of contracting HIV disease or other diseases. And because there are often side effects of the prescribed pills at the beginning of therapy, but they stop after a few months.(P18)
For new HIV disease, fever, lymph node swelling, general feeling of illness would be characteristic.(P22)
Alarm symptoms: Fever, rash, visual disturbances, shortness of breath, chest pain, bleeding signs, opportunistic, and non-opportunistic.(P25)
Classic symptoms that can mask depression include: loss of libido, loss of drive, sleep disturbance, headaches, and the whole psychosomatic range that indicates depression/anxiety.(P31)
Further App Functionalities
For PrEP, as needed and daily: document and to determine compliance, i.e., review/show tablet use, as this is where errors often occur […].(P38)
Problems/Disadvantages
The age group of HIV patients is able to use a smartphone (tends to be younger), no restrictions for specific subgroups […](P43)
PrEP users: especially good, mostly younger, tech-savvy—mostly (high) school graduates, grasp it better.(P44)
A multilingual app is very important; the app should include a translation feature that facilitates communication and can translate what the patient is talking about live and play back the translation on the screen.(P46)
Benefits for HIV Experts
Ability to communicate with patients when they are not on site and discuss how the year was progressing for them. This would have helped a lot during the COVID period, as some patients came out of fear.(P48)
Possible Adaptation of the Clinical Workflow
Free up time to maintain the app—1–2 h/week.(P52)
3.2. User Group Profiles
3.2.1. Late Presenters
3.2.2. PrEP Users
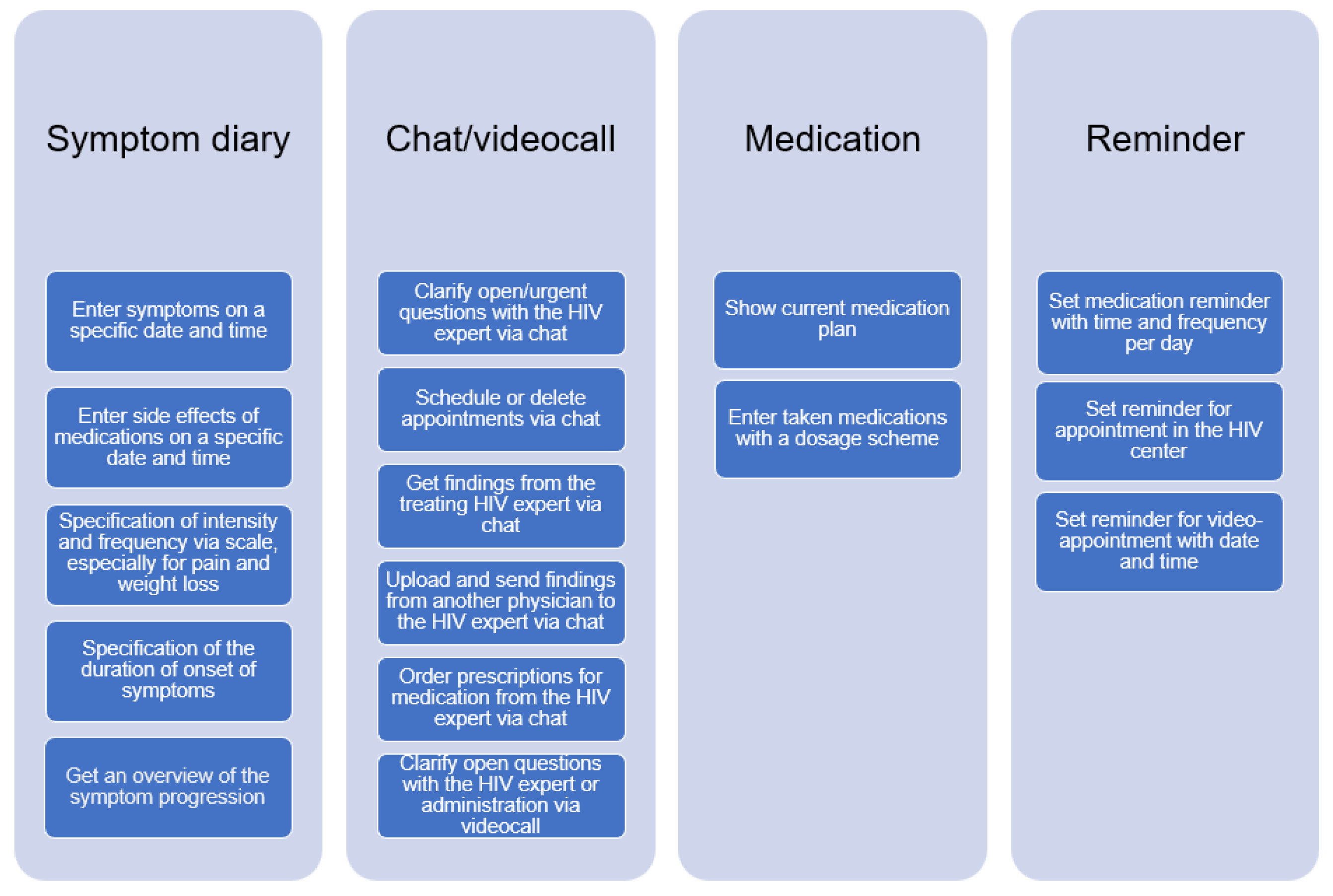
3.3. Tasks
4. Discussion
4.1. Discussion of Results
4.1.1. Organizational Conditions
4.1.2. App Functionalities
4.2. Discussion of Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vaillant, J.; Gulick, P.G. HIV Disease Current Practice. StatPearls 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK534860/ (accessed on 20 July 2023).
- Deeks, S.G.; Overbaug, J.; Phillips, A.; Buchbinder, S. HIV infection. Nat. Rev. Dis. Primers 2015, 1, 15035. [Google Scholar] [CrossRef] [PubMed]
- HIV/AIDS in Deutschland–Eckdaten der Schätzung. Available online: https://www.rki.de/DE/Content/InfAZ/H/HIVAIDS/Eckdaten/EckdatenDeutschland.pdf?__blob=publicationFile (accessed on 20 June 2023).
- Antinori, A.; Coenen, T.; Costagiola, D.; Dedes, N.; Ellefeson, M.; Gatell, J.; Girardi, E.; Johnson, M.; Kirk, O.; Lundgren, J.; et al. Late presentation of HIV infection: A consensus definition. HIV Med. 2011, 12, 61–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, U.; Schmidt, D.; Schink, S.B.; Koppe, U. Analysis of HIV pre-exposure prophylaxis (PrEP) needs and PrEP use in Germany among men who have sex with men. Z. Gesundh. Wiss. 2022, 12, 61–64. [Google Scholar] [CrossRef]
- Evaluation der Einführung der HIV-Präexpositionsprophylaxe als Leistung der Gesetzlichen Krankenversicherung (EvE-PrEP). Available online: https://www.rki.de/DE/Content/InfAZ/H/HIVAIDS/Abschlussbericht_EvE-PrEP.pdf?__blob=publicationFile (accessed on 20 June 2023).
- Henny, K.D.; Wilkes, A.L.; McDonald, C.M.; Denson, D.J.; Neumann, M.S. A Rapid Review of eHealth Interventions Addressing the Continuum of HIV Care (2007–2017). AIDS Behav. 2018, 22, 43–63. [Google Scholar] [CrossRef]
- Mehraeen, E.; Seyed, A.S.; Pashaei, Z.; Mirzapour, P.; Barzegary, A.; Vahedi, F.; Quaderi, K.; Tantiyor, M.M.; Nazeri, Z.; Karimi, A.; et al. Mobile applications in HIV self-management: A systematic review of scientific literature. AIDS Rev. 2022, 24, 24–31. [Google Scholar] [CrossRef]
- Ramsey, S.; Ames, E.; Uber, J.; Habib, S.; Clark, S. A Mobile Health App to Improve HIV Medication Adherence: Protocol for a Pilot Randomized Controlled Trial. JMIR Res. Protoc. 2019, 8, e15356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhns, L.M.; Hereth, J.; Garofalo, R.; Hidalgo, M.; Johnson, A.K.; Schnall, R.; Reisner, S.L.; Belzer, M.; Mimiaga, M.J. A Uniquely Targeted, Mobile App-Based HIV Prevention Intervention for Young Transgender Women: Adaptation and Usability Study. J. Med. Internet Res. 2021, 23, e21839. [Google Scholar] [CrossRef] [PubMed]
- Balán, I.C.; Lopez-Rios, J.; Nayak, S. SMARTtest: A Smartphone App to Facilitate HIV and Syphilis Self- and Partner-Testing, Interpretation of Results, and Linkage to Care. AIDS Behav. 2020, 24, 1560–1573. [Google Scholar] [CrossRef]
- Rana, A.I.; van den Berg, J.J.; Lamy, E.; Beckwith, C.G. Using a Mobile Health Intervention to Support HIV Treatment Adherence and Retention Among Patients at Risk for Disengaging with Care. AIDS Patient Care STDS 2016, 30, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Qu, M.; Chen, B.; Li, C.; Fan, H.; Zhao, Y. Effectiveness of mHealth on Adherence to Antiretroviral Therapy in Patients Living With HIV: Meta-analysis of Randomized Controlled Trials. JMIR Mhealth Uhealth 2023, 11, e42799. [Google Scholar] [CrossRef]
- Prepared–Die App zur PrEP. Available online: https://www.prepared-app.de/ (accessed on 20 June 2023).
- Diagnose HIV–Wie Eine App Dabei Hilft, mit der Unheilbaren Immunschwäche Umzugehen. Available online: https://www.mytherapyapp.com/de/diagnose-hiv-wie-eine-apphilft-mit-der-immunschwaeche-umzugehen (accessed on 20 June 2023).
- LIFE4ME+ E-Health System for Those Living with HIV. Available online: https://hiex.ch/innovation-2019-8.html (accessed on 20 June 2023).
- Staras, S.; Tauscher, J.S.; Rich, N.; Samarah, E.; Thompson, L.A.; Vinson, M.M.; Muszynski, M.J.; Shenkman, E.A. Using a Clinical Workflow Analysis to Enhance eHealth Implementation Planning: Tutorial and Case Study. JMIR Mhealth Uhealth 2021, 9, e18534. [Google Scholar] [CrossRef]
- Gimbel, R.; Shi, L.; Williams, J.E. Enhancing mHealth Technology in the Patient-Centered Medical Home Environment to Activate Patients With Type 2 Diabetes: A Multisite Feasibility Study Protocol. JMIR Res. Protoc. 2017, 6, e38. [Google Scholar] [CrossRef]
- Braune, K.; Boss, K.; Schmidt-Herzel, J.; Gajewska, K.A.; Thieffry, A.; Schulze, L.; Posern, B.; Raile, K. Shaping Workflows in Digital and Remote Diabetes Care During the COVID-19 Pandemic via Service Design: Prospective, Longitudinal, Open-label Feasibility Trial. JMIR Mhealth Uhealth 2021, 9, e24374. [Google Scholar] [CrossRef]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR Mhealth Uhealth 2018, 6, e23. [Google Scholar] [CrossRef] [Green Version]
- Ndlovu, K.; Mars, M.; Scott, R.E. Interoperability frameworks linking mHealth applications to electronic record systems. BMC Health Serv. Res. 2021, 21, 459. [Google Scholar] [CrossRef]
- Lobach, D.F.; Aziz, B.; Nitu, K.; Heaney-Huls, K.; Chiao, A.B.; Rafter, T.; Lomotan, E.A.; Harrison, M.I.; Dymek, C.; Swiger, J.; et al. Integrating a Patient Engagement App into an Electronic Health Record-Enabled Workflow Using Interoperability Standards. Appl. Clin. Inform. 2022, 13, 1163–1171. [Google Scholar] [CrossRef]
- Kao, C.K.; Liebovitz, D.M. Consumer Mobile Health Apps: Current State, Barriers, and Future Directions. PM R 2017, 9, 106–115. [Google Scholar] [CrossRef]
- Zapata, B.C.; Fernández-Alemán, J.L.; Idri, A.; Toval, A. Empirical studies on usability of mHealth apps: A systematic literature review. J. Med. Syst. 2015, 39, 1. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, J.; Zhou, L.; Tian, J.; Chen, X.; Zhang, W.; Wang, H.; Zhou, W.; Gao, Y. Usability evaluation of mHealth apps for elderly individuals: A scoping review. BMC Med. Inform. Decis. Mak. 2022, 22, 317. [Google Scholar] [CrossRef]
- Goswami, R.; Garner, S.L.; George, C.E. Usability of an mHealth application in India for type 2 diabetes mellitus. Health Educ. J. 2023, 82, 108–116. [Google Scholar] [CrossRef]
- Manzano-Monfort, G.; Paluzie, G.; Díaz-Gegúndez, M.; Chabrera, C. Usability of a mobile application for health professionals in home care services: A user-centered approach. Sci. Rep. 2023, 13, 2607. [Google Scholar] [CrossRef]
- Raeesi, A.; Khajouei, R.; Ahmadian, L. Evaluating and rating HIV/AIDS mobile apps using the feature-based application rating method and mobile app rating scale. BMC Med. Inform. Decis. Mak. 2022, 22, 281. [Google Scholar] [CrossRef] [PubMed]
- Farao, J.; Malila, B.; Conrad, N.; Mutsvangwa, T.; Rangaka, M.X.; Douglas, T.S. A user-centred design framework for mHealth. PLoS ONE 2020, 15, e0237910. [Google Scholar] [CrossRef] [PubMed]
- Chandran, S.; Al-Sa’di, A.; Ahmad, E. Exploring User Centered Design in Healthcare: A Literature Review. In Proceedings of the 2020 4th International Symposium on Multidisciplinary Studies and Innovative Technologies (ISMSIT), Istanbul, Turkey, 22 October 2020. [Google Scholar]
- Kim, M.; Kim, Y.; Choi, M. Mobile health platform based on user-centered design to promote exercise for patients with peripheral artery disease. BMC Med. Inform. Decis. Mak. 2022, 22, 206. [Google Scholar] [CrossRef] [PubMed]
- Saparamadu, A.A.D.N.S.; Fernando, P.; Zeng, P.; Teo, H.; Goh, A.; Lee, J.M.Y.; Lam, C.W.L. User-Centered Design Process of an mHealth App for Health Professionals: Case Study. JMIR Mhealth Uhealth 2021, 9, e18079. [Google Scholar] [CrossRef] [PubMed]
- Geis, T.; Pohlkehn, K. Praxiswissen User-Requirements; Dpunkt.Verlag: Heidelberg, Germany, 2018. [Google Scholar]
- ISO 92421-210:2019. Ergonomics of Human-System Interaction-Part 210: Human Centered Design for Interactive Systems. Available online: https://www.iso.org/standard/77520.html (accessed on 31 July 2023).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- ISO/IEC 25063:2014 Systems and Software Engineering—Systems and Software Product Quality Requirements and Evaluation (SQuaRE)—Common Industry Format (CIF) for Usability: Context of Use Description. Available online: https://www.iso.org/standard/35789.html (accessed on 20 June 2023).
- Mays, N.; Pope, C. Rigour and qualitative research. BMJ 1995, 311, 109–112. [Google Scholar] [CrossRef]
- Caley, M.J.; O’Leary, R.A.; Fisher, R.; Low-Choy, S.; Johnson, S.; Mengersen, K. What is an expert? A systems perspective on expertise. Ecol. Evol. 2014, 4, 231–242. [Google Scholar] [CrossRef]
- Genov, A.; Keavney, M.; Zazelenchuk, T. Usability Testing with Real Data. J. Usability Stud. 2009, 4, 85–92. [Google Scholar]
- Why 5 Participants Are Okay in a Qualitative Study, but Not in a Quantitative One. Available online: https://www.nngroup.com/articles/5-test-users-qual-quant/ (accessed on 20 June 2023).
- Helfferich, C. Die Qualität Qualitativer Daten. Manual für die Durchführung Qualitativer Interviews, 2nd ed.; VS-Verlag: Hamburg, Germany, 2011. [Google Scholar]
- Qualitative Content Analysis—Theoretical Foundation, Basic Procedures and Software Solution. Available online: https://www.ssoar.info/ssoar/bitstream/handle/document/39517/ssoar-2014-mayring-Qualitative_content_analysis_theoretical_foundation.pdf (accessed on 20 June 2023).
- Kuckartz, U.; Dresing, T.; Raediker, S.; Stefer, C. Qualitative Evaluation: Der Einstieg in die Praxis, 4th ed; VS-Verlag: Hamburg, Germany, 2007. [Google Scholar]
- Kuckartz, U. Qualitative Text Analysis: A Systematic Approach. In Compendium for Early Career Researchers in Mathematics Education.; Kaiser, G., Presmeg, N., Eds.; Springer International Publishing: Basel, Switzerland; Cham, Switzerland, 2019; pp. 181–197. [Google Scholar]
- Destatis Sharp Rise in Labour Migration in 2022. Available online: https://www.destatis.de/EN/Themes/Society-Environment/Population/Migration-Integration/_node.html (accessed on 20 June 2023).
- Panayiotou, A.; Gardner, A.; Williams, S.; Zucchi, E.; Mascitti-Meuter, M.; Goh, A.M.; You, E.; Chong, T.W.; Logiudice, D.; Lin, X.; et al. Language Translation Apps in Health Care Settings: Expert Opinion. JMIR Mhealth Uhealth 2019, 7, e11316. [Google Scholar] [CrossRef] [PubMed]
- Oberhofer, E. Corona-Pandemie: Zahl der HIV-Late-Presenter deutlich gestiegen. MMW Fortschr. Med. 2022, 16, 20–21. [Google Scholar] [CrossRef]
- van Bremen, K.; Monin, M.; Schlabe, S.; Bischoff, J.; Rieke, G.J.; Schwarze-Zander, C.; Wasmuth, J.C.; Rockstroh, J.K.; Boesecke, C. Impact of COVID-19 on HIV late diagnosis in a specialized German centre. HIV Med. 2022, 23, 1209–1213. [Google Scholar] [CrossRef]
- Biello, K.B.; Daddario, S.R.; Hill-Rorie, J.; Futterman, D.; Sullivan, P.S.; Hightow-Weidman, L.; Jones, J.; Mimiaga, M.J.; Mayer, K.H. Uptake and Acceptability of MyChoices: Results of a Pilot RCT of a Mobile App Designed to Increase HIV Testing and PrEP Uptake Among Young American MSM. AIDS Behav. 2022, 26, 3981–3990. [Google Scholar] [CrossRef] [PubMed]
- Hoagland, B.; Torres, T.S.; Bezerra, D.R.B.; Benedetti, M.; Pimenta, C.; Veloso, V.G.; Grinsztejn, B. High acceptability of PrEP teleconsultation and HIV self-testing among PrEP users during the COVID-19 pandemic in Brazil. Braz. J. Infect. Dis. 2021, 25, 101037. [Google Scholar] [CrossRef]
- Brito-Mutunayagam, S.L.; Fernando, I. Security Concerns to Be Considered When Downloading Human Immunodeficiency Virus/Sexually Transmitted Disease Related Smartphone Applications. J. Med. Internet Res. 2013, 15, e222. [Google Scholar] [CrossRef]
- Shrestha, R.; Fisher, C.; Wickersham, J.A.; Khati, A.; Kim, R.; Azwa, I.; Mistler, C.; Goldsamt, L. Privacy and Confidentiality Concerns Related to the Use of mHealth Apps for HIV Prevention Efforts Among Malaysian Men Who Have Sex With Men: Cross-sectional Survey Study. JMIR Form. Res. 2021, 5, e28311. [Google Scholar] [CrossRef]
- Brennan, A.; Browne, J.P.; Horgan, M. A systematic review of health service interventions to improve linkage with or retention in HIV care. AIDS Care 2014, 26, 804–812. [Google Scholar] [CrossRef]
- Dillingham, R.; Ingersoll, K.; Flickinger, T.E.; Waldman, A.L.; Grabowski, M.; Laurence, C.; Wispelwey, E.; Reynolds, G.; Conaway, M.; Cohn, W.F. PositiveLinks: A Mobile Health Intervention for Retention in HIV Care and Clinical Outcomes with 12-Month Follow-Up. AIDS Patient Care STDS 2018, 32, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Shaw, R.; Stroo, M.; Fiander, C.; McMillan, K. Selecting Mobile Health Technologies for Electronic Health Record Integration: Case Study. J. Med. Internet Res. 2020, 22, e23314. [Google Scholar] [CrossRef]
- Joe, J.; Chaudhuri, S.; Le, T.; Thompson, H.; Demiris, G. The use of think-aloud and instant data analysis in evaluation research: Exemplar and lessons learned. J. Biomed. Inform. 2015, 56, 284–291. [Google Scholar] [CrossRef] [Green Version]
- Lantzsch, H.; Panteli, D.; Martino, F.; Stephani, V.; Seißler, D.; Püschel, C.; Knöppler, K.; Busse, R. Benefit Assessment and Reimbursement of Digital Health Applications: Concepts for Setting Up a New System for Public Coverage. Front. Public Health 2022, 10, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Sauermann, S.; Herzberg, J.; Burkert, S.; Habetha, S. DiGA—A Chance for the German Healthcare System. J. Eur. CME 2022, 11, 2014047. [Google Scholar] [CrossRef] [PubMed]
- Driving the Digital Transformation of Germany’s Healthcare System for the Good of Patients. Available online: https://www.bundesgesundheitsministerium.de/en/digital-healthcare-act.html (accessed on 20 June 2023).
- Chittaranjan, A. The Inconvenient Truth About Convenience and Purposive Samples. Indian. J. Psychol. Med. 2021, 43, 86–88. [Google Scholar]
- Jaychander, D.; Coleman, C.; Rand, V. Novel Eye-Tracking Methods to Evaluate the Usability of Electronic Health Records. Stud. Health Technol. Inform. 2019, 262, 244–247. [Google Scholar]
- Khairat, S.; Coleman, C.; Ottmar, P. Physician’s gender and their use of electronic health records: Finding from a mixed-methods usability study. J. Am. Med. Inform. Assoc. 2019, 26, 1505–1514. [Google Scholar] [CrossRef]
- Huang, Z.; Mou, J. Gender differences in user perception of usability and performance of online travel agency websites. Technol. Soc. 2021, 66, 101671. [Google Scholar] [CrossRef]
- Sandelowski, M.J. Justifying qualitative research. Res. Nurs. Health 2008, 31, 193–195. [Google Scholar] [CrossRef]
- Vasileiou, K.; Barnett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BMC Med. Res. Methodol. 2018, 18, 148. [Google Scholar] [CrossRef] [Green Version]
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Crouch, M.; McKenzie, H. The logic of small samples in interview-based qualitative research. Soc. Sci. Inf. 2006, 45, 483–499. [Google Scholar] [CrossRef]
- Pacheco, C.; García, I.; Reyes, M. Requirements elicitation techniques: A systematic literature review based on the maturity of the techniques. IET Softw. 2018, 12, 365–378. [Google Scholar] [CrossRef]
- Szinay, D.; Perski, O.; Jones, A.; Chadborn, T.; Brown, J.; Naughton, F. Perceptions of Factors Influencing Engagement With Health and Well-being Apps in the United Kingdom: Qualitative Interview Study. JMIR Mhealth Uhealth 2021, 9, 29098. [Google Scholar] [CrossRef]
- Li, J.; Silvera-Tawil, D.; Varnfield, M.; Hussain, M.S.; Math, V. Users’ Perceptions Toward mHealth Technologies for Health and Well-being Monitoring in Pregnancy Care: Qualitative Interview Study. JMIR Form. Res. 2021, 5, e28628. [Google Scholar] [CrossRef]
- Anderson, C. Presenting and evaluating qualitative research. Am. J. Pharm. Educ. 2010, 74, 141. [Google Scholar] [CrossRef]
- Witt, H. Strategies in Qualitative and Quantitative Research. FQS 2021, 2, e28628. [Google Scholar]
- CPUX-DS Curriculum and Glossary. Available online: https://uxqb.org/public/documents/CPUX-DS_EN_Curriculum.pdf (accessed on 20 June 2023).




{kind=link}
{kind=link}
{kind=link}
| Research Objective | Key Terms |
|---|---|
| Investigate the relevant organizational conditions for operation of the app | Current workflow of LP patient care |
| Current workflow of PrEP patient care | |
| Differences in PrEP users and LP patient care | |
| Derivations from the current clinical workflow | |
| Participation of different specialists in patient care | |
| Involvement of other institutions | |
| Communication with patients | |
| Possible benefits for physicians | |
| Adaptation of the current clinical workflow | |
| Necessary functionalities for the app from the physician’s point of view in order to integrate the app into patient care | Planned app functionalities: Symptom diary, chat, and video |
| Relevant further app functionalities |
| Characteristics | Specifics | No. of Participants to Which the Characteristic Applies (n = 8) |
|---|---|---|
| Gender | Male | 7 |
| Female | 1 | |
| Experience with HIV patients | 0–5 years | 1 |
| 6–15 years | 1 | |
| 16–25 years | 3 | |
| ≥26 years | 3 | |
| Medical specialization | Internal medicine | 3 |
| Internal medicine/further training in infectiology | 4 | |
| Internal medicine/further training in nephrology | 1 | |
| Frequency of care of LPs | Several times a week | 5 |
| Monthly | 3 | |
| Frequency of care of PrEP users | Several times a week | 6 |
| Monthly | 2 | |
| Non-German languages of PrEP users and LPs | Arabic | 1 |
| Turkish | 2 | |
| Russian | 2 | |
| English | 2 | |
| Romanian | 1 | |
| Spanish | 1 | |
| Italian | 1 | |
| Languages spoken in sub-Saharan Africa (e.g., Kenya, Ghana) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schaaf, J.; Weber, T.; von Wagner, M.; Stephan, C.; Carney, J.; Köhler, S.M.; Voigt, A.; Noll, R.; Storf, H.; Müller, A. Interviews with HIV Experts for Development of a Mobile Health Application in HIV Care—A Qualitative Study. Healthcare 2023, 11, 2180. https://doi.org/10.3390/healthcare11152180
Schaaf J, Weber T, von Wagner M, Stephan C, Carney J, Köhler SM, Voigt A, Noll R, Storf H, Müller A. Interviews with HIV Experts for Development of a Mobile Health Application in HIV Care—A Qualitative Study. Healthcare. 2023; 11(15):2180. https://doi.org/10.3390/healthcare11152180
Chicago/Turabian StyleSchaaf, Jannik, Timm Weber, Michael von Wagner, Christoph Stephan, Jonathan Carney, Susanne Maria Köhler, Alexander Voigt, Richard Noll, Holger Storf, and Angelina Müller. 2023. "Interviews with HIV Experts for Development of a Mobile Health Application in HIV Care—A Qualitative Study" Healthcare 11, no. 15: 2180. https://doi.org/10.3390/healthcare11152180