

Internet-Based Healthcare Knowledge Service for Improvement of Chinese Medicine Healthcare Service Quality

Abstract
:1. Introduction
2. Concept and Characteristics of Smart CM Knowledge Services
2.1. The Connotation of Smart CM Knowledge Services
2.2. The Connotation of Smart CM Knowledge Services
2.2.1. The Homogenization of Medical Service
2.2.2. The Intelligence of Knowledge Services
2.2.3. The Integration of Medical Education and Research
2.2.4. The Precision of Service
3. The Evolution Process of CM Knowledge Services
3.1. Data Collection
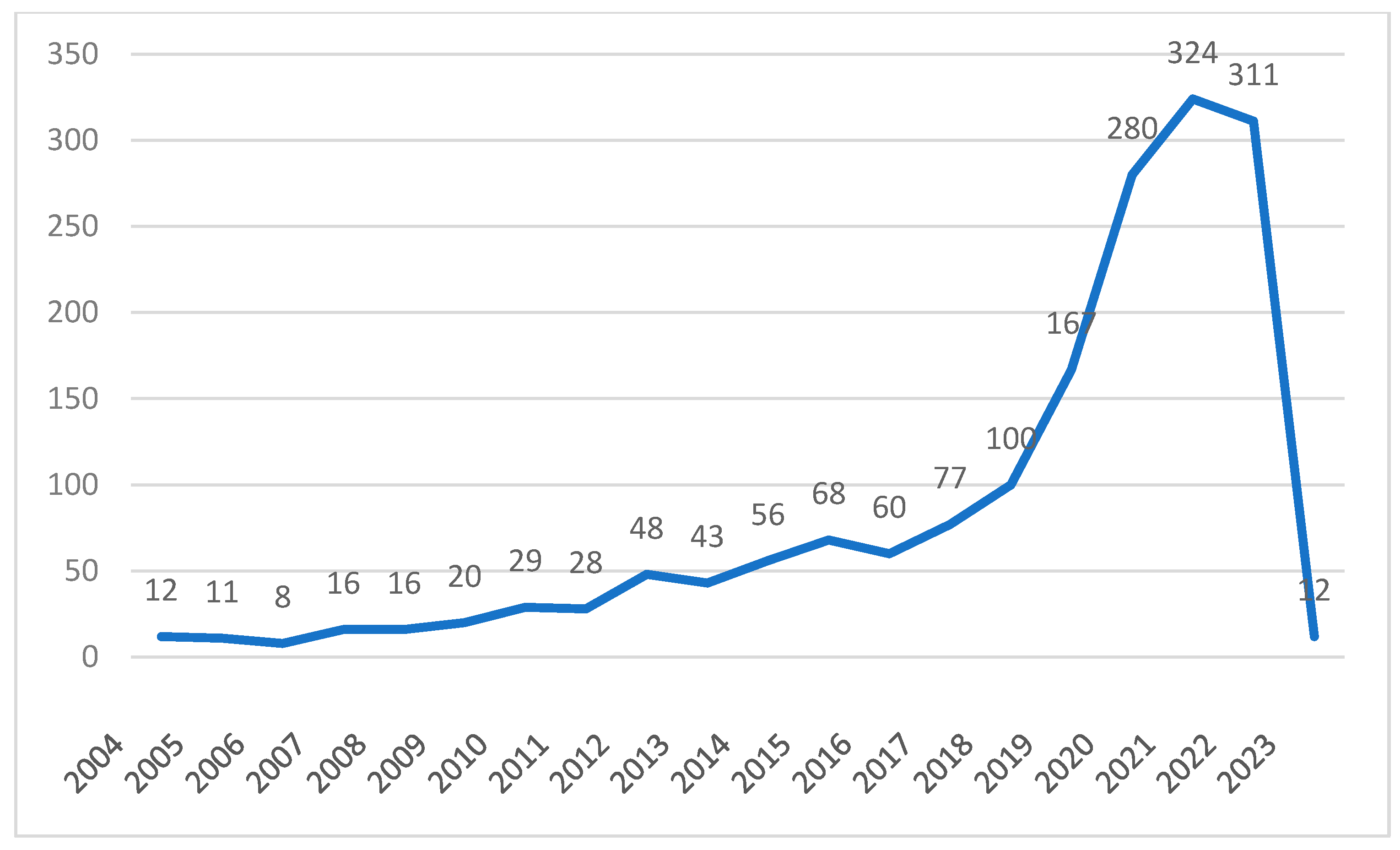
3.2. Time Distribution Map of CM Intelligent Knowledge Service
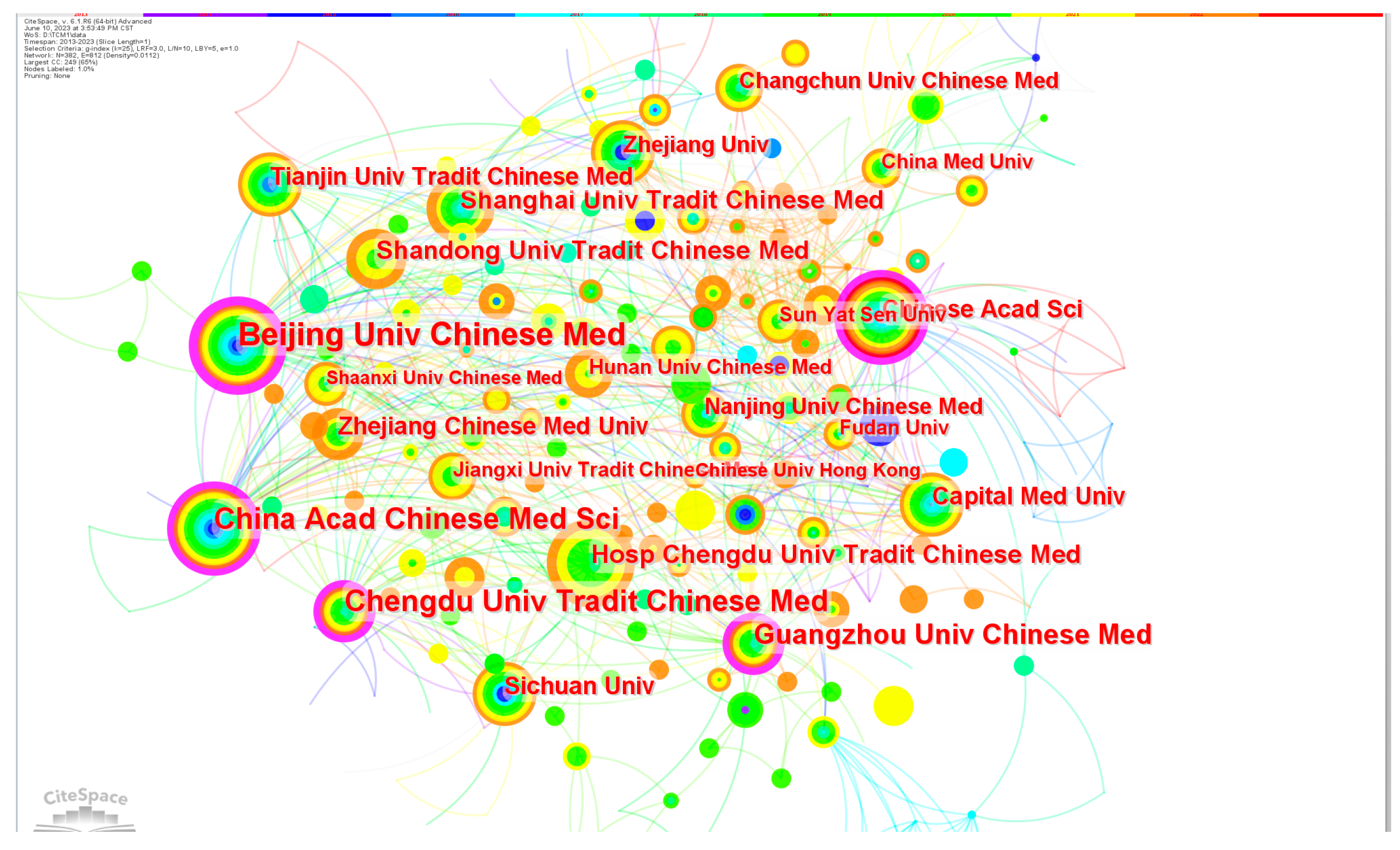
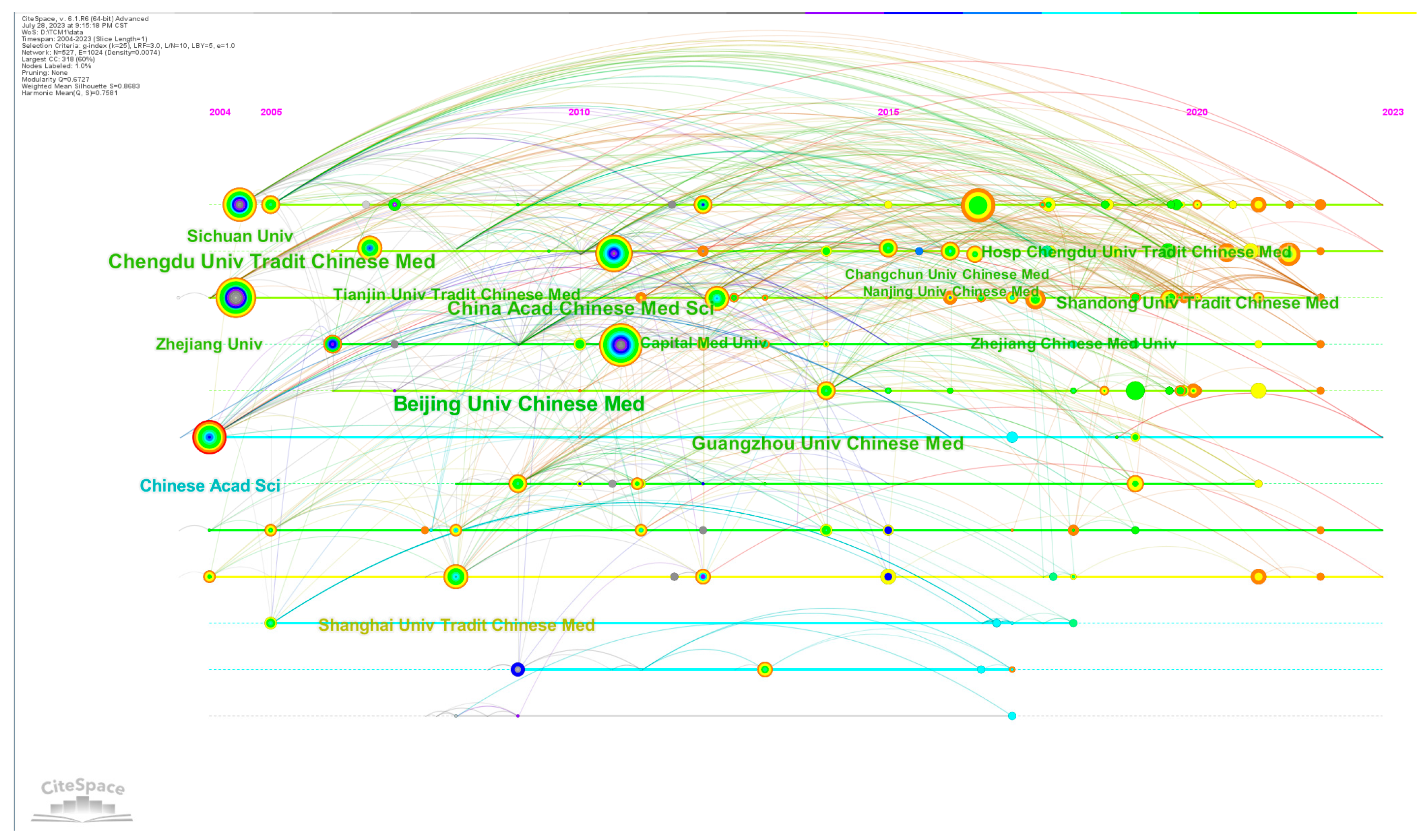
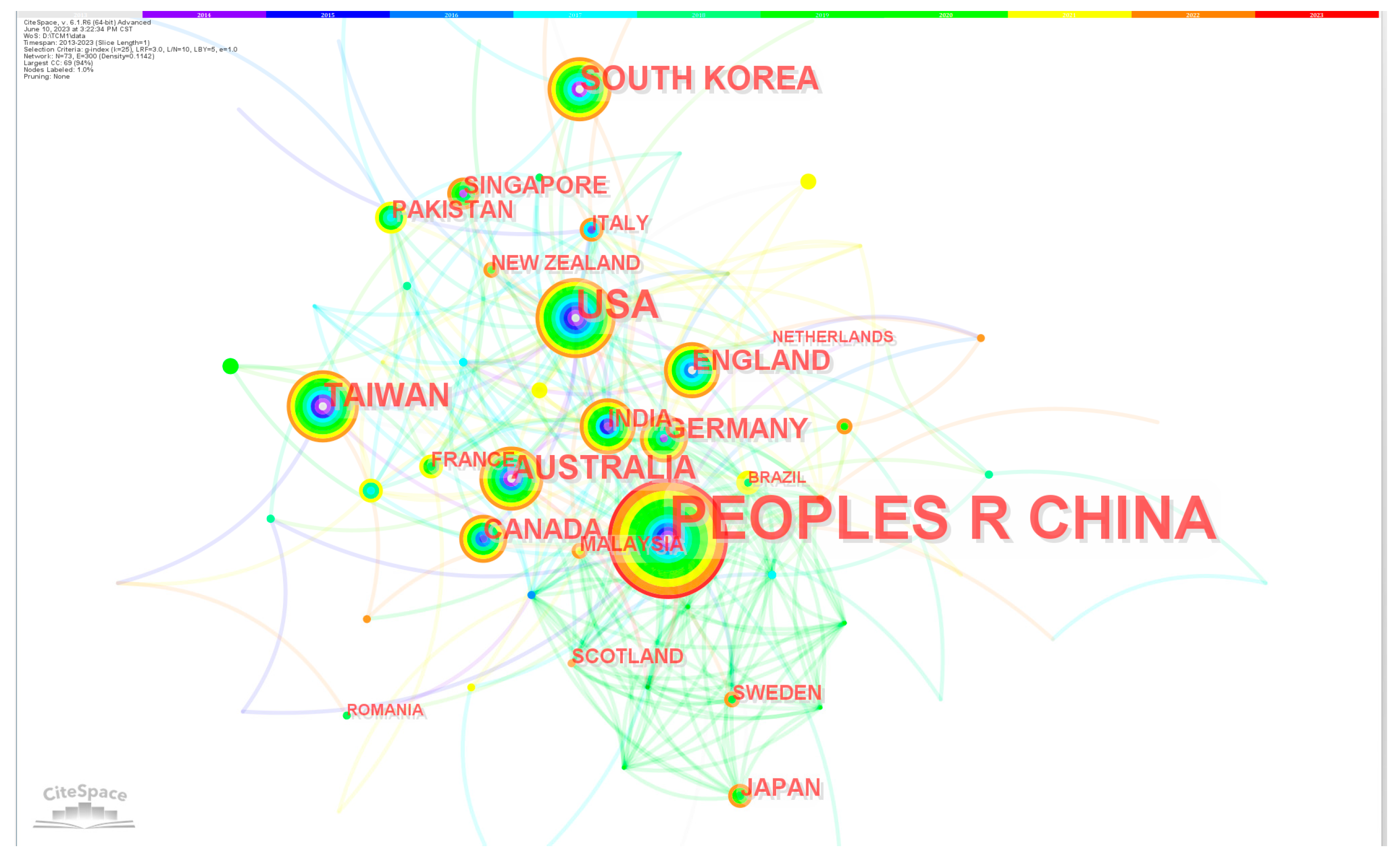
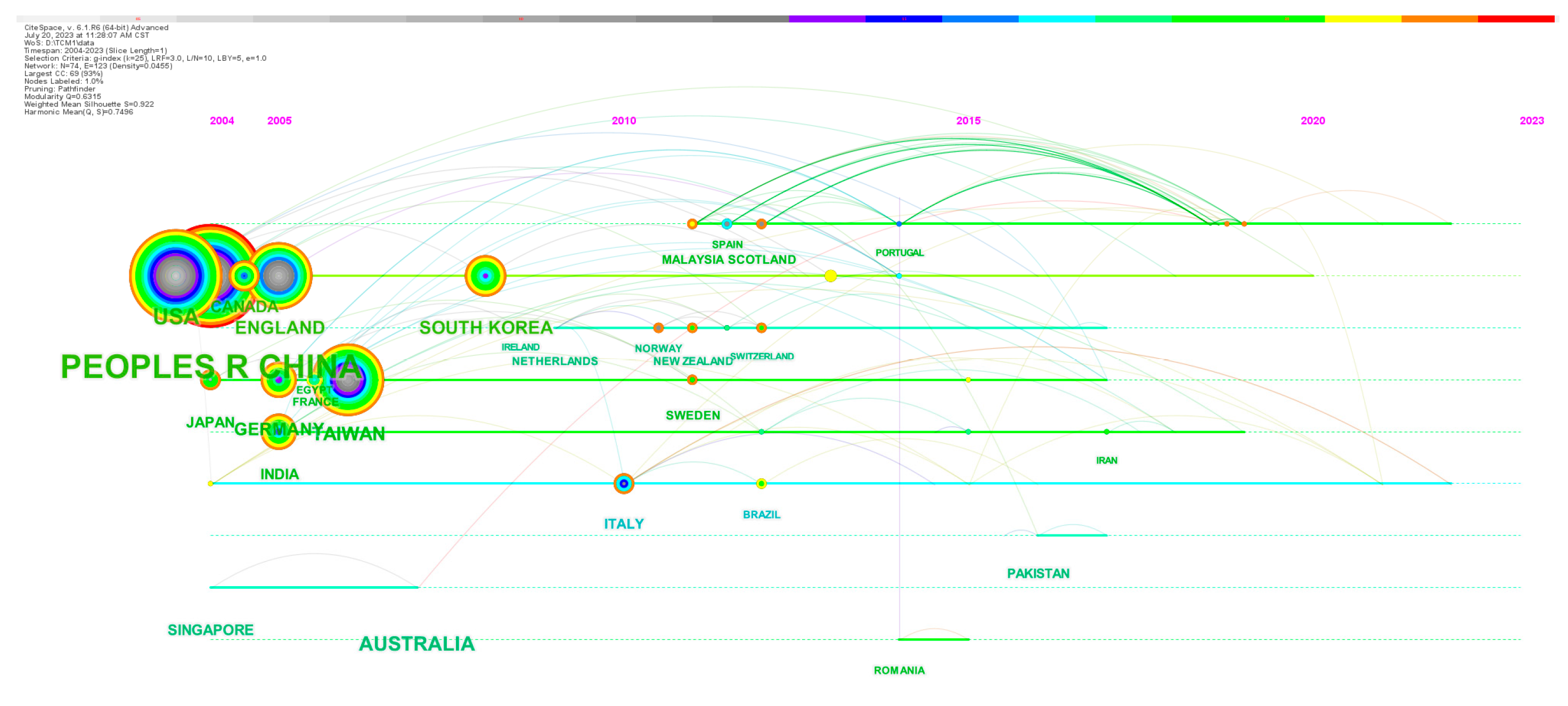
3.3. Space Distribution Analysis
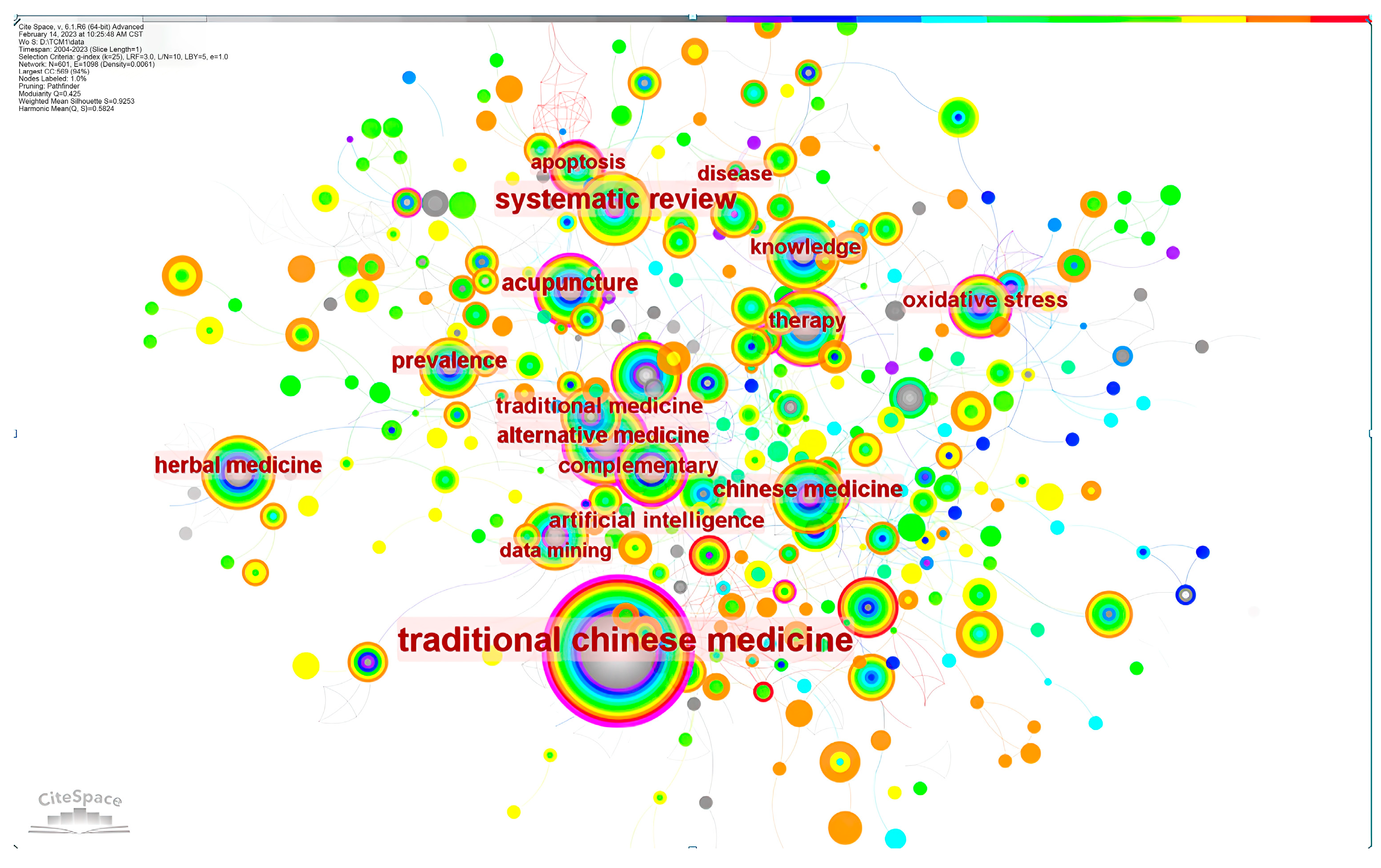
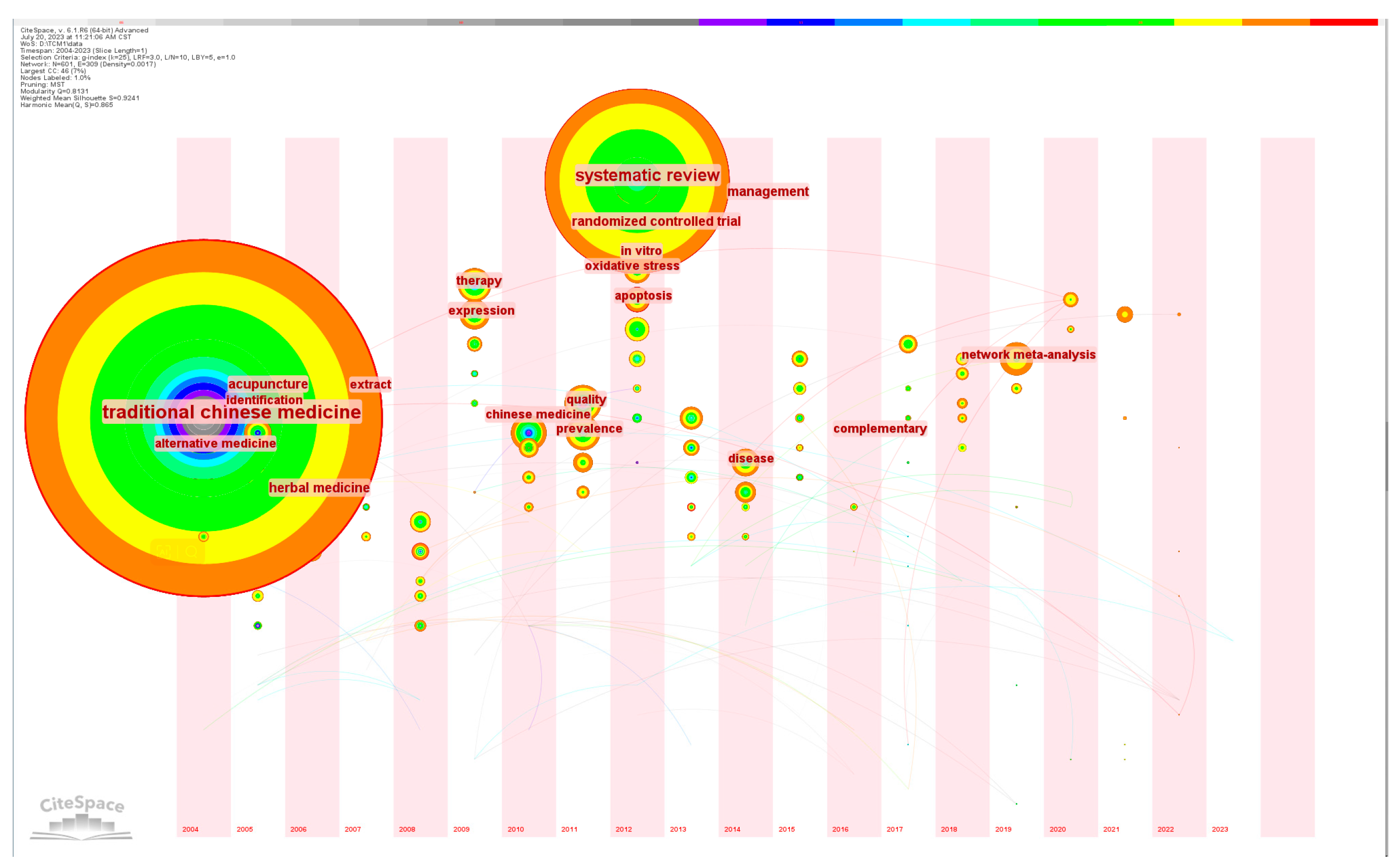
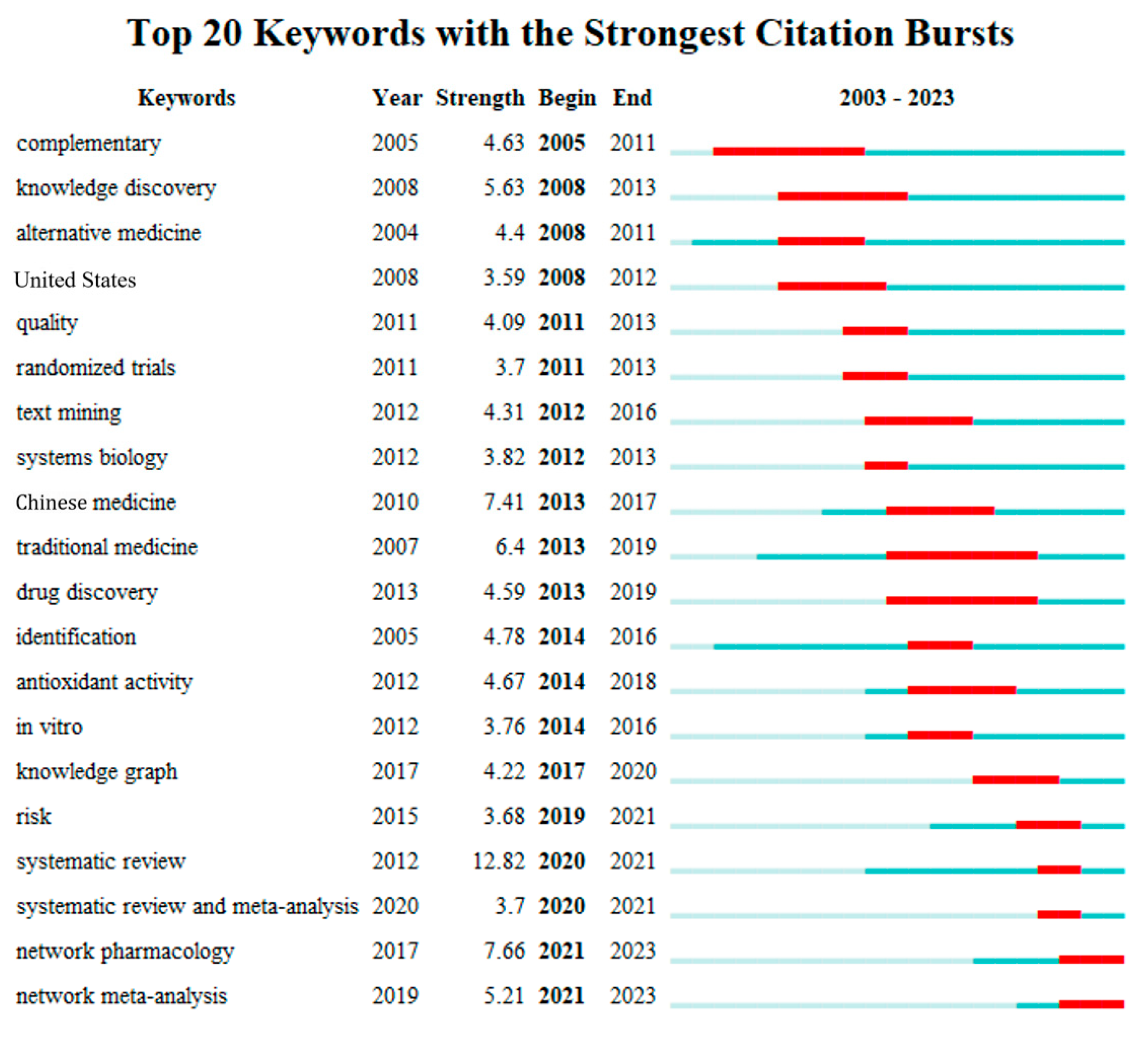
3.4. Evolutionary Analysis of Hot Topics
4. The Smart CM Services under the 5P Healthcare Mode
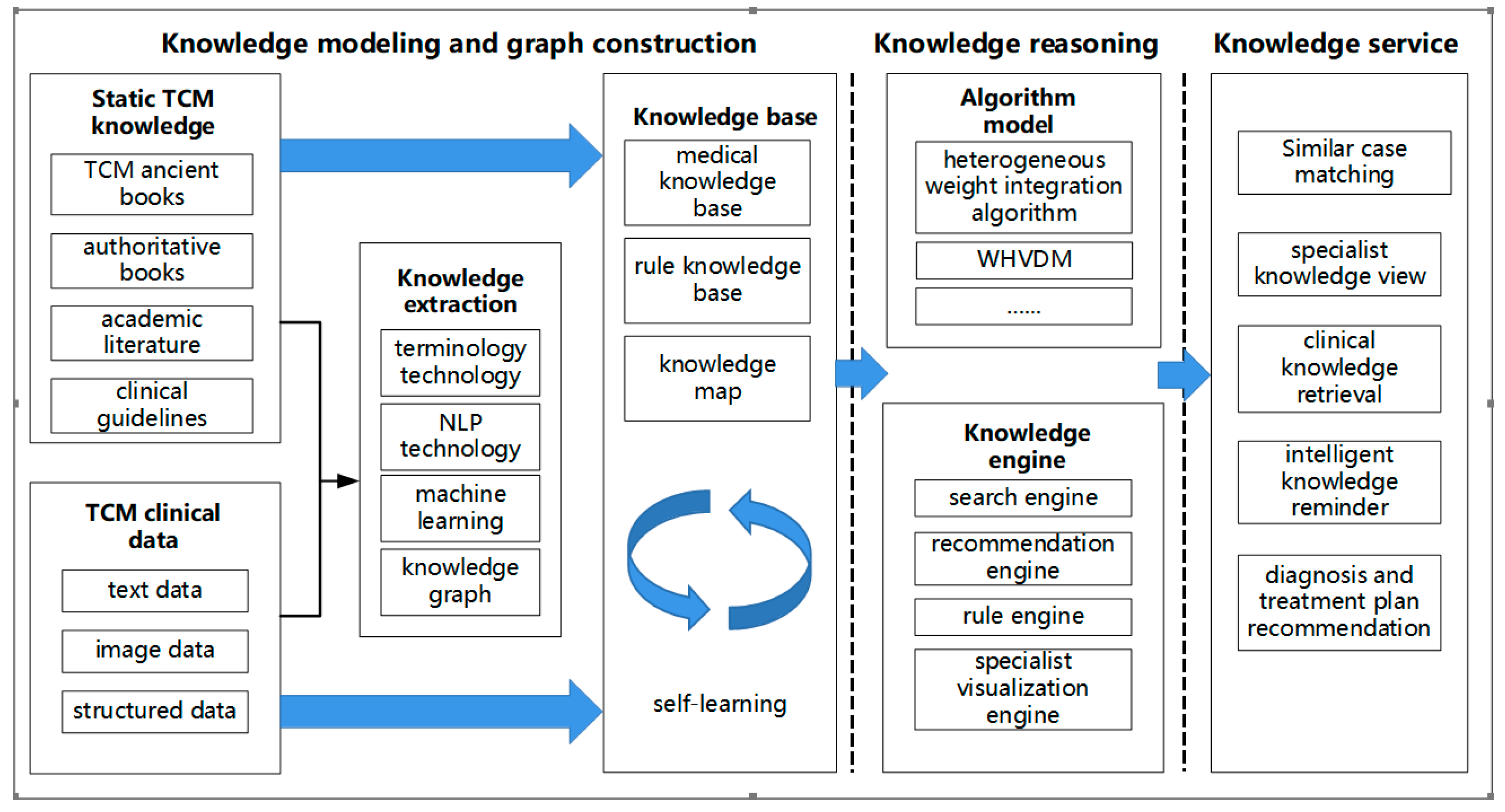
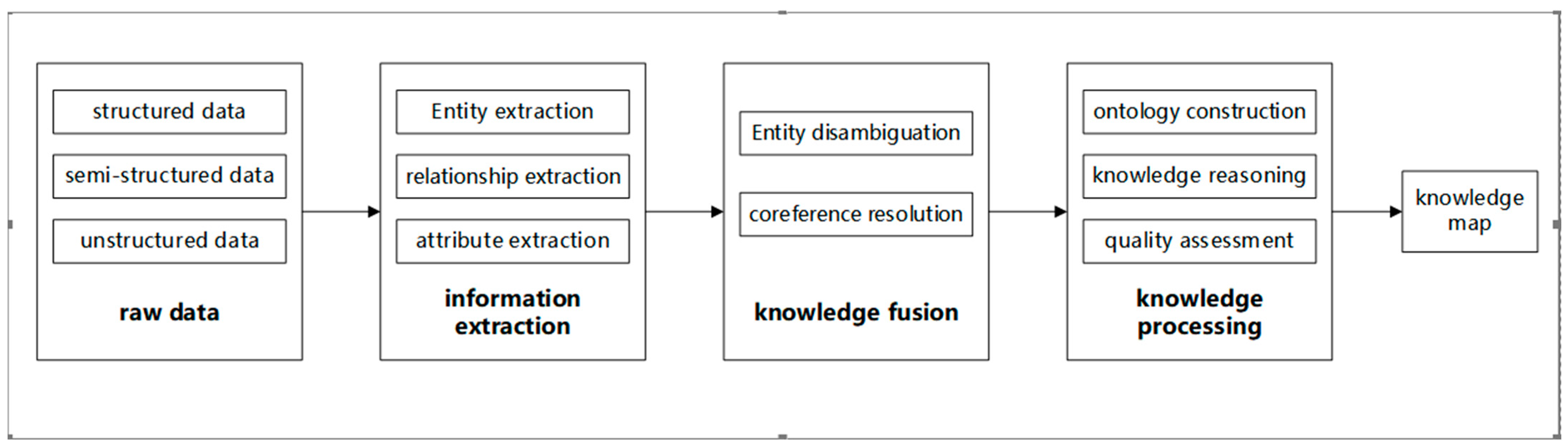
4.1. The Organization of CM Knowledge
4.1.1. CM Case Knowledge Organization Based on Key Clinical Features Extraction
4.1.2. Medical Data Security Sharing Based on Horizontal and Vertical Federated Learning
4.2. CBR Method for Health Knowledge Generation and Discovery
4.2.1. Human–Computer Collaborative Method for CM Case Knowledge Generation
4.2.2. A Case Knowledge Discovery Method Considering Implicit Feedback in Human–Computer Interaction
4.3. Dynamic Personalized Knowledge Recommendation
4.3.1. Health Risk Assessment Based on Time-Series Warning Signals
4.3.2. A Collaborative Recommendation for Medical Research and Education Integration
5. Innovative CM Knowledge Services Models in the Era of Digitalization
5.1. Case-Based CM Knowledge Service Model Guided by Holistic View and Dialectical
5.2. Human–Machine Cooperative Medical Knowledge Recommendation Service Model
5.3. Active Knowledge Service Model for 5P Healthcare
5.4. Panoramic and Dynamic Knowledge Service Mode Driven by Knowledge and Data
6. Conclusions
- Facilitating the Integration of CM and Western Medicine:
- 2.
- Unearthing the Untapped Potential of Folk Chinese Medicine:
- 3.
- Enhancing CM Diagnosis and Medication through Standardized and Precise Prediction:
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- EB152/20 Well-Being and Health Promotion. Available online: https://apps.who.int/gb/e/e_eb152.html (accessed on 18 May 2023).
- Heng, J.; Yang, Z.; Xu, Z. The Current Situation and Countermeasures of the New Forms of Traditional Chinese Medicine Health Services. Chin. Hosp. 2022, 26, 18–21. [Google Scholar] [CrossRef]
- Outline of the “Healthy China 2030” Initiative. Available online: http://www.gov.cn/zhengce/2016-10/25/content_5124174.htm (accessed on 18 May 2023).
- Cheung, F. TCM: Made in China. Nature 2011, 480, S82–S83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Chen, Q.; Shao, Y.; Yin, S.; Liu, C.; Liu, Y.; Wang, R.; Wang, T.; Qiu, Y.; Yu, H. Anticancer Activities of CM and Their Active Components against Tumor Metastasis. Biomed. Pharmacother. 2021, 133, 111044. [Google Scholar] [CrossRef]
- Banik, K.; Ranaware, A.M.; Deshpande, V.; Nalawade, S.P.; Padmavathi, G.; Bordoloi, D.; Sailo, B.L.; Shanmugam, M.K.; Fan, L.; Arfuso, F.; et al. Honokiol for Cancer Therapeutics: A Traditional Medicine that Can Modulate Multiple Oncogenic Targets. Pharmacol. Res. 2019, 144, 192–209. [Google Scholar] [CrossRef]
- Weng, W.; Goel, A. Curcumin and Colorectal Cancer: An Update and Current Perspective on this Natural Medicine. Semin. Cancer Biol. 2022, 80, 73–86. [Google Scholar] [CrossRef]
- Martel, J.; Ojcius, D.M.; Chang, C.; Lin, C.; Lu, C.; Ko, Y.; Tseng, S.; Lai, H.; Young, J.D. Anti-Obesogenic and Antidiabetic Effects of Plants and Mushrooms. Nat. Rev. Endocrinol. 2017, 13, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Sureda, A.; Jafari, S.; Memariani, Z.; Tewari, D.; Annunziata, G.; Barrea, L.; Hassan, S.T.S.; Smejkal, K.; Malanik, M.; et al. Berberine in Cardiovascular and Metabolic Diseases: From Mechanisms to Therapeutics. Theranostics 2019, 9, 1923–1951. [Google Scholar] [CrossRef]
- Hao, X.; Pu, Z.; Cao, G.; You, D.; Zhou, Y.; Deng, C.; Shi, M.; Nile, S.H.; Wang, Y.; Zhou, W.; et al. Tanshinone and Salvianolic Acid Biosynthesis Are Regulated by Smmyb98 in Salvia Miltiorrhiza Hairy Roots. J. Adv. Res. 2020, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, Q.; An, P.; Jia, M.; Luan, X.; Tang, J.; Zhang, H. Ginsenoside Rd: A Promising Natural Neuroprotective Agent. Phytomedicine 2022, 95, 153883. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Gao, J.; Peng, M.; Meng, H.; Ma, H.; Cai, P.; Xu, Y.; Zhao, Q.; Si, G. A Review on Central Nervous System Effects of Gastrodin. Front. Pharmacol. 2018, 9, 24. [Google Scholar] [CrossRef]
- Yan, F.; Li, F.; Liu, J.; Ye, S.; Zhang, Y.; Jia, J.; Li, H.; Chen, D.; Mo, X. The Formulae and Biologically Active Ingredients of Chinese Herbal Medicines for the Treatment of Atopic Dermatitis. Biomed. Pharmacother. 2020, 127, 110142. [Google Scholar] [CrossRef]
- Mu, Z.; Guo, J.; Zhang, D.; Xu, Y.; Zhou, M.; Guo, Y.; Hou, Y.; Gao, X.; Han, X.; Geng, L. Therapeutic Effects of Shikonin on Skin Diseases: A Review. Am. J. Chin. Med. 2021, 49, 1871–1895. [Google Scholar] [CrossRef]
- O’Reilly, E.; Sevigny, M.; Sabarre, K.; Phillips, K.P. Perspectives of Complementary and Alternative Medicine (Cam) Practitioners in the Support and Treatment of Infertility. BMC Complement. Altern. Med. 2014, 14, 394. [Google Scholar] [CrossRef] [Green Version]
- Yang, G.; Tan, Z.; Zhou, L.; Yang, M.; Peng, L.; Liu, J.; Cai, J.; Yang, R.; Han, J.; Huang, Y.; et al. Effects of Angiotensin Ii Receptor Blockers and Ace (Angiotensin-Converting Enzyme) Inhibitors on Virus Infection, Inflammatory Status, and Clinical Outcomes in Patients with COVID-19 and Hypertension a Single-Center Retrospective Study. Hypertension 2020, 76, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Xiang, Y.; Fang, W.; Zheng, Y.; Li, B.; Hu, Y.; Lang, C.; Huang, D.; Sun, Q.; Xiong, Y.; et al. Clinical Features and Treatment of COVID-19 Patients in Northeast Chongqing. J. Med. Virol. 2020, 92, 797–806. [Google Scholar] [CrossRef]
- Lung, J.; Lin, Y.; Yang, Y.; Chou, Y.; Shu, L.; Cheng, Y.; Liu, H.T.; Wu, C. The Potential Chemical Structure of Anti-Sars-Cov-2 Rna-Dependent Rna Polymerase. J. Med. Virol. 2020, 92, 693–697. [Google Scholar] [CrossRef]
- Statistical Bulletin on the Development of China’s Health and Medical Care in 2021. Available online: http://www.gov.cn/xinwen/2022-07/12/content_5700670.htm (accessed on 18 May 2023).
- Enhancement of Chinese Citizens’ Health Literacy in Traditional Chinese Medicine During the 13th Five-Year Plan Period. Available online: https://zhongyi.gmw.cn/2021-10/26/content_35262425.htm (accessed on 18 May 2023).
- Liu, X.; Zhang, B.; Susarla, A.; Padman, R. Go to Youtube and Call Me in the Morning: Use of Social Media for Chronic Conditions. MIS Q. 2020, 44, 257–283. [Google Scholar] [CrossRef]
- Bobroske, K.; Freeman, M.; Huan, L.; Cattrell, A.; Scholtes, S. Curbing the Opioid Epidemic at Its Root: The Effect of Provider Discordance After Opioid Initiation. Manag. Sci. 2022, 68, 2003–2015. [Google Scholar] [CrossRef]
- Hajjar, A.; Alagoz, O. Personalized Disease Screening Decisions Considering a Chronic Condition. Manag. Sci. 2022. [Google Scholar] [CrossRef]
- Basajja, M.; Suchanek, M.; Taye, G.T.; Amare, S.Y.; Nambobi, M.; Folorunso, S.; Plug, R.; Oladipo, F.; van Reisen, M. Proof of Concept and Horizons on Deployment of Fair Data Points in the COVID-19 Pandemic. Data Intell. 2022, 4, 917–937. [Google Scholar] [CrossRef]
- Du, H.; Le, Z.; Wang, H.; Chen, Y.; Yu, J. Cokg-Qa: Multi-Hop Question Answering over COVID-19 Knowledge Graphs. Data Intell. 2022, 4, 471–492. [Google Scholar] [CrossRef]
- Ghardallou, M.; Wirtz, M.; Folorunso, S.; Touati, Z.; Ogundepo, E.; Smits, K.; Mtiraoui, A.; van Reisen, M. Expanding Non-Patient COVID-19 Data: Towards the Fairification of Migrants’ Data in Tunisia, Libya and Niger. Data Intell. 2022, 4, 955–970. [Google Scholar] [CrossRef]
- Jia, T.; Yang, Y.; Lu, X.; Zhu, Q.; Yang, K.; Zhou, X. Link Prediction Based on Tensor Decomposition for the Knowledge Graph of COVID-19 Antiviral Drug. Data Intell. 2022, 4, 134–148. [Google Scholar] [CrossRef]
- Wang, X.; Liu, J.; Wu, C.; Liu, J.; Li, Q.; Chen, Y.; Wang, X.; Chen, X.; Pang, X.; Chang, B.; et al. Artificial Intelligence in Tongue Diagnosis: Using Deep Convolutional Neural Network for Recognizing Unhealthy Tongue with Tooth-Mark. Comp. Struct. Biotechnol. J. 2020, 18, 973–980. [Google Scholar] [CrossRef]
- Chu, X.; Sun, B.; Huang, Q.; Peng, S.; Zhou, Y.; Zhang, Y. Quantitative Knowledge Presentation Models of Traditional Chinese Medicine (CM): A Review. Artif. Intell. Med. 2020, 103, 101810. [Google Scholar] [CrossRef]
- Li, C.; Zhang, D.; Chen, S. Research about Tongue Image of Traditional Chinese Medicine(CM) Based on Artificial Intelligence Technology. In Proceedings of the IEEE 5th Information Technology and Mechatronics Engineering Conference (ITOEC), Chongqing, China, 12–14 June 2020. [Google Scholar]
- Yang, S.; Ding, S.; Gu, D.; Li, X.; Liu, Z. Data-Driven Knowledge Discovery And Knowledge Service Methods in Medical and Health Big Data. J. Manag. World 2022, 38, 219–229. [Google Scholar] [CrossRef]
- Li, L.; Wang, Z.; Wang, J.; Zheng, Y.; Li, Y.; Wang, Q. Enlightenment About Using TCM Constitutions for Individualized Medicine and Construction of Chinese-Style Precision Medicine: Research Progress with TCM Constitutions. Sci. China-Life Sci. 2021, 64, 2092–2099. [Google Scholar] [CrossRef]
- Mingers, J.; Leydesdorff, L. A Review of Theory and Practice in Scientometrics. Eur. J. Oper. Res. 2015, 246, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Chen, C. Citespace II: Detecting and Visualizing Emerging Trends and Transient Patterns in Scientific Literature. J. Am. Soc. Inf. Sci. Technol. 2006, 57, 359–377. [Google Scholar] [CrossRef] [Green Version]
- Donthu, N.; Kumar, S.; Mukherjee, D.; Pandey, N.; Lim, W.M. How to Conduct a Bibliometric Analysis: An Overview and Guidelines. J. Bus. Res. 2021, 133, 285–296. [Google Scholar] [CrossRef]
- Ren, X.; Guo, Y.; Wang, H.; Gao, X.; Chen, W.; Wang, T. The Intelligent Experience Inheritance System for Traditional Chinese Medicine. J. Evid.-Based Med. 2023, 16, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Liu, J.; Li, W.; Liu, Y.; Hui, X.; Qu, P.; Jiang, Z.; Li, J.; Wang, J. Machine Learning in Tcm with Natural Products and Molecules: Current Status and Future Perspectives. Chin. Med. 2023, 18, 43. [Google Scholar] [CrossRef]
- Niu, Q.; Li, H.; Tong, L.; Liu, S.; Zong, W.; Zhang, S.; Tian, S.; Wang, J.; Liu, J.; Li, B.; et al. Tcmfp: A Novel Herbal Formula Prediction Method Based on Network Target’s Score Integrated with Semi-Supervised Learning Genetic Algorithms. Brief. Bioinform. 2023, 24, bbad102. [Google Scholar] [CrossRef]
- Liu, Z.; Luo, C.; Fu, D.; Gui, J.; Zheng, Z.; Qi, L.; Guo, H. A Novel Transfer Learning Model for Traditional Herbal Medicine Prescription Generation from Unstructured Resources and Knowledge. Artif. Intell. Med. 2022, 124, 102232. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Zhang, Q.; Yu, L.; Zhu, J.; Cao, Y.; Gao, X. The Signaling Pathways and Targets of Traditional Chinese Medicine and Natural Medicine in Triple-Negative Breast Cancer. J. Ethnopharmacol. 2021, 264, 113249. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shi, X.; Li, L.; Efferth, T.; Shang, D. The Impact of Artificial Intelligence on Traditional Chinese Medicine. Am. J. Chin. Med. 2021, 49, 1297–1314. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Peng, Y.; Liu, B. Text Mining for Traditional Chinese Medical Knowledge Discovery: A Survey. J. Biomed. Inform. 2010, 43, 650–660. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Zhou, J.; Zhang, B. Computational Traditional Chinese Medicine Diagnosis: A Literature Survey. Comput. Biol. Med. 2021, 133, 104358. [Google Scholar] [CrossRef]
- Gu, D.; Liang, C.; Zhao, H. A Case-Based Reasoning System Based on Weighted Heterogeneous Value Distance Metric for Breast Cancer Diagnosis. Artif. Intell. Med. 2017, 77, 31–47. [Google Scholar] [CrossRef]
- Yang, S.; Ding, S.; Gu, D.; Li, X.; Ouyang, B.; Qi, J. Healthcare Internet of Things: Transformation and Innovative Development of Medical and Health Models in the New Era. J. Manag. Sci. China 2021, 24, 1–11. [Google Scholar] [CrossRef]
- Gu, D.; Su, K.; Zhao, H. A Case-Based Ensemble Learning System for Explainable Breast Cancer Recurrence Prediction. Artif. Intell. Med. 2020, 107, 101858. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Li, H.; Hu, M.; Sun, H. Research on Mining Medical Implicit Knowledge based on CART Algorithm: A Case Study on Traditional Chinese Medicine Case Records. Inf. Sci. 2021, 39, 84–91. [Google Scholar] [CrossRef]
- Xie, Y.; Gu, D.; Wang, X.; Yang, X.; Zhao, W.; Khakimova, A.K.; Liu, H. A Smart Healthcare Knowledge Service Framework for Hierarchical Medical Treatment System. Healthcare 2021, 10, 32. [Google Scholar] [CrossRef]
- Guo, X.; Wang, H.; Xu, M. Research on the Impact of Healthcare Information Sharing on Patient Transfer Quantity and Service Quality Level. Chin. J. Manag. Sci. 2021, 29, 226–236. [Google Scholar] [CrossRef]
- Liu, B.; Hu, J.; Xie, Y.; Weng, W.; Wang, R.; Zhang, Y.; Li, X.; Zhang, K.; Ren, A.; Li, J.; et al. Effects of Integrative Chinese and Western Medicine on Arterial Oxygen Saturation in Patients with Severe Acute Respiratory Syndrome. Chin. J. Integr. Med. 2004, 10, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Tu, B.; Johnston, M.; Hui, K. Elderly Patient Refractory to Multiple Pain Medications Successfully Treated with Integrative East-West Medicine. Int. J. Gen. Med. 2008, 1, 3–6. [Google Scholar] [PubMed] [Green Version]
- Gu, D.; Li, M.; Yang, X.; Gu, Y.; Zhao, Y.; Liang, C.; Liu, H. An Analysis of Cognitive Change in Online Mental Health Communities: A Textual Data Analysis Based on Post Replies of Support Seekers. Inf. Process. Manage. 2023, 60, 103192. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Number of Published Articles | Institution | Centrality | |
|---|---|---|---|---|
| 1 | 2013 | 134 | Beijing Univ Chinese Med | 0.21 |
| 2 | 2013 | 114 | Chengdu Univ Tradit Chinese Med | 0.11 |
| 3 | 2013 | 100 | China Acad Chinese Med Sci | 0.14 |
| 4 | 2014 | 79 | Guangzhou Univ Chinese Med | 0.11 |
| 5 | 2020 | 59 | Shandong Univ Tradit Chinese Med | 0.05 |
| 6 | 2013 | 51 | Shanghai Univ Tradit Chinese Med | 0.05 |
| 7 | 2019 | 48 | Hosp Chengdu Univ Tradit Chinese Med | 0.03 |
| 8 | 2013 | 46 | Tianjin Univ Tradit Chinese Med | 0.07 |
| 9 | 2013 | 46 | Chinese Acad Sci | 0.12 |
| 10 | 2018 | 39 | Zhejiang Chinese Med Univ | 0.04 |
| 11 | 2013 | 38 | Sichuan Univ | 0.04 |
| 12 | 2014 | 34 | Capital Med Univ | 0.08 |
| 13 | 2016 | 27 | Nanjing Univ Chinese Med | 0.02 |
| 14 | 2013 | 26 | Zhejiang Univ | 0.04 |
| 15 | 2016 | 24 | Changchun Univ Chinese Med | 0.01 |
| 16 | 2020 | 21 | Jiangxi Univ Tradit Chinese Med | 0 |
| 17 | 2020 | 20 | Hunan Univ Chinese Med | 0.02 |
| 18 | 2019 | 19 | Sun Yat Sen Univ | 0.02 |
| 19 | 2013 | 18 | Fudan Univ | 0.02 |
| 20 | 2013 | 18 | Kyung Hee Univ | 0 |
| Year | Number of Published Articles | Institution | Centrality | |
|---|---|---|---|---|
| 1 | 2013 | 1270 | PEOPLES R CHINA | 0.69 |
| 2 | 2013 | 96 | USA | 0.26 |
| 3 | 2013 | 48 | AUSTRALIA | 0.03 |
| 4 | 2013 | 42 | TAIWAN | 0.03 |
| 5 | 2013 | 37 | SOUTH KOREA | 0.07 |
| 6 | 2013 | 28 | ENGLAND | 0.02 |
| 7 | 2013 | 25 | CANADA | 0.01 |
| 8 | 2014 | 24 | GERMANY | 0.12 |
| 9 | 2014 | 20 | INDIA | 0.19 |
| 10 | 2014 | 15 | SINGAPORE | 0 |
| 11 | 2016 | 14 | PAKISTAN | 0.09 |
| 12 | 2013 | 13 | JAPAN | 0.01 |
| 13 | 2013 | 12 | ITALY | 0.19 |
| 14 | 2015 | 10 | MALAYSIA | 0.04 |
| 15 | 2018 | 8 | NEW ZEALAND | 0 |
| 16 | 2017 | 8 | FRANCE | 0.05 |
| 17 | 2016 | 8 | SWEDEN | 0.01 |
| 18 | 2013 | 8 | SCOTLAND | 0.02 |
| 19 | 2018 | 7 | BRAZIL | 0.05 |
| 20 | 2014 | 7 | ROMANIA | 0.01 |
| Count | Centrality | Year | Keywords | |
|---|---|---|---|---|
| 1 | 478 | 0.4 | 2003 | traditional Chinese medicine |
| 2 | 161 | 0.04 | 2012 | systematic review |
| 3 | 57 | 0.04 | 2010 | Chinese medicine |
| 4 | 56 | 0.24 | 2005 | acupuncture |
| 5 | 51 | 0.07 | 2006 | herbal medicine |
| 6 | 49 | 0.01 | 2011 | prevalence |
| 7 | 48 | 0.26 | 2004 | alternative medicine |
| 8 | 45 | 0.26 | 2005 | complementary |
| 9 | 43 | 0.13 | 2009 | therapy |
| 10 | 42 | 0.15 | 2012 | oxidative stress |
| 11 | 41 | 0.05 | 2010 | artificial intelligence |
| 12 | 40 | 0.04 | 2005 | knowledge |
| 13 | 40 | 0.06 | 2007 | traditional medicine |
| 14 | 37 | 0.01 | 2003 | disease |
| 15 | 35 | 0.09 | 2004 | data mining |
| CM Knowledge Service | General Medical Knowledge Service | |
|---|---|---|
| Knowledge source | Static knowledge: CM-related academic journals, traditional TCM classics, and guidelines issued by professional TCM organizations. Source of case characteristic data: vision, smell, auscultation, and palpation. | Static knowledge: authoritative sources such as international medical journals, clinical guidelines, and drug registration information. Source of case characteristics data: medical examination report. |
| Knowledge system | CM knowledge services are mainly based on the theory and practice of CM, including CM, acupuncture, and CM diagnostics. | Based on the modern medical system, including various branches of Western medicine, such as internal medicine, surgery, pediatrics, obstetrics and gynecology, etc. |
| Theoretical thinking mode | Traditional Chinese medicine emphasizes syndrome differentiation and treatment, and distinguishes the etiology and pathogenesis of diseases through the four diagnostic methods of CM, such as vision, smell, auscultation, and palpation, and then chooses Chinese medicine or acupuncture and other traditional Chinese medicine treatment methods. | Focus on the physiological and pathological mechanisms of diseases, and draw up treatment plans based on large-scale clinical trials. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Xie, Y.; Yang, X.; Gu, D. Internet-Based Healthcare Knowledge Service for Improvement of Chinese Medicine Healthcare Service Quality. Healthcare 2023, 11, 2170. https://doi.org/10.3390/healthcare11152170
Wang X, Xie Y, Yang X, Gu D. Internet-Based Healthcare Knowledge Service for Improvement of Chinese Medicine Healthcare Service Quality. Healthcare. 2023; 11(15):2170. https://doi.org/10.3390/healthcare11152170
Chicago/Turabian StyleWang, Xiaoyu, Yi Xie, Xuejie Yang, and Dongxiao Gu. 2023. "Internet-Based Healthcare Knowledge Service for Improvement of Chinese Medicine Healthcare Service Quality" Healthcare 11, no. 15: 2170. https://doi.org/10.3390/healthcare11152170