


COVID-19 Pandemic: Did Strict Mobility Restrictions Save Lives and Healthcare Costs in Maharashtra, India?

Abstract
:1. Introduction
2. Data
3. Analysis
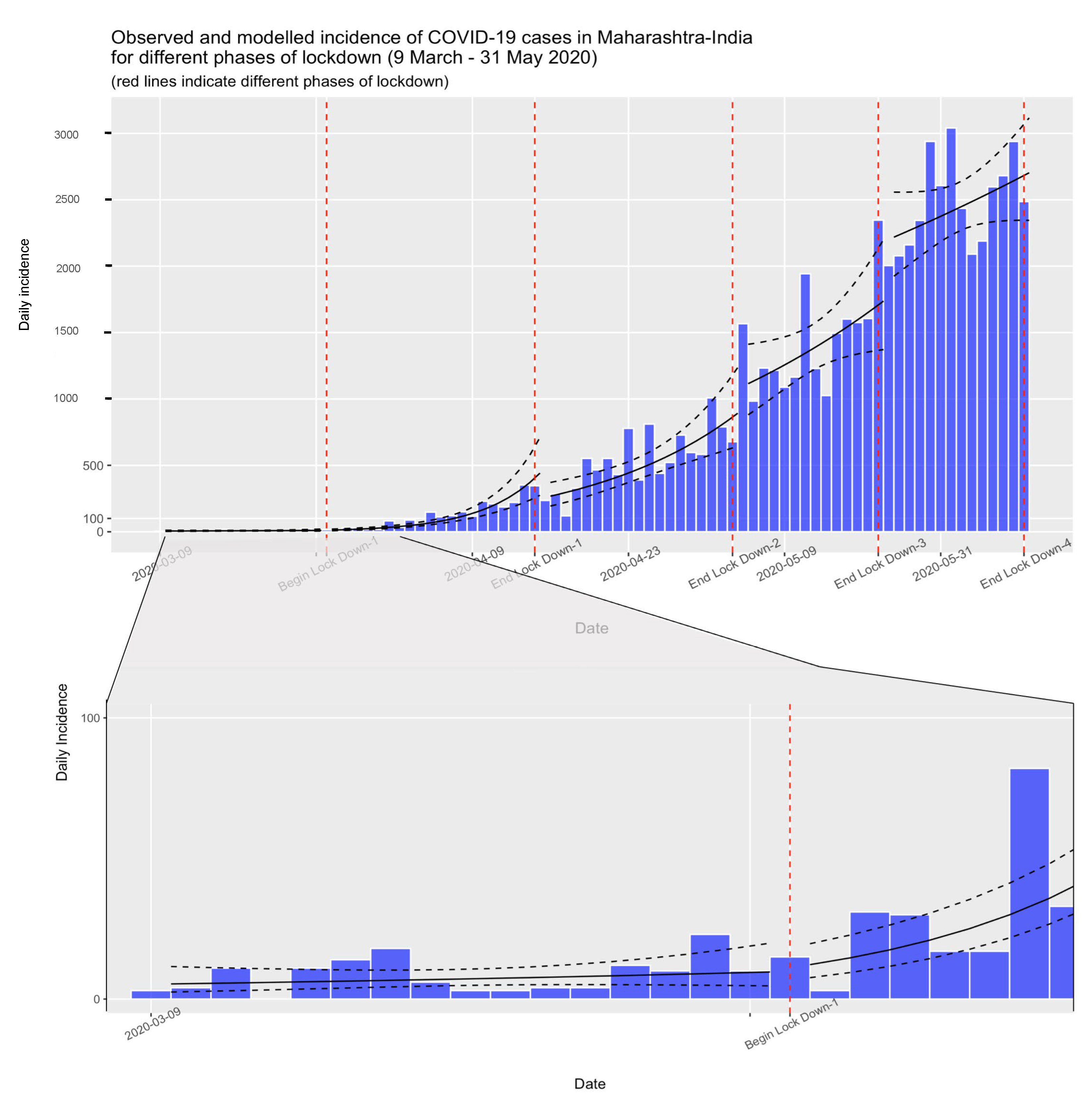
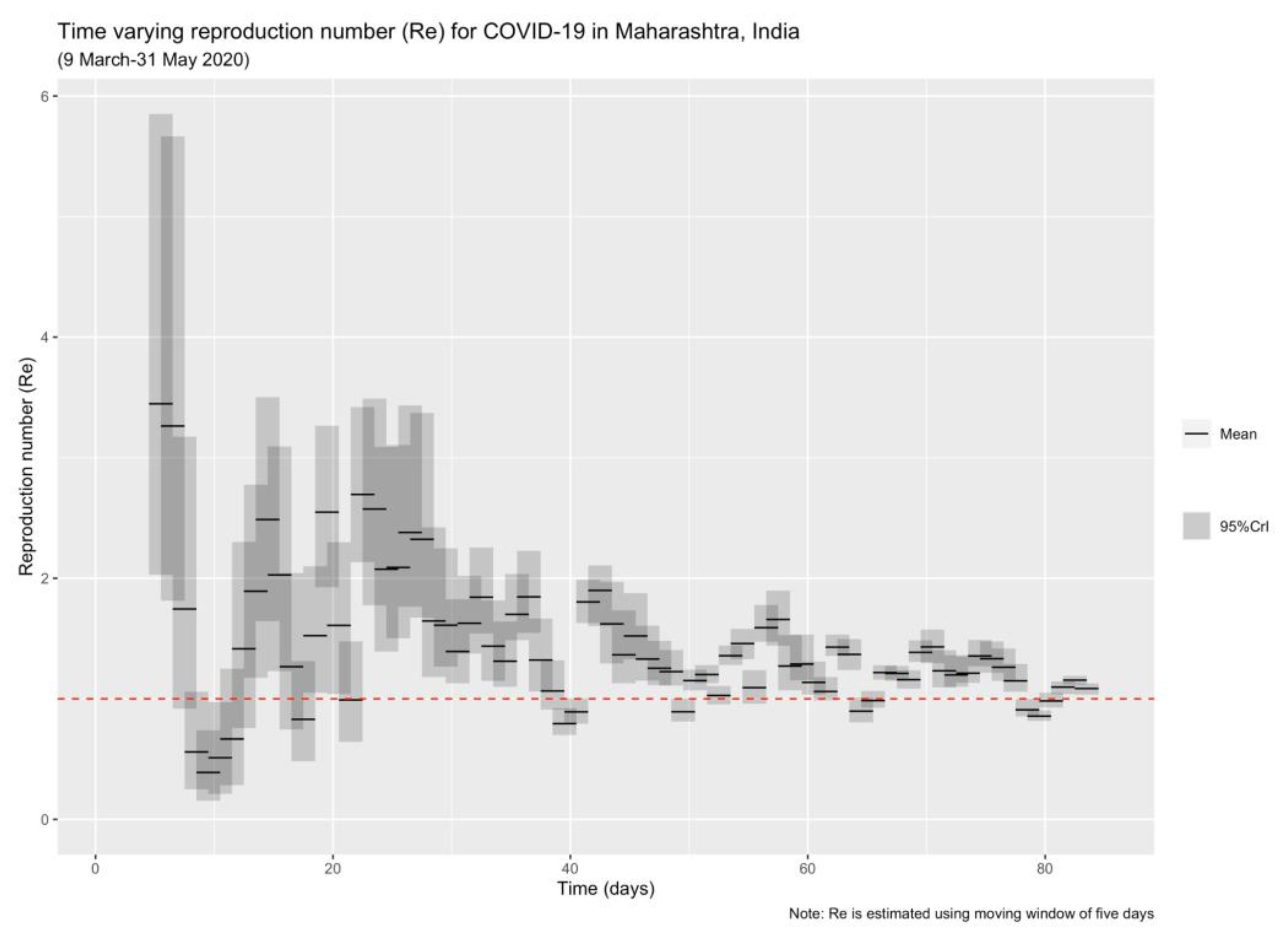
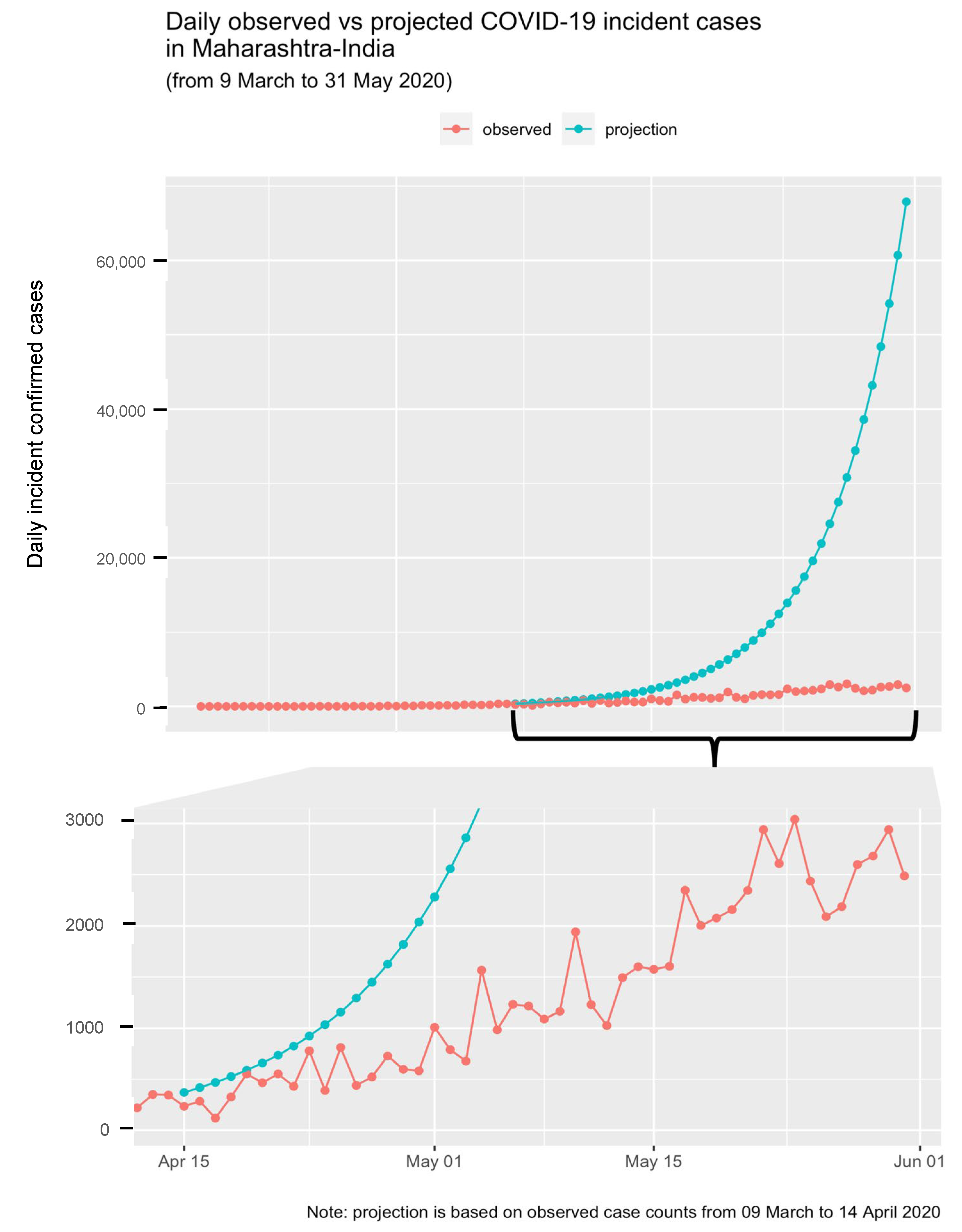
3.1. Epidemic Trajectory Analysis
3.2. Economic Impact Analysis
no. of individuals in ICU care * [(cost of PPE + cost of medicine + cost of general care) * LOSIb (7 days)] (2b) (post-ICU care in general ward for ICU patients)
no. of individuals hospitalized in non-ICU care * [(general ward cost + cost of PPE + cost of medicine) * LOSH (14 days) + cost of test kit] (2c) (non-ICU patients)
no. of non-hospitalized cases in isolation * (cost of test kit + cost of outpatient medicine) (2d) (non-hospitalized isolated patients)
4. Patient and Public Involvement
5. Results
Epidemic Trajectory Analysis
6. Economic Impact Analysis
7. Sensitivity Analysis
8. Discussion
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worldometers.info. Countries Where COVID-19 Has Spread. Available online: https://www.worldometers.info/coronavirus/countries-where-coronavirus-has-spread/ (accessed on 31 December 2022).
- Lally, M. A cost–benefit analysis of COVID-19 lockdowns in Australia. Monash Bioeth. Rev. 2022, 40, 62–93. [Google Scholar] [CrossRef]
- Strzelecki, A.; Azevedo, A.; Rizun, M.; Rutecka, P.; Zagała, K.; Cicha, K.; Albuquerque, A. Human Mobility Restrictions and COVID-19 Infection Rates: Analysis of Mobility Data and Coronavirus Spread in Poland and Portugal. Int. J. Environ. Res. Public Health 2022, 19, 14455. [Google Scholar] [CrossRef] [PubMed]
- Spiliopoulos, L. On the effectiveness of COVID-19 restrictions and lockdowns: Pan metron ariston. BMC Public Health 2022, 22, 1842. [Google Scholar] [CrossRef]
- Hussein, N.R.; Naqid, I.A.; Saleem, Z.S.M.; Almizori, L.A.; Musa, D.H.; Ibrahim, N. A sharp increase in the number of COVID-19 cases and case fatality rates after lifting the lockdown in Kurdistan region of Iraq. Ann. Med. Surg. 2020, 57, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Mati, S. Do as your neighbours do? Assessing the impact of lockdown and reopening on the active COVID-19 cases in Nigeria. Soc. Sci. Med. 2020, 270, 113645. [Google Scholar] [CrossRef] [PubMed]
- Kharroubi, S.; Saleh, F. Are Lockdown Measures Effective Against COVID-19? Front. Public Health 2020, 8, 549692. [Google Scholar] [CrossRef]
- Meo, S.A.; Abukhalaf, A.A.; Alomar, A.A.; AlMutairi, F.J.; Usmani, A.M.; Klonoff, D.C. Impact of lockdown on COVID-19 prevalence and mortality during 2020 pandemic: Observational analysis of 27 countries. Eur. J. Med. Res. 2020, 25, 56. [Google Scholar] [CrossRef]
- Zhang, H.; You, S.; Zhang, M.; Chen, A.; Hu, Z.; Liu, Y.; Liu, D.; Yuan, P.; Tan, Y. Empirical Study of Monthly Economic Losses Assessments for “Standard Unit Lockdown” Due to COVID-19. Front. Public Health 2022, 10, 859751. [Google Scholar] [CrossRef]
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel. Med. 2020, 27, taaa037. [Google Scholar] [CrossRef] [Green Version]
- Mahmoudi, J.; Xiong, C. How social distancing, mobility, and preventive policies affect COVID-19 outcomes: Big data-driven evidence from the District of Columbia-Maryland-Virginia (DMV) megaregion. PLoS ONE 2022, 17, e0263820. [Google Scholar] [CrossRef]
- Ferguson, E.A.; Brum, E.; Chowdhury, A.; Chowdhury, S.; Kundegorski, M.; Mahmud, A.S.; Purno, N.; Sania, A.; Steenson, R.; Tasneem, M.; et al. Modelling how face masks and symptoms-based quarantine synergistically and cost-effectively reduce SARS-CoV-2 transmission in Bangladesh. Epidemics 2022, 40, 100592. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Undurraga, E.A.; Zubizarreta, J.R. Effectiveness of localized lockdowns in the COVID-19 pandemic. Am. J. Epidemiol. 2022, 191, 812–824. [Google Scholar] [CrossRef] [PubMed]
- Barnett-Howell, Z.; Watson, O.J.; Mobarak, A.M. The benefits and costs of social distancing in high- and low-income countries. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Scherbina, A. Assessing the Optimality of a COVID Lockdown in the United States. Econ. Disasters Clim. Change 2021, 5, 177–201. [Google Scholar] [CrossRef] [PubMed]
- Gandjour, A. Cost-effectiveness of future lockdown policies against the COVID-19 pandemic. Health Serv. Manag. Res. 2023, 36, 51–62. [Google Scholar] [CrossRef]
- Joffe, A.R. COVID-19: Rethinking the lockdown groupthink. Front. Public Health 2021, 9, 625778. [Google Scholar] [CrossRef]
- Shlomai, A.; Leshno, A.; Sklan, E.H.; Leshno, M. Modeling Social Distancing Strategies to Prevent SARS-CoV-2 Spread in Israel: A Cost-Effectiveness Analysis. Value Health 2021, 24, 607–614. [Google Scholar] [CrossRef]
- Miles, D.K.; Stedman, M.; Heald, A.H. “Stay at Home, Protect the National Health Service, Save Lives”: A cost benefit analysis of the lockdown in the United Kingdom. Int. J. Clin. Pract. 2021, 75, e13674. [Google Scholar] [CrossRef]
- Lasaulce, S.; Zhang, C.; Varma, V.; Morărescu, I.C. Analysis of the Tradeoff Between Health and Economic Impacts of the COVID-19 Epidemic. Front. Public Health 2021, 9, 620770. [Google Scholar] [CrossRef]
- Verma, B.K.; Verma, M.; Verma, V.K.; Abdullah, R.B.; Nath, D.C.; Khan, H.T.A.; Verma, A.; Vishwakarma, R.K.; Verma, V. Global lockdown: An effective safeguard in responding to the threat of COVID-19. J. Eval. Clin. Pract. 2020, 26, 1592–1598. [Google Scholar] [CrossRef]
- Homburg, S. Effectiveness of corona lockdowns: Evidence for a number of countries. Econ. Voice 2020, 17, 20200010. [Google Scholar] [CrossRef]
- Smyth, B. The fading impact of lockdowns: A data analysis of the effectiveness of COVID-19 travel restrictions during different pandemic phases. PLoS ONE 2022, 17, e0269774. [Google Scholar] [CrossRef]
- Albassam, D.; Nouh, M.; Hosoi, A. The Effectiveness of Mobility Restrictions on Controlling the Spread of COVID-19 in a Resistant Population. Int. J. Environ. Res. Public Health 2023, 20, 5343. [Google Scholar] [CrossRef]
- Andrews, M.A.; Areekal, B.; Rajesh, K.R.; Krishnan, J.; Suryakala, R.; Krishnan, B.; Muraly, C.P.; Santhosh, P.V. First confirmed case of COVID-19 infection in India: A case report. Indian J. Med. Res. 2020, 151, 490–492. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 56; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Mave, V.; Shaikh, A.; Monteiro, J.M.; Bogam, P.; Pujari, B.S.; Gupte, N. Association of national and regional lockdowns with COVID-19 infection rates in Pune, India. Sci. Rep. 2022, 12, 10446. [Google Scholar] [CrossRef] [PubMed]
- John Hopkins University & Medicine. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU); John Hopkins University & Medicine: Baltimore, MD, USA, 2021. [Google Scholar]
- El-Shabasy, R.M.; Nayel, M.A.; Taher, M.M.; Abdelmonem, R.; Shoueir, K.R.; Kenawy, E.R. Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic. Int. J. Biol. Macromol. 2022, 204, 161–168. [Google Scholar] [CrossRef]
- Salvatore, M.; Basu, D.; Ray, D.; Kleinsasser, M.; Purkayastha, S.; Bhattacharyya, R.; Mukherjee, B. Comprehensive public health evaluation of lockdown as a non-pharmaceutical intervention on COVID-19 spread in India: National trends masking state-level variations. BMJ Open 2020, 10, e041778. [Google Scholar] [CrossRef]
- Maity, S.; Ghosh, N.; Barlaskar, U.R. Interstate disparities in the performances in combatting COVID-19 in India: Efficiency estimates across states. BMC Public Health 2020, 20, 1925. [Google Scholar] [CrossRef]
- Marimuthu, S.; Joy, M.; Malavika, B.; Nadaraj, A.; Asirvatham, E.S.; Jeyaseelan, L. Modelling of reproduction number for COVID-19 in India and high incidence states. Clin. Epidemiol. Glob. Health 2021, 9, 57–61. [Google Scholar] [CrossRef]
- Mitra, A.; Pakhare, A.P.; Roy, A.; Joshi, A. Impact of COVID-19 epidemic curtailment strategies in selected Indian states: An analysis by reproduction number and doubling time with incidence modelling. PLoS ONE 2020, 15, e0239026. [Google Scholar] [CrossRef]
- Singh, G.; Patrikar, S.; Sankara Sarma, P.; Soman, B. Time-dependent dynamic transmission potential and instantaneous reproduction number of COVID-19 pandemic in India. medRxiv 2020. [Google Scholar] [CrossRef]
- Office of the Registrar General & Census Commissioner. Census of India 2011: Population Finder. Available online: https://censusindia.gov.in/census.website/data/population-finder (accessed on 22 May 2022).
- Deshpande, A. Maharashtra economy to grow 6.8% in 2022-23: State Economic Survey. The Hindu, 8 March 2023; p. 1. [Google Scholar]
- Shil, P.; Atre, N.M.; Tandale, B.V. Epidemiological findings for the first and second waves of COVID-19 pandemic in Maharashtra, India. Spat. Spatiotemporal Epidemiol. 2022, 41, 100507. [Google Scholar] [CrossRef]
- Akhil, N.R. Maharashtra Government’s Response to COVID-19 (till April 20, 2020). The PRS Blog, 21 April 2020; p. 2. [Google Scholar]
- DMU-RRD-MH. Implementation of Janta Curfew (DMU-2020/CR42/DM-1). DMU-2020/CR42/DM-1. 2020. Available online: https://pune.gov.in/corona-virus-updates/ (accessed on 23 December 2020).
- DMU-RRD-MH. Lockdown Notification (DMU-2020/CR92/DM-1). DMU-2020/CR92/DM-1. 2020. Available online: https://pune.gov.in/corona-virus-updates/ (accessed on 23 December 2020).
- DMU-RRD-MH. Easing of Restrictions and Phase-wise opening of Lockdown. (MISSION BEGIN AGAIN). DMU-2020/CR42/DM-1. 2020. Available online: https://pune.gov.in/corona-virus-updates/ (accessed on 23 December 2020).
- IDSP-Maharashtra. COVID-91 Related Updates Media Bulletin Date: 15th November 2021. 2021. [Google Scholar]
- Mahajan, P.; Kaushal, J. Epidemic Trend of COVID-19 Transmission in India During Lockdown-1 Phase. J. Community Health 2020, 45, 1291–1300. [Google Scholar] [CrossRef]
- Ambikapathy, B.; Krishnamurthy, K. Mathematical Modelling to Assess the Impact of Lockdown on COVID-19 Transmission in India: Model Development and Validation. JMIR Public Health Surveill. 2020, 6, e19368. [Google Scholar] [CrossRef]
- Ghosh, P.; Ghosh, R.; Chakraborty, B. COVID-19 in India: Statewise Analysis and Prediction. JMIR Public Health Surveill. 2020, 6, e20341. [Google Scholar] [CrossRef]
- Malavika, B.; Marimuthu, S.; Joy, M.; Nadaraj, A.; Asirvatham, E.S.; Jeyaseelan, L. Forecasting COVID-19 epidemic in India and high incidence states using SIR and logistic growth models. Clin. Epidemiol. Glob. Health 2021, 9, 26–33. [Google Scholar] [CrossRef]
- Chaturvedi, D.; Chakravarty, U. Predictive analysis of COVID-19 eradication with vaccination in India, Brazil, and U.S.A. Infect. Genet. Evol. 2021, 92, 104834. [Google Scholar] [CrossRef]
- Avhad, A.S.; Sutar, P.P.; Mohite, O.T.; Pawar, V.S. On the COVID-19 Pandemic in Indian State of Maharashtra: Forecasting & Effect of different parameters. medRxiv 2020. [Google Scholar] [CrossRef]
- Mangla, S.; Pathak, A.K.; Arshad, M.; Haque, U. Short-term forecasting of the COVID-19 outbreak in India. Int. Health 2021, 13, 410–420. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Wahl, B.; Dudala, S.R.; Gopal, K.; Mohan, B.C.; Neelima, S.; Jawahar Reddy, K.S.; Radhakrishnan, J.; Lewnard, J.A. Epidemiology and transmission dynamics of COVID-19 in two Indian states. Science 2020, 370, 691–697. [Google Scholar] [CrossRef]
- Bhardwaj, S.D.; Choudhary, M.L.; Gurav, Y.K.; Abraham, P.; Potdar, V.A. Epidemiological characterization of COVID-19—Pune, 2020-2021. Indian J. Med. Res. 2021, 153, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Gajbhiye, R.K.; Mahajan, N.N.; Waghmare, R.B.; Zala, S.; Chaaithanya, I.K.; Kuppusamy, P.; Bhurke, A.V.; Pious, M.; Surve, S.; Modi, D.N.; et al. Clinical characteristics, outcomes, & mortality in pregnant women with COVID-19 in Maharashtra, India: Results from PregCOVID registry. Indian J. Med. Res. 2021, 153, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Bherwani, H.; Gupta, A.; Anjum, S.; Anshul, A.; Kumar, R. Exploring dependence of COVID-19 on environmental factors and spread prediction in India. NPJ Clim. Atmos. Sci. 2020, 3, 38. [Google Scholar] [CrossRef]
- Gautam, S. The Influence of COVID-19 on Air Quality in India: A Boon or Inutile. Bull. Environ. Contam. Toxicol. 2020, 104, 724–726. [Google Scholar] [CrossRef]
- Ravindra, K.; Singh, T.; Biswal, A.; Singh, V.; Mor, S. Impact of COVID-19 lockdown on ambient air quality in megacities of India and implication for air pollution control strategies. Environ. Sci. Pollut. Res. Int. 2021, 28, 21621–21632. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, P.K.; Mangla, S.; Pathak, A.K.; Salãmao, G.N.; Sarkar, D. Pre-to-post lockdown impact on air quality and the role of environmental factors in spreading the COVID-19 cases—A study from a worst-hit state of India. Int. J. Biometeorol. 2020, 65, 205–222. [Google Scholar] [CrossRef]
- Shewale, S.P.; Sane, S.S.; Ujagare, D.D.; Patel, R.; Roy, S.; Juvekar, S.; Kohli, R.; Bangar, S.; Jadhav, A.; Sahay, S. Social Factors Associated With Adherence to Preventive Behaviors Related to COVID-19 Among Rural and Semi-urban Communities in Western Maharashtra, India. Front. Public Health 2021, 9, 722621. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S. Use of cluster analysis to monitor novel coronavirus-19 infections in Maharashtra, India. Indian J. Med. Sci. 2020, 72, 44–48. [Google Scholar] [CrossRef]
- Acharya, R.; Porwal, A. A vulnerability index for the management of and response to the COVID-19 epidemic in India: An ecological study. Lancet Glob. Health 2020, 8, e1142–e1151. [Google Scholar] [CrossRef]
- Mishra, S.V.; Gayen, A.; Haque, S.M. COVID-19 and urban vulnerability in India. Habitat. Int. 2020, 103, 102230. [Google Scholar] [CrossRef]
- Tamrakar, V.; Srivastava, A.; Saikia, N.; Parmar, M.C.; Shukla, S.K.; Shabnam, S.; Boro, B.; Saha, A.; Debbarma, B. District level correlates of COVID-19 pandemic in India during March-October 2020. PLoS ONE 2021, 16, e0257533. [Google Scholar] [CrossRef] [PubMed]
- Padhi, A.; Pradhan, S.; Sahoo, P.P.; Suresh, K.; Behera, B.K.; Panigrahi, P.K. Studying the effect of lockdown using epidemiological modelling of COVID-19 and a quantum computational approach using the Ising spin interaction. Sci. Rep. 2020, 10, 21741. [Google Scholar] [CrossRef]
- Ray, D.; Salvatore, M.; Bhattacharyya, R.; Wang, L.; Du, J.; Mohammed, S.; Purkayastha, S.; Halder, A.; Rix, A.; Barker, D.; et al. Predictions, role of interventions and effects of a historic national lockdown in India’s response to the COVID-19 pandemic: Data science call to arms. Harv. Data Sci. Rev. 2020, 176, 139–148. [Google Scholar] [CrossRef]
- Agrawal, M.; Kanitkar, M.; Vidyasagar, M. Modelling the spread of SARS-CoV-2 pandemic—Impact of lockdowns & interventions. Indian J. Med. Res. 2021, 153, 175. [Google Scholar] [CrossRef]
- Sahoo, B.K.; Sapra, B.K. A data driven epidemic model to analyse the lockdown effect and predict the course of COVID-19 progress in India. Chaos Solitons Fractals 2020, 139, 110034. [Google Scholar] [CrossRef] [PubMed]
- Sardar, T.; Nadim, S.S.; Rana, S.; Chattopadhyay, J. Assessment of lockdown effect in some states and overall India: A predictive mathematical study on COVID-19 outbreak. Chaos Solitons Fractals 2020, 139, 110078. [Google Scholar] [CrossRef]
- Singh, B.P.; Singh, G. Modeling tempo of COVID-19 pandemic in India and significance of lockdown. J. Public Aff. 2020, 20, e2257. [Google Scholar] [CrossRef]
- Saha, J.; Barman, B.; Chouhan, P. Lockdown for COVID-19 and its impact on community mobility in India: An analysis of the COVID-19 Community Mobility Reports, 2020. Child. Youth Serv. Rev. 2020, 116, 105160. [Google Scholar] [CrossRef]
- Singh, B.B.; Lowerison, M.; Lewinson, R.T.; Vallerand, I.A.; Deardon, R.; Gill, J.P.S.; Singh, B.; Barkema, H.W. Public health interventions slowed but did not halt the spread of COVID-19 in India. Transbound. Emerg. Dis. 2021, 68, 2171–2187. [Google Scholar] [CrossRef]
- Kishore, K.; Jaswal, V.; Verma, M.; Koushal, V. Exploring the Utility of Google Mobility Data During the COVID-19 Pandemic in India: Digital Epidemiological Analysis. JMIR Public Health Surveill. 2021, 7, e29957. [Google Scholar] [CrossRef]
- Nanda, D.; Mishra, D.R.; Swain, D. COVID-19 lockdowns induced land surface temperature variability in mega urban agglomerations in India. Environ. Sci. Process Impacts 2021, 23, 144–159. [Google Scholar] [CrossRef] [PubMed]
- Pal, S.C.; Chowdhuri, I.; Saha, A.; Chakrabortty, R.; Roy, P.; Ghosh, M.; Shit, M. Improvement in ambient-air-quality reduced temperature during the COVID-19 lockdown period in India. Environ. Dev. Sustain. 2021, 23, 9581–9608. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Zhang, M.; Anshika; Gao, J.; Zhang, H.; Kota, S.H. Effect of restricted emissions during COVID-19 on air quality in India. Sci. Total Environ. 2020, 728, 138878. [Google Scholar] [CrossRef] [PubMed]
- Venter, Z.S.; Aunan, K.; Chowdhury, S.; Lelieveld, J. Air pollution declines during COVID-19 lockdowns mitigate the global health burden. Environ. Res. 2021, 192, 110403. [Google Scholar] [CrossRef] [PubMed]
- Irudaya Rajan, S.; Sivakumar, P.; Srinivasan, A. The COVID-19 Pandemic and Internal Labour Migration in India: A ‘Crisis of Mobility’. Indian J. Labour Econ. 2020, 63, 1021–1039. [Google Scholar] [CrossRef]
- Mukhra, R.; Krishan, K.; Kanchan, T. COVID-19 Sets off Mass Migration in India. Arch. Med. Res. 2020, 51, 736–738. [Google Scholar] [CrossRef]
- Panneer, S.; Kantamaneni, K.; Akkayasamy, V.S.; Susairaj, A.X.; Panda, P.K.; Acharya, S.S.; Rice, L.; Liyanage, C.; Pushparaj, R.R.B. The Great Lockdown in the Wake of COVID-19 and Its Implications: Lessons for Low and Middle-Income Countries. Int. J. Environ. Res. Public Health 2022, 19, 610. [Google Scholar] [CrossRef]
- Bajiya, V.P.; Bugalia, S.; Tripathi, J.P.; Martcheva, M. Deciphering the transmission dynamics of COVID-19 in India: Optimal control and cost effective analysis. J. Biol. Dyn. 2022, 16, 665–712. [Google Scholar] [CrossRef]
- Mandal, S.; Das, H.; Deo, S.; Arinaminpathy, N. When to relax a lockdown? A modelling-based study of testing-led strategies coupled with sero-surveillance against SARS-CoV-2 infection in India. medRxiv 2020. [Google Scholar] [CrossRef]
- Prinja, S.; Bahuguna, P.; Chugh, Y.; Vassall, A.; Pandey, A.; Aggarwal, S.; Arora, N.K. A model based analysis for COVID-19 pandemic in India: Implications for health systems and policy for low-and middle-income countries. medRxiv 2020. [Google Scholar] [CrossRef]
- Van Damme, W.; Dahake, R.; Delamou, A.; Ingelbeen, B.; Wouters, E.; Vanham, G.; van de Pas, R.; Dossou, J.-P.; Ir, P.; Abimbola, S.; et al. The COVID-19 pandemic: Diverse contexts; different epidemics—How and why? BMJ Global Health 2020, 5, e003098. [Google Scholar] [CrossRef]
- COVID-19 INDIA TRACKER 2020. Available online: https://covid19tracker.in/ (accessed on 23 December 2020).
- MEDD-Maharashtra. REPORT OF COVID-19 CASES Date: 1 April 2020. 2020. Available online: https://drive.google.com/file/d/1JaPQjvL_H-k7hDkzuGkgzTuTXwJS8_wB/view (accessed on 23 December 2020).
- Churches, T. Tim Churches Health Data Science Blog: Analysing COVID-19 (2019-nCoV) Outbreak Data with R—Part 1; R Foundation: Vienna, Austria, 2020. [Google Scholar]
- Churches, T. Tim Churches Health Data Science Blog: Analysing COVID-19 (2019-nCoV) Outbreak Data with R—Part 2; R Foundation: Vienna, Austria, 2020. [Google Scholar]
- Jombart, T.; Kamvar, Z.N.; FitzJohn, R.; Cai, J.; Bhatia, S.; Schumacher, J.; Pulliam, J.R.C. Incidence: Compute, Handle, Plot and Model Incidence of Dated Events; R Package Version 1.7.1; R Foundation: Vienna, Austria, 2020. [Google Scholar]
- Wallinga, J.; Lipsitch, M. How generation intervals shape the relationship between growth rates and reproductive numbers. Proc. Biol. Sci. 2007, 274, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Jombart, T.; Cori, A. Epitrix: Small Helpers and Tricks for Epidemics Analysis; R Package Version 0.2.2; R Foundation: Vienna, Austria, 2019. [Google Scholar]
- Rajendrakumar, A.L.; Nair, A.T.N.; Nangia, C.; Chourasia, P.K.; Chourasia, M.K.; Syed, M.G.; Nair, A.S.; Nair, A.B.; Koya, M.S.F. Epidemic Landscape and Forecasting of SARS-CoV-2 in India. J. Epidemiol. Glob. Health 2021, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Cori, A.; Ferguson, N.M.; Fraser, C.; Cauchemez, S. A new framework and software to estimate time-varying reproduction numbers during epidemics. Am. J. Epidemiol. 2013, 178, 1505–1512. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.N.; Stockwin, J.E.; van Gaalen, R.D.; Polonsky, J.A.; Kamvar, Z.N.; Demarsh, P.A.; Dahlqwist, E.; Li, S.; Miguel, E.; Jombart, T.; et al. Improved inference of time-varying reproduction numbers during infectious disease outbreaks. Epidemics 2019, 29, 100356. [Google Scholar] [CrossRef]
- Saurabh, S.; Verma, M.K.; Gautam, V.; Kumar, N.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Misra, S. Transmission Dynamics of the COVID-19 Epidemic at the District Level in India: Prospective Observational Study. JMIR Public Health Surveill. 2020, 6, e22678. [Google Scholar] [CrossRef] [PubMed]
- Rai, B.; Shukla, A.; Dwivedi, L.K. Estimates of serial interval for COVID-19: A systematic review and meta-analysis. Clin. Epidemiol. Glob. Health 2021, 9, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Cori, A. EpiEstim: Estimate Time Varying Reproduction Numbers from Epidemic Curves; R Package Version 2.2-1; R Foundation: Vienna, Austria, 2019. [Google Scholar]
- Politis, M.D.; Hua, X.; Ogwara, C.A.; Davies, M.R.; Adebile, T.M.; Sherman, M.P.; Zhou, X.; Chowell, G.; Spaulding, A.C.; Fung, I.C. Spatially refined time-varying reproduction numbers of SARS-CoV-2 in Arkansas and Kentucky and their relationship to population size and public health policy, March—November 2020. Ann. Epidemiol. 2022, 68, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Jombart, T.; Nouvellet, P. Projections: Project Future Case Incidence; R Package Version 0.3.1; R Foundation: Vienna, Austria, 2018. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing, 4.0.3 (2020-10-10)—“Bunny-Wunnies Freak Out”; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Singh, P.; Brahma, D.; Chakraborty, S. COVID-19 | Does India Have Enough Doctors? An Analysis of Growing COVID-19 Patients and Existing Medical Capacity; The Brookings Institution: New Delhi, India, 2020. [Google Scholar]
- MEDD-Maharashtra. REPORT OF COVID-19 CASES Date: 15 April 2020. 2020. Available online: https://drive.google.com/file/d/1JaPQjvL_H-k7hDkzuGkgzTuTXwJS8_wB/view (accessed on 23 December 2020).
- MEDD-Maharashtra. REPORT OF COVID-19 CASES Date: 12 May 2020. 2020. Available online: https://drive.google.com/file/d/1JaPQjvL_H-k7hDkzuGkgzTuTXwJS8_wB/view (accessed on 25 December 2020).
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; CA, B.P.; Group, C.W.; Jombart, T.; Procter, S.R.; Knight, G.M. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 270. [Google Scholar] [CrossRef]
- DES-Maharashtra. Economic Survey of Maharashtra 2018-19; Directorate of Economics and Statistics, Planning Department, Government of Maharashtra: Mumbai, India, 2019.
- Asaria, M.; Mazumdar, S.; Chowdhury, S.; Mazumdar, P.; Mukhopadhyay, A.; Gupta, I. Socioeconomic inequality in life expectancy in India. BMJ Global Health 2019, 4, e001445. [Google Scholar] [CrossRef]
- Public Health Department Govt. of Maharashtra. Corona Guidelines Notification Dated 14th March 2020. 2020. Available online: https://pune.gov.in/corona-virus-updates/ (accessed on 23 December 2020).
- European Centre for Disease Prevention Control. Personal protective equipment (PPE) needs in healthcare settings for the care of patients with suspected or confirmed 2019-nCoV. ECDC: Stockholm; 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/novel-coronavirus-personal-protective-equipment-needs-healthcare-settings.pdf (accessed on 26 December 2020).
- ET Online. The costs of hospitalisation for COVID-19. The Economic Times, 23 April 2020; p. 8. [Google Scholar]
- Agrawal, A.; Gandhe, M.B.; Gandhe, S.; Agrawal, N. Study of length of stay and average cost of treatment in Medicine Intensive Care Unit at tertiary care center. J. Health Res. Rev. 2017, 4, 24. [Google Scholar] [CrossRef]
- Mirror Online. COVID-19 treatment: Maharashtra caps per day private hospital charges. Mumbai Mirror, 21 July 2020; p. 14. [Google Scholar]
- Chakraborty, R. Mumbai News: Maharashtra government puts price cap on private hospitals for COVID treatment. Hindustan Times, 21 July 2020; p. 5. [Google Scholar]
- Patel, H.B.; Bhatt, R.; Patel, H.Y.; Singh, S.; Raval, D. Contact tracing during COVID-19 pandemic: Ahmedabad Rural. Int. J. Dent. Med. Sci. Res. (IJDMSR) 2020, 4, 45–51. [Google Scholar]
- Disaster management Division-MoHA, I. Items and Norms of assistance from the State Disaster Response Fund (SDRF) in wake of COVID-19 Virus Outbreak Letter 14 March 2020. 2020. Available online: https://www.ndmindia.nic.in/images/gallery/Items%20and%20%20norms%20(14.07.2020).PDF (accessed on 25 December 2020).
- Thomas, T.; Majumdar, R. Coronavirus update: Maharashtra allocates ₹45 crore to fight COVID-19 as cases rise to 39. Mint, 16 March 2020; p. 41. [Google Scholar]
- MoHFW, G. COVID-19 Cases: 17th Lok Sabha Unstarred Question No. 966 to be answered on 18th September, 2020. 2020. Available online: https://sansad.in/ls/questions/questions-and-answers (accessed on 28 December 2020).
- Disaster management Division-MoHA, I. Advance release of Central share from State Disaster Risk Management Fund (SDRMF) for the year 2020-21 Letter 3rd April 2020. 2020. Available online: https://www.ndmindia.nic.in/images/gallery/SDRMF%20.pdf (accessed on 25 December 2020).
- PTI. Maharashtra CM fund receives Rs 342 cr in donations till mid-May; Rs 23 cr spent on COVID-19, Rs 55 cr on migrant fare, reveals RTI query. Firstpost, 2 June 2020; p. 18. [Google Scholar]
- Directorate of Economics and Statistics. Economic survey of Maharashtra 2019–20. 2020. Available online: https://mahades.maharashtra.gov.in/files/publication/ESM_2019_20_Eng_Book.pdf (accessed on 28 December 2020).
- Hutubessy, R.; Chisholm, D.; Edejer, T.T.-T. Generalized cost-effectiveness analysis for national-level priority-setting in the health sector. Cost. Eff. Resour. Alloc. 2003, 1, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pichon-Riviere, A.; Drummond, M.; Palacios, A.; Garcia-Marti, S.; Augustovski, F. Determining the efficiency path to universal health coverage: Cost-effectiveness thresholds for 174 countries based on growth in life expectancy and health expenditures. Lancet Glob. Health 2023, 11, e833–e842. [Google Scholar] [CrossRef]
- Bertram, M.Y.; Lauer, J.A.; De Joncheere, K.; Edejer, T.; Hutubessy, R.; Kieny, M.-P.; Hill, S.R. Cost–effectiveness thresholds: Pros and cons. Bull. World Health Organ. 2016, 94, 925. [Google Scholar] [CrossRef]
- Alfano, V.; Ercolano, S. Stay at Home! Governance Quality and Effectiveness of Lockdown. Soc. Indic. Res. 2022, 159, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Yanovskiy, M.; Socol, Y. Are Lockdowns Effective in Managing Pandemics? Int. J. Environ. Res. Public Health 2022, 19, 9295. [Google Scholar] [CrossRef]
- Marcu, S. Towards Sustainable Mobility? The Influence of the COVID-19 Pandemic on Romanian Mobile Citizens in Spain. Sustainability 2021, 13, 4023. [Google Scholar] [CrossRef]
- Long, E.; Patterson, S.; Maxwell, K.; Blake, C.; Pérez, R.B.; Lewis, R.; McCann, M.; Riddell, J.; Skivington, K.; Wilson-Lowe, R. COVID-19 pandemic and its impact on social relationships and health. J. Epidemiol. Community Health 2022, 76, 128–132. [Google Scholar] [CrossRef]
- Paliath, S. A Year After Exodus, No Reliable Data Or Policy On Migrant Workers. IndiaSpend, 21 March 2021; p. 25. [Google Scholar]
- Azad, S.; Devi, S. Tracking the spread of COVID-19 in India via social networks in the early phase of the pandemic. J. Travel. Med. 2020, 27, taaa130. [Google Scholar] [CrossRef]
- Chakravarti, I. Coronavirus: VIP privilege is hampering India’s fight against COVID-19. Scroll, 21 March 2020; p. 34. [Google Scholar]
- Cheung, H. Coronavirus: What could the West learn from Asia. BBC News, 21 March 2020; p. 1. [Google Scholar]
- Huang, Y.; Sun, M.; Sui, Y. How digital contact tracing slowed COVID-19 in East Asia. Harvard Business Review, 15 April 2020; p. 10. [Google Scholar]
- Summers, J.; Cheng, H.-Y.; Lin, H.-H.; Barnard, L.T.; Kvalsvig, A.; Wilson, N.; Baker, M.G. Potential lessons from the Taiwan and New Zealand health responses to the COVID-19 pandemic. Lancet Reg. Health-West. Pac. 2020, 4, 100044. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–21. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef] [PubMed]
- Murhekar, M.V.; Bhatnagar, T.; Selvaraju, S.; Rade, K.; Saravanakumar, V.; Vivian Thangaraj, J.W.; Kumar, M.S.; Shah, N.; Sabarinathan, R.; Turuk, A.; et al. Prevalence of SARS-CoV-2 infection in India: Findings from the national serosurvey, May-June 2020. Indian J. Med. Res. 2020, 152, 48–60. [Google Scholar] [CrossRef]
- Reuters. Millions of COVID-19 cases went undetected in India, research paper estimates. The Economic Times, 11 September 2020; p. 23. [Google Scholar]
- Hamidi, S.; Sabouri, S.; Ewing, R. Does density aggravate the COVID-19 pandemic? Early findings and lessons for planners. J. Am. Plan. Assoc. 2020, 86, 495–509. [Google Scholar] [CrossRef]
- Carozzi, F.; Provenzano, S.; Roth, S. Urban Density and COVID-19 (No. 13440). IZA Discussion Papers. 2020. Available online: https://www.iza.org/publications/dp/13440/urban-density-and-covid-19 (accessed on 21 January 2021).
- Bhadra, A.; Mukherjee, A.; Sarkar, K. Impact of population density on COVID-19 infected and mortality rate in India. Model. Earth Syst. Environ. 2021, 7, 623–629. [Google Scholar] [CrossRef]
- Gupta, A.; Banerjee, S.; Das, S. Significance of geographical factors to the COVID-19 outbreak in India. Model. Earth Syst. Environ. 2020, 6, 2645–2653. [Google Scholar] [CrossRef]
- Vinchurkar, S.; Jain, N.; Punamiya, V. Exploratory Analysis of Demographic Factors and the Temporal Evolution of COVID-19 in India. J. Epidemiol. Glob. Health 2021, 11, 10–14. [Google Scholar] [CrossRef]
- Debroy, S. COVID-19: Maharashtra testing 5 high-risk and 10 low-risk contacts per patient. The Times of India, 14 September 2020; p. 7. [Google Scholar]
- Singh, L.; Barnagarwala, T. Contact tracing: How Mumbai lost the momentum. The Indian Express, 28 May 2020; p. 6. [Google Scholar]
- Desk, L.E. BMC to increase contact tracing in city from 1:10 ratio to 1:15. Lokmat English, 17 June 2020; p. 11. [Google Scholar]
- Bhalerao, S. A fifth of COVID-19 patients in Maharashtra had no contact history. The Indian Express, 1 April 2020; p. 5. [Google Scholar]
- Ashar, S.A. Quarantine challenge: How wards in Mumbai are contact tracing. The Indian Express, 27 April 2020; p. 17. [Google Scholar]
- Jog, S. Coronavirus in Maharashtra: Poor record in contact tracing; Less than 10 contacts of patients traced in 31 districts. Free Press J. 2020. Available online: https://www.freepressjournal.in/mumbai/coronavirus-in-maharashtra-poor…tact-tracing-less-than-10-contacts-of-patients-traced-in-31-districts (accessed on 21 January 2021).
- The Lancet. India under COVID-19 lockdown. Lancet 2020, 395, 1315. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Input Parameters | Unit Values | Calculation Notes |
|---|---|---|
| Probability of hospitalization after COVID-19 infection [99] | 0.15 | |
| Probability of ICU care after COVID-19 infection [100,101] | 0.02 | Based on MEDD reports published on 15 April 2020 and 12 May 2020. |
| Number of deaths due to COVID-19/probability of death [100] | 0.04 | Based on MEDD Report 15 April 2020 fig16 |
| Average length of stay for non-ICU hospitalization (Sensitivity analysis range 4–21 days) [102] | 14 days | Authors’ assumption based on treatment and quarantine guidelines of that time. Range 4–21 days used for sensitivity analysis. |
| Average length of stay for ICU [102] (range 4–19 days) | 7 days * | A range of 4–19 days was used in sensitivity analysis. |
| Average length of stay for ICU patient in general ward post ICU care (range 3–10 days) | 7 days * | Authors’ assumption. |
| Income per capita/year for Maharashtra state [103] | 191,827 (INR) | Estimated annual per capita income as per the report for the year 2020. |
| Average daily wage | 761.218254 (INR) | Working days in 2018–2019 from 1 April to 31 March = 252 days used to calculate daily per capita wage from annual estimates. |
| Average life expectancy [104] | 68.3 yrs. | |
| Average age of dying due to COVID19 | 58 yrs. | Authors’ calculations based on table-4 of MEDD report published on 15 April 2020. |
| Number of years of potential life lost | 10.3 yrs. | Subtracting average age of dying from average life expectancy |
| Average days of quarantine [105] | 14 days | A range of 7–21 days used for sensitivity analysis. |
| Number of PPE required per patient per day [106] | 15 | As per estimates from European CDC |
| Cost of PPE (range 750–1000 INR) [107] | 750 (INR) | A range of INR 500–1000 used for sensitivity analysis |
| Cost of Inpatient medicine (daily) [107] | 1000 (INR) | |
| Cost of Outpatient medicine (for entire period) | 500 (INR) | Authors’ assumption |
| Cost of test kit/test [107] | 4500 (INR) | |
| Cost of ICU care (per day) [108,109,110] (range 7500–9000 INR) | 8825 (INR) | This figure is based on per day ICU stay cost including ventilator support for COPD patient. For sensitivity analysis range is used. |
| Non-ICU General ward bed charges [109,110] | 4000 (INR) | |
| Loss of income (for 14 day) | 10,657 (INR) | Average daily wage X Average days of quarantine |
| Loss of income due to premature death | 1,975,818.1 (INR) | Number of years of potential life loss X Income per capita per year for Maharashtra state |
| Phase | Case Doubling Rate in Days # | Median Reproduction Number (R0) # |
|---|---|---|
| Pre-lockdown (9–24 March) | 17.78 (5.61, −15.19) | 1.14 (0.85, 1.45) |
| Lockdown-1 (25 March–14 April) | 3.87 (3.15, 5.00) | 1.67 (1.50, 1.82) |
| Lockdown-2 (15 April–3 May) | 10.37 (7.10, 19.30) | 1.24 (1.12, 1.35) |
| Lockdown-3 (4–17 May) | 20.31 (10.70, 212.50) | 1.12 (1.01, 1.23) |
| Lockdown-4 (18–31 May) | 45.56 (20.50, −204.52) | 1.05 (0.99, 1.12) |
| Case Categories and Estimated Costs | Projected | Actual |
|---|---|---|
| Total cases for the projected period | 631,891 | 64,975 |
| Hospitalized individuals | 94,784 | 9746 |
| Individuals admitted to ICU | 12,638 | 1300 |
| Total number of deaths | 25,276 | 2108 |
| Isolated infected individuals | 499,194 | 53,929 |
| Number of premature deaths | 21,138 | 1763 |
| Total contacts quarantine/isolated | 12,637,820 | 1,299,500 |
| Direct Cost due to hospitalization * | ||
| ICU patient cost | 3472.56 | 357.07 |
| Non-ICU patient cost | 22,842.86 | 2348.85 |
| Testing and Medicine cost for isolated cases | 6988.71 | 755.01 |
| Sub-Total | 33,304.13 | 3460.93 |
| Indirect Cost * | ||
| Loss of wages for ICU patients | 134.68 | 13.85 |
| Loss of wages for hospitalized non-ICU patients | 1010.11 | 103.87 |
| Loss of wages for isolated cases | 5319.94 | 574.73 |
| Loss of total yearly wages due to premature death | 41,764.88 | 3483.21 |
| Loss of wages for exposed contacts/individuals | 134,681.95 | 13,848.84 |
| Sub-Total | 182,911.56 | 18,024.50 |
| Govt. of Maharashtra’s fund allocation/expenditure for COVID-19 pandemic * | 15,470.03 | |
| Total * | 231,685.72 | 36,955.45 |
| Value of averted cases * | 194,730.27 | |
| (2.60 billion USD) # | ||
| Cost Savings | 84.05% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ambade, P.N.; Thavorn, K.; Pakhale, S. COVID-19 Pandemic: Did Strict Mobility Restrictions Save Lives and Healthcare Costs in Maharashtra, India? Healthcare 2023, 11, 2112. https://doi.org/10.3390/healthcare11142112
Ambade PN, Thavorn K, Pakhale S. COVID-19 Pandemic: Did Strict Mobility Restrictions Save Lives and Healthcare Costs in Maharashtra, India? Healthcare. 2023; 11(14):2112. https://doi.org/10.3390/healthcare11142112
Chicago/Turabian StyleAmbade, Preshit Nemdas, Kednapa Thavorn, and Smita Pakhale. 2023. "COVID-19 Pandemic: Did Strict Mobility Restrictions Save Lives and Healthcare Costs in Maharashtra, India?" Healthcare 11, no. 14: 2112. https://doi.org/10.3390/healthcare11142112