

Portuguese Validation of the Unified Theory of Acceptance and Use of Technology Scale (UTAUT) to a COVID-19 Mobile Application: A Pilot Study

Abstract
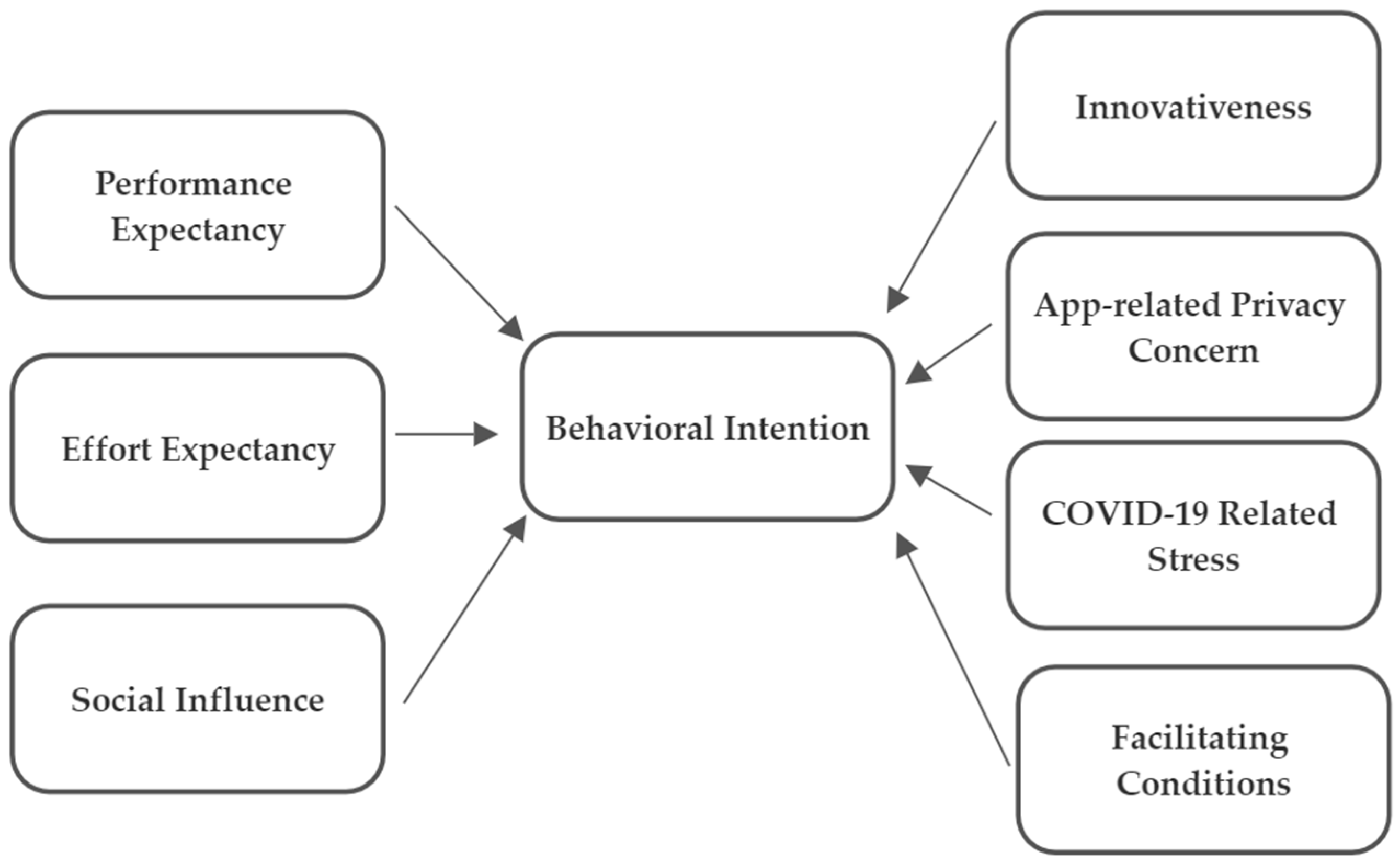
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Ethical Considerations
2.3. Questionnaire
2.4. Translation Process
- Forward translation: the scale was independently translated into Portuguese European language by four native speakers of Portuguese who were fluent in English.
- Reconciliation: the four versions were compared, and a single version was produced.
- Blind back-translation: the previous version was subjected to a back-translation. It was explained to the translator the study’s objectives without showing the original questionnaire.
- Preliminary version: the versions obtained in the second and third steps were compared, and a preliminary version was created.
- Pre-test: the questionnaire obtained in the fourth step was subjected to a pre-test to identify possible semantics errors and ambiguous questions. A total of 5 individuals from the general population participated in the pre-test: 3 men and 2 women, aged between 18 and 45. Most participants indicated that some consecutive items seemed to have the same meaning. Therefore, to reduce this ambiguity, we randomly ordered the sentences. The participants also suggested eliminating the pronouns from the sentences so that reading becomes less tiring. Corrections were made, and the final questionnaire was obtained (Table 1).
2.5. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Reliability
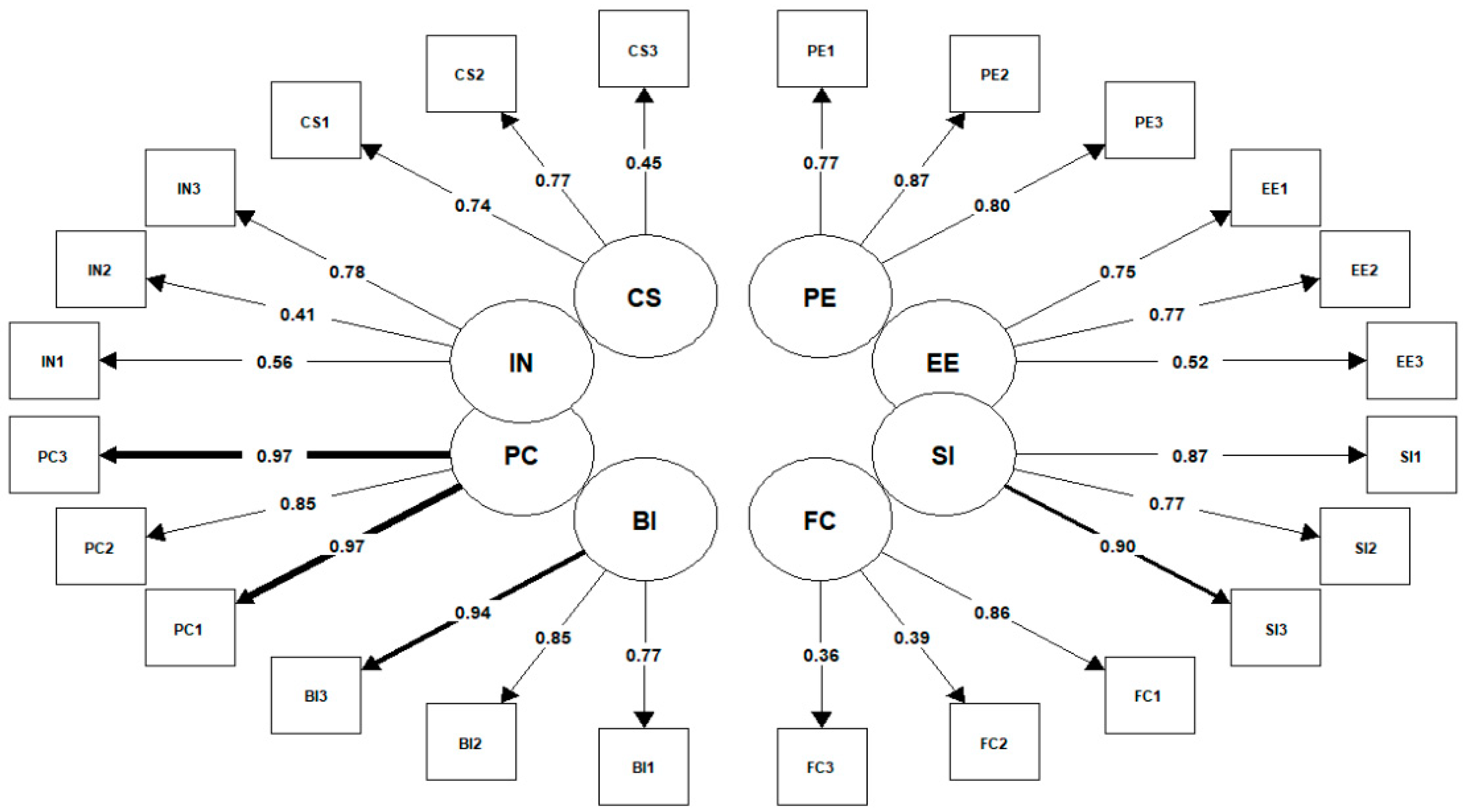
3.3. Validity
3.4. Goodness of Fit Indices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- OECD/European Union. Health at a Glance: Europe 2022: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2022. [Google Scholar] [CrossRef]
- Walrave, M.; Waeterloos, C.; Ponnet, K. Ready or Not for Contact Tracing? Investigating the Adoption Intention of COVID-19 Contact-Tracing Technology Using an Extended Unified Theory of Acceptance and Use of Technology Model. Cyberpsychol. Behav. Soc. Netw. 2020, 24, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Portugal In. Tech Innovation Hub. Available online: http://www.portugalin.gov.pt/innovation/ (accessed on 24 December 2021).
- Instituto Nacional de Estatística. Portal do INE—Proporção de Agregados Domésticos Privados com Pelo Menos um Indivíduo com Idade Entre 16 e 74 Anos e com Ligação à Internet em Casa. 2020. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&indOcorrCod=0001031&contexto=bd&selTab=tab2 (accessed on 3 January 2021).
- Global Change Data Lab. Our World in Data. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer (accessed on 24 December 2021).
- Kukuk, L. Analyzing Adoption of COVID-19 Contact Tracing Apps Using UTAUT. Bachelor’s Thesis, University of Twente, Faculty of Electrical Engineering, Mathematics and Computer Science, Enschede, The Netherlands, 2020; pp. 1–8. Available online: http://essay.utwente.nl/81983/1/Kukuk_BA_EEMCS.pdf (accessed on 12 January 2021).
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User Acceptance of Information Technology: Toward a Unified View. Manag. Inf. Syst. Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Zhang, R.; Zhu, X. An empirical study on patients’ acceptance of physician-patient interaction in online Health Communities. Int. J. Environ. Res. Public Health 2019, 16, 5084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naranjo-Zolotov, M.; Oliveira, T.; Casteleyn, S. Citizens’ intention to use and recommend e-participation: Drawing upon UTAUT and citizen empowerment. Inf. Technol. People 2019, 32, 364–386. [Google Scholar] [CrossRef] [Green Version]
- LeRouge, C.M.; Hah, H.; Deckard, G.J.; Jiang, H. Designing for the Co-use of consumer health technology in self-management of adolescent overweight and obesity: Mixed methods qualitative study. JMIR mHealth uHealth 2020, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Dar, A.; Lone, A.; Zahoor, S.; Khan, A.; Naaz, R. Applicability of mobile contact tracing in fighting pandemic (COVID-19): Issues, challenges and solutions. Comput. Sci. Rev. 2020, 38, 100307. [Google Scholar] [CrossRef] [PubMed]
- Westcott, R.; Ronan, K.; Bambrick, H.; Taylor, M. Expanding protection motivation theory: Investigating an application to animal owners and emergency responders in bushfire emergencies. BMC Psychol. 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Vijver, F.; Hambleton, R.K. Translating Tests: Some Practical Guidelines. Eur. Psychol. 2006, 1, 89–99. [Google Scholar] [CrossRef]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Bolarinwa, O.A. Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger. Postgrad. Med. J. 2015, 22, 195–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Child, D. The Essentials of Factor Analysis, 3rd ed.; Continuum: London, UK, 2006. [Google Scholar]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef] [Green Version]
- Green, S.B.; Lissitz, R.W.; Mulaik, S.A. Limitations of coefficient alpha as an index of test unidimensionality. Educ. Psychol. Meas. 1977, 37, 827–838. [Google Scholar] [CrossRef]
- Niemand, T.; Mai, R. Flexible cutoff values for fit indices in the evaluation of structural equation models. J. Acad. Mark. Sci. 2018, 46, 1148–1172. [Google Scholar] [CrossRef]
- Saris, W.E.; Gallhofer, I.N. Design, Evaluation, and Analysis of Questionnaires for Survey Research, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 60–65. ISBN 9781118634646. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural Equation Modelling: Guidelines for Determining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Chi-square for model fit in confirmatory factor analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Apolinário-Hagen, J.; Menzel, M.; Hennemann, S.; Salewski, C. Acceptance of Mobile Health Apps for Disease Management Among People with Multiple Sclerosis: Web-Based Survey Study. JMIR Form. Res. 2018, 2, e11977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paganin, G.; Apolinário-Hagen, J.; Simbula, S. Introducing mobile apps to promote the well-being of German and Italian university students. A cross-national application of the Technology Acceptance Model. Curr. Psychol. 2022, 27, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rosi, A.; Vugt, F.T.; Lecce, S.; Ceccato, I.; Vallarino, M.; Rapisarda, F.; Vecchi, T.; Cavallini, E. Risk Perception in a Real-World Situation (COVID-19): How It Changes from 18 to 87 Years Old. Front. Psychol. 2021, 12, 646558. [Google Scholar] [CrossRef] [PubMed]
- Franzen, A.; Wöhner, F. Fatigue during the COVID-19 pandemic: Evidence of social distancing adherence from a panel study of young adults in Switzerland. PLoS ONE 2021, 16, e0261276. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Construct | Item Code | Item |
|---|---|---|
| Performance expectancy | PE1 | Using the COVID-19 app will improve my knowledge about the hazard of being infected by COVID-19. |
| PE2 | I Consider the STAYAWAY COVID app would be helpful to evaluate the risks of contracting COVID-19. | |
| PE3 | By using the STAYAWAY COVID app can the infection rate of COVID-19 be limited. | |
| Effort expectancy | EE1 | Learning to use the STAYWAY COVID app, will be easy for me. |
| EE2 | The STAYWAY COVID app, would not be difficult for me to use. | |
| EE3 | I will rapidly be able to manage the STAYWAY COVID app. Using STAYWAY COVID app will be easy task for me. | |
| Social influence | SI1 | People that are important to me, think that I should use the STAYWAY COVID app. |
| SI2 | People that have influence over me, recommend that I use the STAYWAY COVID app. | |
| SI3 | People whom I value their opinion, recommend that I use the STAYWAY COVID app. | |
| Facilitating conditions | FC1 | I have the necessary knowledge to use the STAYWAY COVID app. |
| FC2 | I have the necessary resources to use the STAYWAY COVID app. | |
| FC3 | The STAYWAY COVID app is compatible with other apps on my smartphone. | |
| Behavioral intention | BI1 | I could be willing to use the STAYWAY COVID app. |
| BI2 | I plan on using the STAYWAY COVID app. | |
| BI3 | I want to use the STAYWAY COVID app in the future | |
| App-related privacy concerns | PC1 * | I am concerned over my privacy being exposed by the use of the STAYWAY COVID app. |
| PC2 * | Using the STAYWAY COVID app will make me uncomfortable regarding any privacy exposure. | |
| PC3 * | I would be worried over my privacy being breached by using the STAYWAY COVID app. | |
| Innovativeness | IN1 | People seek my advice on new technology. |
| IN2 | Usually/In general, on my social circle I am the first to acquire new technology when it comes out. | |
| IN3 | Usually, I can work out how to use new technology products without other’s help. | |
| COVID-19 related stress | CS1 | Even when I am busy with other things, I worry with the COVID-19 situation. |
| CS2 | The current COVID-19 situation/issue is very stressful for me. | |
| CS3 | I am worried with the consequences of the crises provoked by COVID-19 pandemic. |
| Frequency n = 1081 | (%) | ||
|---|---|---|---|
| Gender | Female | 768 | 71.0 |
| Male | 310 | 28.7 | |
| Other | 3 | 0.3 | |
| Age group | 16–24 | 640 | 59.2 |
| 25–34 | 155 | 14.3 | |
| 35–44 | 113 | 10.5 | |
| 45–54 | 96 | 8.9 | |
| 55–64 | 68 | 6.3 | |
| More than 65 | 9 | 0.8 | |
| Educational qualifications | High School or Technological/Vocational Courses | 381 | 35.2 |
| Bachelor’s degree | 445 | 41.2 | |
| Master’s degree | 145 | 13.4 | |
| PhD degree | 97 | 9.0 | |
| Other | 13 | 1.2 | |
| Occupation | Student | 845 | 78.2 |
| Teacher | 164 | 15.2 | |
| Other school staff | 72 | 6.7 |
| Construct | Item | Q1 | Median | Q3 | Factor Loadings (λij) | AVE | CR | Cronbach’s α |
|---|---|---|---|---|---|---|---|---|
| Behavioral intention (BI) | BI1 | 2 | 3 | 4 | 0.773 | 0.73 | 0.89 | 0.88 |
| BI2 | 1 | 2 | 3 | 0.852 | ||||
| BI3 | 1 | 2 | 3 | 0.936 | ||||
| Performance expectancy (PE) | PE1 | 1 | 2 | 3 | 0.774 | 0.67 | 0.86 | 0.86 |
| PE2 | 2 | 3 | 3 | 0.874 | ||||
| PE3 | 2 | 2 | 3 | 0.800 | ||||
| Effort expectancy (EE) | EE1 | 4 | 4 | 5 | 0.751 | 0.48 | 0.73 | 0.70 |
| EE2 | 4 | 4 | 5 | 0.773 | ||||
| EE3 | 3 | 4 | 5 | 0.516 | ||||
| Social influence (SI) | SI1 | 1 | 2 | 3 | 0.867 | 0.72 | 0.89 | 0.88 |
| SI2 | 1 | 2 | 3 | 0.771 | ||||
| SI3 | 1 | 2 | 3 | 0.903 | ||||
| Facilitating conditions (FC) | FC1 | 4 | 4 | 5 | 0.869 | 0.34 | 0.55 | 0.58 |
| FC2 | 3 | 4 | 5 | 0.368 | ||||
| FC3 | 3 | 4 | 5 | 0.337 | ||||
| Innovativeness (IN) | IN1 | 2 | 3 | 4 | 0.497 | 0.36 | 0.60 | 0.62 |
| IN2 | 1 | 2 | 3 | 0.341 | ||||
| IN3 | 3 | 4 | 5 | 0.853 | ||||
| App-related privacy concerns (PC) | PC1 | 2 | 3 | 4 | 0.967 | 0.87 | 0.95 | 0.95 |
| PC2 | 2 | 3 | 4 | 0.853 | ||||
| PC3 | 2 | 3 | 4 | 0.967 | ||||
| COVID-19-related stress (CS) | CS1 | 3 | 4 | 4 | 0.740 | 0.45 | 0.69 | 0.68 |
| CS2 | 3 | 4 | 4 | 0.765 | ||||
| CS3 | 4 | 5 | 5 | 0.452 |
| PE | EE | SI | FC | PC | IN | CS | BI | |
| PE | 0.817 | |||||||
| EE | 0.042 | 0.690 | ||||||
| SI | 0.555 *** | 0.028 | 0.849 | |||||
| FC | −0.110 ** | 0.930 *** | −0.035 | 0.582 | ||||
| PC | 0.095 ** | 0.228 *** | 0.059 † | 0.153 *** | 0.930 | |||
| IN | −0.012 | 0.665 *** | 0.045 | 0.652 *** | 0.065 † | 0.603 | ||
| CS | 0.208 *** | 0.113 ** | 0.219 *** | 0.035 | 0.005 | 0.032 | 0.668 | |
| BI | 0.753 *** | 0.040 | 0.545 *** | −0.087 * | 0.199 *** | −0.003 | 0.287 *** | 0.856 |
| Fit Index | Recommended Value [14,19] | Initial Model | Modified Model |
|---|---|---|---|
| χ2 | The lower its value, the better it is. | 835.915 | 208.032 |
| χ2/df | [2; 5]—Poor fit | 3.732 | 2.600 |
| CFI | ≥0.95—Very good fit | 0.955 | 0.988 |
| TLI | [0.9; 0.95]—Good fit ≥0.95—Very good fit | 0.944 | 0.984 |
| RMSEA | ≤0.05—Very good fit | 0.050 | 0.038 |
| SRMR | Values ≤ 0.08 are recommended | 0.060 | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araújo, I.; Grilo, A.; Silva, C. Portuguese Validation of the Unified Theory of Acceptance and Use of Technology Scale (UTAUT) to a COVID-19 Mobile Application: A Pilot Study. Healthcare 2023, 11, 1916. https://doi.org/10.3390/healthcare11131916
Araújo I, Grilo A, Silva C. Portuguese Validation of the Unified Theory of Acceptance and Use of Technology Scale (UTAUT) to a COVID-19 Mobile Application: A Pilot Study. Healthcare. 2023; 11(13):1916. https://doi.org/10.3390/healthcare11131916
Chicago/Turabian StyleAraújo, Ivandra, Ana Grilo, and Carina Silva. 2023. "Portuguese Validation of the Unified Theory of Acceptance and Use of Technology Scale (UTAUT) to a COVID-19 Mobile Application: A Pilot Study" Healthcare 11, no. 13: 1916. https://doi.org/10.3390/healthcare11131916