

Optimal Physical Activity Is Associated with the Reduction of Depressive Symptoms via Neuroticism and Resilience
 , , , and
, , , and
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects
2.2. Questionnaires
2.3. Physical Activity
2.4. Statistical Analysis
3. Results
3.1. Measured Variables
3.2. Association of PHQ-9 Scores with Demographic and Clinical Data and Questionnaire Data of the Study Population
3.3. Multiple Regression Analysis with PHQ-9 as the Dependent Variable
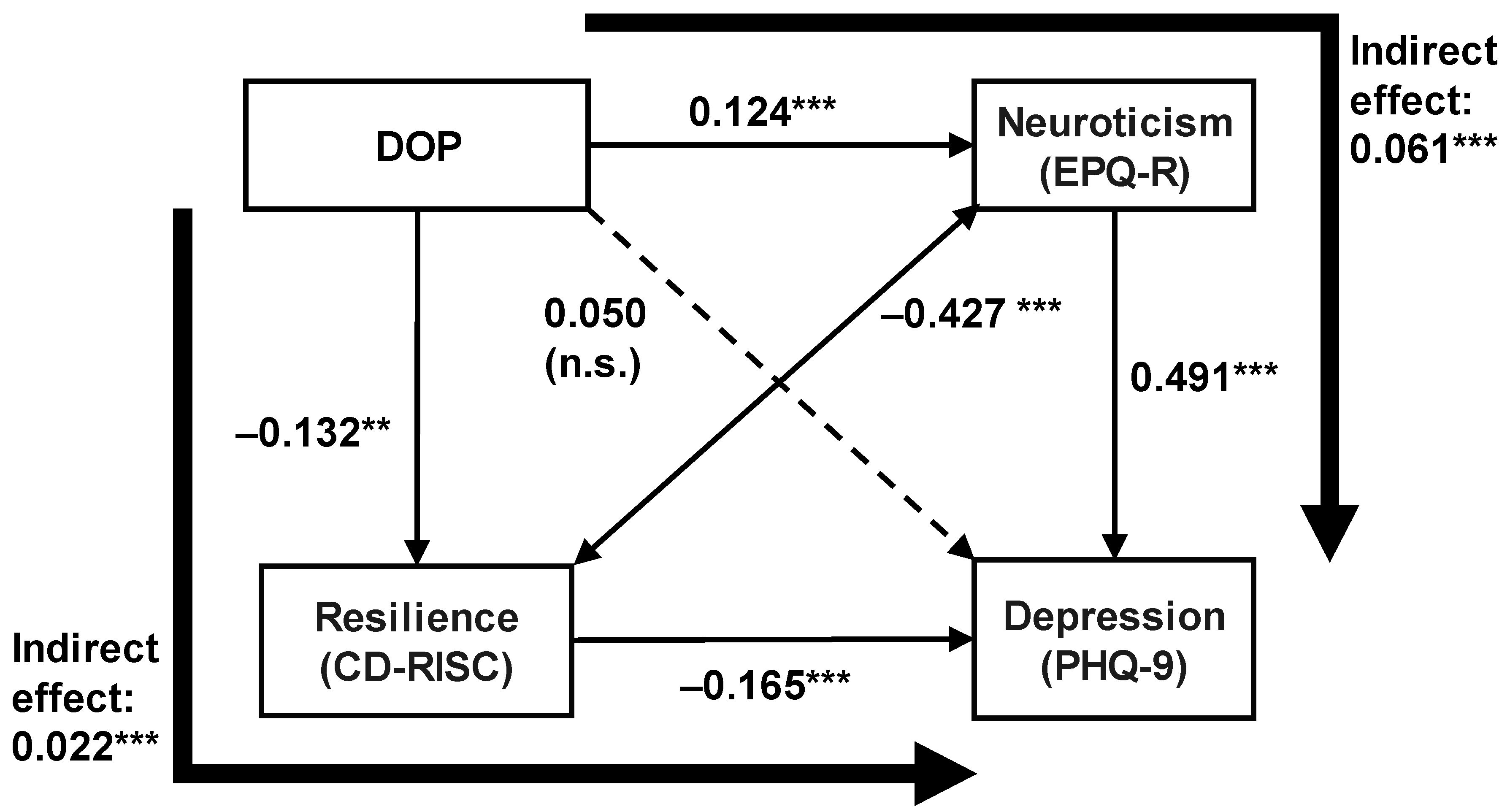
3.4. Analysis of the Path Model
4. Discussion
4.1. Resilience Mediates the Effect of Regular Physical Activity Habits on Depressive Symptoms
4.2. Neuroticism Mediates the Effect of Regular Physical Activity Habits on Depressive Symptoms
4.3. Interactions of Resilience and Neuroticism
4.4. Clinical Significance of the Results
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Panagiotakos, D.B.; Pitsavos, C.; Lentzas, Y.; Skoumas, Y.; Papadimitriou, L.; Zeimbekis, A.; Stefanadis, C. Determinants of physical inactivity among men and women from Greece: A 5-year follow-up of the ATTICA study. Ann. Epidemiol. 2008, 18, 387–394. [Google Scholar] [CrossRef]
- Bridle, C.; Spanjers, K.; Patel, S.; Atherton, N.M.; Lamb, S.E. Effect of exercise on depression severity in older people: Systematic review and meta-analysis of randomised controlled trials. Br. J. Psychiatry 2012, 201, 180–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Josefsson, T.; Lindwall, M.; Archer, T. Physical exercise intervention in depressive disorders: Meta-analysis and systematic review. Scand. J. Med. Sci. Sport. 2014, 24, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Zeeuw, E.L.; Tak, E.C.; Dusseldorp, E.; Hendriksen, I.J. Workplace exercise intervention to prevent depression: A pilot randomized controlled trial. Ment. Health Phys. Act. 2010, 3, 72–77. [Google Scholar] [CrossRef]
- Choi, K.W.; Chen, C.-Y.; Stein, M.B.; Klimentidis, Y.C.; Wang, M.-J.; Koenen, K.C.; Smoller, J.W. Assessment of bidirectional relationships between physical activity and depression among adults: A 2-sample mendelian randomization study. JAMA Psychiatry 2019, 76, 399–408. [Google Scholar] [CrossRef]
- Teychenne, M.; Ball, K.; Salmon, J. Physical activity and likelihood of depression in adults: A review. Prev. Med. 2008, 46, 397–411. [Google Scholar] [CrossRef]
- Southwick, S.M.; Bonanno, G.A.; Masten, A.S.; Panter-Brick, C.; Yehuda, R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatol. 2014, 5, 25338. [Google Scholar] [CrossRef] [Green Version]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Liu, W.J.; Zhou, L.; Wang, X.Q.; Yang, B.X.; Wang, Y.; Jiang, J.F. Mediating role of resilience in relationship between negative life events and depression among Chinese adolescents. Arch. Psychiatr. Nurs. 2019, 33, 116–122. [Google Scholar] [CrossRef]
- Havnen, A.; Anyan, F.; Hjemdal, O.; Solem, S.; Gurigard Riksfjord, M.; Hagen, K. Resilience moderates negative outcome from stress during the COVID-19 pandemic: A moderated-mediation approach. Int. J. Environ. Res. Public Health 2020, 17, 6461. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zhang, Y.; Huang, C.; Cui, Z. Resilience-oriented cognitive behavioral interventions for depressive symptoms in children and adolescents: A meta-analytic review. J. Affect. Disord. 2020, 270, 150–164. [Google Scholar] [CrossRef]
- Kermott, C.A.; Johnson, R.E.; Sood, R.; Jenkins, S.M.; Sood, A. Is higher resilience predictive of lower stress and better mental health among corporate executives? PLoS ONE 2019, 14, e0218092. [Google Scholar] [CrossRef] [Green Version]
- McCrae, R.R.; John, O.P. An introduction to the five-factor model and its applications. J. Personal. 1992, 60, 175–215. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association, D.; Association, A.P. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Kendler, K.S.; Kuhn, J.; Prescott, C.A. The interrelationship of neuroticism, sex, and stressful life events in the prediction of episodes of major depression. Am. J. Psychiatry 2004, 161, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Kendler, K.S.; Gardner, C.O. Sex differences in the pathways to major depression: A study of opposite-sex twin pairs. Am. J. Psychiatry 2014, 171, 426–435. [Google Scholar] [CrossRef] [Green Version]
- Ono, K.; Takaesu, Y.; Nakai, Y.; Shimura, A.; Ono, Y.; Murakoshi, A.; Matsumoto, Y.; Tanabe, H.; Kusumi, I.; Inoue, T. Associations among depressive symptoms, childhood abuse, neuroticism, and adult stressful life events in the general adult population. Neuropsychiatr. Dis. Treat. 2017, 13, 477–482. [Google Scholar] [CrossRef] [Green Version]
- Ono, Y.; Takaesu, Y.; Nakai, Y.; Ichiki, M.; Masuya, J.; Kusumi, I.; Inoue, T. The influence of parental care and overprotection, neuroticism and adult stressful life events on depressive symptoms in the general adult population. J. Affect. Disord. 2017, 217, 66–72. [Google Scholar] [CrossRef]
- Saklofske, D.H.; Austin, E.J.; Rohr, B.A.; Andrews, J.J. Personality, emotional intelligence and exercise. J. Health Psychol. 2007, 12, 937–948. [Google Scholar] [CrossRef]
- De Moor, M.H.; Beem, A.; Stubbe, J.H.; Boomsma, D.I.; De Geus, E.J. Regular exercise, anxiety, depression and personality: A population-based study. Prev. Med. 2006, 42, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Kroencke, L.; Harari, G.M.; Katana, M.; Gosling, S.D. Personality trait predictors and mental well-being correlates of exercise frequency across the academic semester. Soc. Sci. Med. 2019, 236, 112400. [Google Scholar] [CrossRef] [PubMed]
- Childs, E.; De Wit, H. Regular exercise is associated with emotional resilience to acute stress in healthy adults. Front. Physiol. 2014, 5, 161. [Google Scholar] [CrossRef]
- Li, X.; Yu, H.; Yang, N. The mediating role of resilience in the effects of physical exercise on college students’ negative emotions during the COVID-19 epidemic. Sci. Rep. 2021, 11, 24510. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Zhao, S.; Wang, Q.; Zhang, Y.; Chen, C. Effects of Physical Exercise on Mobile Phone Addiction in College Students: The Chain Mediation Effect of Psychological Resilience and Perceived Stress. Int. J. Environ. Res. Public Health 2022, 19, 15679. [Google Scholar] [CrossRef]
- Yoshikawa, E.; Nishi, D.; Matsuoka, Y.J. Association between regular physical exercise and depressive symptoms mediated through social support and resilience in Japanese company workers: A cross-sectional study. BMC Public Health 2016, 16, 553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belcher, B.R.; Zink, J.; Azad, A.; Campbell, C.E.; Chakravartti, S.P.; Herting, M.M. The roles of physical activity, exercise, and fitness in promoting resilience during adolescence: Effects on mental well-being and brain development. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 225–237. [Google Scholar] [CrossRef]
- Kikkawa, M.; Shimura, A.; Nakajima, K.; Morishita, C.; Honyashiki, M.; Tamada, Y.; Higashi, S.; Ichiki, M.; Inoue, T.; Masuya, J. Mediating Effects of Trait Anxiety and State Anxiety on the Effects of Physical Activity on Depressive Symptoms. Int. J. Environ. Res. Public Health 2023, 20, 5319. [Google Scholar] [CrossRef]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1· 2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Shimura, A.; Masuya, J.; Yokoi, K.; Morishita, C.; Kikkawa, M.; Nakajima, K.; Chen, C.; Nakagawa, S.; Inoue, T. Too much is too little: Estimating the optimal physical activity level for a healthy mental state. Front. Psychol. 2023, 13, 8149. [Google Scholar] [CrossRef]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychol. 2000, 19, 586. [Google Scholar] [CrossRef]
- Eysenck, S.B.; Eysenck, H.J.; Barrett, P. A revised version of the psychoticism scale. Personal. Individ. Differ. 1985, 6, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Nakai, Y.; Inoue, T.; Toyomaki, A. A Study of Validation of the Japanese Version of the Shortened Eysenck Personality Questionnaire-Revised. In Proceedings of the 35th Congress of Japanese Society for Psychiatric Diagnosis, Sapporo, Japan, 6–7 August 2015. [Google Scholar]
- Nakajima, S.; Kim, Y.; Konishi, T.; Ito, M.; Sirai, A. Reliability and validity of Japanese version of the Connor-Davidson Resilience Scale. In The Ministry of Health Labour and Welfare Sponsored Grant for Research on the Actual Situation of Psychiatric Illnesses Caused by Large-Scale Disasters and Crime Damage and the Development of Intervention Methods; FY 2009 Report; Ministry of Health Labour and Welfare: Tokyo, Japan, 2009; pp. 93–97. Available online: https://mhlw-grants.niph.go.jp/project/16995 (accessed on 12 May 2023).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Group, P.H.Q.P.C.S.; Group, P.H.Q.P.C.S. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muramatsu, K.; Kamijima, K.; Yoshida, M.; Otsubo, T.; Miyaoka, H.; Muramatsu, Y.; Gejyo, F. The patient health questionnaire, Japanese version: Validity according to the mini-international neuropsychiatric interview–plus. Psychol. Rep. 2007, 101, 952–960. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murase, N. Validity and reliability of Japanese version of international physical activity questionnaire. J. Health Welf. Stat. 2002, 49, 1–9. [Google Scholar]
- Jetté, M.; Sidney, K.; Blümchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol. 1990, 13, 555–565. [Google Scholar] [CrossRef]
- Cortina, J.M. What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 1993, 78, 98. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, T.; Kuang, J.; Herold, F.; Ludyga, S.; Li, J.; Hall, D.L.; Taylor, A.; Healy, S.; Yeung, A.S. The roles of exercise tolerance and resilience in the effect of physical activity on emotional states among college students. Int. J. Clin. Health Psychol. 2022, 22, 100312. [Google Scholar] [CrossRef]
- Klein, D.N.; Kotov, R.; Bufferd, S.J. Personality and depression: Explanatory models and review of the evidence. Annu. Rev. Clin. Psychol. 2011, 7, 269–295. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, R.E.; Smith, N. Personality correlates of physical activity: A review and meta-analysis. Br. J. Sport. Med. 2006, 40, 958–965. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B.; Committee, P.A.G.A. Sedentary behavior and health: Update from the 2018 physical activity guidelines advisory committee. Med. Sci. Sport. Exerc. 2019, 51, 1227. [Google Scholar] [CrossRef] [PubMed]
- Navrady, L.; Adams, M.; Chan, S.; Ritchie, S.; McIntosh, A. Genetic risk of major depressive disorder: The moderating and mediating effects of neuroticism and psychological resilience on clinical and self-reported depression. Psychol. Med. 2018, 48, 1890–1899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, S.; Morishita, C.; Masuya, J.; Ono, M.; Honyashiki, M.; Higashi, S.; Tamada, Y.; Fujimura, Y.; Inoue, T. Moderating and Mediating Effects of Resilience Together with Neuroticism on Depressive Symptoms in Adult Volunteers. Neuropsychiatr. Dis. Treat. 2022, 18, 1751–1761. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, K.; Honda, T.; Nakagawa, T.; Yamamoto, S.; Akter, S.; Hayashi, T.; Mizoue, T. Associations of leisure-time, occupational, and commuting physical activity with risk of depressive symptoms among Japanese workers: A cohort study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feder, A.; Nestler, E.J.; Charney, D.S. Psychobiology and molecular genetics of resilience. Nat. Rev. Neurosci. 2009, 10, 446–457. [Google Scholar] [CrossRef] [Green Version]
- Chan, S.W.; Goodwin, G.M.; Harmer, C.J. Highly neurotic never-depressed students have negative biases in information processing. Psychol. Med. 2007, 37, 1281–1291. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic or Measure | Value (Number or Mean ± SD) | Correlation with PHQ-9 Score (r) or Effect on PHQ-9 Score (Mean ± SD of PHQ-9 Score, t-Test) |
|---|---|---|
| Age (years) | 41.2 ± 11.9 | r = −0.022, p = 0.310 |
| Sex (men:women) | 228:298 | Men 3.3 ± 3.8 vs. women 4.5 ± 4.4, p < 0.001 (t-test) |
| Education years | 14.8 ± 1.8 | r = −0.105, p = 0.009 |
| Marital status (yes:no) | 346:176 | Yes 3.5 ± 3.9 vs. no 5.0 ± 4.4, p < 0.001 (t-test) |
| Employment (yes:no) | 514:9 | Yes 4.0 ± 4.2 vs. no 3.3 ± 5.1, p = 0.714 (t-test) |
| Subjective social status (1: lowest; 10: highest) | 5.2 ± 1.7 | r = −0.274, p < 0.001 |
| Past history of psychiatric disease (yes:no) | 62:464 | Yes 6.7 ± 5.4 vs. no 3.6 ± 3.8, p < 0.001 (t-test) |
| Current psychiatric disease (yes:no) | 21:496 | Yes 8.1 ± 5.0 vs. no 3.8 ± 4.1, p < 0.001 (t-test) |
| Current physical disease (yes:no) | 103:423 | Yes 4.2 ± 4.7 vs. no 3.9 ± 4.0, p = 0.461 (t-test) |
| First-degree relative with psychiatric disease (yes:no) | 53:422 | Yes 4.5 ± 4.2 vs. no 3.9 ± 4.2, p = 0.326 (t-test) |
| EPQ-R-neuroticism score | 4.4 ± 3.5 | r = 0.571, p < 0.001 |
| CD-RISC score | 55.2 ± 17.4 | r = −0.386, p < 0.001 |
| DOP (hours/week) | 19.5 ± 7.5 | r = 0.124, p = 0.004 |
| PHQ-9 score | 4.0 ± 4.2 |
| Explanatory Variable for Depression (PHQ-9) | Univariate Model | Quadratic Equation Model | |||
|---|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | VIF | |
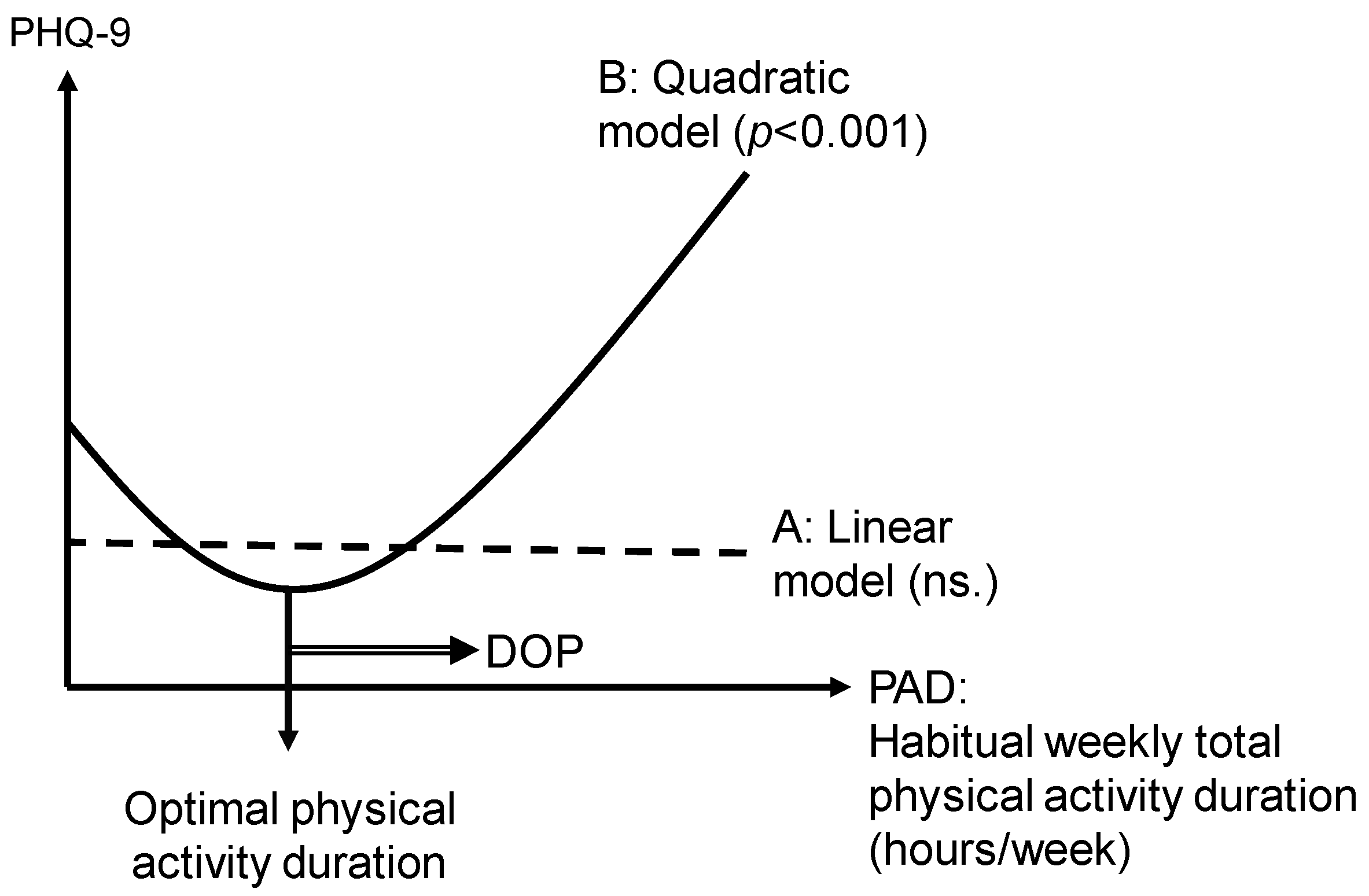
| Physical activity duration (hours/week) | −0.244 × 10−3 | 0.985 | −119.965 × 10–3 | <0.001 | 7.575 |
| (Physical activity duration)2 | 2.334 × 10–3 | <0.001 | 7.575 | ||
| F-value | 6.906 | 0.001 | |||
| Vertex value of habitual physical activity duration (hours/week) | 25.70 | ||||
| Variable | Beta | p-Value | VIF |
|---|---|---|---|
| EPQ-R (neuroticism) | 0.466 | <0.001 | 1.398 |
| Past history of psychiatric disease (1: no; 2: yes) | 0.086 | 0.035 | 1.375 |
| Current psychiatric disease (1: no; 2: yes) | 0.079 | 0.050 | 1.320 |
| Age | 0.079 | 0.058 | 1.433 |
| Sex (1: male; 2: female) | 0.076 | 0.040 | 1.118 |
| Education years | 0.023 | 0.594 | 1.499 |
| DOP | 0.016 | 0.649 | 1.067 |
| Marital status (1: unmarried; 2: married) | −0.067 | 0.080 | 1.203 |
| CD-RISC score | −0.108 | 0.010 | 1.433 |
| Subjective social status | −0.124 | 0.003 | 1.394 |
| Adjusted R2 = 0.390, F = 33.266, p < 0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakajima, K.; Shimura, A.; Kikkawa, M.; Ito, S.; Honyashiki, M.; Tamada, Y.; Higashi, S.; Ichiki, M.; Inoue, T.; Masuya, J. Optimal Physical Activity Is Associated with the Reduction of Depressive Symptoms via Neuroticism and Resilience. Healthcare 2023, 11, 1900. https://doi.org/10.3390/healthcare11131900
Nakajima K, Shimura A, Kikkawa M, Ito S, Honyashiki M, Tamada Y, Higashi S, Ichiki M, Inoue T, Masuya J. Optimal Physical Activity Is Associated with the Reduction of Depressive Symptoms via Neuroticism and Resilience. Healthcare. 2023; 11(13):1900. https://doi.org/10.3390/healthcare11131900
Chicago/Turabian StyleNakajima, Kazuki, Akiyoshi Shimura, Masayuki Kikkawa, Shunichiro Ito, Mina Honyashiki, Yu Tamada, Shinji Higashi, Masahiko Ichiki, Takeshi Inoue, and Jiro Masuya. 2023. "Optimal Physical Activity Is Associated with the Reduction of Depressive Symptoms via Neuroticism and Resilience" Healthcare 11, no. 13: 1900. https://doi.org/10.3390/healthcare11131900