
The Experience of Women Giving Birth after Cesarean Section—A Longitudinal Observational Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting
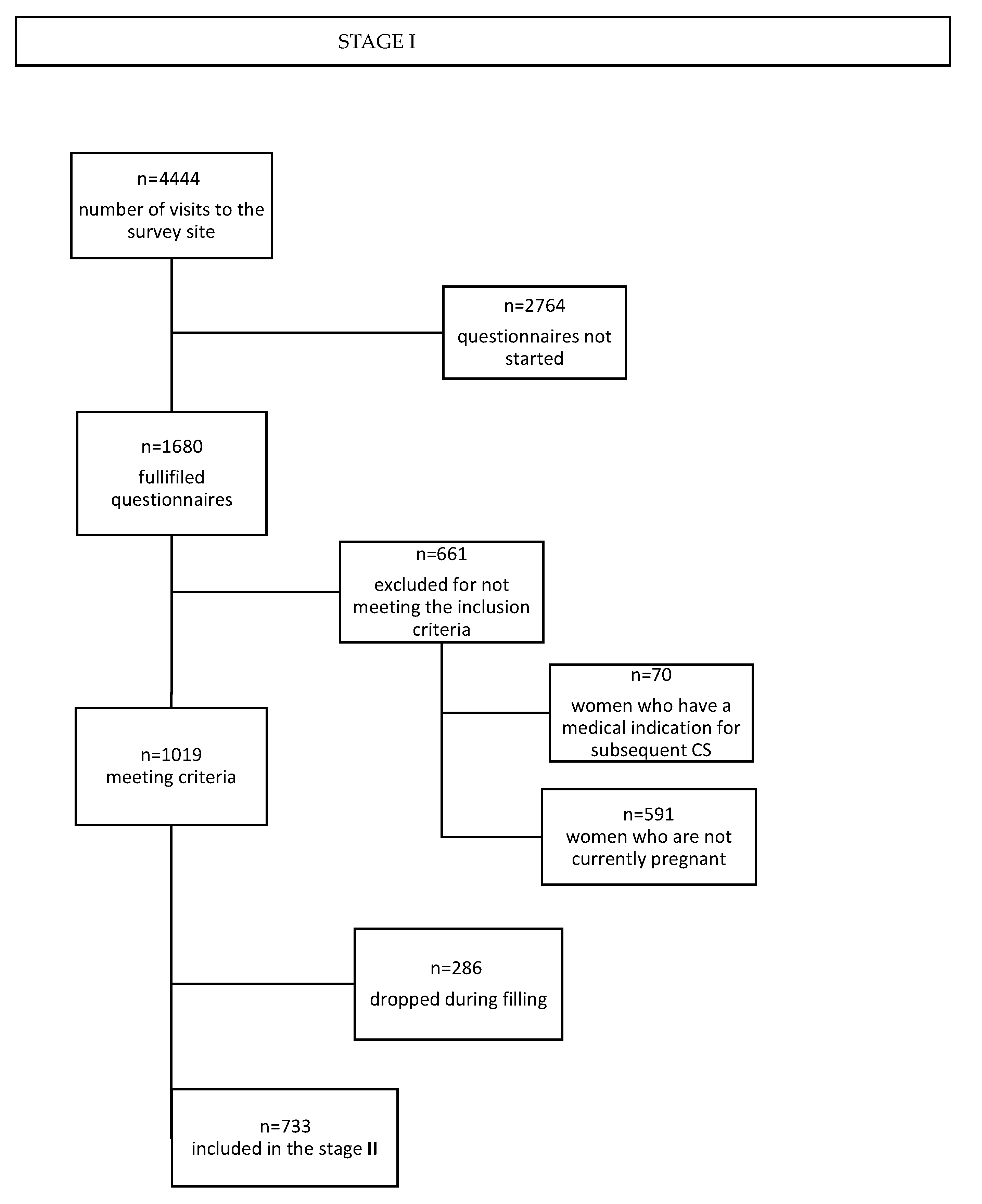
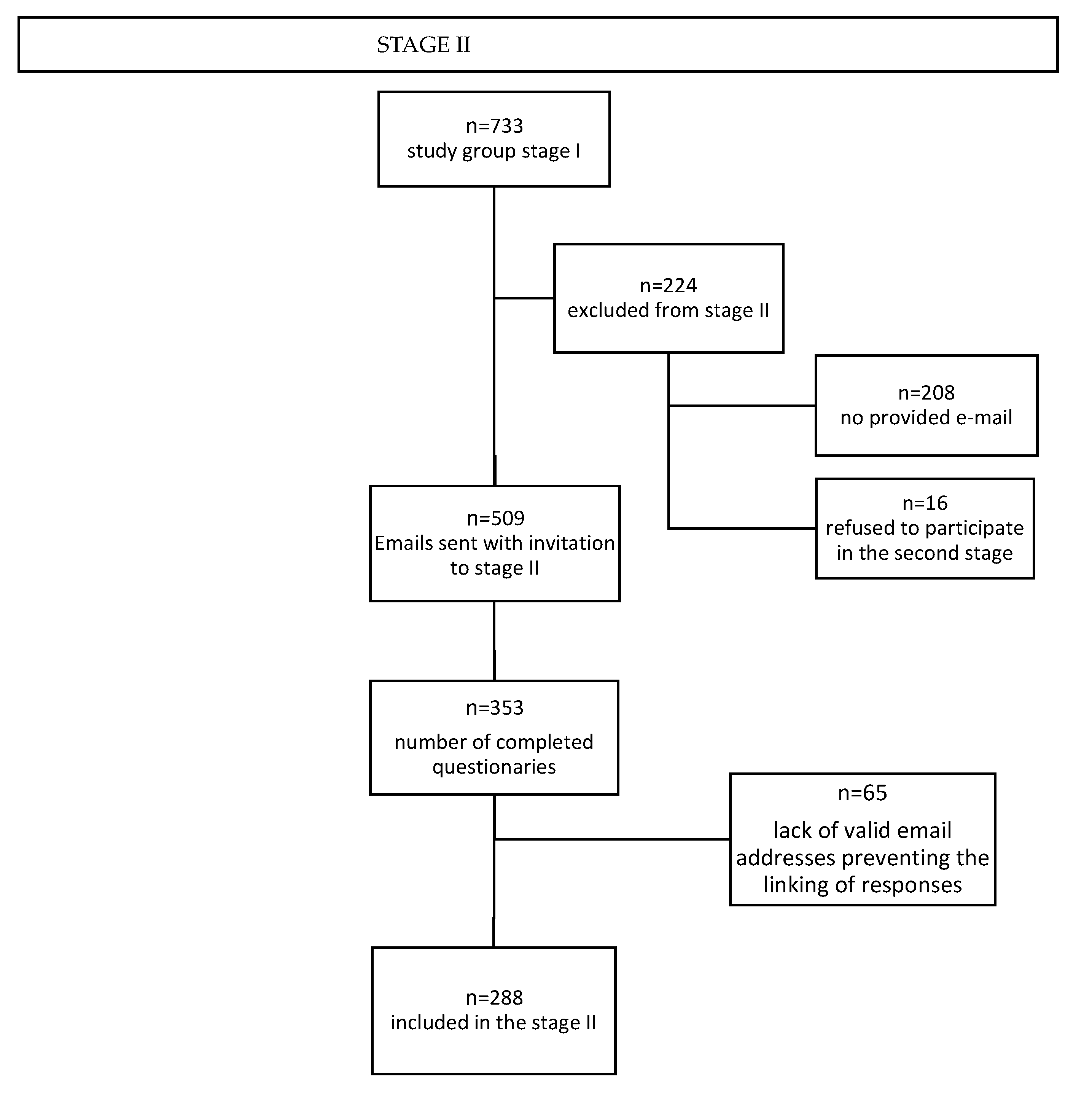
2.3. Study Group
2.4. Sample Size
2.5. Tool
2.6. Recruitment
2.7. Measures
- ✓
- demographic data: level of education, status of relationship, age, place of residence;
- ✓
- childbirth information: mode of delivery, indications for a cesarean section (if applicable), Apgar score for neonates, skin-to-skin contact, childbirth experiences, assessment of the decision about mode of delivery (if applicable), lactation experience;
- ✓
- women’s perspectives: factors influencing the mode of delivery, methods of preparing for delivery.
2.8. Statistical Analysis
- −
- Vaginal birth after cesarean section (VBAC) group—women who preferred vaginal childbirth;
- −
- Cesarean section preference (CSP) group—women who preferred a cesarean section due to a previous cesarean section;
- −
- No preference group—women who, at the time they completed the questionnaire, had no stated preference for the mode of birth in their current pregnancy.
- −
- Emergency CS group—“I tried a vaginal delivery, but it ended with an emergency cesarean section”;
- −
- VBAC group—“I gave birth vaginally”;
- −
- Elective CS group—“I wanted to attempt a vaginal birth, but it was not possible due to medical reasons, so I had a planned cesarean section”;
- −
- Lack of consent for trial of labor after cesarean section (TOLAC) group—“I did not consent to a vaginal birth, instead I had a planned cesarean section.”
3. Results
Study Group Characteristics
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ACOG Practice Bulletin, No. 205: Vaginal Birth After Cesarean Delivery. Obstet. Gynecol. 2019, 133, e110–e127. [CrossRef] [PubMed]
- Birth after Previous Caesarean Birth (Green-Top Guideline No. 45). Available online: https://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg45/ (accessed on 7 September 2020).
- Martel, M.-J.; MacKinnon, C.J. Clinical Practice Obstetrics Committee, Society of Obstetricians and Gynaecologists of Canada Guidelines for Vaginal Birth after Previous Caesarean Birth. J. Obstet. Gynaecol. Can. 2005, 27, 164–188. [Google Scholar] [CrossRef] [PubMed]
- Sentilhes, L.; Vayssière, C.; Beucher, G.; Deneux-Tharaux, C.; Deruelle, P.; Diemunsch, P.; Gallot, D.; Haumonté, J.-B.; Heimann, S.; Kayem, G.; et al. Delivery for Women with a Previous Cesarean: Guidelines for Clinical Practice from the French College of Gynecologists and Obstetricians (CNGOF). Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Reif, P.; Brezinka, C.; Fischer, T.; Husslein, P.; Lang, U.; Ramoni, A.; Zeisler, H.; Klaritsch, P. Labour and Childbirth After Previous Caesarean Section. Geburtshilfe Frauenheilkd 2016, 76, 1279–1286. [Google Scholar] [CrossRef] [Green Version]
- Wielgoś, M.; Bomba-Opoń, D.; Bręborowicz, G.H.; Czajkowski, K.; Dębski, R.; Leszczyńska-Gorzelak, B.; Oszukowski, P.; Radowicki, S.; Zimmer, M. Rekomendacje Polskiego Towarzystwa Ginekologów i Położników dotyczące cięcia cesarskiego. Ginekol. Perinatol. Prakt. 2018, 3, 159–174. [Google Scholar]
- Ryan, G.A.; Nicholson, S.M.; Morrison, J.J. Vaginal Birth after Caesarean Section: Current Status and Where to from Here? Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 52–57. [Google Scholar] [CrossRef]
- Institute for Applied Quality Improvement and Research in Health Care GmbH. German Hospital Quality Report 2013; AQUA Institute GmbH: Göttingen, Germany, 2013; p. 256. [Google Scholar]
- Roddy Mitchell, A.; Gordon, H.; Lindquist, A.; Walker, S.P.; Homer, C.S.E.; Middleton, A.; Cluver, C.A.; Tong, S.; Hastie, R. Prevalence of Perinatal Depression in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2023, 80, 425–431. [Google Scholar] [CrossRef]
- Gurol-Urganci, I.; Bou-Antoun, S.; Lim, C.P.; Cromwell, D.A.; Mahmood, T.A.; Templeton, A.; van der Meulen, J.H. Impact of Caesarean Section on Subsequent Fertility: A Systematic Review and Meta-Analysis. Hum. Reprod. 2013, 28, 1943–1952. [Google Scholar] [CrossRef] [Green Version]
- Mueller, N.T.; Mao, G.; Bennet, W.; Hourigan, S.; Dominguez-Bello, M.G.; Appel, L.J.; Wang, X. Can Vaginal Delivery Reduce the Intergenerational Transmission of Overweight and Obesity? Findings from the Boston Birth Cohort. Circulation 2016, 134, A15885. [Google Scholar]
- Sevelsted, A.; Stokholm, J.; Bønnelykke, K.; Bisgaard, H. Cesarean Section and Chronic Immune Disorders. Pediatrics 2015, 135, e92–e98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Recommendations on Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-155021-5. [Google Scholar]
- Baranowska, B. The Quality of Childbirth in the Light of Research the New Guidelines of the World Health Organization and Polish Perinatal Care Standards. J. Mother Child 2019, 23, 54–59. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Poreba, R.; Brazert, J.; Chazan, B.; Czajka, R.; Czajkowski, K.; Debski, R.; Drews, K.; Jaworski, S.; Karowicz-Bilińska, A.; Kubicki, J.; et al. Rekomendacje Polskiego Towarzystwa Ginekologicznego. Cięcie cesarskie. Ginekol. Pol. 2008, 79, 378–384. [Google Scholar] [PubMed]
- GUS. Rocznik Demograficzny 2019; GUS: Warszawa, Poland, 2019. [Google Scholar]
- Peristat, E.; Macfarlane, A.J. Euro-Peristat Project European Perinatal Health Report. Core Indicators of the Health and Care of Pregnant Women and Babies in Europe in 2015; Euro-Peristat: Paris, France, 2018. [Google Scholar]
- Kaimal, A.J.; Grobman, W.A.; Bryant, A.; Blat, C.; Bacchetti, P.; Gonzalez, J.; Thiet, M.-P.; Bermingham, Y.; Kuppermann, M. The Association of Patient Preferences and Attitudes with Trial of Labor after Cesarean. J. Perinatol. 2019, 39, 1340–1348. [Google Scholar] [CrossRef]
- Fumagalli, S.; Colciago, E.; Antolini, L.; Perego, S.; Fiorasi, M.; Fossati, V.; Nespoli, A.; Vergani, P. Women’s Decision-Making about Mode of Birth after a Previous Caesarean Section. Br. J. Midwifery 2020, 28, 104–113. [Google Scholar] [CrossRef]
- Sys, D.; Baranowska, B.; Kajdy, A.; Tataj-Puzyna, U.; Gotlib, J.; Bączek, G.; Juszczakiewicz, P.; Rabijewski, M. Women’s Views and Preferences Regarding the Mode of Birth after Cesarean Section: Polish Cross-Sectional Web-Based Survey. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 273, 26–32. [Google Scholar] [CrossRef]
- Micek, M.; Kosinska-Kaczynska, K.; Godek, B.; Krowicka, M.; Szymusik, I.; Wielgos, M. Birth after a Previous Cesarean Section—What Is Most Important in Making a Decision? Neuroendocrinol. Lett. 2014, 35, 718–723. [Google Scholar]
- Pietrzak, B.; Kosińska-Kaczyńska, K.; Langiewicz, I.; Stasiełuk, A.; Wielgoś, M. Is the Epidemic of Cesarean Sections the Result of More Liberal Indications? Ginekol. Pol. 2012, 83, 604–608. [Google Scholar]
- Santorek, N.; Biłas, K.; Tokarska, A.; Zarzycka, K.; Kasprzak, P.; Kwiatkowski, S.; Torbe, A. Cięcie cesarskie. Rosnący odsetek i zmiana trendów we wskazaniach. Varia Med. 2019, 3, 279–288. [Google Scholar]
- Szumska, M.; Kozłowska-Wytyk, M.; Olejniczak, T. Analiza Wskazań Do Porodów Operacyjnych w Latach 2016–2018 w Szpitalu Św. Rodziny w Poznaniu. Pol. Przegląd Nauk. Zdrowiu 2019, 59, 184–190. [Google Scholar] [CrossRef] [Green Version]
- McGrath, P.; Phillips, E.; Vaughan, G. Speaking out! Qualitative Insights on the Experience of Mothers Who Wanted a Vaginal Birth after a Birth by Cesarean Section. Patient 2010, 3, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Pilch, D. The influence of birth modus on the emotional state of the mother, bonding, and the newborn’s neurobehavioural state. Pomeranian J. Life Sci. 2015, 61, 249–256. [Google Scholar] [PubMed]
- Prado, D.S.; Mendes, R.B.; Gurgel, R.Q.; de Barreto, I.D.C.; Cipolotti, R.; Gurgel, R.Q. The Influence of Mode of Delivery on Neonatal and Maternal Short and Long-Term Outcomes. Rev. Saude Publica 2018, 52, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maria, A.; Shukla, A.; Wadhwa, R.; Kaur, B.; Sarkar, B.; Kaur, M. Achieving Early Mother-Baby Skin-to-Skin Contact in Caesarean Section: A Quality Improvement Initiative. Indian Pediatr. 2018, 55, 765–767. [Google Scholar] [CrossRef]
- Achieving Skin to Skin Contact in Theatre for Healthy Newborns. Pract. Midwife 2015, 18, 9–10+12.
- Cohen, S.S.; Alexander, D.D.; Krebs, N.F.; Young, B.E.; Cabana, M.D.; Erdmann, P.; Hays, N.P.; Bezold, C.P.; Levin-Sparenberg, E.; Turini, M.; et al. Factors Associated with Breastfeeding Initiation and Continuation: A Meta-Analysis. J. Pediatr. 2018, 203, 190–196.e21. [Google Scholar] [CrossRef] [Green Version]
- Bodner, K.; Wierrani, F.; Grünberger, W.; Bodner-Adler, B. Influence of the Mode of Delivery on Maternal and Neonatal Outcomes: A Comparison between Elective Cesarean Section and Planned Vaginal Delivery in a Low-Risk Obstetric Population. Arch. Gynecol. Obstet. 2011, 283, 1193–1198. [Google Scholar] [CrossRef]
- Pang, M.W.; Leung, T.N.; Lau, T.K.; Chung, T.K.H. Impact of First Childbirth on Changes in Women’s Preference for Mode of Delivery: Follow-up of a Longitudinal Observational Study. Birth 2008, 35, 121–128. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| (1) Emergency CS n = 75 | (2) VBAC n = 122 | (3) Elective CS n = 64 | (4) Lack of Consent for TOLAC n = 27 | H | p | Post-Hoc | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | ||||
| Minimizing pain | 0.05 | 1.46 | −0.12 | 1.46 | −0.16 | 1.47 | 0.37 | 1.62 | 2.926 | 0.403 | N/A |
| Convenience and predictability of ECS | −1.41 | 1.15 | −1.47 | 1.11 | −1.06 | 1.04 | 1.07 | 1.47 | 64.997 | <0.001 | ALL |
| Severity of cesarean section | 0.97 | 1.35 | 1.18 | 1.23 | 0.80 | 1.45 | −0.30 | 1.30 | 26.874 | <0.001 | 1 vs. 4 2 vs. 4 3 vs. 4 |
| Better bond between mother and child | 1.19 | 1.15 | 0.97 | 1.41 | 0.91 | 1.43 | 0.19 | 1.44 | 10.820 | 0.013 | 1 vs. 4 |
| Ensuring better health for the child | 1.57 | 0.74 | 1.47 | 0.99 | 1.50 | 0.87 | 1.15 | 1.29 | 1.771 | 0.621 | N/A |
| Ensuring better health of the mother | 1.56 | 0.72 | 1.47 | 0.94 | 1.38 | 0.98 | 0.85 | 1.41 | 6.884 | 0.076 | N/A |
| Ensuring skin-to-skin contact | 1.63 | 0.83 | 1.62 | 0.94 | 1.53 | 0.89 | 0.96 | 1.34 | 11.487 | 0.009 | - |
| Better conditions for breastfeeding | 1.01 | 1.26 | 1.10 | 1.24 | 1.11 | 1.25 | 0.26 | 1.40 | 11.425 | 0.009 | 2 vs. 4 3 vs. 4 |
| Influence of the mode of birth on subsequent pregnancies and deliveries | 1.45 | 1.06 | 1.18 | 1.27 | 1.25 | 1.18 | −0.07 | 1.57 | 24.613 | <0.001 | 1 vs. 4 2 vs. 4 3 vs. 4 |
| Faster recovery | 1.55 | 0.83 | 1.49 | 0.98 | 1.47 | 0.94 | 0.37 | 1.52 | 22.976 | <0.001 | 1 vs. 4 2 vs. 4 3 vs. 4 |
| Less blood loss | 0.83 | 1.27 | 0.55 | 1.32 | 0.56 | 1.22 | 0.00 | 1.44 | 7.659 | 0.054 | N/A |
| Sense of fulfillment | 1.29 | 1.12 | 1.20 | 1.30 | 0.89 | 1.46 | −0.15 | 1.61 | 20.856 | <0.001 | 1 vs. 4 2 vs. 4 |
| Strengthening the sense of femininity | 0.81 | 1.48 | 0.80 | 1.47 | 0.38 | 1.54 | −0.26 | 1.63 | 12.923 | 0.005 | 1 vs. 4 2 vs. 4 |
| Improving your relationship with your partner | −0.04 | 1.46 | −0.02 | 1.43 | −0.31 | 1.40 | −0.26 | 1.63 | 2.460 | 0.483 | N/A |
| Previous birth experiences | 1.31 | 0.97 | 1.59 | 0.86 | 1.06 | 1.21 | 1.19 | 1.42 | 15.028 | 0.002 | 2 vs. 3 |
| Previous postpartum experiences | 0.80 | 1.25 | 1.01 | 1.28 | 0.83 | 1.33 | 0.78 | 1.58 | 2.636 | 0.451 | N/A |
| Before Labor | After Labor | z | p | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | |||
| Minimizing pain | −0.74 | 1.23 | −0.02 | 1.47 | 5.790 | <0.001 |
| Convenience and predictability of ECS | −1.49 | 1.02 | −1.12 | 1.35 | 3.301 | 0.001 |
| Severity of cesarean section | 0.40 | 1.44 | 0.90 | 1.38 | 4.946 | <0.001 |
| Better bond between mother and child | 0.72 | 1.44 | 0.93 | 1.38 | 2.256 | 0.024 |
| Ensuring better health for the child | 1.34 | 0.96 | 1.47 | 0.94 | 2.071 | 0.038 |
| Ensuring better health of the mother | 1.24 | 1.01 | 1.41 | 0.97 | 2.790 | 0.005 |
| Ensuring skin-to-skin contact | 1.34 | 1.10 | 1.54 | 0.96 | 3.228 | 0.001 |
| Better conditions for breastfeeding | 1.02 | 1.24 | 1.00 | 1.28 | 0.024 | 0.981 |
| Influence of the mode of birth on subsequent pregnancies and deliveries | 0.84 | 1.47 | 1.15 | 1.30 | 3.716 | <0.001 |
| Faster recovery | 1.29 | 1.14 | 1.40 | 1.05 | 1.320 | 0.187 |
| Less blood loss | 0.06 | 1.34 | 0.57 | 1.31 | 4.841 | <0.001 |
| Sense of fulfillment | 0.89 | 1.46 | 1.02 | 1.39 | 2.070 | 0.038 |
| Strengthening the sense of femininity | 0.43 | 1.58 | 0.60 | 1.53 | 2.027 | 0.043 |
| Improving your relationship with your partner | −0.49 | 1.31 | −0.13 | 1.45 | 3.773 | <0.001 |
| Previous birth experiences | 1.25 | 1.10 | 1.36 | 1.05 | 1.601 | 0.109 |
| Previous postpartum experiences | 0.76 | 1.37 | 0.88 | 1.31 | 1.285 | 0.199 |
| aOR | 95% CI | p | ||
|---|---|---|---|---|
| Minimizing pain | 0.90 | 0.73 | 1.11 | 0.329 |
| Convenience and predictability of ECS | 0.55 | 0.42 | 0.76 | 0.001 |
| Severity of cesarean section | 1.21 | 1.01 | 1.45 | 0.039 |
| Better bond between mother and child | 0.95 | 0.80 | 1.12 | 0.515 |
| Ensuring better health for the child | 1.33 | 1.01 | 1.78 | 0.051 |
| Ensuring better health of the mother | 1.42 | 1.10 | 1.88 | 0.010 |
| Ensuring skin-to-skin contact | 1.13 | 0.89 | 1.44 | 0.324 |
| Better conditions for breastfeeding | 1.15 | 0.94 | 1.42 | 0.187 |
| Influence of the mode of birth on subsequent pregnancies and deliveries | 1.11 | 0.93 | 1.32 | 0.256 |
| Faster recovery | 1.20 | 0.95 | 1.53 | 0.126 |
| Less blood loss | 1.00 | 0.84 | 1.21 | 0.966 |
| Sense of fulfillment | 1.10 | 0.92 | 1.32 | 0.290 |
| Strengthening the sense of femininity | 1.10 | 0.94 | 1.29 | 0.244 |
| Improving your relationship with your partner | 1.06 | 0.87 | 1.28 | 0.571 |
| Previous birth experiences | 1.04 | 0.83 | 1.31 | 0.752 |
| Previous postpartum experiences | 0.98 | 0.83 | 1.17 | 0.850 |
| OR | 95% CI | p | ||
|---|---|---|---|---|
| Convenience and predictability of ECS | 0.60 | 0.42 | 0.85 | 0.004 |
| Severity of cesarean section | 1.08 | 0.89 | 1.31 | 0.425 |
| Ensuring better health for the child | 1.04 | 0.71 | 1.52 | 0.832 |
| Ensuring better health of the mother | 1.15 | 0.79 | 1.67 | 0.479 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sys, D.; Kajdy, A.; Niżniowska, M.; Baranowska, B.; Raczkiewicz, D.; Tataj-Puzyna, U. The Experience of Women Giving Birth after Cesarean Section—A Longitudinal Observational Study. Healthcare 2023, 11, 1806. https://doi.org/10.3390/healthcare11121806
Sys D, Kajdy A, Niżniowska M, Baranowska B, Raczkiewicz D, Tataj-Puzyna U. The Experience of Women Giving Birth after Cesarean Section—A Longitudinal Observational Study. Healthcare. 2023; 11(12):1806. https://doi.org/10.3390/healthcare11121806
Chicago/Turabian StyleSys, Dorota, Anna Kajdy, Martyna Niżniowska, Barbara Baranowska, Dorota Raczkiewicz, and Urszula Tataj-Puzyna. 2023. "The Experience of Women Giving Birth after Cesarean Section—A Longitudinal Observational Study" Healthcare 11, no. 12: 1806. https://doi.org/10.3390/healthcare11121806