
A Mixed-Methods Systematic Review of Group Reflective Practice in Medical Students

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Protocol, and Registration
2.2. Search Strategy
- ‘reflection’, or ‘reflective practice’, or ‘reflective thinking’, or ‘reflective learning’, or reflective group’, or ‘balint group’, AND
- ‘group’, AND
- ‘medical students’, AND
- ‘empathy’, or ‘clinical competence’, or ‘patient centred care’, or ‘communication’, or ‘doctor patient relationship’, or ‘burnout’.
2.3. Study Selection
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Review Team
2.5. Screening and Data Extraction
2.6. Quality Assessment
2.7. Data Analysis
3. Results
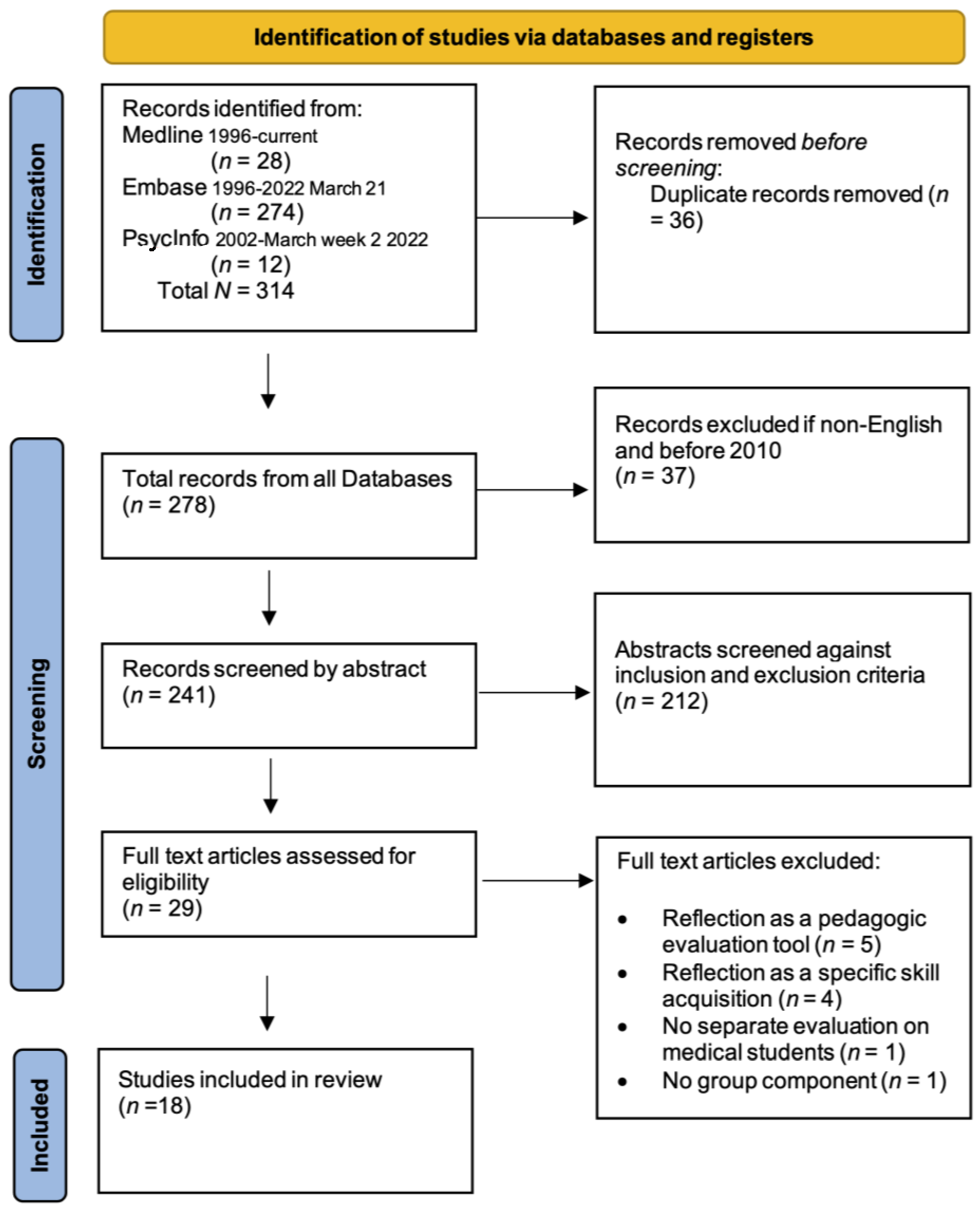
3.1. Search Results
3.2. Study Characteristics
3.3. Quality and Bias Analysis
3.4. Synthesis of Results
3.4.1. Professionalism: Bridging Clinical and Theoretical Paradigms to Serve the Doctor Patient-Relationship
3.4.2. Empathy: Halting Empathy Decline
3.4.3. Wellbeing: The Value of Shared Experience
3.4.4. Ingredients for Successful RP Groups
3.4.5. Innovative Delivery Methods
4. Discussion
4.1. Limitations
4.2. Implications for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Study Author/Year/Country | Research Aim/Question(s) | Participants Sample Size/Nature/ Settings | Description Study Design/Comparison Group(s), If Any | Outcomes | Methodological Quality Notes and Limitations | Level of Evidence OCEBM | Quantitative Rating | Qualitative Rating |
|---|---|---|---|---|---|---|---|---|
| Airagnes et al., 2014 [34] France | To examine changes in empathic abilities in an optional Balint groups | 34 fourth-year medical students in an optional “doctor-patient relationship training” certificate | Quantitative methodology Measured interpersonal reactivity index (IRI) and emotional reactions (empathic-approach, rejecting-attitude, intellectual-interest and fear of emotion contagion) in response to two case-reports before the training sessions and 4 months later Compared with 129 participating in other certificates | An increase of IRI fantasy-scale (p = 0.02) and a decrease of IRI empathic-concern (p = 0.006) at follow-up, regardless of the group. Empathic-approach only increased in the “Balint group” and for the first case-report (p = 0.023), with a difference between the groups at follow-up (p = 0.003). Balint groups may enable students to better handle difficult clinical situations, e.g., those presented by patients with borderline personality traits. | Intervention group (“Balint group”) not described in details Lack of randomisation and scale justification which impact on the causality of conclusion Sample size not justified | 2 | 77% | - |
| Bird et al., 2020 [22] United States | To cultivate resilience and promote wellness during students’ core clerkship rotations | 144 clerkship students at two academic institutions (74 at University A; 70 at University B) | Both quantitative and qualitative data collected Learners completed pre- and post-curriculum surveys, including the Connor-Davidson Resilience Scale (CD-RISC; optional) Focus groups conducted with seven students at University A | Students valued connecting with peers and feeling less alone. The need to construct a setting conducive to comfortable reflection for all learners-not all students found these sessions necessary. Sessions may have improved resilience | Research question not clearly stated Subject characteristics not described Larger sample size but not justified CD-RISC fluctuation might subject to confounders which were not considered Reflexivity not considered | 3 | 41% | C |
| Brand et al., 2016 [28] United Kingdom | To explore if photographs, narratives and small group collaborative dialogue fosters reflective learning, enhances reflective capacity and shift attitudes towards caring for older adults | 128 (out of a cohort of 240) second year medical students; 95 students submitted an individual written reflection | Mixed method evaluation design, measuring attitudes using pre and post questionnaire responses and individual written reflections, exploring their perceptions toward older adults A 13-item validated Geriatric Attitude Scale was included. | Positive shifts in medical students’ perceptions towards older adults. The qualitative reflections were captured in four main themes: the opportunity provided to envision working with older adults; the tension created to challenge learners’ misinformed assumptions, and the work of dismantling those assumptions, leading to seeing older people as individuals | Small sample size No attempt to reach data saturation Thematic analysis described Reflexivity considered Conclusion supported by the results | 3 | 86% | A |
| Chou et al., 2011 [23] United States | To describe a clerkship model called Veteran Affairs Longitudinal Rotations (VALOR), designed to establish a supportive learning environment for small peer groups | Seven groups of third year medical students (42 total) across three academic years, one hour per week during VALOR | Immediate post surveys and focus groups at the end of VALOR, and with follow-up surveys 5 to 27 months after completing VALOR | Students strongly valued support through clerkship challenges, meeting for facilitated reflection, appreciating patient experiences across the continuum of care, developing critical professional skills, and communication around patient care | Voluntary participation might skew the results No clear research question stated Some triangulation through both focus group and survey No reflexibility considered Confounder of concurrent clerkship activities not taken into account | - | - | C |
| Chu et al., 2018 [36] Taiwan | To determine psychosocial issues among patients and their family members through reflective dialogue groups | 50 medical students were rotated to the department of Paediatrics for one month (7–9 on each rotation) Each student completed the reflective writing assignment and participated in one of the six group discussion sessions. | The recordings of the six reflective group sessions were transcribed for thematic analysis. A six-step theme generation process was conducted in the first reading stage of all transcripts by four researchers. | A total of 108 psychosocial issues were coded and categorized into six main themes: medical communication, the intricate medical ecological system, role and function of a family, development of medical professionalism, ethical dilemmas, and various patient perspectives from diverse cultural backgrounds. They illustrate that medical care should focus not only on illnesses but also patients’ psychosocial narratives | Clear aim of the study Sample size not justified Form of data recorded and transcribed with audit trail Using the content of the reflective groups for research analysis might introduce bias. | - | - | B |
| Duke et al., 2015 [24] United States | To analyse the effects of a professionalism course on empathy and self-reflection (two elements of professionalism) and their perceptions about the course | Third year medical students, meeting virtually throughout the year. 240 students who provided online feedback | Mixed methodology including the Groningen Reflection Ability Scale (GRAS) and the Jefferson Scale of Empathy (JSE) before and after the course and anonymous online feedback, which was analysed using thematic content analysis. | JSE demonstrated preservation of empathy rather than its decline. A statistically significant increase in GRAS scores (p < 0.001) This study supports previous findings showing that students benefit from peer groups and discussion in a safe environment, which may include the use of a virtual group video platform | Poor generalisability due to single institution involvement No clear research question stated Sample size not justified No reflexivity considered No subgroup analysis | 3 | 82% | B |
| Gajree 2021 [29] United Kingdom | To assess whether a Balint group helped gain a better understanding of the role of emotions in the doctor–patient relationship | 16 fourth or fifth year (of the 41 third, fourth and fifth year) medical students on clinical placement following their voluntary 5-week Balint groups | All completed an anonymous questionnaire following the final Balint group session about their experience. The questionnaire [4] entailed responding to a number of statements on a 5-point Likert scale and providing written feedback to open-ended questions about the group. | The groups helped students to think about the place of emotions in patient encounters, and the doctor-patient relationship. Most agreed that participating in a Balint group was an important part of their training as a doctor. Students overwhelmingly indicated that Balint groups provide an aspect of training that is not currently addressed elsewhere in the curriculum | Low number of participants reducing its generalisability The potential for selection bias due to its voluntary nature No reflexivity considered Clear statement of aim | - | - | B |
| Gold et al., 2019 [25] United States | To create a safe space to regularly discuss shared experiences in medical school while providing a near peer opportunity for psychiatry residents to acquire group facilitation experience | 30 students participated in groups led by psychiatry residents 18 completed post-surveys in first- and second-year medical students attending voluntary, biweekly support groups | Surveys at baseline and 6 months included qualitative assessments of groups and validated surveys to assess empathy, wellness, and loneliness. Separate surveys assessed attrition. Statistical analyses (descriptive statistics) and thematic analysis | Groups may benefit in improving impostor syndrome and connection with others (decreased loneliness), allowing exposure to and tolerance of diverse perspectives, increasing insight into the importance of self-care and emotional self-awareness, allowing practice for collaborative skills, and increasing thoughtful approaches to patient care | Unclear objective Study design inappropriate–hypothesis driven Unclear sampling strategy Reflexivity identified as limitation Study participants’ characteristics not described Lack of control group Voluntary participation might skew results | 5 | 27% | C |
| Imperato et al., 2021 [26] United States | To analyse what structured Reflection Rounds had on self-reported empathy and emotional intelligence scores | 285 voluntary third-year medical students during their core clinical clerkships Small-group meetings, where students reflect upon their thoughts, feelings, and emotions about clinical experiences and receive feedback from peers and a trained facilitator | Quantitative measures of pre- and post-intervention utilizing the self-reported Jefferson scale of empathy (JSE) student version and Wong law emotional intelligence scale (WLEIS) | Empathy scores increased from 80.4 to 82.6 (p = 0.02) post-intervention. No significant difference in EI scores was demonstrated post-intervention, 5.4 to 5.5 (p = 0.55) | Lack of a control group No justification of sample size Lack of compliance with consistent utilization of unique identification coding precluded individual analysis of matched data | 3 | 73% | - |
| Lemogne et al., 2020 [35] France | To assess the effects of Balint groups and narrative medicine training on clinical empathy | 362 out of the 392 fourth year medical students completed The intervention groups received either seven sessions of 1.5-h Balint groups or a 2-h lecture and five sessions of 1.5-h narrative medicine training | 117 fourth-year medical students in the control group, 125 in the Balint group and 120 in the narrative medicine group The main quantitative outcome was the change in JSPE-MS© score from baseline to one week after the last session. | Adjusting for participants’ characteristics at baseline, Balint groups remained associated with better outcomes compared to the control group (beta = 2.673, p = 0.030) Balint groups may promote clinical empathy to some extent among medical students, at least in the short run | Clear aim and objective Appropriate study design Confounding considered with control and comparison groups Underpower between the two intervention groups to draw conclusions as regards the lack of difference self-reported measures may be more influenced by social desirability biases than objective measures | 2 | 93% | - |
| Lutz et al., 2017 [38] Germany | To explore both the attitudes of those students towards the program and factors that might hinder or enhance how students engage in reflective discourse | Of the 168 contacted preclinical students who attended a group mentoring program, 14 consented to participating in the focus group interviews. Eight mentors and one co-mentor agreed to participate in individual interviews. | A qualitative design was applied using semi-structured focus group interviews with preclinical students and semi-structured individual interviews with mentors and co-mentors | Some students valued the new program and named positive outcomes regarding several features of professional development and enriching experiences. Others expressed aversive attitudes: unclear goals and benefits, interpersonal problems within the groups hindering development and intrapersonal issues such as insecurity and traditional views of medical education | Clear research question Appropriate and clear sampling strategy Reflexivity considered Triangulation from different sources attempted One setting attitude analysis limited the generalizability The students who agreed to take part in the interviews may have been particularly motivated and reflective | - | - | A |
| McManus et al., 2020 [39] Ireland | To establish and evaluate the impact of a 6-week Balint group on empathy and resilience during psychiatry rotation | 28 out of the 50 eligible fourth-year medical students | A prospective study used the Jefferson Scale of Empathy–Student Version and the Brief Resilience Scale before and after 6-week Balint groups One week after the final Balint group in each course, the Balint lead and co-lead met with the participants to conduct a focus group | Enthusiasm regarding the value of Balint groups in promoting self-reflection and gaining insight into self- and patient-care dynamics. There was a significant difference in empathy scores pre- and post-Balint intervention. There was no significant difference in resilience scores | Clear study aims and design No control group limiting generalisability Sample size is relatively small Confounding variables such as whether lectures and practical teaching in psychiatry could have improved empathy or whether impending exams could have affected post-group scores in resilience or empathy | 4 | 77% | B |
| O’Neill et al., 2016 [31] Australia | To pilot and employ the traditional method pioneered by Michael and Enid Balint for general practitioners working in London after the Second World War | One group of six third-year graduate students, meeting weekly over six weeks. | Evaluation includes pre- and post-questionnaires, a 1000-word essay and leaders’ observations. | Traditional Balint method needs to be modified for students at a point in their training where they have not yet been exposed to patients for long enough to develop meaningful patient relationships. Some evidence of a heightened awareness of the dynamics of doctor–patient relationships and the importance of psychological/emotional factors (including their own prejudices) Balint-style groups could be an effective way of encouraging reflection on the importance of emotions in the doctor–patient relationship. | Small sample size Recall bias: notes are memory-dependent and may be influenced by the leaders’ own (unconscious) prejudices and interpretations procedural change introduced after the third session No baseline measurement | - | - | C |
| Parker et al., 2012 [32] Australia | To examine whether groups could be effectively implemented within the curriculum and whether the student participants would value such an opportunity | Ten third-year medical students during six of the eight weeks of their clinical rotation in psychiatry Two rotations have been completed | The educational value of each meeting and the group overall is assessed using questionnaires. | Students were less certain of the relevance to their clinical practice, which requires adaptation of method and process to context Short-term clinical reflection groups can be effectively implemented for medical students in a hospital environment, supporting students in the process of learning to work in doctor-patient relationships | No comparison group Small sample size limiting its generalisability. No reflexivity considered No clear analysis methodology | - | - | C |
| Parker et al., 2014 [33] Australia | To consider whether clinical reflection groups following the Balint process would be perceived as useful and relevant to the learning needs of the student participants. | All group members (n = 42) medical students in psychiatry at a large Australian tertiary referral hospital This paper presents the outcomes of the named project at the conclusion of its one-year trial [32]. | A grounded theory approach, including survey data, thematic analysis of written feedback, and facilitator reflection on the process. | The evaluation suggested that fidelity of the Balint group experience was achieved and that student attitudes were neutral to mildly positive regarding the educational experience. Balint groups are potentially useful to medical students in the Australian context. More useful when applied in less alienating learning environments, such as during general practice rotations. | Larger sample size compared to previously presented data [32] No reflexivity considered Tape recording and triangulation of multiple sources of data attempted | - | - | B |
| Plack et al., 2010 [27] United States | To determine whether peer-facilitated virtual action learning (VAL) demonstrated reflection and critical thinking around complex issues during their paediatric clerkship | 70 clerkship students were introduced to reflection and participated in VAL by using an electronic discussion board 70 critical incidents, 210 discussion board entries, 70 revised critical incidents, and 70 reflective essays were analysed | Qualitative methods were used to analyse initial critical incidents, discussion threads, and summative reflective essays. Two non-physician researchers involved in data analysis helped design the study but were not involved in its implementation. | Broadened perspectives (44/70), questioned assumptions (12/70), and reconfirmed thinking (14/70). Content themes included communication, role identification, medical treatment concerns, and limited voice and power. Most students demonstrated reflection on complex clinical issues. Themes portrayed struggles encountered and exposed issues in the hidden curriculum, suggesting a lack of voice and power that may lead to missed learning opportunities | Small sample of convenience No baseline measures or use of a control group Triangulation of several written data sources Analysis done by separate investigators Reflexivity considered | - | - | A |
| Wen et al., 2015 [37] Taiwan | To investigate the characteristics of feedback in a reflective dialogue group, involving a structured narrative reflective writing combined with pluralistic group discussion with a tutor and peers | 40 fifth-year medical students of five monthly interval rotations at the paediatric department of a medical centre in eastern Taiwan | The evaluative questionnaire regarding the benefits of reflection with others was administrated following the group session | Each student attained 1.25 times the depth or breadth of reflection after receiving feedback and experienced the benefits of reflection with others. the medical students had time to think deeply and broadly about psychosocial issues among patients and their family members. Facilitative feedback providing new knowledge, deeper discussion, and exploring new ways of action planning for psychosocial issues was recommended to promote students’ reflective capacity. | Clear research question and aim Context and setting adequately described Sample size not justified Triangulation of different data sources with systematic transcription and subsequent analysis Reflexivity not considered | - | - | B |
| Yakeley et al., 2011 [30] United Kingdom | To evaluate the effectiveness of two psychodynamic psychotherapy teaching methods, student psychotherapy scheme (SPS) and Balint group, on doctor-patient communication and the doctor-patient relationship | 28 (out of the 49 volunteered, who were subsequently interviewed for suitability) first-year clinical medical students | Randomised controlled trial of three groups, 10 students each (SPS group, Balint group starting at baseline and Balint group starting at 3 months-acting as partial controls) They were rated on a questionnaire testing their knowledge of emotional and psychodynamic aspects of the doctor-patient relationship administered at baseline, at 3 months and at 1 year | At 3 months, students in the SPS and Balint groups scored higher than the partial control group, the difference approaching significance at the 5% level. At 1 year, participation in either teaching method led to significantly higher scores compared with baseline. Psychodynamic psychotherapy teaching methods are effective in increasing students’ knowledge of the doctor-patient relationship and potentially also improving their communication skills | No control group at 1 year The small number of students involved and the low number of questionnaires returns at 3 months underpower the analysis Unvalidated measure of communication skill No attempt on investigator blinding | 3 | 77% | - |
References
- Sandars, J. The use of reflection in medical education: AMEE guide no. 44. Med. Teach. 2009, 31, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, A. Reflective practice: Has it really changed over time? Reflective Pract. 2015, 16, 717–730. [Google Scholar] [CrossRef]
- de Cossart, L.; Fish, D.; Hillman, K. Clinical Reflection: A vital process for supporting the development of wisdom in doctors. Curr. Opin. Crit. Care 2012, 18, 712–717. [Google Scholar] [CrossRef]
- Atkinson, D.; Rosentock, J. A role for Balint groups in medical student training. Ann. Behav. Sci. Med. Educ. 2015, 21, 38–43. [Google Scholar] [CrossRef]
- O’Sullivan, H.; van Mook, W.; Fewtrell, R.; Wass, V. Integrating professionalism into the curriculum: AMEE guide no. 61. Med. Teach. 2012, 34, e64–e77. [Google Scholar] [CrossRef] [Green Version]
- Peters, A.; Greenberger-Rosovsky, R.; Crowder, C.; Block, S.; Moore, G.T. Long-term outcomes of the New Pathway Program at Harvard Medical School: A randomized controlled trial. Acad. Med. 2000, 75, 470–479. [Google Scholar] [CrossRef]
- Watling, C.; Brown, J. Education research: Communication skills for neurology residents: Structured teaching and reflective practice. Neurology 2007, 69, E20–E26. [Google Scholar] [CrossRef] [Green Version]
- Kanthan, R.; Senger, J. An appraisal of students’ awareness of ‘self-reflection’ in a first-year pathology course of undergraduate medical/dental education. BMC Med. Educ. 2011, 23, 67. [Google Scholar] [CrossRef] [Green Version]
- Koole, S.; Dornan, T.; Aper, L.; Scherpbier, A.; Valcke, M.; Cohen-Schotanus, J.; Derese, A. Does reflection have an effect upon case-solving abilities of undergraduate medical students? BMC Med. Educ. 2012, 12, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, B.R.; Mack, J.; Sabus, C.; Becker, D.; Shaw, P.; Diederich, E. Interprofessional Procedure Training for Medicine and Nursing Students. MedEdPORTAL 2020, 16, 10884. [Google Scholar] [CrossRef]
- Oldham, D. A Year Like No Other: The Impact of COVID-19 on Medical Student Stress in WA [Internet]. AMA WA. 2021. Available online: https://www.amawa.com.au/blog/a-year-like-no-other-the-impact-of-covid-19-on-medical-student-stress-in-wa/ (accessed on 15 March 2022).
- Kemp, S.; Hu, W.; Bishop, J.; Forrest, K.; Hudson, J.N.; Wilson, I.; Teodorczuk, A.; Rogers, G.D.; Roberts, C.; Wearn, A. Medical student wellbeing—A consensus statement from Australia and New Zealand. BMC Med. Educ. 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Curtin University. Systematic Reviews: Formulating the Research Question [Internet]. 2021. Available online: https://libguides.library.curtin.edu.au/c.php?g=https://libguides.library.curtin.edu.au/c.php?g=863554&p=6191899 (accessed on 29 March 2022).
- PRISMA-P Group; Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attree, P.; Milton, B. Critically appraising qualitative research for systematic reviews: Defusing the methodological cluster bombs. Evid. Policy J. Res. Debate Pract. 2006, 2, 109–126. [Google Scholar] [CrossRef]
- Kmet, L.; Cook, L.; Lee, R. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research (AHFMR): Edmonton, AB, Canada, 2004. [Google Scholar]
- Bhutada, A.; Davis, T.; Focht, K. Electrophysiological Measures of Swallowing Functions: A Systematic Review. Dysphagia 2022, 37, 1633–1650. [Google Scholar] [CrossRef] [PubMed]
- Heilbronn, B.; Doma, K.; Sinclair, W.; Connor, J.; Irvine-Brown, L.; Leicht, A. Acute Fatigue Responses to Occupational Training in Military Personnel: A Systematic Review and Meta-Analysis. Mil. Med. 2022, 188, 969–977. [Google Scholar] [CrossRef]
- OCEBM Levels of Evidence Working Group. The Oxford 2011 Levels of Evidence [Internet]; Oxford Centre for Evidence-Based Medicine: Oxford, UK, 2011; Available online: http://www.cebm.net/index.aspx?o=5653 (accessed on 4 January 2022).
- Higgins, J.; Green, S. What Is Heterogeneity? Cochrane Handbook for Systematic Reviews of Interventions Version 510 [Internet]; The Cochrane Collaboration: London, UK, 2011; Available online: http://www.handbook.cochrane.org (accessed on 22 March 2022).
- Braun, V.; Clarke, V. Thematic analysis. In APA Handbook of Research Methods in Psychology; American Psychological Association: Washington, DC, USA, 2012; pp. 57–71. [Google Scholar]
- Bird, A.; Tomescu, O.; Oyola, S.; Houpy, J.; Anderson, I.; Pincavage, A. A Curriculum to Teach Resilience Skills to Medical Students During Clinical Training. MedEdPORTAL 2020, 16, 10975. [Google Scholar] [CrossRef]
- Chou, C.; Johnston, C.; Singh, B.; Garber, J.; Kaplan, E.; Lee, K.; Teherani, A. A “safe space” for learning and reflection: One school’s design for continuity with a peer group across clinical clerkships. Acad. Med. 2011, 86, 1560–1565. [Google Scholar] [CrossRef] [Green Version]
- Duke, P.; Grosseman, S.; Novack, D.; Rosenzweig, S. Preserving third year medical students’ empathy and enhancing self-reflection using small group “virtual hangout” technology. Med. Teach. 2015, 37, 566–571. [Google Scholar] [CrossRef]
- Gold, J.A.; Bentzley, J.P.; Franciscus, A.M.; Forte, C.; De Golia, S.G. An Intervention in Social Connection: Medical Student Reflection Groups. Acad. Psychiatry 2019, 43, 375–380. [Google Scholar] [CrossRef]
- Imperato, A.; Strano-Paul, L. Impact of Reflection on Empathy and Emotional Intelligence in Third-Year Medical Students. Acad. Psychiatry 2021, 45, 350–353. [Google Scholar] [CrossRef]
- Plack, M.M.; Driscoll, M.; Marquez, M.; Greenberg, L. Peer-Facilitated Virtual Action Learning: Reflecting on Critical Incidents During a Pediatric Clerkship. Acad. Pediatr. 2010, 10, 146–152. [Google Scholar] [CrossRef]
- Brand, G.; Osborne, A.; Carroll, M.; Carr, S.E.; Etherton-Beer, C. Do photographs, older adults’ narratives and collaborative dialogue foster anticipatory reflection (“preflection”) in medical students? BMC Med. Educ. 2016, 16, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajree, N. Can Balint groups fill a gap in medical curricula? Clin. Teach. 2021, 18, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Yakeley, J.; Shoenberg, P.; Morris, R.; Sturgeon, D.; Majid, S. Psychodynamic approaches to teaching medical students about the doctor-patient relationship: Randomised controlled trial. Psychiatrist 2011, 35, 308–313. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, S.; Foster, K.; Gilbert-Obrart, A. The Balint group experience for medical students: A pilot project. Psychoanal. Psychother. 2015, 30, 96–108. [Google Scholar] [CrossRef]
- Parker, S.; Leggett, A. Teaching the clinical encounter in psychiatry: A trial of Balint groups for medical students. Australas. Psychiatry 2012, 20, 343–347. [Google Scholar] [CrossRef]
- Parker, S.; Leggett, A. Reflecting on our practice: An evaluation of Balint groups for medical students in psychiatry. Australas. Psychiatry 2014, 22, 190–194. [Google Scholar] [CrossRef]
- Airagnes, G.; Consoli, S.; De Morlhon, O.; Galliot, A.-M.; Lemogne, C.; Jaury, P. Appropriate training based on Balint groups can improve the empathic abilities of medical students: A preliminary study. J. Psychosom. Res. 2014, 76, 426–429. [Google Scholar] [CrossRef]
- Lemogne, C.; Buffel du Vaure, C.; Hoertel, N.; Catu-Pinault, A.; Limosin, F.; Ghasarossian, C.; Le Jeunne, C.; Jaury, P. Balint groups and narrative medicine compared to a control condition in promoting students’ empathy. BMC Med. Educ. 2020, 20, 412. [Google Scholar] [CrossRef]
- Chu, S.; Lin, C.; Lin, M.; Wen, C. Psychosocial issues discovered through reflective group dialogue between medical students. BMC Med. Educ. 2018, 18, 12. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.; Lin, M.; Lin, C.; Chu, S. Exploratory study of the characteristics of feedback in the reflective dialogue group given to medical students in a clinical clerkship. Med. Educ. Online 2015, 20, 25965. [Google Scholar] [CrossRef]
- Lutz, G.; Pankoke, N.; Goldblatt, H.; Hofmann, M.; Zupanic, M. Enhancing medical students’ reflectivity in mentoring groups for professional development—A qualitative analysis. BMC Med. Educ. 2017, 17, 122. [Google Scholar] [CrossRef] [Green Version]
- McManus, S.; Killeen, D.; Hartnett, Y.; Fitzgerald, G.; Murphy, K.C. Establishing and evaluating a Balint group for fourth-year medical students at an Irish University. Ir. J. Psychol. Med. 2020, 37, 99–105. [Google Scholar] [CrossRef]
- Engel, G. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Borrell-Carrió, F.; Suchman, A.; Epstein, R. The Biopsychosocial Model 25 Years Later: Principles, Practice, and Scientific Inquiry. Ann. Fam. Med. 2004, 2, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Moscrop, A. ‘Heartsink’ patients in general practice: A defining paper, its impact, and psychodynamic potential. Br. J. Gen. Pract. 2011, 61, 346–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senger, E. Ageism in medicine a pressing problem. Can. Med. Assoc. J. 2019, 191, E55–E56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badenhorst, W.; Rubitel, A. Freud and medical student education: Introducing an elective course. J. Am. Psychoanal. Assoc. 2021, 69, 1145–1152. [Google Scholar] [CrossRef]
- Maudsley, G.; Strivens, J. Promoting professional knowledge, experiential learning and critical thinking for medical students. Med. Educ. 2000, 34, 535–544. [Google Scholar] [CrossRef]
- Guraya, S.; Guraya, S.; Almaramhy, H. The legacy of teaching medical professionalism for promoting professional practice: A systematic review. Biomed. Pharmacol. J. 2016, 9, 809–817. [Google Scholar] [CrossRef]
- Cribb, A.; Bignold, S. Towards the reflexive medical school: The hidden curriculum and medical education research. Stud. High. Educ. 1999, 24, 195–209. [Google Scholar] [CrossRef]
- Coulehan, J. Viewpoint: Today’s professionalism: Engaging the mind but not the heart. Acad. Med. 2005, 80, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Lack, L.; Yielder, J.; Goodyear-Smith, F. Evaluation of a compulsory reflective group for medical students. J. Prim. Health Care 2019, 11, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Patnode, C.; Berkman, N.; Bass, E.B.; Chang, S.; Hartling, L.; Murad, M.H.; Treadwell, J.R.; Kane, R.L. Recommendations for assessing the risk of bias in systematic reviews of health-care interventions. J. Clin. Epidemiol. 2018, 97, 26–34. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, K.C.Y.; Peisah, C. A Mixed-Methods Systematic Review of Group Reflective Practice in Medical Students. Healthcare 2023, 11, 1798. https://doi.org/10.3390/healthcare11121798
Leung KCY, Peisah C. A Mixed-Methods Systematic Review of Group Reflective Practice in Medical Students. Healthcare. 2023; 11(12):1798. https://doi.org/10.3390/healthcare11121798
Chicago/Turabian StyleLeung, Kelvin C. Y., and Carmelle Peisah. 2023. "A Mixed-Methods Systematic Review of Group Reflective Practice in Medical Students" Healthcare 11, no. 12: 1798. https://doi.org/10.3390/healthcare11121798